
Abstract
-
Wide range of pathologies may present with abdominal pain.
-
Key to reach proper diagnosis is adequate history and physical examination along with laboratory tests and imaging.
-
Disposition of patients with abdominal pain is as difficult as its diagnosis.
-
Low threshold should be kept for high-risk patients.
-
Life-threatening diseases should not be missed in emergency.
You have full access to this open access chapter, Download chapter PDF
Similar content being viewed by others



Keywords
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
FormalPara Key Points-
Wide range of pathologies may present with abdominal pain.
-
Key to reach proper diagnosis is adequate history and physical examination along with laboratory tests and imaging.
-
Disposition of patients with abdominal pain is as difficult as its diagnosis.
-
Low threshold should be kept for high-risk patients.
-
Life-threatening diseases should not be missed in emergency.
Introduction
-
Abdominal pain is one of the most common reasons for emergency department visits. Incidence is around 10–12 % globally. Demographic factors like age, gender, ethnicity and family history affect its presentation.
-
It is paramount for emergency physicians to have methodical approach in history, physical examination, investigation and treatment. Clinical suspicion of life-threatening diseases in high-risk patients is utmost important.
Pathophysiology
-
Many intra-abdominal and extra-abdominal diseases are responsible for abdominal pain.
-
Nature of abdominal pain can be divided into three categories based on neurological pathways:
-
Somatic (parietal) pain:
It results from irritation of parietal peritoneum caused by inflammation, infection or chemical reaction. It is supplied by myelinated nerve fibres. It is localised and constant. As the disease process evolves and irritates parietal peritoneum, we can elicit tenderness, guarding and rigidity. The patient prefers to lie immobile.
-
Visceral pain:
It is caused by stretching of walls of hollow viscera, innervated by unmyelinated fibres. It is diffuse and intermittent, dull aching and colicky in nature. Patients keep tossing on the bed. It is felt in the abdominal region which correlates to the somatic segment of embryonic region. Foregut, midgut and hindgut structures (Table 26.1) relate to upper, middle and lower abdomen, respectively. Visceral pain can be perceived away from actual disease process, i.e. pain of acute appendicitis is felt around umbilicus initially as it corresponds to T10 somatic distribution.
Table 26.1 Abdominal structures and its origin -
Referred pain:
It is defined as a pain that is felt away from the site of origin. Common anatomical origin or same nerve root innervations are primary reasons for such pain (Fig. 26.1).
Fig. 26.1 
Common locations for referred pain
-

Clinical Features
-
History:
-
Age and gender are important history points. Elderly patients with nonspecific complaints may have serious pathology. In females, obstetrics and gynaecological causes should be considered.
-
Pain can be described as (SCRIPT FADO):
-
Site
-
Character
-
Radiation
-
Intensity
-
Precipitating/relieving factors
-
Time duration
-
Frequency
-
Associated features
-
Diurnal variation
-
Onset
-
-
Gastrointestinal complaints (anorexia, nausea, vomiting, altered bowel habits, haematemesis, haematochezia, abdominal distension, back pain), genitourinary problems (urinary complains, foul discharge), thoracic complaints (chest pain, breathlessness, palpitation) and constitutional symptoms (fever, weight loss)
-
Past history: Regarding previous similar episodes, admissions, investigations and treatment
-
Pre-existing medical illness: Diabetes, hypertension, heart diseases, liver/renal diseases, HIV, STD and tuberculosis
-
Medication history: Antibiotics, antiplatelets/anticoagulants, steroids, beta-blockers/calcium channel blockers, NSAIDs, chemotherapeutic agents, etc.
-
Surgical history: Laparotomy, caesarean sections, etc.
-
Obstetric history: Last menstrual period, previous pregnancies/deliveries, abortions, ectopic, IVF, IUCDs and other contraceptive measures
-
Allergies, social history (alcohol/drug addiction), history of last meal and history of trauma
-
-
Physical examination:
-
Despite the development of newer imaging modalities, i.e. ultrasound, CT scan and MRI, physical examination holds a key role in patient evaluation. Some specific signs are summarised in Table 26.2.
Table 26.2 Physical examination correlation -
General examination and vital signs: Appearance, temperature, pulse, blood pressure, respiratory rate, oxygen saturation, GCS, blood glucose measurement and pain score.
-
Inspection: With consent, inspect abdominal skin for scars (adhesions), dilated tortuous vein (spider angiomata, caput medusa), skin eruptions (herpes zoster), haemorrhage or signs of trauma (ecchymosis), foreign body and entry/exit wounds. Distension of abdomen (ascites, intestinal obstruction, ileus) and obvious masses (tumour, hernia, pregnancy, distended bladder, aneurysm) should be examined. Hernia orifices and external genitalia should not be forgotten.
-
Palpation: Focus on locating the site of tenderness, signs of peritonism and palpation of masses. Abdomen is divided into right upper, right lower, left upper and left lower quadrants. Localisation of tenderness guides physician to generate differential diagnosis pertaining to that area. However, one can have diffuse abdominal pain spreading to more than one quadrant, i.e. pain of renal calculus extends from lumbar region to the iliac fossa and groin.
Patients with peritoneal irritation show tenderness, guarding/rigidity and pain with coughing. Guarding could be voluntary or involuntary. Due to lax abdominal wall musculature, guarding and rigidity may be absent in the elderly. Typical rebound tenderness is no longer considered an important examination tool due to painful procedure [1].
Abdominal aorta, liver and spleen sizes can be evaluated by palpation. Elderly patients with history of recent abdominal/flank/low back pain, known hypertension, pulsatile abdominal mass and feeble/absent distal pulses are suggestive of abdominal aortic aneurysm/dissection. Bedside ultrasound facilitates visualisation of increased abdominal aortic diameter and determines further surgical/medical management.
-
Percussion: Helpful to assess free air intraperitoneum, degree of ascites, gas-filled bowel loops and peritonitis. It is not very useful in noisy ED.
-
Auscultation: It gives information regarding bowel and vascular status. Absent or diminished bowel sound indicates ileus, mesenteric ischaemia, narcotic use or peritonitis. Hyperactive bowel sounds suggest small bowel obstruction, enteritis or early ischaemic intestine. High pitched tinkling sound reflects mechanical obstruction.
-
Digital rectal examination: Useful for detection of perianal and rectal pathologies (haemorrhoids, fissure and fistula), intraluminal intestinal haemorrhage (dark maroon/red stool), proctitis and constipation (faecal impaction and intestinal obstruction). It is no more useful in diagnosing acute appendicitis [2].
-
Emergency physicians should be vigilant and think of serious pathology in presence of any of the following clinical features:
-
Abdominal pain prior to vomiting
-
Haematemesis/haematochezia
-
Confusion
-
Toxic appearance
-
Signs of shock/dehydration
-
Localised/generalised tenderness
-
Guarding/rigidity
-
Absent bowel sound
-
-
Differential Diagnosis
Extensive differential considerations ranging from simple nonspecific abdominal pain to severe life-threatening conditions are mentioned in Table 26.3.
It is essential to suspect life-threatening conditions (Box 26.1) in haemodynamically unstable. Early resuscitation and stabilisation should be followed by investigations and hospitalisation of such patients.
Box 26.1 Life-Threatening Conditions
Acute intestinal obstruction |
Viscus perforation |
Traumatic rupture of the spleen/liver/bowel |
Acute pancreatitis |
Mesenteric ischaemia |
Ruptured abdominal aortic aneurysm |
Ruptured ectopic pregnancy |
Myocardial infarction |
Women of reproductive age group with abdominal pain should undergo pregnancy test and seek gynaecological consult and bedside ultrasonography if necessary. Consider ectopic pregnancy in such patients unless proven otherwise.
It is not necessary to reach proper diagnosis despite availability of various tests. It is incumbent to consider extra-abdominal causes (Table 26.4) in such patients before considering it as nonspecific.
Investigations
-
Laboratory evaluation in addition to history and clinical findings aid in diagnosis (Box 26.2).
Box 26.2 Routine Laboratory Workup
Haematocrit: GI bleed |
WBC count: infection/inflammation, though of limited value [4, 5] |
Platelet count: bleeding disorders |
Liver profile: hepatitis, cholecystitis, post hepatic biliary tract obstruction |
Coagulation profile: status of coagulopathy, bleeding disorders, trauma |
Renal profile: prerenal, renal or post renal failure, degree of dehydration, renal insufficiency, electrolyte imbalance |
Pancreatic enzymes: pancreatitis, other pancreatic pathologies. Lipase is more sensitive when it is 3 times higher than normal value [6] |
Serum lactate level: mesenteric ischaemia, bowel infarction. May be normal in 25 % of patients with intestinal ischaemia [7] |
Serum glucose: pancreatitis, diabetic/alcoholic ketoacidosis |
Urine analysis: UTI, nephrolithiasis, pyelonephritis, cystitis, renal parenchymal disorders |
Urine sugar/ketone dipstick: diabetic ketoacidosis |
Urine culture: UTI |
Urine pregnancy test: females in reproductive age group |
Stool for occult blood: upper GI bleed |
Stool culture, stool for ova and hanging drop test: diarrhoea |
-
-
Diagnostic imaging: Traditional x-rays, ultrasonography, computed tomography (CT) scan and magnetic resonance imaging (MRI) are available modalities.
Upright chest and abdomen x-rays: An upright chest x-ray detects 1 ml of air in peritoneal cavity [8]. Lateral decubitus x-ray shows 5–10 ml of intraperitoneal air (pneumoperitoneum) in bedridden patients.
Indications (Fig. 26.2):
Small/large bowel obstruction
Hollow viscus perforation
Sigmoid/caecal volvulus
Foreign body
Ingested metal (e.g. mercury)
Ultrasonography: Ultrasound probe is emergency physician’s stethoscope in recent times. It has 94 % sensitivity and 78 % specificity for detecting acute cholecystitis [9]. It is efficient in detecting gallstones and intrahepatic and extrahepatic biliary tract diameter. Abdominal/transvaginal sonography is useful in detecting ovarian, uterine and adnexal abnormalities.
Intraperitoneal free fluid can be visualised on US scan in trauma (FAST) and nontrauma patients.
Bedside sonography is useful in following conditions:
-
Intraperitoneal free fluid
-
Hydronephrosis/hydroureter
-
Intrauterine pregnancy
-
Abdominal aorta diameter (aneurysm)
-
Volume status with IVC diameter (RUSH protocol)
-
Bladder volume (urinary retention)
Disadvantages: Operator dependent
-
Fig. 26.2 
Step-ladder pattern in cases of bowel obstruction
Fig. 26.3 
Intraperitoneal free fluid (FF) in cases of ascites or trauma
Fig. 26.4 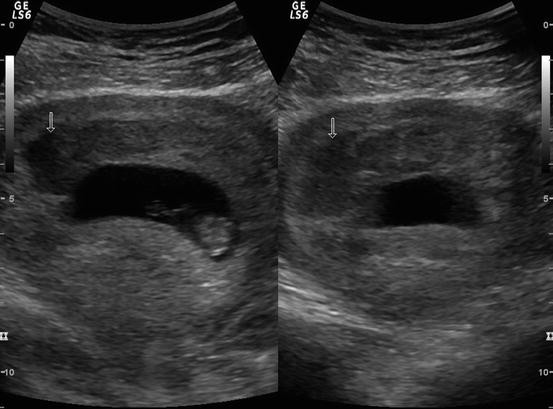
Intrauterine gestational sac with sub-chorionic haemorrhage (marked as arrow)
-



Computed tomography: It is sensitive and accurate in diagnosing acute appendicitis, bowel wall diseases, solid organs, urinary tract calculi, mesenteric ischaemia and retroperitoneal structures. It is useful in differentiating mechanical vs. paralytic bowel obstruction.
CT scan of abdomen has become an imaging modality of choice. Intraperitoneal and extraperitoneal structures can be visualised through CT scan. It helps to reduce morbidity and mortality. Elderly people are more prone to undergo surgery and have higher mortality than young patients. Moreover, history, vital signs and physical examination are not reliable in elderly due to comorbid conditions and medication use [10].
CT scan is associated with radiation risk. Improved technology and better image resolution have made oral contrast obsolete, and pathologies of solid organ and bowel wall are detected with intravenous contrast only [11] (Fig. 26.5).

CT abdomen with contrast film showing multiple air fluid levels suggestive of intestinal obstruction
Recommended imaging studies based on location of abdominal pain is shown in Table 26.5.
Electrocardiogram is essential especially in elderly people with risk factors.
Treatment
Therapeutic goals for acute abdominal pain patients are primary stabilisation, mitigation from symptoms, diagnosis and treatment of cause.
Primary Stabilisation
Haemodynamic instability may be present in patients with following features:
-
Extremes of age
-
Immunocompromised state
-
Abnormal vital signs
-
Signs of dehydration
Early resuscitation and identification of primary cause are the mainstay of treatment. This includes (OMIV): O, oxygen; M, cardiac monitor; IV, large bore IV lines; and V, vitals. Blood samples should be collected for routine investigations. Blood transfusion should be anticipated in haemorrhagic conditions (ruptured abdominal aortic aneurysm, massive GI haemorrhage, ruptured ectopic pregnancy, traumatic spleen rupture). Bedside ultrasound helps in identification of undifferentiated shock. These patients require prompt surgical consultation.
Analgesics
Early pain management doesn’t mask physical findings, delay diagnosis or increase morbidity and mortality. Analgesics in the form of paracetamol, NSAIDs and opioids like fentanyl or morphine are used depending on pain score. Cope’s early diagnosis of acute abdomen [15] favours opioid analgesia in abdominal pain patients.
Antacids and Antiemetics
Antacids relieve burning pain due to gastric acid production [16]. Antiemetics like ondansetron and metoclopramide are useful in remitting nausea and vomiting. NG tube is essential in patients with small bowel obstruction to decompress stomach and provide symptomatic relief. Metoclopramide has extrapyramidal side effects.
Antibiotics
Administration of antibiotics is useful in cessation of disease process and early recovery. Antibiotics should cover gram-negative anaerobic and aerobics and extended to gram-positive pathogens too. Table 26.6 shows some commonly used regimens.
Disposition and Follow-Up
Decision to discharge is as difficult as diagnosis of acute abdominal pain. Various available options are:
-
Admission and surgical/nonsurgical consultation
-
Admission for observation
-
Discharge with follow-up advice
Indications for hospitalisation:
-
Elderly and immunocompromised
-
Intractable nausea, vomiting and abdominal pain
-
Appears ill with unclear diagnosis
-
Intolerable oral intake
-
Abnormal physical examination (signs of peritonitis)
-
Poor social support
Patients with less severe symptoms without specific diagnosis need laboratory/radiological evaluation and observation for 8–10 h in ED. Follow-up with primary care physician in 12 h is another valid option.
Stable asymptomatic patients can be discharged from emergency. Discharge criteria may include:
-
Asymptomatic
-
No abnormal clinical features
-
Normal vital signs
-
Tolerate oral intake
-
Adequate social support at home
Patients should be given proper diet advice and safety instructions.
References
Macaluso CR, McNamara RM. Evaluation and management of acute abdominal pain in the emergency department. Int J Gen Med. 2012;5:789–97.
Brewster GS, Herbert ME. Medical myth: a digital rectal examination should be performed on all individuals with suspected appendicitis. West J Med. 2000;173:207–8.
Purcell TB. Nonsurgical and extraperitoneal causes of abdominal pain. Emerg Med Clin North Am. 1989;7:721.
Bundy DG, Byerley JS, Liles EA, et al. Does this child have appendicitis? JAMA. 2007;298:438–51.
Kessler N, Cyteval C, Gallix B, et al. Appendicitis: evaluation of sensitivity, specificity, and predictive value of US, Doppler US, and laboratory findings. Radiology. 2004;230:472–8.
Chang JWY, Chung CH. Diagnosing acute pancreatitis: amylase or lipase? Hong Kong J Emerg Med. 2011;18(1):20–5.
Kassahun WT, Schulz T, Richter O, Hauss J. Unchanged high mortality rates from acute occlusive intestinal ischemia: six year review. Langenbecks Arch Surg. 2008;393:163. PMID: 18172675.
Miller RE, Nelson SW. The roentgenologic demonstration of tiny amounts of free intraperitoneal gas: experimental and clinical studies. AJR Am J Roentgenol. 1971;112:574–85.
Spence SC, Teichgraeber D, Chandrasekhar C. Emergent right upper quadrant sonography. J Ultrasound Med. 2009;28:479. PMID: 19321676.
Esses D, et al. Ability of CT to alter decision making in elderly patients with acute abdominal pain. Am J Emerg Med. 2004;22:270.
Lee SY, et al. Prospective comparison of helical CT of the abdomen and pelvis without and with oral contrast in assessing acute abdominal pain in adult emergency department patients. Emerg Radiol. 2006;12:150.
Bree RL, Foley WD, Gay SB, et al., for the Expert Panel on Gastrointestinal Imaging. American College of Radiology ACR Appropriateness Criteria. Right upper quadrant pain. http://www.acr.org/SecondaryMainMenuCategories/quality_safety/app_criteria.aspx. Accessed 24 Aug 2007.
Bree RL, Blackmore CC, Foley WD, et al., for the Expert Panel on Gastrointestinal Imaging. American College of Radiology ACR Appropriateness Criteria. Right lower quadrantpain. http://www.acr.org/SecondaryMainMenuCategories/quality_safety/app_criteria.aspx. Accessed 24 Aug 2007.
Levine MS, Bree RL, Foley WD, et al., for the Expert Panel on Gastrointestinal Imaging. American College of Radiology ACR Appropriateness Criteria. Left lower quadrantpain. http://www.acr.org/SecondaryMainMenuCategories/quality_safety/app_criteria.aspx. Accessed 24 Aug 2007.
Silen W. Cope’s early diagnosis of the acute abdomen. 21st ed. New York: Oxford University Press; 2005.
Berman DA, Porter RS, Graber M. The GI cocktail is no more effective than plain liquid antacid: a randomized, double blind clinical trial. J Emerg Med. 2003;25:239.
Chey WD, et al. American College of Gastroenterology guideline on the management of H. Pylori infection. Am J Gastroenterol. 2007;102:1808–25.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2016 Springer India
About this chapter
Cite this chapter
Mehta, H. (2016). Abdominal Pain. In: David, S. (eds) Clinical Pathways in Emergency Medicine. Springer, New Delhi. https://doi.org/10.1007/978-81-322-2710-6_26
Download citation
DOI: https://doi.org/10.1007/978-81-322-2710-6_26
Published:
Publisher Name: Springer, New Delhi
Print ISBN: 978-81-322-2708-3
Online ISBN: 978-81-322-2710-6
eBook Packages: MedicineMedicine (R0)