
Abstract
Deformities of the elbow in the sagittal plane (flexion and extension deformities) will result in reduction in the range of motion of the elbow but coronal plane deformities will not restrict motion (Fig. 27.1). Unlike what is seen in the shoulder, minor degrees of reduction of both flexion and extension will attract the attention of the parents even though they may not cause significant functional disability.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others



Keywords
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
1 Introduction
Deformities of the elbow in the sagittal plane (flexion and extension deformities) will result in reduction in the range of motion of the elbow but coronal plane deformities will not restrict motion (Fig. 27.1). Unlike what is seen in the shoulder, minor degrees of reduction of both flexion and extension will attract the attention of the parents even though they may not cause significant functional disability.

(a, b) Full range of motion of the elbow in a child with cubitus varus
Cubitus varus and valgus develop secondary to bony abnormalities, while flexion and extension deformities are more often due to soft tissue contractures.
Apart from deformities of the elbow that are evident at birth and persist into later childhood (see Chap. 8), there are developmental and acquired deformities that initially manifest in the young child; these are discussed in this chapter.
2 Establishing the Diagnosis of the Cause of Cubitus Varus and Valgus
2.1 Questions to Establish a Diagnosis of Cubitus Varus and Valgus
-
Are there bilateral symmetric deformities?
-
Is there a history of trauma preceding the onset of the deformity?
-
Is the deformity progressive?
-
Are the radius and ulna of normal length and alignment?
-
Are the stature and body proportions normal?
-
Are there bilateral symmetric deformities?
-
Unilateral cubitus varus or valgus is likely to be on account of trauma or localized growth abnormality. Bilateral symmetric deformities occur in skeletal dysplasia and in children with chromosomal abnormalities.
-
Is there a history of trauma preceding the onset of the deformity?
-
The commonest cause for unilateral cubitus varus in childhood is malunion of a supracondylar fracture of the humerus. The deformity that develops due to the malunion is aptly described as a gunstock deformity (Fig. 27.2). Cubitus valgus more commonly follows a fracture of the lateral condyle. Though these injuries may occur in the preschool age, they are more frequently seen in children who are a few years older.
Fig. 27.2 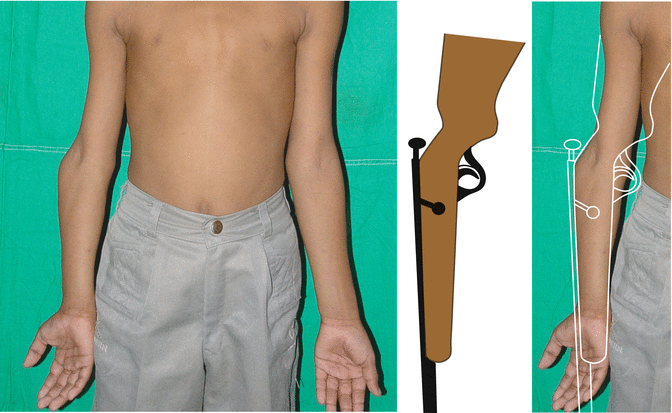
Cubitus varus of the right elbow due to malunion of a supracondylar fracture of the humerus. The loss of the carrying angle as compared to the normal side and the typical gunstock deformity is seen

-
Is the deformity progressive?
-
Progression of deformity suggests that the growth plate is affected.
-
Are the radius and ulna of normal length and alignment?
-
A short ulna as in hereditary multiple osteochondromatosis may be associated with cubitus varus (Fig. 27.3). A chronically dislocated radial head may be associated with cubitus valgus.
Fig. 27.3 
Radiograph of the forearm of a child with hereditary multiple osteochondromatosis and cubitus varus

-
Are the stature and body proportions normal?
-
Cubitus varus and cubitus valgus are seen in some skeletal dysplasias where altered body proportions and short stature may be present. Sex chromosomal anomalies associated with short stature tend to have cubitus valgus (Baughman et al. 1974).
2.2 Physical Examination
2.2.1 Look
Note the stature of the child and if there is proportionate or disproportionate dwarfism.
Examine the limb in full extension as cubitus varus and valgus may be masked if the elbow is flexed.
2.2.2 Feel
Palpate the distal end of the humerus, proximal ulna, and radius. Note if they are of normal lengths, if their relative positions are maintained, and if there are abnormal prominences close to the end of any of these bones.
2.2.3 Move
Check the active and passive movements of the elbow and forearm.
2.2.4 Measure
Measure the carrying angle with a goniometer and compare the values against available normative data for the age and gender of the child (Balasubramanian et al. 2006; Golden et al. 2007; Yilmaz et al. 2005). The normal mean carrying angle measured clinically in boys aged 5 years is 8.6° ± 4.2° and 10.0° ± 3.0° in girls of the same age (Balasubramanian et al. 2006).
Measure the lengths of the humerus, radius, and ulna.
2.3 Investigations to Confirm the Diagnosis
Plain Radiographs
Plain radiographs of the affected limb should enable a definitive diagnosis and the severity of the deformity can be estimated by measuring the Baumann’s angle provided the elbow extends fully (Acton and McNally 2001) (Fig. 27.4).

Technique of measuring the Baumann’s angle from an anteroposterior radiograph
MRI Scan
If growth plate damage is suspected, MR imaging may be undertaken to delineate the growth plate clearly (Kim et al. 2002).
An outline of the approach to establishing the cause of cubitus varus or valgus in the school-going child is shown in Table 27.1.
2.4 Differential Diagnosis
2.4.1 Complication of Fracture of Distal Humerus
Cubitus varus and valgus deformities following fractures of the distal humerus are frequently seen in older children; cubitus varus is most frequently seen after malunion of a supracondylar fracture, while cubitus valgus is seen following a lateral condylar fracture. Though this is the common pattern, in rare instances the reverse pattern may be encountered.
2.4.2 Hereditary Multiple Osteochondromatosis
Abnormal growth patterns are seen in bones in hereditary multiple osteochondromatosis. The location of the osteochondroma and its proximity to the growth plate determine the pattern of growth abnormality (Cho and Jung 2014; Matsubara et al. 2006).
3 Establishing the Cause of Limitation of Elbow Motion and Flexion or Extension Deformity of the Elbow
Limitation of active motion of the elbow is mainly due to weakness of the flexors or extensors, while the loss of passive motion is due to fixed deformities. Fixed flexion or extension deformities that are not evident at birth and first noted in the young child are almost always due to soft tissue contractures frequently involving the flexor or extensor muscles.
3.1 Questions to Establish a Diagnosis of Flexion or Extension Deformity of the Elbow
-
Is there a history of injections into the arm?
-
Are there features of obstetric brachial plexus palsy or cerebral palsy?
-
Are there features of a skeletal dysplasia?
-
Is there a history of injections into the arm?
-
A history of injections into the triceps in infancy may be present.
-
Are there features of obstetric brachial plexus palsy or cerebral palsy?
-
A history of a difficult birth or delayed milestones may point to a neurological insult resulting in muscle contracture.
-
Are there features of a skeletal dysplasia?
-
If there are features such as dwarfism and symmetric deformities of the upper and lower limbs, the child may have a skeletal dysplasia.
-
Is there a history of infection at or in the vicinity of the elbow?
-
Fibrosis of the flexor or extensor muscles of the arm can ensue after osteomyelitis of the humerus or bony ankylosis of the elbow can follow septic arthritis of the elbow.
3.2 Physical Examination
3.2.1 Look
Note if there is wasting of the muscles of the shoulder, arm, and forearm. Note if the affected limb is hypoplastic. Note if there are other symmetric abnormalities suggestive of a skeletal dysplasia.
Ask the child to raise the arm above the shoulder and note if the elbow remains extended (Fig. 27.5) or if it drops into flexion.

Flexion deformity of the right elbow in a child with obstetric brachial plexus palsy. Note that when she raises her arms above the shoulder, the elbow remains extended up to the point of the fixed flexion deformity. This demonstrates that the power of the triceps is at least Grade III on the MRC scale. Note that the limb is hypoplastic; this is a feature of paralytic conditions affecting growing children
3.2.2 Move and Measure
Measure the ranges of active and passive movements of the elbow and note if they are the same. Measure and record the muscle power of the flexors and extensors of the elbow.
3.3 Investigations to Confirm the Diagnosis
Plain Radiographs
Plain radiographs of the affected limb and a complete skeletal survey are indicated if a skeletal dysplasia is suspected.
3.4 Differential Diagnosis
3.4.1 Obstetric Brachial Plexus Palsy
A flexion deformity of the elbow may develop in children with weak elbow extensors, while an extension deformity may develop if the flexors are weaker than the extensors. Demonstrable weakness of the antagonistic muscle is usually present in these children; the weakness however may not be profound (Fig. 27.5).
3.4.2 Cerebral Palsy
Flexion deformity of the elbow may be seen in children with cerebral palsy. This is usually in association with pronation of the forearm and flexion of the wrist due to spasticity of the flexors and pronators (Landi et al. 2003; Manske et al. 2001).
3.4.3 Arthrogryposis
The elbow may be in flexion or extension in arthrogryposis. When the elbow is extended often, there are associated weakness of the biceps and contracture of the triceps. Both these issues will need to be addressed to restore function.
3.4.4 Injection Fibrosis of the Triceps Muscle
Fibrosis and contracture of the triceps muscle have been described following injections into the muscle (Babhulkar 1985).
3.4.5 Ankylosis of the Elbow
The elbow joint is particularly prone to develop extra-articular stiffness following trauma or infection. Rarely bony ankylosis may develop as a complication of joint sepsis. The position of fusion determines the extent of functional disability. An elbow ankylosed in some degree of flexion is more functional than one fused in full extension (Fig. 27.6).

Ankylosis of the elbow following septic arthritis complicating osteomyelitis of the humerus. The functional limitations of an elbow fused in flexion are shown
3.4.6 Fixed Flexion Deformity of the Elbow Associated with a Dysplasia or Syndrome
Flexion deformity of the elbow may be seen in several syndromes and skeletal dysplasias including chondrodysplasia punctata, mucopolysaccharidoses, and Schmid metaphyseal dysplasia, Larsen syndrome (Fig. 27.7), and distal humeral dysplasia (Joseph 2000; Joseph and Varghese 2003). In some of these situations, the radial head may be dislocated and in a few the distal end of the humerus may be dysplastic and the elbow dislocated (Hermanns et al. 2008; Joseph and Varghese 2003).

Flexion deformity of the elbow in a child with Larsen syndrome
An outline of establishing the cause of limitation of motion and flexion or extension deformities of the elbow in a young child is shown in Table 27.2. The table does not set out the process of identifying the etiology but attempts to show how to identify the pathology since the treatment hinges on recognizing the pathology and correcting it.
References
Acton JD, McNally MA. Baumann’s confusing legacy. Injury. 2001;32:41–3.
Babhulkar SS. Triceps contracture caused by injections. A report of 11 cases. J Bone Joint Surg Br. 1985;67:94–6.
Balasubramanian P, Madhuri V, Muliyil J. Carrying angle in children: a normative study. J Pediatr Orthop B. 2006;15:37–40.
Baughman Jr FA, Higgins JV, Wadsworth TG, et al. The carrying angle in sex chromosome anomalies. JAMA. 1974;230:718–20.
Cho YJ, Jung ST. Gradual lengthening of the ulna in patients with multiple hereditary exostoses with a dislocated radial head. Yonsei Med J. 2014;55:178–84.
Golden DW, Jhee JT, Gilpin SP, et al. Elbow range of motion and clinical carrying angle in a healthy pediatric population. J Pediatr Orthop B. 2007;16:144–9.
Hermanns P, Unger S, Rossi A, et al. Congenital joint dislocations caused by carbohydrate sulfotransferase 3 deficiency in recessive Larsen syndrome and humero-spinal dysostosis. Am J Hum Genet. 2008;82:1368–74.
Joseph B. Elbow problems in children. In: Gupta A, Kay SPJ, Schecker RL, editors. The growing hand. London: Mosby; 2000. p. 769–82.
Joseph B, Varghese RA. Congenital distal humeral dysplasia: a case report. Pediatr Radiol. 2003;33:7–10.
Kim HT, Song MB, Conjares JN, et al. Trochlear deformity occurring after distal humeral fractures: magnetic resonance imaging and its natural progression. J Pediatr Orthop. 2002;22:188–93.
Landi A, Cavazza S, Caserta G, et al. The upper limb in cerebral palsy: surgical management of shoulder and elbow deformities. Hand Clin. 2003;19:631–48, vii.
Manske PR, Langewisch KR, Strecker WB, et al. Anterior elbow release of spastic elbow flexion deformity in children with cerebral palsy. J Pediatr Orthop. 2001;21:772–7.
Matsubara H, Tsuchiya H, Sakurakichi K, et al. Correction and lengthening for deformities of the forearm in multiple cartilaginous exostoses. J Orthop Sci. 2006;11:459–66.
Yilmaz E, Karakurt L, Belhan O, et al. Variation of carrying angle with age, sex, and special reference to side. Orthopedics. 2005;28:1360–3.
Author information
Authors and Affiliations
Rights and permissions
Copyright information
© 2015 Springer India
About this chapter
Cite this chapter
Joseph, B. (2015). Deformities and Limitation of Movement of the Elbow. In: Paediatric Orthopaedic Diagnosis. Springer, New Delhi. https://doi.org/10.1007/978-81-322-2392-4_27
Download citation
DOI: https://doi.org/10.1007/978-81-322-2392-4_27
Publisher Name: Springer, New Delhi
Print ISBN: 978-81-322-2391-7
Online ISBN: 978-81-322-2392-4
eBook Packages: MedicineMedicine (R0)