
Abstract
Various biopsy procedures such as core needle biopsy, laparoscopic/thoracoscopic biopsy, and excisional/incisional open biopsy are selected according to the purpose, tumor site, and condition of the patient. Tumor biopsy is performed not only for pathological diagnosis but for evaluation of the chemotherapy effects, confirmation of the remaining of the viable malignant cells, and analysis of tumor biology. Biopsy specimens should be divided and appropriately stored for each analysis, for example, formalin fixation-paraffin embedding for histological diagnosis, sterile tissue culture medium for chromosomal analysis, and snap frozen deep freezer storage for DNA/RNA analysis. After biopsy, confirmation of hemostasis is most important.
The figures in this chapter are reprinted with permission from Standard Pediatric Operative Surgery (in Japanese), Medical View Co., Ltd., 2013, with the exception of occasional newly added figures that may appear.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others



Keywords
1 Preoperative Management
1.1 Check the Purpose and Minimum Requirement of the Samples
Ordinary, the purpose of tumor biopsy is to confirm the pathological diagnosis. But in some cases, tumor biopsy is performed not only to identify the pathological diagnosis but for other purposes, such as the evaluation of the chemotherapy effects, confirmation of the remaining of the viable malignant cells, and analysis of tumor biology. Therefore, surgeons should recognize the purposes of the biopsy before operation to obtain the appropriate biopsy samples.
Pathologists and oncologists analyze the various biomarkers such as chromosomal anomalies, gene mutations, and surface markers, so that surgeons should discuss with pathologists and oncologists before biopsy to obtain the sufficient amount of the tumor specimen. And the samples should be divided and appropriately stored for each analysis, for example, formalin fixation-paraffin embedding for histological diagnosis, sterile tissue culture medium for chromosomal analysis, and snap frozen deep freezer storage for DNA/RNA analysis (Fig. 10.1).

Managements of the biopsy specimen
1.2 Check the Image Analysis and Decide the Site and Route of Biopsy
Before biopsy, surgeons should check carefully the image analysis such as CT scan, ultrasonography, and MRI to discuss which part of the tumor should be cut and route should be chosen to approach the tumor. Generally, large vessels and organs should be evaded.
The suitable biopsy site should contain the viable tumor tissue and not contain the necrotic nor hemorrhagic tissue. Biopsy site does not represent the whole of the tumor. If the image analysis shows that the tumor is heterogeneous, biopsy specimens should be obtained from the several different parts.
1.3 Select the Procedure
The decision of the procedure depends on the required amount of the biopsy specimen and biopsy site. The condition of the patients, schedule of chemotherapy, and cosmetic results should also be considered to decide the suitable procedure. In the malignant cases, biopsy procedure should not disturb the schedule of chemotherapy; therefore surgical complication should be minimized. Followings are various biopsy procedures from lower surgical stress to higher. Surgeons will choose the suitable procedure in case by case.
1.3.1 Core Needle Biopsy
Core needle biopsy uses needles which remove a small cylinder of tissue. Ordinary, biopsy is performed using the disposable biopsy needles such as “Tru-Cut™” under the guide of ultrasonography. The main advantages are that it does not require general anesthesia and an incision. It therefore often selected in cases general anesthesia is difficult, such as the cases with huge mediastinal tumor. If the tumor is deep inside the body and cannot be felt, the needle is guided by imaging test such as an ultrasound or CT scan.
In children, pathological diagnosis of the tumors is sometimes very difficult. The specimens of needle biopsy are very small so that sometimes insufficient for the pathological diagnosis. Therefore the indication of needle biopsy is limited in the pediatric cases.
1.3.2 Laparoscopic/Thoracoscopic Needle Biopsy
Needle biopsy is performed under the monitoring of laparoscopy or thoracoscopy. Although general anesthesia is required, this method enables to check the gross appearance of the tumor, and needle biopsy can be performed more accurately and safely.
1.3.3 Laparoscopic/Thoracoscopic Incisional Biopsy
Laparoscopic/thoracoscopic biopsy is less invasive and achieves the good cosmetic results than open biopsy. However it is difficult when the tumor is too large because working space maybe too small. If hemostasis is not achieved, it should immediately be changed to the open surgery.
1.3.4 Open Biopsy
Biopsy is performed under laparotomy or thoracotomy. A surgeon removes the entire tumor (called an excisional biopsy) or a small part of a large tumor (called an incisional biopsy) (Fig.10.2). Surgical stress and operative wound will be large, but sufficient amount of the specimen can be obtained certainly and safely.

Open incisional biopsy for intrathoracic tumor via thoracotomy. The tumor was soft and vascular rich, so that felts were used to press the biopsy site for hemostasis
1.4 Operations
1.4.1 Open Biopsy via Laparotomy
-
1.
Laparotomy should be performed via a part of the estimated surgical incision of the tumor resection surgery in the future to reduce the surgical scar (Fig. 10.3).
Fig. 10.3 
Laparotomy was performed via a part of the estimated surgical incision of the liver resection surgery in the future
-
2.
After laparotomy, search and palpitate the whole of the abdomen to evaluate the tumor extension and metastasis.
-
3.
Dissect the organs in front of the tumor and sufficiently disclose the tumor surface.
-
4.
Biopsy specimens may be damaged by the heat of the electric scalpel or energy devices. Therefore tumor had better be cut sharply by scalpel or surgical scissors to obtain the specimen (Fig. 10.4). Biopsy should be performed quickly to reduce the hemorrhage and hemostasis should be performed immediately. The biopsy specimens should be gently treated to avoid the compression injury.
Fig. 10.4 
Biopsy specimens may be damaged by the heat of the electric scalpel or energy devices. Therefore, the tumor had better be cut sharply by scalpel or surgical scissors
-
5.
Before biopsy, state the suture for hemostasis using a large surgical needle. If the tumor is soft, put the felts or pledgets beside the biopsy sites to avoid cutting of the tumor by the threads (Fig.10.5). Hemostasis is performed using electric scalpel and compresses the tumor tissue by ligating the suture (Figs. 10.2 and 10.6a). When the hemostasis is difficult, fill the biopsy site with hemostatic materials such as Surgicel™ or TachoSil™ and tie over the bleeding site using the suture (Fig. 10.6b).
Fig. 10.5 
Open incisional biopsy for hepatoblastoma via laparotomy. Expose the surface of the tumor sufficiently. Before biopsy, state the suture for hemostasis using a large surgical needle. If the tumor is soft, put the felts or pledgets beside the biopsy sites to avoid cutting of the tumor by the threads. Cut the tumor sharply using surgical scalpel or scissors to avoid the crushing of the specimen
Fig. 10.6 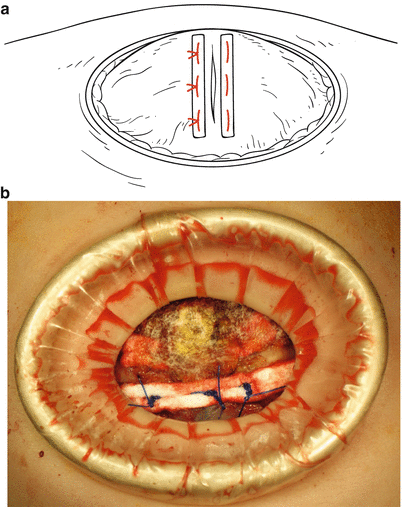
Hemostasis. (a) Hepatoblastoma is soft and vascular rich, to state the suture and put the felts beside the biopsy sites. Hemostasis is performed by filling the biopsy site with hemostatic materials and ligating the suture to tie over the biopsy site. (b) Hemostasis is performed using electric scalpel. When the hemostasis is difficult, fill the biopsy site with hemostatic materials such as Surgicel™ or TachoSil™ and press the bleeding site using the suture
-
6.
During the hemostasis, intraoperative pathological examination will be performed using the frozen sections to confirm that appropriate tumor tissue was included in the specimen.




1.4.2 Laparoscopic/Thoracoscopic Biopsy (Figs. 10.7 and 10.8)

Laparoscopic biopsy for left adrenal neuroblastoma. (a) Three ports, one camera port and two working ports, are inserted before biopsy. (b) Sufficiently disclose the tumor surface. Put the traction suture and cut the tumor sharply by surgical scissors. Hemorrhage from the biopsy site could be controlled by raising the intra-abdominal pressure to 12 cm H2O. The biopsy specimens were put in the plastic bag to collect

Thoracoscopic biopsy for the right mediastinal Ewing sarcoma. Three ports, one camera port and two working ports, are inserted. Biopsy was performed under differential lung ventilation and artificial pneumothorax. Disclose the tumor surface sufficiently and cut the tumor sharply by surgical scissors. Hemorrhage from the biopsy site could be controlled by raising the intrathoracic pressure to 12 cm H2O
-
1.
Decide the port site according to the location of tumor and biopsy route. Ordinary, three ports, one camera port and two working ports, are inserted before biopsy (Fig. 10.7a).
-
2.
Thoracoscopic biopsy is ordinary performed under differential lung ventilation. When the differential lung ventilation is difficult, make the artificial pneumothorax by carbon dioxide gas using the laparoscopic trocar (Fig. 10.8). Search the whole of the abdominal/thoracic space to evaluate the tumor invasion and metastasis.
-
3.
Dissect the organs in front of the tumor and sufficiently disclose the tumor surface.
-
4.
Tumor had better be sharply cut by surgical scissors instead of energy devices to avoid the heat damage of the biopsy specimen. Biopsy should be performed quickly to reduce the hemorrhage. After the biopsy, hemostasis should be performed immediately. Small hemorrhage from the biopsy site can be controlled by raising the intrathoracic pressure to 10 cm H2O or more (Figs. 10.7b and 10.8). If hemostasis is difficult, do not hesitate to convert to the open surgery.
-
5.
The biopsy specimens will be put in the plastic bag to collect.
-
6.
During the hemostasis, intraoperative pathological examination will be performed using the frozen sections to confirm that appropriate tumor tissue was included in the specimen.
2 Postoperative Management
The most important point is hemostasis. Hemorrhage at the biopsy site will be sometimes observed after surgery, therefore watch carefully the hemodynamics and blood count. If hemorrhage is suspected by low-output syndrome or anemia, immediately confirm imaging analysis such as ultrasonography and CT scan.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2016 Springer Japan
About this chapter
Cite this chapter
Oue, T. (2016). Biopsy of Tumor. In: Taguchi, T., Iwanaka, T., Okamatsu, T. (eds) Operative General Surgery in Neonates and Infants. Springer, Tokyo. https://doi.org/10.1007/978-4-431-55876-7_10
Download citation
DOI: https://doi.org/10.1007/978-4-431-55876-7_10
Published:
Publisher Name: Springer, Tokyo
Print ISBN: 978-4-431-55874-3
Online ISBN: 978-4-431-55876-7
eBook Packages: MedicineMedicine (R0)