
Abstract
This chapter reviews the surgical pathologic findings that provided the framework for the General Rules for Clinical and Pathological Studies on Oral Cancer (first edition), which currently serves as the common foundation for the diagnosis, treatment, and study of oral cancer in Japan. Although oral cancer varies from case to case, the clinical findings to which attention should be paid were determined for different cancer types after investigating the factors that can be used to accurately predict clinical manifestations and prognosis. It took approximately 10 years to accumulate a sufficient number of cases and perform data analysis, the findings of which were amassed in the general rules, thereby providing the current notions on oral cancer. We also review the pathologic and prognostic factors, such as clinical type, tumor depth, and invasion route; oral intraepithelial neoplasia/carcinoma in situ; and the histopathological factors associated with malignancy, such as mode of invasion and mode of mandibular invasion.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others



Keywords
2.1 Introduction
For medical professionals in different disciplines to have common knowledge for the diagnosis, treatment, and study of oral cancer, it is necessary to establish criteria and general rules for the management of oral cancer, as exists for other cancers, in Japan. Proper oral cancer general rules will enable the same standards to be used to search imaging, surgical, and pathological findings of oral cancers and to understand the intricate pathology. Useful information should also be accumulated on actual clinical cases across institutions. All of the above will contribute to advancing the diagnostic, treatment, and research approaches for different cancers.
The Japan Society for Oral Tumors (JSOT) focuses on the issues and cases associated with oral cancer. After 10 years of review by 19 oral surgeons, oral radiologists, and oral pathologists, the society published the first edition of General Rules for Clinical and Pathological Studies on Oral Cancer in 2010 [1, 2]. In this chapter, we introduce some of the current notions about oral cancer by reviewing the surgical pathologic findings that served as the foundation for the general rules.
In principle, these general rules conform to the classification recommended by the International Union against Cancer (UICC) [3] and the World Health Organization (WHO) [4]. However, some general rule items were thought to require some modification from these international classifications, and these modifications were proposed in the official journal [5–8] and website of the JSOT.
In this chapter, oral cancer is defined as primary, not secondary, mucosal carcinoma originating at 6 locations in the oral cavity, as defined in the UICC classification: (1) tongue cancer, (2) upper gingival and alveolar cancer, (3) lower gingival and alveolar cancer, (4) buccal mucosal cancer, (5) floor of mouth (FOM) cancer, and (6) hard palate cancer.
2.2 Primary Lesion
The oral cavity is lined with stratified squamous epithelium and is anatomically adjacent to the oropharynx, extending from the upper and lower lips to the terminal sulcus of tongue—the palatoglossal arch—to the posterior margin of the hard palate. The upper and lower teeth and gingiva separate the oral cavity into the oral vestibule and the oral cavity proper. The oral cavity is also the opening to the digestive tract and plays a role in respiration and articulation.
2.2.1 Anatomical Sites and Subsites
-
Tongue (TON-0, 1, 2)
-
Upper gingiva and alveolus (UG)
-
Lower gingiva and alveolus (LG)
-
Buccal mucosa (BM-0, 1, 2, 3, 4)
-
Floor of mouth (FOM)
-
Hard palate (HP)
-
(1)
Tongue: The lingual mucosa encompasses the dorsal surface of the tongue anterior to the circumvallate papillae (anterior 2/3) and the lateral borders (anterior 2/3) and inferior surface of the tongue.
-
(2)
Gingival and alveolar mucosa (maxillary or mandibular): There are two types of gingiva: free gingiva and attached gingiva. The latter is contiguous with the alveolar mucosa and occupies the area surrounded by a transition region to the lips and cheeks on the buccolabial side, the borderline between the horizontal region and the transverse ridges or the vertical region of the upper palate, and the borderline between the horizontal and vertical regions of the soft palate on the labiomandibular side. Although there is no anatomical name for the gingiva of edentulous alveolar ridges because the study of anatomy involves only normal body structures, “alveolar ridge mucosa” may most appropriately explain the gingiva of edentulous alveolar ridges. Gingival cancers include cancers originating from alveolar and alveolar ridge mucosae (Fig. 2.1).
Fig. 2.1 
Anatomical structure of the mandibular gingiva
-
(3)
Buccal mucosa: According to the UICC classification, the mucosal layer of the cheeks, mucosa of the upper and lower alveolobuccal sulci (oral vestibule), mucosa in the retromolar areas, and labial mucosa of the upper and lower lips are collectively termed the buccal mucosa.
-
(a)
Mucosal layer of the cheeks: Area between the upper and lower buccal sulci.
-
(b)
Upper and lower alveolobuccal sulci (oral vestibule): Area extending from the distal surface of the canine anteriorly to the palatoglossal arch posteriorly. This square-shaped area is surrounded by the mucogingival junction and the junction on the buccal mucosa 1 cm from the deepest point in the buccal sulcus.
-
(c)
Retromolar areas: The area posterior to the gingiva, forming the margin of the tonsillar fossa.
-
(d)
Labial mucosa of the upper and lower lips: A square region bordered by the line connecting the corner of the mouth and the distal surface of the canine on the maxilla or mandible, the mucocutaneous junction, and the line 1 cm from the deepest part of the labial groove toward the mucocutaneous junction.
-
(a)
-
(4)
Floor of mouth: The mucosa of the FOM is bordered by the mucogingival junction on the lingual side of the mandible and the tongue–FOM junction.
-
(5)
Hard palate: The mucosa of the hard palate is the triangular region encompassed within the borderline between the horizontal and vertical regions of the palate, the midline of the palate, and the borderline with the soft palate which lacks bone.

2.2.2 Locations of the Lesions (Fig. 2.2)

Anatomical sites and subsites
-
Tongue (TON-0, 1, 2)—dorsal surface (0)/lateral borders (1)/ventral surface (2)
-
Upper gingival and alveolus (UG)
-
Dentulous jaw (teeth: 8/7/6/5/4/3/2/1/1/2/3/4/5/6/7/8)
-
Edentulous jaw (Molar/Premolar/Canine/Incisor/I/C/P/M)
-
-
Lower gingiva and alveolus (LG)
-
Dentulous jaw (teeth: 8/7/6/5/4/3/2/1/1/2/3/4/5/6/7/8)
-
Edentulous jaw (Molar/Premolar/Canine/Incisor/I/C/P/M)
-
-
Buccal mucosa (BM-0, 1, 2, 3, 4)
-
Buccal mucosa (0)/upper buccoalveolar sulcus (oral vestibule) (1U)/lower buccoalveolar sulcus (oral vestibule) (1 L)/retromolar area(2)/upper labial mucosa (3)/lower labial mucosa (4)
-
Anterior type (a)/posterior type (b)
-
-
Floor of mouth (FOM)—median type (a)/lateral type (b)
-
Hard palate (HP)
-
(1)
According to the UICC classification, the tongue is divided into three subsites: the dorsum of the tongue anterior to the circumvallate papillae (anterior 2/3 of the tongue) (TON-0), the lateral boaders of the tongue (TON-1), and the inferior (or ventral) surface of the tongue (TON-2).
-
(2)
The location of lesions in the upper and lower gingival cancer is determined in relation to the teeth on the dentulous jaw or the corresponding teeth on the edentulous jaw. In the latter case, the location of lesion may be specified as an anterior teeth region (A), premolar region (P), or molar region (M). Because the presence and absence of teeth is thought to affect the progress of gingival cancer, the presence of impacted teeth should be recorded.
-
(3)
Similarly, the location of buccal mucosal cancers is determined by dividing the buccal mucosa into five subsites: the mucosa of the cheeks (BM-0), the upper and lower alveolobuccal sulcus (oral vestibule) (BM-1), the retromolar area (BM-2), the labial mucosa of the upper lip (BM-3), and the labial mucosa of the lower lip (BM-4). In addition, because the tissue structure deep inside the oral mucosa varies depending on the anatomical locations, buccal mucosal cancers are further classified into the anterior or posterior type. Anterior type (the mucosa of the cheeks, most of the oral vestibule, and the upper and lower labial mucosae): muscles and fat tissue are present beneath the mucosa, and the outermost layer is the skin. Posterior type (primarily retromolar area): due to the presence of the masseter muscle just adjacent to the buccinator muscle, the medial pterygoid muscle on the side of the pharynx, and the mandible, tumors readily extend into the space between the muscles of mastication (hereinafter masticator space), which is among the poor prognostic factors for oral cancer. Consequently, it is useful to subclassify buccal mucosal cancers into the anterior or posterior type with respect to the anterior margin of the masseter muscle.
-
(4)
FOM cancers are subclassified into the medial and lateral types. Medial FOM cancers are located in the anterior region of the FOM mesial to the junction of the canine and the first premolar on the mandible. Any cancers located in the posterior region of the FOM distal to the region defined above are considered the lateral type. Medial-type FOM cancers, which account for the majority of FOM cancers, often expand into the opening of the salivary gland, sublingual caruncle, and eventually into the contralateral side of the FOM. This type of FOM cancer may also extend to the Wharton tube, sublingual gland, genioglossus muscle, geniohyoid muscle, and the lower anterior tooth area. The submandibular lymph nodes are a frequent site of cervical lymph node metastasis, but metastasis to the submental lymph nodes is rare. Lateral-type FOM cancers often originate from the lateral margin or the root of the tongue, and the determination of tumor range is sometimes difficult in advanced cases. There are two routes for lateral FOM cancers to invade adjacent tissues. First, along the mandibular periosteum, they may invade the mylohyoid muscle and submandibular space from the sublingual gland. These cancers may also invade internally the genioglossus muscle, geniohyoid muscle, styloglossus, and then the hyoglossus and posteriorly the medial pterygoid muscle (masticator space). Cervical lymph node metastasis often involves the submandibular and upper jugular lymph nodes.
2.2.3 Size
-
(long diameter) × (short diameter) × (thickness) cm
-
(mesiodistal diameter) × (buccolingual diameter) × (thickness) cm
2.2.4 Clinical Types
-
Superficial type: tumors primarily showing superficial growth
-
Exophytic type: those primarily showing exophytic growth
-
Endophytic type: those primarily showing endophytic growth
-
Unclassified type: those not belonging to any of the above types
Oral cancers are classified into superficial (Fig. 2.3a), exophytic (Fig. 2.3b), and endophytic (Fig. 2.3c) types based on the clinical manifestations. In general, early (T1, T2) tongue cancers are diagnosed by visual inspection and palpation; however, it is preferable to perform ultrasonographic (US) imaging to confirm the diagnosis. Although visual inspection and palpation are performed to determine tumor invasion depth in or under the mucosal layer, because of individual variations in palpation skills among clinicians, diagnostic accuracy may have a margin of error of ±0.5 cm. Nonetheless, for the diagnosis of T1-2 cancers in soft tissue, palpation can provide fairly accurate supplementary findings to visual inspection. With continued advances in and dissemination of probe-based US examination, it may be possible in the near future to determine the invasion depth of tumors in millimeter increments. At that point, it will be necessary to reestablish a next-generation classification method for invasion patterns of tumors including those in gastric cancer.

Clinical types. (a) Superficial type. (b) Exophytic type. (c) Endophytic type
A previous study investigating the efficacy of clinical classification in 2,224 patients with T1-2 tongue cancer [5] revealed that this clinical type can be used as a prognostic factor for local recurrence, lymph node metastasis, distant metastasis, and 5-year survival rate (Fig. 2.4a, b). Although such classification has some utility in buccal mucosa and FOM cancers, utility is affected by the site of the tumor. Consequently, we decided to subclassify buccal mucosa and FOM cancers into anterior/posterior type and medial/lateral type [6]. However, the utility of clinical classification based on growth patterns is not clear for cancers with a risk of bone invasion, such as gingival and hard palate cancers [7, 8], necessitating further investigation. As we describe later, the classification of lower gingival cancer by mandibular resorption type [9], which reflects mandibular invasion pattern [10], has proven useful [7, 10–13]. After incorporating diagnostic imaging that shows the pathological features at the apical end of cancer invasion, this classification method may be considered to fulfill all the requirements of a next-generation method. However, we decided to record the invasion of adjacent tissues in advanced oral cancers in detail without performing clinical classification, due to unproven utility.

(a) Frequency of clinical types in lingual carcinoma. (b) Prognostic factors of clinical types
The clinical types of oral cancer, which are the superficial, exophytic, and endophytic types, correspond to the macroscopic classification of digestive tract cancers (e.g., esophageal, gastric, and colon cancers [14–16]), namely, type 0, type 1, and type 2–4, respectively. A small number of endophytic oral cancers are reported to be highly malignant, corresponding to type 4 oral cancer. Preliminary investigation of clinical cases at Saitama Cancer Center showed that 5 % of all T1-2 tongue cancers were the scirrhous type exhibiting the characteristic macroscopic features of a small ulcer with broad expansion into the deep tissue layer and with broad hard induration (Fig. 2.5a). In addition to these invasion patterns, such as broad invasion at depth and submucosal lateral infiltration (Fig. 2.5b Left, c), these cancers also exhibited histopathological features corresponding to a Yamamoto-Kohama’s (YK) Mode of Invasion [17] (Fig. 2.5b Right) of YK-4D and a scirrhous pattern, and they were also identified as a subtype with particularly poor prognosis, even among endophytic oral cancers (Fig. 2.5d). To improve the treatment of tongue cancer, further retrospective studies are being conducted to elucidate the pathological features associated with poor prognosis.


(a) Macroscopic presentation of the scirrhous type of lingual carcinoma. Palpation of a small ulcer with broad expansion into the deep tissue layer and extensive induration (outlined in ink). (b) Histologic presentation of the scirrhous type of lingual carcinoma. Left panel: low-magnification image showing a small ulcer on the surface with broad expansion into the deep tissue layer. Right panel: high-magnification image of the opening showing diffuse invasion (YK-4D) of small nests or single cells. (c) Spread pattern of endophytic and scirrhous types of lingual carcinoma. Left panel: broad endophytic ulcer with tapering depth. Right panel: small ulcer with broad expansion in the deep tissue layer and lateral expansion in the submucosal layer. (d) Prognostic factors of the endophytic and scirrhous types of lingual carcinoma
2.2.5 Depth and Deepness of Invasion
-
Depth: Tissue name of the deepest part of cancer invasion. (See tissue names below according to subsite. Underlined tissue names refer to adjacent tissues.)
-
Deepness: Distance from the surface of the assumed normal mucosa to the deepest part of cancer invasion, which is different from the thickness of tumor.
T factors in the UICC classification of oral cancers are determined based on greatest tumor diameter. However, the prognosis of primary tumors correlates with tumor invasion depth much more strongly than with tumor diameter. For this reason, we plan to define the invasion depth of a tumor as the T factor in future studies. Determination of invasion depth is relatively easy in esophageal and gastric cancers because of the six clear layers of the wall: the mucosa (M), muscularis mucosae (MM), submucosa (SM), muscularis propria (MP), subserosa (SS), and serosa (S).
However, in oral cancers, it is not possible to standardize tumor depth because of the complex three-dimensional structure of the oral cavity, which has different deep tissue structures at different anatomical locations. Accordingly, albeit somewhat cumbersome, invasion depth of the vertical structures is recorded in detail from the mucosa to the deeper layers by anatomical site and subsite.
In the present rules, original evaluation criteria were developed for the invasion of adjacent tissues (T4a) by considering evaluation of the depth.
-
(1)
Invasion depth of tongue cancer
Tongue (TON): mucosa (M)/submucosa (SM)/shallow part of the proper muscle layer of the tongue (MP1)/deep part of the proper muscle layer of the tongue (MP2)/extrinsic muscles of the tongue (HG)
Scanning of a healthy tongue with the most widely used US [18–20] device shows three layers of different US intensities and features at the lateral boarder of the tongue, which is the most frequent site of the cancer. These are the outermost, second, and innermost layers of heterogenous hyperechoic or hypoechoic signal intensity (Fig. 2.6a). The outermost hyperechoic layer is thought to represent signal reflection at the mucosal surface, the second hypoechoic layer likely represents mucosa (M), and the innermost layer therefore represents submucosa (SM) and muscularis propria (MP). Because of the hyperechoic signal in the muscularis propria, cancer invading this layer is displayed as an area of hypoechoic intensity (Fig. 2.6b).
Fig. 2.6 

(a) Ultrasonographic findings of normal lingual tissue. (b) Assessment of tumor invasion in the muscular layer and comparison between ultrasonographic and histological images. (c) Assessment of tumor depth
Given the extroverted growth of the tumor and the formation of a depression due to ulcer, it is important to measure the deepness of tumor from the assumed normal mucosal surface, instead of measuring the actual thickness of tumor (Fig. 2.6c). It is also important to record the method of measurement (palpation or US), the extent of tumor invasion in the existing structure, and the depth of invasion in centimeters if palpated or millimeters if scanned by US.
-
(2)
Invasion depth of upper gingival cancer
Upper gingival and alveolus (UG): mucosa (M)/submucosa (SM)/periosteum (PER)/ cortical bone (CB)/bone marrow (CAN)/maxillary sinus (MS) and nasal cavity (NC)
At present, we tentatively use the sinus and nasal floor (SNF) criteria [21, 22] which classify tumor invasion in the maxillary sinus and nasal cavity as T4a.
-
(3)
Invasion depth of lower gingival cancer
Lower gingiva and alveolus (LG): mucosa (M)/submucosa (SM)/periosteum (PER)/cortical bone (CB)/upper part of the mandibular canal in bone marrow (CAN1)/lower part of the mandibular canal in bone marrow (CAN2)
According to the UICC classification, superficial erosion alone of the bone/tooth socket by gingival primary carcinoma is not sufficient to classify a tumor as T4a, and consequently, the diagnosis of any mandibular infiltration beyond this point is crucial. By classifying mandibular infiltration patterns as shown in Fig. 2.7, the JSOT demonstrated the appropriateness of mandibular canal classification that defines CAN2 as T4a in a multicenter study of 1,187 cases of mandibular gingival cancer [23]. The present general rules define CAN2 in mandibular bone invasion as T4a.
Fig. 2.7 
Invasion depth of lower gingival carcinoma
The mandibular invasion of lower gingival cancer is an important indication for surgery. The invasion depth of squamous cell carcinoma (SSC) in the mandible shows a fair correlation with the degree of mandibular resorption on X-ray absorptiometry [9, 12]. By also assessing the pattern of bone resorption, it is possible to determine which resection method is appropriate for the mandible [9, 11–13, 23]. Consequently, in addition to the invasion depth from the gingival mucosa, the images of mandibular resorption by lower gingival cancer should be examined carefully for the following points.
Note: Images of mandibular resorption
In the evaluation of the depth of lower gingival cancer, additional comments concerning the following findings on X-ray studies are attached.
-
(a)
Type of images examined
-
(b)
Degree of mandibular resorption: none/alveolar process of bone marrow/upper mandibular canal of bone marrow/lower mandibular canal of bone marrow
-
(c)
Deepest part of mandibular bone resorption:
Dentulous jaw (Retromolar/8/7/6/5/4/3/2/1/2/3/4/5/6/7/8/R)
Edentulous jaw (Retromolar/ Molar/Premolar/Canine/Incisor/I/C/P/M/R)
-
(d)
Mandibular resorption type: pressure type/mixed type/moth-eaten type
The patterns of bone resorption on radiograms are grouped into the pressure type, moth-eaten type, and mixed type in accordance with the Swearingen classification [9] (Fig. 2.8). It is common to observe all bone resorption patterns distributed continuously on the same radiogram of upper or lower gingival cancer.
Fig. 2.8 
Patterns of bone resorption in lower gingival carcinoma
-
(1)
Pressure type: The margins of bone resorption are clear and smooth with no displaced bone fragments.
-
(2)
Mixed type: Despite somewhat unclear and irregular margins of bone resorption, no displaced bone fragments are observed.
-
(3)
Moth-eaten type: The margins are unclear and irregular, and bone fragments are observed.
In the initial examination of bone resorption, panoramic radiograms may be useful for differential diagnosis of the pressure and moth-eaten types. However, computed tomography (CT) or other imaging modality is necessary to obtain higher detailed imaging findings [24–26].
-
(a)
-
(4)
Invasion depth of buccal mucosal cancer
-
Buccal mucosa (BM): mucosa (M)/submucosa (SM)/buccinator muscle (oral orbicular muscle) (BM, OOM)/buccal sulcus (BS)/buccal fat (BF)/muscles of facial expression and superficial musculoaponeurotic system (SMAS) (FM)/subcutaneous fat (SCF)
-
Anterior type: buccal space→muscles of facial expression and superficial musculoaponeurotic system (SMAS) (FM)/subcutaneous fat (SCF)
-
Posterior type: buccal space→masticator muscle space (MS)
Because of the small number of cases and the complex deep tissue structure, a search of the literature does not produce sufficient information on the clinical and pathological features of buccal mucosal cancer. In the general rules, buccal mucosal cancers are subclassified into the anterior and posterior type on the basis of deep tissue structure. It is important to carefully examine diagnostic images and histopathological samples to accumulate sufficient information on tumor depth in the mucosa, submucosal tissues, buccinator muscle, buccal space, buccal fat pad, muscles of facial expression interlinked via the superficial musculoaponeurotic system (SMAS) [27, 28], subcutaneous fat, skin, masticator space, maxilla, and mandible, as well as information on the invasion of the surrounding tissues.
-
-
(5)
Invasion depth of FOM cancer
-
Floor of mouth (FOM): mucosa (M)/submucosa (SM)/sublingual space (SLS)/mylohyoid muscle (MH)/submandibular space (SMS)
-
Median type: sublingual space→genioglossus muscle (GG)/geniohyoid muscle (GH)/ mylohyoid muscle (MH)/submandibular space (SMS)
-
Lateral type: sublingual space→mylohyoid muscle (MH)/submandibular space (SMS)
Median-type FOM cancers infiltrate into the tissues surrounding the Wharton duct immediately below the mucosa and sublingual gland in the relatively early stages; these cancers infiltrate into the genioglossus (extrinsic tongue muscle) and may further advance into the geniohyoideus and mylohyoideus muscles and the submental space. Lateral-type FOM cancers infiltrate into the mylohyoid and submandibular space vertically via the tissues surrounding the Wharton duct and sublingual gland. In addition, it is important to pay clinical attention to the invasion of the intrinsic muscles of the tongue, the outer periosteum on the mandibular lingual side, and the masticator space.
-
-
(6)
Invasion depth of hard palate cancer
Hard palate (HP): mucosa (M)/submucosa (SM)/periosteum (PER)/cortical bone (CB)/bone marrow (CAN)/maxillary sinus (MS) and nasal cavity (NC)
In general, hard palate cancers located in the posterior region have poor prognosis and a high risk of lymph node metastasis. Prognosis for hard palate cancers invading the nasal cavity and maxillary sinus is thought to be even worse; however, hard palate cancers have not been studied in great detail due to the extremely small number of cases. To reveal their clinical manifestations, it is necessary to carefully investigate their invasion depth into surrounding tissues, including the nasal cavity and maxillary sinus. At present, we tentatively use the SNF criteria [21, 22], which classify tumor invasion in the maxillary sinus and nasal cavity as T4a.




2.2.6 Invasion into Adjacent Structures
In principle, the UICC TNM classification of malignant tumors [3] is used to assess the infiltration of primary lesions, except T4a lesions, into surrounding tissues. For T4a lesions, we propose our own classification criteria specific to the site of invasion, as described below. In the following section, we review the association between T factors and the UICC classification.
-
(1)
Invasion into adjacent tissues by tongue cancer
None/FOM/sublingual space/mylohyoid muscle/extrinsic muscles of the tongue/root of the tongue/gingiva/mandibular cortex/mandibular bone marrow
The tongue consists of four extrinsic muscles (genioglossus, hyoglossus, styloglossus, and palatoglossus) and four intrinsic muscles (superior longitudinal, inferior longitudinal, verticalis, and transversus muscles). Infiltration into the intrinsic muscles is used as an indication of deep tissue invasion in T4a tumors. Infiltration into individual intrinsic muscles is not regarded as an indication of T4a tumors. The intrinsic muscles move the tongue, whereas the extrinsic muscles change its shape during swallowing and speech. For example, the genioglossus muscle moves the tongue anteriorly or toward the mentum, whereas the hyoglossus pulls the root of the tongue posteriorly. In addition, the styloglossus pulls the tongue toward the upper posterior direction, and the palatoglossus plays a role in narrowing the faucial area by elevating the root of tongue and lowering the palate. The lingual and hypoglossal nerves serve to regulate the tongue’s sensory and motor functions, respectively. The extent of invasion is diagnosed while taking account of the function of individual muscles and nerves as well as the current symptoms. With regard to bone metastasis, infiltration into bone marrow is clearly an indication of T4a. In addition, as in the other oral cancers, the diagnosis of T4a is made when the submandibular space is infiltrated via the mylohyoid muscle. Invasion into the skin, which also appears in the UICC classification criteria, occurs only through the mandible or submandibular space and therefore is excluded from the criteria for T4a lesions in these general rules. T4b is also diagnosed upon tumor invasion into the posteriorly located masticator space. The UICC T4b criteria are used for infiltration into the internal carotid artery and pterygoid process, both of which rarely occur without the invasion of the masticator space.
-
(2)
Invasion of adjacent tissues by upper gingival cancer
None/maxillary sinus/nasal cavity/buccinator muscles/buccal space/muscles of facial expression/masticator space/pterygoid plate/skull base/internal carotid artery/subcutaneous fat/skin
Figure 2.9 shows the potential infiltration routes of upper gingival and hard palate cancers into the surrounding tissues in the coronal section. In these general rules, infiltration into surrounding tissues beyond the buccinator muscle is classed as T4a in upper and in lower gingival cancer. Because the orbicularis oris muscle and buccinator muscles are adjacent to each other, any tumor invasion beyond the orbicularis oris muscle is diagnosed as T4a as well. In contrast to the UICC classification for lower gingival cancer, which defines T4a by bone marrow infiltration, we define tumor invasion reaching the mandibular canal as T4a. However, compared with the mandible, the bone cortex of the maxilla is thin and thus readily allows tumor invasion into the bone marrow. Accordingly, the invasion of the nasal cavity or maxillary sinus, but not the bone marrow, is also defined as T4a for upper gingival cancers in accordance with the SNF criteria (Fig. 2.10). Infiltration into the skin, which is described in the UICC classification, occurs only through the buccinator muscle and therefore is excluded from the T4a criteria in these general rules. As described earlier, anterior and posterior infiltration into the buccal space and subcutaneous fat is considered to be T4a. However, as described in the section on buccal mucosal cancer, none of the infiltration routes in the horizontal direction (Fig. 2.11) are considered T4b (the routes in Figs. 2.9a and 2.11a). The most important factor that affects prognosis is tumor invasion in a posterior direction. Because infiltration into the medial and lateral pterygoid muscles, masseter muscle, and temporal muscle is invasion of the muscles of mastication (the routes in Fig. 2.11c–e) and because of the potential invasion of the pterygoid process (the route in Fig. 2.11b), infiltration into these muscles is defined as T4b in accordance with the UICC classification.
Fig. 2.9 
Invasion routes of upper gingival and hard palate carcinomas on a coronal section
Fig. 2.10 
Maxillary invasion of upper gingival carcinoma according to the sinus and nasal floor criteria. (a) The carcinoma advancing through and expansively absorbing the bone marrow on the buccal side is not classified as T4a because of no infiltration into the maxillary sinus. (b) The carcinoma infiltrating the maxillary sinus through the bone is classified as T4a
Fig. 2.11 
Invasion routes of upper gingival carcinoma in the horizontal section
-
(3)
Invasion of adjacent tissues by lower gingival cancer
None/FOM/sublingual space/tongue/buccal mucosa/buccinator muscles/buccal space/ masticator space/muscles of facial expression/subcutaneous fat/skin
The progression of lower gingival cancer toward the buccal mucosa may lead to tumor infiltration into the buccinator muscle, buccal space, and even the skin (Fig. 2.12a). In the direction of the FOM, lower gingival cancer may infiltrate superficially into the lingual gingiva, FOM mucosa, and even the tongue (Fig. 2.12b) and infiltrate deeply into the sublingual gland, Wharton duct, lingual nerve, and as far as the submandibular space via the mylohyoid muscle (Fig. 2.12c). The progression of lower gingival cancer toward the retromolar areas may cause invasion of the submandibular space via the posterior edge of the mylohyoid muscle medially (Fig. 2.12d), invasion of the masseter muscle via the buccinator muscle laterally (Fig. 2.12e), and invasion of the base of the skull and the parapharyngeal space via the pterygomandibular space posteriorly (Fig. 2.12f). In the JSOT general rules, tumor infiltration reaching the mandibular canal via the deep interior region of the mandible is defined as T4a. Invasion of the adjacent tissues that are defined as T4a includes the extrinsic muscles of the tongue on the FOM side, the submandibular space, and the skin, buccal space, and even subcutaneous fat on the buccal mucosal side. The problem associated with the UICC criteria of T4b for lower gingival cancers is the invasion of the masticator space because lower gingival cancers originating from the retromolar areas readily invade the masticator space (Fig. 2.13).
Fig. 2.12 
Invasion routes of lower gingival carcinoma
Fig. 2.13 
Masticatory space and pterygomandibular space
-
(4)
Invasion of adjacent tissues by buccal mucosal cancer
None/masticator space/lower gingiva/mandibular cortex/mandibular bone marrow/FOM/upper gingiva/maxillary cortex/maxillary bone marrow/ oropharynx/lips/subcutaneous fat/skin
The major invasion routes of FOM cancers into the adjacent tissues and the relationship between the routes and fascial spaces are shown in Fig. 2.14. In the upper and lower gingival cancer section of the JSOP general rules, the invasion of buccal space or subcutaneous fat is defined as T4a. However, it can be problematic to apply this definition as is because buccal mucosal cancers easily invade the buccal space. Figure 2.15 therefore shows the different degrees of invasion of buccal mucosal cancers in the coronal plane. The buccal space is present between the buccinator muscle and the SMAS muscles for facial expression and contains the buccal fat pad with a distinctive coating. Although invasion into the skin is defined as T4a in the UICC classification, the JSOT general rules define invasion of the subcutaneous fat via the buccal space or via the orbicularis oris muscle which lacks the buccal space as T4a. On the other hand, the invasion of the maxilla and mandible (Fig. 2.15f1, f2) is defined as T4a only when accompanied by bone marrow invasion, in accordance with the UICC classification. The posterior type of buccal mucosal cancer may bypass the buccal space and posteriorly invade the masseter muscle, i.e., the masticator space (the route in Fig. 2.14b). In this case, the invasion is defined as T4b in accordance with the UICC classification.
Fig. 2.14 
Invasion routes of buccal mucosal and floor of mouth (FOM) carcinoma and fascial spaces
Fig. 2.15 
Depth of buccal carcinoma on a coronal section
-
(5)
Invasion of adjacent tissues by FOM cancer
None/mylohyoid muscle/tongue/extrinsic muscles of the tongue /gingiva/mandibular cortex/mandibular bone marrow/submandibular space/masticator space/oropharynx
The invasion routes of FOM cancers in the coronal plane may involve the sublingual gland (a), intrinsic tongue muscles (b), extrinsic tongue muscles (c), mylohyoid muscle (d), and mandible (e), as shown in Fig. 2.16. Non-superficial lesions generally involve tumor invasion into the sublingual gland and rarely infiltration into the mandible or the submandibular space beyond the mylohyoid muscle. However, with regard to the progression of lateral FOM cancers in the posterior direction, attention must be paid to the invasion of the submandibular space via the posterior margin of the mylohyoid muscle and the invasion of the medial pterygoid muscle. The T4a definitions of FOM cancers conform to the corresponding UICC criteria, and accordingly, FOM cancers are defined as T4a when accompanied by the invasion of the extrinsic tongue muscles and mandibular bone marrow and the invasion of the submandibular space by coming around the posterior margin of the mylohyoid muscle (the route in Fig. 2.14d) or by passing over the mylohyoid muscle (the route in Fig. 2.14c). Invasion into the skin is excluded from the UICC T4a criteria because it is possible only via the mandible or submandibular space. Invasion of the medial pterygoid muscle is defined as T4b in accordance with the UICC classification because the invasion is equivalent to the invasion of the masticator space (the route in Fig. 2.14f).
Fig. 2.16 
Invasion routes of FOM carcinoma on a coronal section
-
(6)
Invasion of adjacent tissues by hard palate cancer
None/maxillary sinus/nasal cavity/gingiva/soft palate/masticator space/ pterygoid plate/skull base/internal carotid artery
The potential invasion routes of upper gingival and hard palate cancers in the coronal plane are shown in Fig. 2.9. Although hard palate cancers may invade posteriorly into the soft palate, pterygoid process, and medial pterygoid muscle (masticator space), invasion of the soft palate is not included in the UICC T4 criteria. On the other hand, despite the contiguous mucosal structure, invasion of soft palate cancer (oropharyngeal cancer) into the hard palate is considered to be T4a according to the UICC criteria. To ensure consistency among the criteria, it may be necessary to define the invasion of hard palate cancer into the soft palate as T4a. However, define such simple invasion of contiguous anatomical regions as T4a independently of the depth is questionable. We will therefore continue to investigate the prognosis of soft palate cancer accompanied by invasion of the hard palate.
Note: Description of the superficial muscular aponeurotic system (SMAS)
In 1976, Mitz et al. reported the presence of the SMAS [27], which is connected to the platysma muscle, muscles of facial expression, temporoparietal fascia, and galea aponeurotica [28]. The SMAS is an important anatomical structure in cosmetic surgery, especially rhytidectomy, because the system stabilizes facial expression and transmits contraction signals to the facial skin. Compared with the adipose tissue medial to the SMAS, the adipose tissue lateral to it (i.e., toward the skin) contains small adipocytes partitioned by fibrous tissues that transmit muscular movement to the skin. The SMAS is wide at the para-parotid gland area but becomes thinner and discontinuous anteriorly. As indicated by the arrow in the coronal section of the masseter muscle stained with hematoxylin and eosin of Fig. 2.17, the SMAS is contiguous to the platysma muscle and forms a thin layer of muscle or a layer of connective tissue outside the masseter muscle.
Fig. 2.17 
Histologic figure at the masseter muscle on a coronal section









2.2.7 T Score
The assessment of T score in primary tumors, except T4a tumors, is performed in accordance with the UICC TNM malignant tumor criteria [3].
-
TX: Primary tumor cannot be assessed
-
T0: No evidence of primary tumor
-
Tis: Carcinoma in situ (squamous intraepithelial neoplasia)
-
T1: Maximum diameter ≤2 cm
-
T2: Maximum diameter >2 and ≤4 cm
-
T3: Maximum diameter >4 cm
-
T4: Invasion into adjacent structures
However, as stated earlier, the criteria for T4a lesions were developed by invasion sites, and therefore we summarize the differences between our general rules and the UICC classification below.
In addition, tumors 2–3 and 3–4 cm in the greatest diameter are occasionally called early T2 and late (or advanced) T2, respectively. This appears to be an effective subclassification for:
<Comparative relations to the UICC T4a criteria>
-
(1)
Tongue cancer:
T4a: Invasion into the mandibular bone marrow, invasion into the submandibular space, and invasion into the extrinsic tongue muscles
T4b: Invasion into the masticator space, invasion into the pterygoid plate, invasion into the skull base, and invasion circumferentially surrounding the internal carotid artery
-
Addition of “invasion into the submandibular space”
-
Omission of “invasion into the skin” in the UICC classification because it does not occur without the invasion of the mandible or submandibular space
-
Deletion of “invasion into the maxillary sinus” in the UICC classification
-
Retention of “invasion into the mandibular bone marrow” and “invasion into the extrinsic tongue muscles” in the UICC classification
-
-
(2)
Upper gingival cancer:
T4a: Invasion into the maxillary sinus and nasal cavity and invasion into the buccal space or subcutaneous fat
T4b: Invasion into the masticator space, invasion into the pterygoid plate, invasion into the skull base, and invasion circumferentially surrounding the internal carotid artery
Note 1: If the tumor is confined to the alveolar bone, the tumor is classified as T1-3 according to its size.
Note 2: Tumors invading the maxillary sinus are judged to be T4a regardless of their size.
-
Omission of “invasion of the bone marrow” and change of “invasion of the maxillary sinus” in the UICC classification to “invasion of the maxillary sinus and nasal cavity”
-
Change of “invasion of the skin” in the UICC classification to “invasion of the buccal space or subcutaneous fat”
-
Omission of “invasion of the extrinsic tongue muscles” in the UICC classification
-
-
(3)
Lower gingival cancer:
T4a: Invasion reaching the mandibular canal, invasion into the buccal space or subcutaneous fat, invasion into the submandibular space, and invasion into the extrinsic tongue muscles
T4b: Invasion into the masticator space, invasion into the pterygoid plate, invasion into the skull base, and invasion circumferentially surrounding the internal carotid artery
Note 1: If the tumor is confined to the upper part of the mandibular canal in the bone marrow, the tumor is classified as T1-3 according to its size.
Note 2: Tumors invading the mandibular canal are judged to be T4a regardless of their size.
-
Addition of “invasion of the submandibular space”
-
Change of “invasion of the skin” in the UICC classification to “invasion of the buccal space or subcutaneous fat”
-
Change of “invasion of the bone marrow” in the UICC classification to “invasion reaching the mandibular canal”
-
Omission of “invasion of the maxillary sinus” in the UICC classification
-
Retention of “invasion of the extrinsic tongue muscles” in the UICC classification”
-
-
(4)
Buccal mucosal cancer:
T4a: Invasion into the subcutaneous fat, invasion into the maxillary and mandibular bone marrow, and invasion into the maxillary sinus
T4b: Invasion into the masticator space, invasion into the pterygoid plate, invasion into the skull base, and invasion circumferentially surrounding the internal carotid artery
-
Change of “invasion of the skin” in the UICC classification to “invasion of the subcutaneous fat”
-
Retention of “invasion of the mandibular bone marrow” and “invasion of the maxillary sinus” in the UICC classification
-
Omission of “invasion of the extrinsic tongue muscles” in the UICC classification
-
-
(5)
FOM cancer:
T4a: Invasion into the mandibular bone marrow, invasion into the submandibular space, and invasion into the extrinsic tongue muscles
T4b: Invasion into the masticator space, invasion into the pterygoid plate, invasion into the skull base, and invasion circumferentially surrounding the internal carotid artery
-
Addition of “invasion of the submandibular space”
-
Omission of “invasion of the skin” in the UICC classification because it does not occur without the invasion of the mandible or submandibular space
-
Omission of “invasion of the maxillary sinus” in the UICC classification
-
Retention of “invasion of the mandibular bone marrow” and “invasion of the extrinsic muscles of the tongue” in the UICC classification
-
-
(6)
Hard palate cancer:
T4a: Invasion into the maxillary sinus and nasal cavity
T4b: Invasion into the masticatory muscle space, invasion into the pterygoid process, invasion into the base of the skull, and invasion circumferentially surrounding the internal carotid artery
-
Addition of “nasal cavity” into “invasion of the maxillary sinus” in the UICC classification while omitting “invasion of the mandibular bone marrow”
-
Change of “invasion of the skin” in the UICC classification to “invasion of the buccal space or subcutaneous fat”
-
Omission of “invasion of the extrinsic tongue muscles” in the UICC classification
-
2.2.8 Histological Classification
2.2.8.1 Tis Cancer: Oral Intraepithelial Neoplasia (OIN)/Carcinoma In Situ
-
(1)
Basaloid type
-
(2)
Differentiated type
The histological classification of early oral SCC has been performed universally in accordance with WHO’s classification of “dysplasia” [29–31], which grades the severity of dysplasia as mild, moderate, or severe and defines carcinoma in situ (CIS) as a precursor to oral SCC. The definition of CIS as the presence of atypical cells in all layers of the epithelium has remained unchanged since the first edition (1971). However, this diagnostic criterion is controversial because the criterion was established by emulating the pathological concept of dysplasia in cervical cancer [32–34] and because differentiated precancerous lesions and CIS are typically present in the mucosa of the oral cavity, pharynx, and larynx [35–41]. Against this background, when the classification of squamous intraepithelial neoplasia (SIN) [39–42] and the Ljubljana classification of laryngeal lesions [43–54] were proposed, WHO included these classifications alongside the criteria for dysplasia in head and neck tumors (2005) [31]. Nevertheless, in the WHO classification, the pathologic concept of dysplasia and SIN includes both neoplastic lesion and atypical reactive lesion. This concept is not only incomplete for pathological classification but also useless as a diagnostic indicator for deciding the treatment strategy. Furthermore, it remains a descriptive diagnosis and cannot be used to qualitatively diagnose tumor malignancy.
Although the WHO classification has been conventionally used in Japan, recent developments in oral oncology have promoted certain modifications in the diagnosis of early cancerous lesions in the oral cavity. After conducting its own investigation of precancerous lesions, in 2005 the Working Group of the JSOT proposed the differentiated type of CIS [5, 35]. In 2007, the other group of the Japan Society for Oral Pathology published an Oral CIS Catalog which contained histopathological variations including a histological image of differentiated CIS [36, 37]. These studies revealed the existence of an oral type of Tis SCC derived from atypical squamous epithelial lesions distinct from “full thickness or almost full thickness architectural abnormalities,” one of the diagnostic criteria for CIS in the WHO classification. Differentiated type is a type of CIS that becomes cancerous while maintaining the maturation and differentiation of stratified squamous epithelium and accounts for the majority of oral CIS [1, 35–37]. Therefore, the dysplasia-carcinoma sequence theory, which was established for cervical cancer and classifies atypical cells into mild, moderate, and severe dysplasia based on the involvement of 3 epithelial layers before turning into CIS, should not be used to define precancerous lesions in oral cancer. Because of the difficulty in diagnosing cellular atypia in the stratum corneum or superficial layer using this criterion based on three layers, it is highly possible to underdiagnose moderate dysplasia [31, 55, 56]. For diagnosing CIS in oral mucosa, cytologic atypia is more important than the classification based on layers. It is important to remember that in histological examination, many CIS in the oral mucosa are highly differentiated, unlike cervical and esophageal cancers. Against this background, the first edition of the General Rules for Clinical and Pathological Studies on Oral Cancer published in 2010 [1, 2] clearly states the concept of oral intraepithelial neoplasia (OIN), which takes the place of CIS. OIN was used to avoid confusion with CIS in WHO’s diagnostic criteria and to define a pathological feature specific to oral cancer. Although histological examination shows the basaloid type and differentiated type, OIN often reveals a transition between the two.
-
(1)
The basaloid type of OIN/CIS corresponds to CIS in the WHO classification, and the histological images of OIN show basal-like cells in all or almost all layers (Fig. 2.18). Although in reality it is rare to observe this type of OIN in the oral cavity, when present, macroscopic observation reveals an erosive erythroid lesion, which rapidly progresses to invasive carcinoma within 6 months.
Fig. 2.18 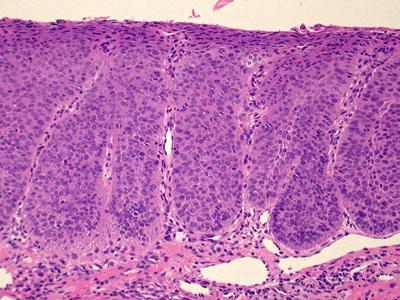
Basaloid type of oral intraepithelial neoplasia/carcinoma in situ (OIN/CIS)
-
(2)
The differentiated type of OIN/CIS is specific to the oral type of intraepithelial neoplasia and shows highly atypical cells in the basal layer, but not in the stratum corneum or stratum spinosum. It is histopathologically important to pay attention to atypical cells in the first layer of the stratum basale and to examine for irregularities in the size and shape of the nucleus, the ratio of the nucleus to the cytoplasm, prominent nucleolus, mitotic features, and the disturbance and loss of polarity (Fig. 2.19). Because oncogenic transformation occurs while maintaining the maturation and differentiation characteristics of the stratified squamous epithelium, it is often difficult to recognize structural atypia in this type of OIN. However, the diagnosis of intraepithelial neoplasia can be made based on the specific pathological features of CIS, including the formation of a tumor front between the lesion and adjacent mucosal epithelium and the establishment of other aspects of CIS, after multilayer formation and lateral expansion of atypical cells. Most OIN in the oral cavity are the differentiated type or the mixed type of CIS. These OIN have white lesions and progress to invasive carcinoma within 5 years.
Fig. 2.19 
Differentiated type of OIN/CIS
-
(a)
Molecular markers
Although it is difficult to differentiate OIN, especially the differentiated type of OIN, from oral epithelial dysplasia (see below) and reactive atypical epithelium, many studies have reported the utility of morphological diagnostic criteria and immunostaining with Ki-67, cytokeratin 13, and cytokeratin 17 [1, 35, 37, 57–73]. However, immunostaining findings should be supplementary to histopathological findings because the gene expression mechanism of cytokeratin with a molecular weight different from that of the common type of cytokeratin has not been elucidated. Here, we introduce several useful immunostaining findings.
-
(1)
Ki-67/MIB1 (Fig. 2.20)
Fig. 2.20 
Immunohistochemistry for Ki-67/MIB1 of OIN. (a) OIN, differentiated type. (b) OIN, basaloid type. (c) Large immunoreactive atypical cells in the first basal layer. (d) Immunoreactive cells across several layers
-
# Cell-cycle cells are immunoreactive for Ki-67/MIB1. In healthy oral mucosa, cells positive for Ki-67/MIB1 are scattered in the second basal layer.
-
# Ki-67/MIB1 immunoreactive cells with a large nucleus and prominent nucleolus are observed in the stratum basale of OIN.
-
# Multilayer Ki-67/MIB1 immunoreactive cells are observed throughout the parabasal and spinous layers of OIN.
-
-
(2)
Cytokeratins 13 and 17 (Fig. 2.21)
Fig. 2.21 
Immunohistochemistry for cytokeratin 13 and 17 of OIN. (a) OIN, arrow shows the front line. (b, c) Immunohistochemistry for ki-67/MIB1 (b), cytokeratin 13 (c), and cytokeratin 17 (d)
-
# In the oral cavity, healthy mucosal cells are negative, while OIN are positive for CK13 immunoreactivity.
-
# OIN, but not healthy mucosal cells, is immunoreactive for CK17.
-
# The above changes are sometimes observed in reactive atypical lesions.
-
A number of gene expression and immunohistochemical studies indicate that transglutaminase 3, a squamous differentiated marker, is useful for the diagnosis of OIN [71, 72, 74], although further examination is required to substantiate these findings. It is anticipated that an increase in the number of useful molecular markers available will improve the objectivity of diagnosis. The justification for diagnosis on which the OIN classification as well as the other classifications relies is based on findings from retrospective studies, and there have been only a few prospective studies that have examined the description of oncogenesis at the molecular level. It is well known that genomic instability due to telomere shortening plays an important role in carcinoma development. Telomere shortening is the initial phenomenon in cancerization, and genomic instability is accelerated by the chromosomal instability that results from such shortening [75, 76]. It has been reported that mean telomere length was significantly shorter in OIN cases diagnosed histopathologically than in normal mucosal epithelium [77].
-
(1)
-
(b)
Relations with other classification methods
Table 2.1 shows the comparative relations among different classification methods [35]. Although a one-to-one comparison is not made here because the methods used different diagnostic criteria, this table shows their comparative relationships conceptually. It has long been known that some cases of mild to moderate dysplasia diagnosed according to the WHO classification develop into invasive cancer later on. We believe such cases actually involve superficial and differentiated intraepithelial neoplasia.
Table 2.1 Schemas for histologically categorizing precursor CIS and related lesions Note: Oral epithelial dysplasia (OED)
Atypical epithelium is divided into two pathological entities, one with progression to cancer (true preinvasive SCC, OIN/CIS) and the other without (reactive atypical epithelium). However, as it is difficult in practice to distinguish between these clearly at present, the term “OED” is used to denote a borderline lesion that is difficult to differentiate from reactive atypical epithelium, although OIN/CIS may be suspected. These cases require 5 years or more of long-term follow-up [1]. Although dysplasia in the esophagus is defined as an intraepithelial neoplastic lesion [78], in the oral mucosa located in front of Waldeyer’s tonsillar ring, the differential diagnosis of neoplastic lesion and reactive atypical epithelium is frequently difficult to make. Therefore, practically speaking, the application of this boundary classification to the oral mucosa is useful [1].
Note: Lugol (iodine) staining
It is very difficult to detect OIN/CIS on macroscopic examination. Generally, OIN/CIS is composed of flat or slight elevated white or erosive red lesions, or an admixture of focal white and red ones. It can be detected as an unstained area by Lugol’s (iodine) staining [1, 79–81] (Fig. 2.22). Since superficial layers of the normal squamous mucosa are rich in glycogen, any lesions with a loss of superficial glycogen, such as reactive atypical epithelium, oral epithelial dysplasia, oral intraepithelial neoplasia, or early invasive squamous cell carcinoma (Fig. 2.23), can be recognized as unstained areas [1, 5–8]. However, in hyperkeratinized mucosa, especially in the gingiva and palate, Lugol may not show a clear unstained area or may instead show a lightly stained area [1]. Although further classification of any iodine-free areas is necessary, in principle it is desirable to resect an iodine-free area in the vicinity of cancer as much as possible.
Fig. 2.22 
Lugol’s (iodine) staining of OIN. (a) Macroscopic presentation of early invasive cancer located posterior to OIN and appearing white. (b) Lugol’s (iodine) staining showing lightly stained early invasive cancer located posterior to the OIN and appearing as an unstained area
Fig. 2.23 
Histological varieties of Lugol-free oral mucosa. (a) Reactive atypical epithelium. (b) Oral epithelial dysplasia. (c) Oral intraepithelial neoplasia. (d) Early invasive squamous cell carcinoma
-
(a)






2.2.8.2 Squamous Cell Carcinoma, Common Type
-
(1)
Histological Grade (WHO) (Fig. 2.24):
Fig. 2.24 
World Health Organization histological grade of SCC
-
Grade 1: Well-differentiated type
-
Grade 2: Moderately differentiated type
-
Grade 3: Poorly differentiated type
Histological grading is a useful indicator for the degree of malignancy in SCC. The WHO grading system [29, 30], which was derived from the Broders’ classification for lip cancer (1920) [82] and classifies oral SCC into well-, moderately, and poorly differentiated tumors based on the degree of cell differentiation, has been the most widely used method worldwide. The method is still used routinely at many institutions because of its moderate correlation with prognosis and lymph node metastasis reported by a large-population study.
However, the WHO grading system is not particularly useful for determining treatment options in individual cases, and consequently various malignancy grading systems have been proposed including the Jakobsson classification (1973) [83], Willen classification [84], and Anneroth classification [85, 86]. These grading systems evaluate factors related to tumor–host interactions as well as tumor-related factors to diagnose the degree of malignancy, by scoring 6–8 factors at the tumor–host junction and calculating the total score. Despite their proven efficacy in many studies, these systems are not widely used because of their complexity.
In Japan, Imai conducted a study on tumor growth by focusing on tumor–host interactions and compared SCC in the oral cavity, larynx, and uterine cervix with adenocarcinoma in the stomach and breast (1954) [87]. The author classified tumors into elongation, hypertrophic, and budding growth types based on the morphology of the tumor margin and reported that the budding-type tumors had the worst prognosis. The author defines budding-type tumors as small tumor nests containing approximately 2–3 tumor cells on average or free tumors growing individually.
-
-
(2)
Mode of Invasion/YK classification (Fig. 2.25):
Fig. 2.25 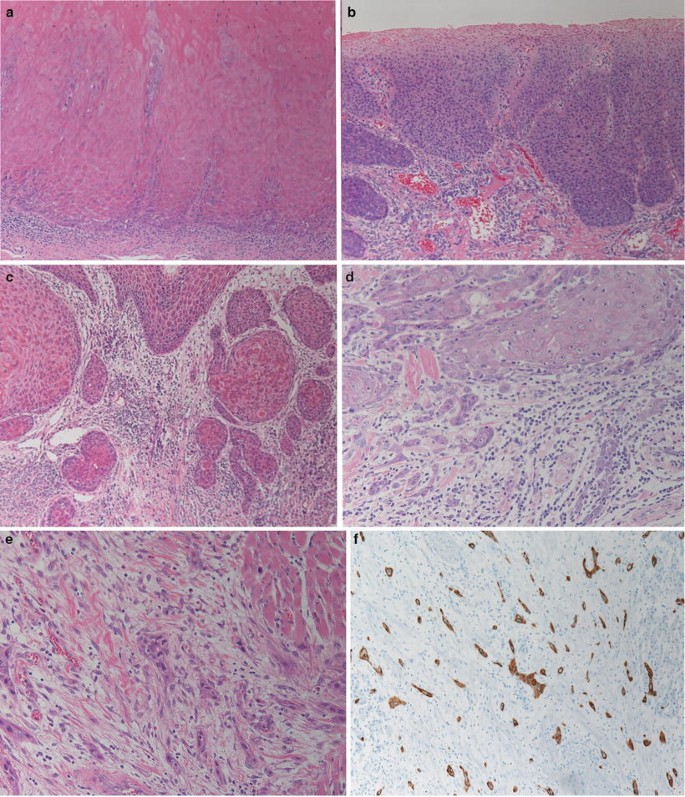
YK-classification histologic figures. (a) YK-1, (b) YK-2, (c) YK-3, (d) YK-4C, (e) YK-4D, (f) YK-4D, immunohistochemistry for cytokeratin
-
YK-1: Well-defined borderline
-
YK-2: Cords, less-marked borderline
-
YK-3: Groups of cells, no distinct borderline
-
YK-4C: Diffuse invasion, cord-like type invasion
-
YK-4D: Diffuse invasion, diffuse-type invasion
After reporting that invasion characteristics are the most important indicator of malignancy among the histopathological factors used in the Jakobsson classification [83], Yamamoto systematically continued his study for many years before eventually elucidating their biological property [17, 88]. In Japan, a relatively large number of oral surgery clinics use tumor classification based on the patterns of tumor invasion, namely the YK Mode of Invasion that focuses on invasion patterns at tumor–host junctions and correlates highly with lymph node metastasis [89] and prognosis compared with the WHO grading system. The YK Mode of Invasion is also compatible with infiltrative growth patterns (INF: INFa, INFb, and INFc) observed in gastrointestinal cancer (esophageal, gastric, and colorectal cancers) [14–16], showing that YK-1, YK-2, YK-3, and YK-4C/4D correspond to oral cancer-specific well-differentiated SCC, INFa, INFb, and INFc, respectively. Although rare, YK-4D is highly malignant and possesses a specific biological property accompanied by desmoplastic reaction [89].
-
-
(3)
Mode of mandibular invasion (Figs. 2.26, 2.27, 2.28, and 2.29):
Fig. 2.26 
Schemas for mode of mandibular invasion. Left panel: the expansive type of carcinoma has a well-defined borderline. Right panel: the invasive type of carcinoma has a diffuse irregular margin
Fig. 2.27 
Mode of mandibular invasion showing an image obtained using a magnifying glass. Left panel: expansive type of lower gingival carcinoma infiltrating the mandibular canal. Right panel: invasive type of lower gingival carcinoma infiltrating the mandibular canal
Fig. 2.28 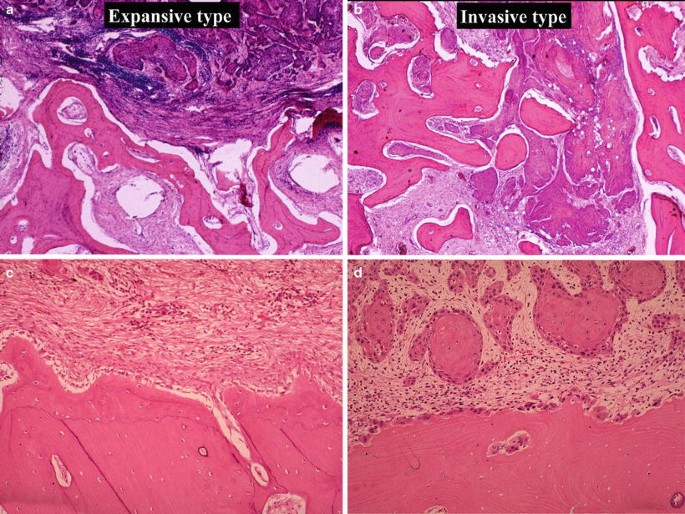
Mode of mandibular invasion showing histologic presentation. (a) Expansive type carcinoma having a well-defined margin. (b) Invasive type carcinoma having diffuse irregular margins. (c) Reversal line seen on the bone surface, indicating that the bone is in the remodeling phase. (d) Howship’s lacunae accompanied by a large number of osteoclasts, indicating that the bone is in the resorption phase
Fig. 2.29 
Mode of mandibular invasion on scanning electron microscopy. Left panel: shallow Howship’s lacunae accompanied by remineralization. Right panel: deep Howship’s lacunae with many bone canaliculi at the bottom
Expansive type/invasive type
The malignancy of mandibular gingival cancer may be graded using the patterns of mandibular invasion [10, 12]. According to the mode of mandibular invasion, lower gingival carcinomas are histologically classified into two groups: invasive type and expansive type. The invasive type has a diffuse irregular margin, while the expansive type has a well-defined borderline. The pathological changes during bone resorption are comparable in both types of carcinoma. Histologically, in the invasive type, a large number of Howship’s lacunae are observed in the resorption phase. In the expansive type, Howship’s lacunae are relatively marked by reversal lines in the formation phase. Scanning electron microscopy of the invasive type has shown marked destruction of the bone surface with Howship’s lacunae in the resorption phase, whereas scanning electron microscopy in the expansive type of carcinoma has shown a smooth bone surface with Howship’s lacunae in the formation phase.
The utility of mandibular invasion patterns in determining tumor malignancy was investigated in a previous study examining 102 cases (1975–1990) [10, 12] and our multi-institutional study of 524 cases (1992–2005) [7] (Fig. 2.30). In both studies, a significant difference was observed in prognosis, but not lymph node metastasis, between the expansive and invasive types, indicating that the use of mandibular invasion patterns is an effective grading system that reflects the activity of local invasion. Furthermore, because of the correlation with imaging findings of bone resorption, this grading system may be regarded as a clinical classification method, as in the classification based on invasion patterns.
Fig. 2.30 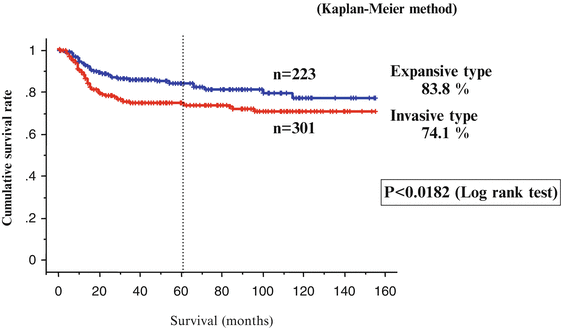
Mode of mandibular invasion and prognosis
Note: Correlation between mode of mandibular invasion and image classification of bone resorption
Because radiographic findings of bone resorption simply reflect bone resorption caused by tumor invasion, they may not necessarily reflect the front line of bone invasion histopathologically. Yet, there is a certain correlation between the types of bone resorption and the patterns of bone invasion in SCC. A previous study comparing imaging findings of a surgical specimen using soft X-ray with histopathological findings revealed that the radiographic images of SCC of the mandibular gingiva show two types of bone resorption which reflect tumor invasion patterns. The two types of bone resorption correspond to the pressure and moth-eaten types in the conventional Swearingen classification [9], where the lesions with relatively uniform X-ray transmission and with clear and smooth bone resorption margins are defined as the pressure type and where lesions with uneven transmission due to diffused moth-eaten patterns are defined as the moth-eaten type (Fig. 2.31). The pressure and moth-eaten types correspond to the expansive and invasive types described in the previous section, with a significant correlation between the patterns of mandibular invasion and bone resorption and with a diagnostic accuracy of 76 % [10]. However, it is often difficult to classify actual clinical images into either type; consequently, the mixed type was introduced into the present general rules as the third bone resorption pattern. The clinical approach of this mixed type is similar to that of the moth-eaten type.
Fig. 2.31 
Soft X-ray image of a surgical specimen of mandibular gingival squamous cell carcinoma. Upper panel: expansive type of lower gingival carcinoma. Lower panel: invasive type of lower gingival carcinoma
The diagnostic accuracy of bone resorption is affected by images used for the assessment, as shown by a study comparing the histological patterns of bone invasion with the patterns of bone resorption on panoramic X-ray images and CT images. Both types of image were statistically significantly correlated with bone invasion patterns; however, the correlation differed by pattern, and a greater correlation was observed between prognosis and bone resorption diagnosed by CT. Moreover, because a simple radiographic image compresses an entire visual plane, there is a chance of misdiagnosing the type of bone resorption, as an area of bone resorption could overlap with healthy trabecular bone located outside of the zone of tumor invasion. It is therefore necessary to incorporate the most advanced imaging technology to make clinically a significant diagnosis of bone resorption.
-
(4)
Route of intramandibular development:
-
Development through the periodontal membrane (+/-)
-
Development in the mandibular canal (+/-)
It should be noted that tumor invasion in the mandibular soft tissue is not displayed as bone resorption on radiographic images. When assessing the range of tumor invasion, potential tumor invasion routes to consider are the periodontal ligament space and mandibular canal. Regardless of bone invasion patterns, the periodontal ligament space is the invasion route for early-stage cancers in the dentulous mandible (Fig. 2.32a). In contrast, tumor progression to the mandibular canal is observed only in the invasive type of pT4 cancers (Fig. 2.32b).
Fig. 2.32 
Routes of intramandibular spread. (a) Developmental route through the periodontal membrane. (b) Developmental route in the mandibular canal
-









2.2.8.3 Squamous Cell Carcinoma, Variants
-
(1)
Verrucous carcinoma (Fig. 2.33a)
Fig. 2.33 
Histological variants of squamous cell carcinoma. (a) Verrucous carcinoma, (b) basaloid squamous cell carcinoma, (c) adenoid squamous cell carcinoma, (d) spindle cell carcinoma, (e) adenosquamous carcinoma, (f) papillary squamous cell carcinoma
This is a high-grade carcinoma that exhibits prominent exophytic growth of well-differentiated keratinized stratified squamous epithelium and locally destructive expansive subepithelial growth. It is difficult to diagnose this carcinoma when biopsy findings lack clear images of expansive growth into the subepithelial tissues. Although metastasis is an extremely rare clinical occurrence, attention must be paid to the fact that approximately 20 % of verrucous carcinoma cases are accompanied by typical SCC.
-
(2)
Basaloid squamous cell carcinoma (Fig. 2.33b)
This is a highly malignant carcinoma that resembles the basal cells and is accompanied in part by clearly differentiated SCC. Basaloid SCC cells are either solid or arranged in cords, and a palisade arrangement of tumor cells is often observed in the vicinity of tumor nests, while coagulative necrosis of tumor nests and an expanding cystic cavity are observed in the central area.
-
(3)
Adenoid squamous cell carcinoma (Fig. 2.33c)
This SCC presents with histological findings of adenosquamous carcinoma due to false spaces and ducts on diagnostic images caused by the liquefactive necrosis of the nests. No epithelial mucus is present. Although currently unclear, the clinicopathological malignancy of this SCC is thought to be similar to typical SCC. The classification of this SSC is currently under debate.
-
(4)
Spindle cell carcinoma (Fig. 2.33d)
This is a highly malignant carcinoma that presents with sarcoma-like histological findings due to the proliferation of mostly spindle cells and other polygonal cells. It is occasionally accompanied by CIS or SCC. These cells are positive for vimentin and some cytokeratins. It is important to perform complete resection of spindle cell carcinoma in the early stages when it presents with pedunculated or sessile exophytic growth.
-
(5)
Adenosquamous carcinoma (Fig. 2.33e)
This is a highly malignant carcinoma with histological findings of SCC and adenocarcinoma, with a ductal structure and mucus. The pathological features of invasion rather resemble those of adenocarcinoma, and attention must be paid to tumor progression through the trabecular bone so that bone destruction does not occur.
-
(6)
Papillary squamous cell carcinoma (Fig. 2.33f)
This invasive SCC presents with exophytic papillary growth as well as expansive growth similar to verrucous carcinoma at the tumor–host margin, with clear cellular atypia. For definitive diagnosis, it is important to examine for invasive characteristics.

2.2.9 Invasion to Lymphatic Vessels, Veins, and Nerves
-
(1)
Lymphatic vessel invasion
-
ly0: No lymphatic vessel invasion
-
ly1: Mild lymphatic vessel invasion
-
ly2: Marked lymphatic vessel invasion
Note: If immunostaining has been used for the evaluation of lymphatic vessel invasion, it must be recorded.
-
-
(2)
Venous invasion
-
v0: No venous invasion
-
v1: Mild venous invasion
-
v2: Marked venous invasion
Note: If elastic fiber staining has been used for the evaluation of venous invasion, it must be recorded.
-
-
(3)
Neural invasion
-
neu0: No neural invasion
-
neu1: Mild neural invasion
-
neu2: Marked neural invasion
Note: If immunostaining has been used for the evaluation of neural invasion, it must be recorded.
-
When examining the invasion of vessels, it is important to separate the invasion of lymph vessels (ly) and veins (v). When they are indistinguishable on a hematoxylin–eosin-stained specimen, elastic fiber staining such as Elastica van Gieson staining and immunostaining with monoclonal antibody D2-40 are used to confirm v and ly, respectively.
Among oral cavity cancers, perineural infiltration by adenoid cystic carcinoma is well known to affect prognosis. In SCC, it is rare for perineural infiltration to extend very far from the primary lesion site. However, it is important to pay attention to neural invasion near the resection margin or neural invasion into the mandibular canal.
2.2.10 Evaluation of the Resection Margin
-
(1)
Horizontal margin (HM), distance from margin ( ) mm
-
pHMX Impossible to evaluate the resection margin
-
pHM0 Margin (-)
-
pHM1 Margin (+)
Note: Also record presence or absence of OED at the mucosal stump.
-
-
(2)
Vertical margin (VM), distance from margin ( ) mm
-
pVMX Impossible to evaluate the resection margin
-
pVM0 Margin (-)
-
pVM1 Margin (+)
Note: Also record the results of evaluation of the bone stump in patients after osteotomy and stump of the inferior alveolar nerve in patients after mandibular/mandibular canal resection.
-
The most important point to remember during the histopathological examination of the resected specimen in oral cavity cancer is to determine the presence of cancer cells. For this reason, the pathologist should be provided with clinical information about where to conduct detailed examination. It is a good idea to mark (e.g., using a thread) the region of tissue suggestive of Ca(+) or (+/-) based on the preoperative findings of tumor margin, intraoperative palpation, and postoperative visual inspection of the specimen. It is also important to explain whether the resection margin in the mucosal surface was set in the area stained by iodine.
2.3 Regional Lymph Node Metastasis
The classification and range of cervical lymph nodes are the same as described in the Rules Regarding Lymph Nodes by the Japan Society of Clinical Oncology (JSCO) (Fig. 2.34), and lymph node metastasis was evaluated according to the UICC classification. Internationally, the level classification (Fig. 2.35) system by ACHNSO based on the area of neck dissection is widely used, and the American Academy of Otolaryngology-Head and Neck Surgery (AAO-HNS) classification, a fragmented version of the ACHNSO classification, has also been proposed.

Classification of cervical lymph nodes according to the classification of regional lymph nodes published by the Japan society of clinical oncology

Classification of cervical lymph node levels
-
(1)
Site
Regional lymph node groups (JSCO), level classification (AAO-HNS)
-
(2)
Number of metastasis
Number of metastatic lymph nodes/number of resected lymph nodes
-
(3)
Size (<3 < 6<) cm
-
(4)
Adhesiveness (−/+), extranodal invasion (−/+)
-
(5)
N factor
-
NX: Regional lymph nodes cannot be assessed
-
N0: No regional lymph node metastasis
-
N1: Metastasis in a single ipsilateral lymph node, ≤3 cm in greatest dimension
-
N2a: Metastasis in a single ipsilateral lymph node, >3 cm but ≤6 cm in greatest dimension
-
N2b: Metastasis in multiple ipsilateral lymph nodes, none >6 cm in greatest dimension
-
N2c: Metastasis in bilateral or contralateral lymph nodes, none >6 cm in greatest dimension
-
N3: Metastasis in a lymph node, >6 cm in greatest dimension
-
Note 1: Lymph nodes of the median region are ipsilateral lymph nodes.
-
Note 2: Direct invasion of the primary tumor to lymph nodes is classified as lymph node metastasis.
-
Note 3: Tumors ≥ 3 mm at sites corresponding to lymph nodes are classified as regional lymph node metastases even without a histological lymph node remnant.
-
Note 4: If the size is within the evaluation criteria of the pN classification, the size of the metastatic focus rather than the entire lymph node is measured.
Level classification (Fig. 2.35)
-
Level IA: Submental lymph nodes
-
Level IB: Submandibular lymph nodes
-
Level IIA: Superior deep cervical lymph nodes (jugulodigastric nodes) (anterior)
-
Level IIB: Superior deep cervical lymph nodes (jugulodigastric nodes) (posterior)
-
Level III: Middle deep cervical lymph nodes (jugulo-omohyoid nodes)
-
Level IV: Inferior deep cervical lymph nodes
-
Level VA: Spinal accessory lymph nodes
-
Level VB: Supraclavicular lymph nodes
-
Note: Examination of sentinel lymph node
Sentinel nodes (SNs) are the first lymph nodes to receive lymph flowing from a tumor. The SN theory states that the tumor metastasizes further after invading an SN. If this theory is correct, cases without SN metastasis are thought to be free of lymph node metastasis and therefore require no neck dissection. Consequently, by using SNs as an indicator of metastasis and performing detailed examination of SNs, it is possible to perform highly sensitive and effective diagnosis of micrometastasis. In recent years, the SN-based diagnosis of metastasis has produced good clinical outcomes in many fields.
In oral cancers, the site and frequency of SN metastasis vary due to individual variations in lymph drainage and to differences in tumor sites and tissue types. However, it is possible to determine the area of lymph node dissection required individually based on the severity of SN metastasis. Clinical application of SN biopsy in treating oral cavity cancer is expected to become widespread in the future; however, further studies are needed to improve the accuracy of intraoperative diagnosis of micrometastasis.
2.4 M Score
-
MX: Presence of distant metastasis cannot be assessed
-
M0: No distant metastasis
-
M1: Distant metastasis
The category M1 may be further specified according to the following notation:
Pulmonary (PUL), hepatic (HEP), osseous (OSS), lymph nodes (LYM), adrenal gland (ADR), brain (BRA), skin (SKI), and other (OTH)
2.5 Staging
The stage is determined according to the UICC classification. The T, N, and M scores and stage are recorded (Table 2.2).
2.6 Multiple, Double, and Multiple Primary Cancers
-
(1)
Multiple oral cancers: The occurrence of 2 or more primary cancers fulfilling the following conditions:
-
(a)
Cancers located at different sites according to the UICC classification.
-
(b)
Cancers located at corresponding contralateral sites.
-
(c)
Cancers located at ipsilateral sites, but not continuous and are clinically separated by ≥1.5 cm.
-
(d)
Each lesion is histopathologically confirmed to be a carcinoma.
-
(a)
-
(2)
Double cancer: The concurrence of primary oral cancer with primary malignant tumors of other organs. If both multiple and double cancers are observed, they are expressed as multiple-double cancers.
-
(3)
Multiple primary cancers: The term multiple primary cancers is used to comprehensively express multiple and double cancers.
-
(4)
Synchronous and heterochronous cancers
-
(a)
Cancers diagnosed within a period of <1 year are defined as synchronous cancers.
-
(b)
Cancers diagnosed at an interval of ≥1 year are defined as heterochronous cancers.
-
(c)
If there are both synchronous and heterochronous cancers, they are called synchronous/heterochronous cancers.
-
(a)
Note 1: The organs affected by double cancers are indicated.
Note 2: Whether the cancers are synchronous or heterochronous is indicated.
2.7 Histological Evaluation of Therapeutic Effect
If radiation therapy or chemotherapy has been used to treat oral cancer, conditions of treatment including the dose and method of irradiation, the kind, dose, and administration method of the drugs used, and the time from last treatment to resection of the lesion should be recorded.
In examining patients after preoperative treatment, specimens of the grossly estimated lesion must be prepared as thoroughly as possible, and the state of the remaining tumor must be evaluated histologically.
Grade 0: Ineffective
No therapeutic effect is noted in cancer tissue or cancer cells.
Grade 1: Slightly effective
Some degenerative change is noted in cancer tissue/cells, but cancer cells considered capable of proliferation (those showing eosinophilic cytoplasm with vacuolation and enlargement of the nucleus are also included) occupy ≥1/3 of the cancer in a tissue section.
Grade 1a: Very slightly effective
Cancer cells considered “capable of proliferation” occupy ≥2/3 of the cancer.
Grade 1b: Mildly effective
Cancer cells considered “capable of proliferation” occupy between 1/3 and 2/3 of the cancer.
Grade 2: Moderately effective
Cancer cells considered “capable of proliferation” occupy <1/3 of the cancer, and those showing a tendency toward nuclear disintegration are dominant.
Grade 3: Markedly effective
No cancer cells considered “capable of proliferation” are observed, and all cancer cells show a tendency toward nuclear disintegration, or only a trace of cancer is noted.
Note: If a section clearly judged to be a focus of reproliferation is noted in a treated cancer focus, the entry “evidence of reproliferation (+)” should be made after the judgment.
-
(1)
Study methods
To histologically assess the treatment outcome, it is necessary to examine all specimens for morphological changes in cancer cells, cell nests, and cytoplasm with the emphasis on changes in cancer cell morphology and the degree of destruction in cell nests. The ratio of areas showing any of the changes stated above is calculated by setting the entire section containing the cancerous tissue as 1. It is also important to record treatment conditions and preoperative duration because these factors influence tissue morphology.
-
(2)
Histological changes observed in cancer cells and cell nests (Fig. 2.36)
Fig. 2.36 
Histologic findings showing the effect of radiotherapy and chemotherapy
-
(a)
Changes in cancer cells
-
(1)
Increase in abnormal mitotic figures
-
(2)
Enlarged nucleus, prominent nucleolus, chromatin condensation on the nuclear membrane, and appearance of multinucleated giant cell
-
(3)
Lysis of cancer cells and nuclei, dark staining of cytoplasm with eosin, dark staining of the nucleus, and appearance of bizarre cells
-
(1)
-
(b)
Changes in cancer cell nests
-
(1)
Lymphocyte infiltration around cancer cell nests
-
(2)
Lysis of cancer cells and inflammatory cell infiltration
-
(3)
Moth-eaten-like changes to cell nests and shrinkage and disappearance of cell nests
-
(4)
Foreign-body granuloma and xanthomatous granuloma
-
(1)
-
(c)
“Nonviable cells”
-
(1)
Greatly eosinophilic cytoplasm
-
(2)
Pyknosis or karyolysis
-
(3)
Karyorrhexis
-
(4)
Cell membrane lysis
-
(5)
Cellular infiltration of leukocytes
-
(1)
-
(d)
“Viable cells”
Active cells without the features of “nonviable cell”
-
(a)

2.8 Biopsy
When obtaining a biopsy specimen prior to treatment, it is common to perform wedge biopsy, where a wedge-shaped specimen contains both the tumor and non-tumorous mucosa. The purpose of biopsy is not only to verify the presence of cancerous lesions but also to obtain detailed clinical information, including histological grade, invasion features, vascular invasion, and prediction of lymph node metastasis. At biopsy, a tissue specimen greater than 5 mm in diameter that contains invasion front tissue is collected. However, if vital iodine staining reveals a wide iodine-free area in the vicinity of the tumor, it is important to obtain a wedge-shape tissue specimen containing both the stained and non-stained areas with the aim to determine tumor resection margin.
Mucosal resection including the iodine-free area is recommended when the diagnosis of a small, early cancer (up to early T2) is made after careful assessment of tumor depth by palpation and diagnostic imaging.
2.9 Handling of Surgical Materials
2.9.1 Sectioning Method
It is a principle of surgical pathological studies of mucosal cancer to prepare cross sections perpendicular to the mucosal surface.
-
(1)
Sampling of soft tissues of the tongue, buccal mucosa, and FOM
In cancers of the tongue, buccal mucosa, and FOM, examination of coronal sections is preferable. Sections are obtained at intervals of 5–7 mm by step sectioning, and tumoral and ulcerative lesions in each section are photographed as magnified images. Large samples containing skin, muscle, or bone tissue are sectioned at intervals of 1–2 cm and photographed after checking the spread of the tumor on the mucosal surface and depth. Subsequently, a tissue block 4–5 mm thick is sectioned from a representative cross section to prepare specimens (Figs. 2.37, 2.38, 2.39, and 2.40).
Fig. 2.37 
How to resect tongue cancer
Fig. 2.38 
How to resect buccal mucosal cancer
Fig. 2.39 
How to resect floor of mouth cancer
Fig. 2.40 
How to resect upper gingival cancer
-
(2)
Sampling of maxillary or mandibular gingival cancer
-
(a)
Surgical sample consisting of only soft tissues
After checking the extent of the lesion (particularly, the anteroposterior dimension, lateral margins, and gingival margin at the dental neck adjacent to the next tooth), the sample is sectioned coronally or sagittally by referring to image information such as CT and MRI. First, the resection margin is sectioned and then the center of the primary lesion, and serial sections are obtained at intervals of 4–5 mm.
-
(b)
Surgical samples containing hard tissues
-
(1)
Method to examine the sample without separating hard and soft tissues
The basic method to section samples of upper or lower gingival cancer containing tooth or bone tissue is to section them perpendicularly to the dental arch, centering around the deepest part of the primary tumor. If the tumor is located in the incisor region, the dental arch is markedly curved, so the sample should be sectioned radially. Because the lateral and molar regions are also arched gently, sections should be made by checking the direction of the teeth. Sections containing hard tissue are cut out at intervals of 7–8 mm using a diamond cutter and decalcified after photographing the cross sections (Fig. 2.39).
-
(2)
Method to examine the sample by separating soft tissue and bone
Since the stainability of soft tissue is expected to be reduced by the decalcification of bone, specimens may also be prepared after separating hard and soft tissues. When this method is employed, accurate diagnosis is impossible unless the spatial relationship between bone and soft tissue is clear. Their locations must be determined on photographs or through other such techniques, and the spatial relationships of invasion sites and the resection margin should be clarified before their separation. In mandibular gingival cancer, because tumor cells are more numerous in the margin of soft tissue than in bone, judgment using high-quality specimens is meaningful. Particularly in patients who have undergone preoperative treatments such as chemotherapy, the judgment of the therapeutic effect using decalcified soft tissue specimens is often difficult.
-
(1)
-
(a)




2.9.2 Decalcification Methods
Tissue sections 7–8 mm thick containing hard tissue are placed in a decalcification solution after washing under running water, without washing, or after defatting in a mixture of equal volumes of methanol and chloroform for 1 day as a pretreatment. Plank-Rychlo’s rapid decalcification solution is typically used. Stainability after decalcification is preserved by performing low-temperature decalcification in a refrigerator (low-temperature decalcification). A sufficient amount of decalcification solution for the sample (several tens of times) should be prepared and changed during the decalcification process when considered appropriate. Decalcification is accelerated by shaking the decalcification solution. EDTA decalcification solution must be used if a process such as immunostaining is anticipated.
References
Japan Society for Oral Tumors (2010) General rules for clinical and pathological studies on oral cancer (in Japanese), 1st edn. Kanehara, Tokyo
Izumo T, Kirita T, Ajiri E et al (2012) General rules for clinical and pathological studies on oral cancer: a synopsis. Jpn J Clin Oncol 42:1099–1109
Sobin LH, Gospodarowicz MK, Wittekind C (eds) (2009) TNM classification of malignant tumours, 7th edn. UK Wiley-Blackwell, Chichester
Barnes L, Everson JW, Reichart P et al (eds) (2005) World Health Organization classification on tumours: pathology and genetics of head and neck tumours. IARC Press, Lyon
Working Group 1, Scientific Committee, Japan Society for Oral Tumors (2005) General rules for the clinical and pathological studies on oral carcinoma: 1, carcinoma of the tongue (in Japanese). J Jpn Soc Oral Tumor 17:13–86
Working Group 1, Scientific Committee, Japan Society for Oral Tumors (2008) General rules for the clinical and pathological studies on oral carcinoma: 3, carcinoma of the buccal mucosa and floor of mouth (in Japanese). J Jpn Soc Oral Tumor 20:25–117
Working Group 1, Scientific Committee, Japan Society for Oral Tumors (2007) General rules for the clinical and pathological studies on oral carcinoma: 2, Carcinoma of the lower gingiva (in Japanese). J Jpn Soc Oral Tumor 19:37–124
Working Group 1, Scientific Committee, Japan Society for Oral Tumors (2009) General rules for the clinical and pathological studies on oral carcinoma: 3, carcinoma of the upper gingiva and palate (in Japanese). J Jpn Soc Oral Tumor 20:25–117
Swearingen AG, McGraw JP, Palumbo VD (1966) Roentgenographic pathologic correlation of carcinoma of the gingiva involving the mandible. Am J Roentgenol Radium Ther Nucl Med 96:15–18
Izumo T (1986) Bone resorption by invasive squamous cell carcinoma of mandibular gingiva (in Japanese). J Stomatol Soc Jpn 53:343–356
Totsuka Y, Usui T, Tei K et al (1991) Mandibular involvement by squamous cell carcinoma of the lower alveolus: analysis and comparative study of histologic and radiologic features. Head Neck 13:40–50
Izumo T (2001) Surgical pathology of squamous cell carcinoma in the mandibular gingiva: mode of mandibular invasion (in Japanese). J Jpn Soc Oral Tumor 13:223–228
Tei K, Totsuka Y, Iizuka T et al (2004) Marginal resection for carcinoma of the mandibular alveolus and gingiva where radiologically detected bone defects do not extend beyond the mandibular canal. J Oral Maxillofac Surg 62:834–839
Japanese Society for Esophageal Diseases (2008) Japanese classification of esophageal cancer. Kanehara, Tokyo
Japanese Gastric Cancer Association (2011) Japanese classification of gastric carcinoma: 3rd edition. Gastric Cancer 14:101–112
Japanese Society for Cancer of the Colon and Rectum (2009) Japanese classification of colorectal carcinoma. Kanehara, Tokyo
Yamamoto E, Kohama G, Sunakawa H et al (1983) Mode of invasion, bleomycin sensitivity, and clinical course in squamous cell carcinoma of the oral cavity. Cancer 51:2175–2180
Hayashi T, Ito J, Taira S et al (2001) The relationship of primary tumor thickness in carcinoma of the tongue to subsequent lymph node metastasis. Dentomaxillofac Radiol 30:242–245
Shintani S, Yoshihama Y, Ueyama Y et al (2001) The usefulness of intraoral ultrasonography in the evaluation of oral cancer. Int J Oral Maxillofac Surg 30:139–143
Kimura Y, Ariji Y, Gotoh M et al (2001) Doppler sonography of the deep lingual artery. Acta Radiol 42:306–311
Sasaki T, Fujibayashi T, Imai Y et al (1999) A study on T-classifications of carcinomas of upper alveolus and gingiva and carcinoma of hard palate: a proposal of “sinus and nasal floor (SNF) criteria” (in Japanese). J Jpn Soc Oral Tumor 11:98–105
Sasaki T, Imai Y, Fujibayashi T (2004) New proposal for T classification of gingival carcinomas arising in the maxilla. Int J Oral Maxillofac Surg 33:349–352
Fujibayashi T (2004) Level of mandibular canal (LMC) criteria of lower gingival carcinomas and mode of mandibulectomy according to LMC criteria and bone invasion pattern (in Japanese). J Jpn Soc Oral Tumor 16:35–48
Nakayama E, Yoshiura K, Ozeki S et al (2003) The correlation of histologic features with a panoramic radiography pattern and a computed tomography pattern of bone destruction in carcinoma of the mandibular gingiva. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 96:774–782
Nakayama E, Yoshiura K, Yuasa K et al (2000) A study of the association between the prognosis of carcinoma of the mandibular gingiva and the pattern of bone destruction on computed tomography. Dentomaxillofac Radiol 29:163–169
Kimura Y, Sumi M, Sumi T et al (2002) Deep extension from carcinoma arising from the gingiva: CT and MR imaging features. AJNR Am J Neuroradiol 23:468–472
Mitz V, Peyronie M (1976) The superficial musculo-aponeurotic system (SMAS) in the parotid and cheek area. Plast Reconstr Surg 58:80–88
Janfaza P, Fabian RL (2011) Fasciae and fascial spaces of the head and neck. In: Janfaza P, Nadol JB, Galla R et al (eds) Surgical anatomy of the head and neck. Harvard University Press, Cambridge, pp 685–703
Wahi PN, Cohen B, Luthra UK et al (1971) Histological typing of oral and oropharyngeal tumours, vol 4, International histological classification of tumours. World Health Organization, Geneva
Pindborg JJ, Reichart P, Smith CJ et al (1997) World Health Organization: histological typing of cancer and precancer of the oral mucosa, 2nd edn. Springer, Berlin
Gale N, Westra W, Pilch BZ et al (2005) Epithelial precursor lesions. In: Barnes L, Everson JW, Reichart P et al (eds) World Health Organization classification on tumours: pathology and genetics of head and neck tumours. IARC Press, Lyon, pp 177–179
International Committee on Histological Definition (1962) An international agreement on histological terminology for the lesions of the uterine cervix. Acta Cytol 6:235–236
Reagan JW, Hamonic MJ (1956) Dysplasia of the uterine cervix. Ann N Y Acad Sci 63:1236–1244
Poulsen HE, Taylor CW, Sobin LH (1975) Histological typing of female genital tract tumours, vol 13, International histological classification of tumours. World Health Organization, Geneva
Izumo T (2011) Oral premalignant lesions: from the pathological view-point. Int J Clin Oncol 16:15–26
Working Committee of New Histopathological Criteria for Borderline Malignancies of the Oral Mucosa, Japanese Society for Oral Pathology (JSOP) (2007) JSOP Oral CIS Catalog: histopathological variations. Sunashobo Publishing, Tokyo
Working Committee of New Histopathological Criteria for Borderline Malignancies of the Oral Mucosa, Japanese Society for Oral Pathology (JSOP) (2014) Carcinoma in-situ of the oral mucosa: its pathological diagnostic concept based on the recognition of histological varieties proposed in the JSOP Oral CIS Catalog. J Oral Maxillofacial Surg Med Pathol 26:397–406. doi:10.1016/j.ajoms.2013.11.003
Shafer WG (1975) Oral carcinoma in situ. Oral Surg 39:227–238
Crissman JD, Zarbo RJ (1989) Dysplasia, in situ carcinoma, and progression to invasive squamous cell carcinoma of the upper aerodigestive tract. Am J Surg Pathol 13:5–16
Crissman JD, Sakr WA (2001) Squamous intraepithelial neoplasia of upper aerodigestive tract. In: Diagnostic surgical pathology of the head and neck. Saunders, Philadelphia, pp 1–17
Sakr WA, Gale N, Gnepp DR et al (2009) Squamous intraepithelial neoplasia of the upper aerodigestive tract. In: Diagnostic surgical pathology of the head and neck, 2nd edn. Saunders, Philadelphia, pp 1–44
Kuffer R, Lombardi T (2002) Premalignant lesions of the oral mucosa. A discussion about the place of oral intraepithelial neoplasia (OIN). Oral Oncol 38:125–130
Crissman JD, Zarbo RJ, Drozdowicz S et al (1988) Carcinoma in situ and microinvasive squamous carcinoma of the laryngeal glottis. Arch Otolaryngol Head Neck Surg 114:299–307
Sllamniku B, Bauer W, Painter C et al (1989) The transformation of laryngeal keratosis into invasive carcinoma. Am J Otolaryngol 10:42–54
Crissman JD, Visscher DW, Sarkar FH (1993) Premalignant lesion of the upper aerodigestive tract: biomakers of genetic alterations, proliferation, and differentiation. J Cell Biochem Suppl 17F:192–198
Blackwell KE, Fu YS, Calcaterra TC (1995) Laryngeal dysplasia. A clinico-pathologic study. Cancer 75:457–463
Kambic V (1997) Epithelial hyperplastic lesions-a challenging topic in laryngology. Acta Otolaryngol Suppl 527:7–11
Michaels L (1997) The Kambic-Gale method of assessment of epithelial hyperplastic lesions of the larynx in comparison with the dysplasia grade method. Acta Otolaryngol 527:17–20
Hellquist H, Cardesa A, Gale N et al (1999) Criteria for grading in Ljubljana classification of epithelial hyperplastic laryngeal lesions. A study by members of the working group on epithelial hyperplastic laryngeal lesions of the European Society of Pathology Histopathology 34:226–233
Gale N, Kambic V, Michaels L et al (2000) The Ljubljana classification: a practical strategy for the diagnosis of laryngeal precancerous lesions. Adv Anat Pathol 7:240–251
Gale N, Zidar N, Fischinger J et al (2000) Clinical applicability of the Ljubljana classification of epithelial hyperplastic laryngeal lesions. Clin Otolaryngol 25:227–232
Warnakulasuriya S (2001) Histological grading of oral epithelial dysplasia: revisited. J Pathol 194:294–297
Koren R, Kristt D, Shvero J et al (2002) The spectrum of laryngeal neoplasia: the pathologist’s view. Pathol Res Pract 198:709–715
Gale N, Michaels L, Luzar B et al (2009) Current review on squamous intraepithelial lesions of the larynx. Histopathology 54:639–656
Robinson RA (2010) Upper airway squamous dysplasia, early invasive squamous carcinoma, and squamous carcinoma variant. In: Head and neck pathology: atlas for histologic and cytologic diagnosis. Lippincott Williams & Wilkins, Philadelphia
Richardson MS, Barns L, Carison DL et al (2012) Protocol for the examination of specimens from patients with carcinoma of the lip and oral cavity, 7th edn. College of American Pathologists. http://www.cap.org/apps/docs/committees/cancer/cancer_protocols/2012/LipOralCav_12protocol.pdf. Accessed 1 July 2012
Mikata T, Cheng J, Maruyama S et al (2011) Emergence of keratin 17 vs. loss of keratin 13: their reciprocal immunohistochemical profiles in oral carcinoma in situ. Oral Oncol 47:497–503
Pitiyage G, Tilakaratne WM, Tavhvash M et al (2009) Molecular markers in oral epithelial dysplasia: review. J Oral Pathol Med 38:737–752
Hunter K, Thurlow JK, Fleming J et al (2006) Divergent routes to oral cancer. Cancer Res 66:7405–7413
Braakhuis BJM, Leemans CR, Brakenhoff RH (2004) A genetic progression model of oral cancer: current evidence and clinical implications. J Oral Pathol Med 33:317–322
Tabor MP, Braakhuis BJM, van der Wal JE et al (2003) Comparative molecular and histological grading of epithelial dysplasia of oral cavity and the oropharynx. J Pathol 199:354–360
Brieger J, Jacob R, Riazimand HS et al (2003) Chromosomal aberrations in premalignant and malignant squamous epithelium. Cancer Genet Cytogenet 144:148–155
Ha PK, Pilkington TA, Westra WH et al (2002) Progression of microsatellite instability from premalignant lesion to tumors of head and neck. Int J Cancer 102:615–617
Gelb AB, Kamel OW, LeBrun DP et al (1992) Estimation of tumor growth fractions in archival formalin-fixed, paraffin-embedded tissues using two anti-PCNA/cyclin monoclonal antibodies: factors affecting reactivity. Am J Pathol 141:1453–1458
Scott RE, Wilke MS, Wille JJ et al (1988) Human squamous carcinoma cells express complex defects in the control of proliferation and differentiation. Am J Pathol 133:374–380
Lindberg K, Rheinwald JG (1989) Suprabasal 40 kd keratin (K19) expression as an immunohistologic marker of premalignancy in oral epithelium. Am J Pathol 134:89–98
Klijanienko J, Micheau C, Carluc-Caillaud JM (1989) Significance of keratin 13 and 6 expression in normal, dysplastic and malignant squamous epithelium of pyriform fossa. Virchows Arch A Pathol Anat Histopathol 416:121–124
Coltrera MD, Zarbo RJ, Sakr WA et al (1992) Markers for dysplasia of the upper aerodigestive tract. Suprabasal expression of PCNA, p53, CK19 in alcohol-fixed, embedded tissue. Am J Pathol 141:817–825
Ogden GR, Chisholm DM, Adi M et al (1993) Cytokeratin expression in oral cancer and its relationship to tumor differentiation. J Oral Pathol Med 22:82–86
Kobayashi T, Ida H, Cheng J et al (2005) Histopathological evaluation of borderline malignancies of the oral mucosa by the aid of immunohistochemistry for keratin species and Ki-67. Oral Med Pathol 10:45
Kondoh N, Ohkura S, Arai M et al (2007) Gene expression signature that can discriminate oral leukoplakia subtypes and squamous cell carcinoma. Oral Oncol 43:455–462
Ohkura S, Kondoh N, Arai M et al (2005) Differential expression on the keratin-4, -13, -14, -17 and transglutaminase 3 genes during the development of oral squamous cell carcinoma from leukoplakia. Oral Oncol 41:607–613
Whipple ME, Mendez E, Farwell DG et al (2004) A genomic predictor of oral squamous cell carcinoma. Laryngoscope 114:1364–1354
Izumo T (2009) Squamous intraepithelial neoplasia (SIN) of the oral mucosa (in Japanese). J Jpn Soc Oral Tumors 22:15–24
Londono-Vallejo JA (2008) Telomere instability and cancer. Biochimie 90:73–82
Luzar B, Poljak M, Marin IJ et al (2003) Telomerase reaction is an early event in laryngeal carcinogenesis. Mod Pathol 16:841–848
Aida J, Izumo T, Shimomura N et al (2010) Telomere lengths in the oral epithelia with and without carcinoma. Eur J Cancer 46:430–439
Hamilton SR, Aaltonen LA (2000) World Health Organization classification of tumours: pathology and genetics of tumours of the digestive system. IARC, Lyon, pp 9–19
Epstein JB, Scully C, Spinelli JJ (1992) Toluidine blue and Lugol’s iodine application in the assessment of oral malignant disease and lesions at risk of malignancy. J Oral Patho Med 21:160–163
Kurita H, Kurashina K (1996) Vital staining with iodine solution in delineating the border of oral dysplastic lesions. Oral Surg Oral Med Oral Pathol 81:275–280
Shibahara T, Tanaka Y (2000) New method for detecting early oral cancer: a study of image uptake analysis with magnifying endoscopy (in Japanese). Oral Tumors 22:2–9
Broders AC (1920) Squamous-cell epithelioma of the lip. LAMA 74:656–664
Jakobsson PA, Eneroth CM, Killander D et al (1973) Histological classification and grading of malignancy in carcinoma of larynx. Acta Radiol 12:1–7
Willen R, Nathanson A, Moberger G et al (1975) Squamous cell carcinoma of the gingiva. Histological classification and grading of malignancy. Acta Otolaryngol 79:146–154
Anneroth G, Hansen LS (1984) A methodologic study of histologic classification and grading of malignancy in oral squamous cell carcinoma. Scand J Dent Res 92:448–468
Anneroth G, Batsakis J, Luna M (1987) Review of the literature and a recommended system of malignant grading in oral squamous cell carcinoma. Scand J Dent Res 95:229–249
Imai K (1954) Jintai ganshu hatsuiku joukyo no keitaigakuteki kousatsu. (in Japanese). Fukuoka Acta Medica 45:72–102
Yamamoto E, Kawajiri H, Katou K, Yoshizawa K, Noguchi N, Kitahara H (2009) Biological characteristics of the most invasive squamous cell carcinoma (Grade 4D) of the oral cavity (in Japanese). J Jpn Soc Oral Tumor 21:131–169
Yamamoto E, Miyakawa A, Kohama G (1984) Mode of invasion and lymph node metastasis in squamous cell carcinoma of the oral cavity. Head Neck Surg 6:938–947
Acknowledgments
Development of the first edition of General Rules for Clinical and Pathological Studies on Oral Cancer was made possible by the efforts of many oral surgeons, oral radiologists, and oral pathologists. We thank Eiichiro Ariji, Satoru Ozeki, Norihiko Okada, Sadao Okabe, Yuichiro Okazaki, Ken Omura, Tadaaki Kirita, Mikio Kusama, Toru Sato, Masanori Shinohara, Kazuo Shimozato, Satoru Shintani, Yoichi Tanaka, Eiji Nakayama, Takahumi Hayashi, Akihiro Miyazaki, HisaoYagishita, and Masayuki Yamane for their contribution to many parts of this chapter.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2015 Springer Japan
About this chapter
Cite this chapter
Izumo, T. (2015). Surgical Pathology of Oral Cancer. In: Kirita, T., Omura, K. (eds) Oral Cancer. Springer, Tokyo. https://doi.org/10.1007/978-4-431-54938-3_2
Download citation
DOI: https://doi.org/10.1007/978-4-431-54938-3_2
Published:
Publisher Name: Springer, Tokyo
Print ISBN: 978-4-431-54937-6
Online ISBN: 978-4-431-54938-3
eBook Packages: MedicineMedicine (R0)