
Abstract
Autophagy is degradation of intracellular proteins and organelles to maintain cytoplasmic homeostasis, and it is also involved in various pathophysiological processes in many diseases. We previously investigated alternation of autophagic activity in damaged neural tissue after SCI. It was also examined whether administration of rapamycin to promote autophagy can induce neuroprotective effect in SCI. Our results of these studies demonstrated that molecular markers of autophagy such as Beclin 1 and LC3 were significantly upregulated in the injured spinal cord. The increased activity of autophagy was observed in neurons, astrocytes, and oligodendrocytes at the lesion site. Electron microscopy showed an increased formation of autophagic vacuoles in the damaged neural cells. In addition, the rapamycin administration in acute phase of SCI promoted autophagy in the injured spinal cord and reduced neural tissue damage and locomotor impairment. These findings indicated that autophagic activity is increased in damaged neural tissue after SCI. Furthermore the promotion of autophagy by rapamycin treatment can provide neuroprotective effect to improve locomotor function following SCI. Here, we summarize our previous studies and review the evidence in related articles regarding the role of autophagy in SCI.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
1 Introduction
Autophagy is degradation of intracellular proteins and organelles to maintain cytoplasmic homeostasis, and it is also involved in various pathophysiological processes in many diseases [1–4]. Autophagy works for the elimination and recycling of long-lived proteins and unwanted organelles in a cell during development and under stress conditions [1, 5, 6] (Fig. 3.1). Amino acid starvation is a well-known trigger for autophagy, which degrades proteins to free amino acids that help cell survival [2].

Process of autophagy. A small volume of cytoplasm is enclosed by the isolation membrane, which results in the formation of an autophagosome. The autophagosome fuses with the lysosome where the cytoplasm is degraded. LC3 is bound to the autophagosomal membrane
Previous studies suggested that autophagy has a cytoprotective function against cell death [7, 8]. Autophagy contributed to cytoprotection in neurodegenerative disease and traumatic brain injury [9–13]. On the contrary, previous studies suggested that autophagy also contributes to the induction of cell death [8, 14, 15]. Autophagy can lead to nonapoptotic programmed cell death, which is called autophagic cell death [3, 16]. Activation of autophagy can induce cell death in a myocardial ischemia and reperfusion model [17]. In addition, autophagy can lead to autophagic cell death in cerebral ischemia and in a renal ischemia and reperfusion injury [18, 19].
Beclin 1, a Bcl-2-interacting protein, is a mammalian ortholog of yeast Atg6/Vps30 and it is known to be a promoter of autophagy [20]. Beclin 1 is a component of the class III phosphatidylinositol-3-kinase (PI3K) complex that works for the formation of autophagosomes [21]. The Atg8 protein, known as microtubule-associated protein 1 light chain 3 (LC3), is essential for autophagy [22]. LC3 is bound to autophagosomal membrane and thus is considered a specific marker protein to monitor autophagy [23] (Fig. 3.1). Autophagy may be dysregulated in several disorders, including metabolic diseases, neurodegenerative disorders, infectious diseases, and cancer. Pharmacological approaches to upregulate or inhibit this pathway are currently receiving considerable attention [24]. The mammalian target of rapamycin (mTOR) signaling pathway is known as a main molecular mechanism to regulate autophagic activity (Fig. 3.2). Recent studies revealed modulation of autophagy via mTOR signaling can be a therapeutic target for various diseases [24].

Signaling pathway of autophagy regulation. mTOR pathway negatively regulates autophagy. Rapamycin, a specific inhibitor of mTOR, prevents phosphorylation of p70S6K and promotes autophagy. Beclin 1 protein promotes autophagy
We previously reported that autophagic activity was upregulated in damaged neural tissue after SCI [25–27]. Furthermore our study demonstrated that pharmacological enhancement of autophagy provided neuroprotective effect following SCI [28, 29]. Here, we summarize our previous studies and review the evidence in related articles regarding the role of autophagy in SCI.
2 Upregulation of Beclin 1 Expression After Spinal Cord Injury
2.1 Summary
Beclin 1, a Bcl-2-interacting protein, is known to be a promoter of autophagy. We previously investigated the alterations in the Beclin 1 protein expression and the involvement of autophagy after SCI using a spinal cord hemisection model in mice [25]. In our results of immunohistochemistry and Western blot analysis, the Beclin 1 expression significantly increased at the lesion site after hemisection. The Beclin 1 expression was observed in neurons, astrocytes, and oligodendrocytes. These results suggested that autophagy can be activated in the injured spinal cord.
2.2 Increased Expression of Beclin 1 After SCI
To investigate an alteration of the Beclin 1 expression in the spinal cord, immunohistochemical staining of Beclin 1 was performed at 4 and 24 h and 3, 7, and 21 days after hemisection. The cells expressing Beclin 1 were increased in the injured side after hemisection (Fig. 3.3a). The cells expressing Beclin 1 were observed in both the gray matter and white matter of the injured side. In counting Beclin 1-positive cells, the number of Beclin 1-positive cells on the injured side was significantly higher than those on the contralateral side at each time point. The increased expression of Beclin 1 started from 4 h, peaked at 3 days, and lasted for at least 21 days after hemisection. Western blot analysis confirmed that the level of Beclin 1 protein was significantly higher in the injured side than in the contralateral side.

Immunohistochemical staining of Beclin1 and LC3 in transverse sections at 3 days after hemisection. (a), (b) The cells expressing Beclin1 and LC3 were increased on the injured side (R) in comparison to the contralateral side (L). Scale bars = 500 μm. (c)–(k) In double staining of LC3 and cell type makers (green) on the injured side in transverse section at 3 days after hemisection, the LC3-positive cells were observed in the NeuN-, GFAP-, and Olig2-labeled cells (arrowheads in (e), (h), (k)). Scale bars = 50 μm
2.3 Beclin 1 Expression in Various Neural Cells After SCI
To investigate the Beclin 1 expression in a specific type of cells including neurons, astrocytes, and oligodendrocytes, the spinal cord sections at 3 days after hemisection were double stained for Beclin 1 and various cell type markers: NeuN for neurons, GFAP for astrocytes, and Olig2 for oligodendrocytes. In the double staining, the expression of Beclin 1 was observed in NeuN-, GFAP-, and Olig2-labeled cells. These results demonstrated the Beclin 1 expression to be observed in neurons, astrocytes, and oligodendrocytes.
2.4 Expression of Beclin 1 in Dying Cells
To detect Beclin 1 expression in dying cells, we performed double staining of Beclin 1 and TUNEL in the sections at 3 days after hemisection. The TUNEL-positive cells occasionally showed as Beclin 1 positive. Under higher magnification, most of the nuclei of the TUNEL-positive cells that did not show Beclin 1 positive were shrunken or fragmented, as is typical of apoptotic nuclei. On the other hand, most of the nuclei of the TUNEL-positive cells that were found to be Beclin 1 positive were round, as in autophagic cell death, and they had neither shrunken nor were fragmented.
3 Confirmation of Autophagy Induction After Spinal Cord Injury
3.1 Summary
To confirm induction of autophagy after SCI, we previously investigated expression of LC3, a characteristic marker of autophagy, in immunohistochemistry and Western blot using an SCI model in mice [26]. Electron microscopic analysis was also performed to examine the formation of autophagy in the injured spinal cord. Immunohistochemistry showed that the number of the LC3-positive cells significantly increased at the lesion site after hemisection. The LC3-positive cells were observed in neurons, astrocytes, and oligodendrocytes. Western blot analysis demonstrated that the level of LC3-II protein expression significantly increased in the injured spinal cord. Electron microscopy showed an increased formation of autophagic vacuoles in the damaged neural cells. This study confirmed both biochemically and anatomically that autophagy was clearly activated in the damaged neural tissue after SCI.
3.2 Upregulation of Autophagy Marker, LC3 in Injured Spinal Cord
Immunohistochemical analysis showed that cells expressing LC3 were increased on the injured side in comparison to the contralateral side after hemisection. The cells expressing LC3 were observed in both the gray matter and the white matter of the injured side (Fig. 3.3b). In higher magnification on the injured side, the cells expressing LC3 displayed bright, punctate LC3 dots in the cytoplasm, indicating formation of autophagic vacuoles. The number of LC3-positive cells on the injured side was significantly higher than those on the contralateral side at 3 days. The increase of the LC3-positive cells commenced at 4 h and lasted for at least 21 days. The maximum number of LC3-positive cells on the injured side was observed at 3 days, and it thereafter decreased at 7 days after hemisection. Western blot analysis confirmed the level of LC3-II protein was significantly higher in the injured side than in uninjured spinal cord.
3.3 LC3 Expression in Various Neural Cells
Double staining of LC3 and various cell type markers revealed that the LC3-positive cells were observed in NeuN-, GFAP-, and Olig2-labeled cells on the injured side after hemisection (Fig. 3.3c–k).
3.4 Electron Microscopic Analysis for Autophagy Formation
Electron microscopic analysis after the hemisection demonstrated that the formations of numerous autophagic vacuoles including autophagosome with double-membrane structures (Fig. 3.1) were observed in the damaged cells on the injured side. A higher magnification showed that the autophagosomes were containing membranous structures and parts of the cytoplasm.
3.5 Expression of LC3 in Dying Cells
To confirm autophagy induction in dying cells, we performed double staining of LC3 and TUNEL using the spinal cord section at 3 days after hemisection. The double staining showed that the TUNEL-positive cells were occasionally LC3 positive. Higher magnification revealed that the nuclei of the TUNEL-positive cells that were not LC3 positive were shrunken or fragmented, typical of apoptotic nuclei. On the contrary, the nuclei of the TUNEL-positive cells that were found to be LC3 positive were round, as in autophagic cell death.
4 Autophagy Modulation as a Potential Therapeutic Target for Spinal Cord Injury
4.1 Summary
The mTOR is a serine/threonine kinase that negatively regulates autophagy (Fig. 3.2). Rapamycin, an inhibitor of mTOR signaling, can promote autophagy and exert neuroprotective effects in several diseases of the central nervous system. We previously investigated whether administration of rapamycin promotes autophagy and reduces neural tissue damage and locomotor impairment after spinal cord contusion injury in mice [28]. Our results demonstrated that the administration of rapamycin at 4 h after injury significantly promoted autophagic activity in the injured spinal cord. In addition, the rapamycin treatment significantly reduced neural tissue damage and locomotor impairment after SCI. These results indicate that rapamycin promoted autophagy by inhibiting the mTOR signaling pathway and induced neuroprotective effect after SCI (Fig. 3.4).

Neuroprotective mechanism of rapamycin treatment in acute SCI. Rapamycin suppresses mTOR signaling pathway and promotes autophagy after SCI. The increased autophagic activity can produce neuroprotective effect and reduce neural tissue damage and locomotor impairment following SCI
4.2 Inhibition of mTOR Promotes Autophagy After Spinal Cord Injury
To examine the effectiveness of the rapamycin treatment on the mTOR signaling pathway, the phosphorylation of p70S6K was evaluated by Western blot analysis. In our results, the phosphorylated p70S6K protein was significantly decreased after administration of rapamycin, indicating rapamycin actually inhibited mTOR after SCI (Fig. 3.4). We also investigated the activation of autophagy after rapamycin treatment, immunohistochemical staining, and Western blot analysis of LC3 were performed. Immunostaining of LC3 showed the number of LC3-positive cells was significantly increased in the rapamycin-treated mice compared with the vehicle-treated mice. In the Western blot analysis, the expression of LC3-II protein was significantly increased in the rapamycin-treated mice compared with the vehicle-treated mice.
4.3 Inhibition of mTOR Produces Neuroprotective Effect in Injured Spinal Cord
To investigate neural cell loss after injury, the number of NeuN-positive cells was compared between the vehicle and the rapamycin-treated mice by immunohistochemical staining. In our results, the number of NeuN-positive cells in the rapamycin-treated mice was significantly higher than those in the vehicle-treated mice at 42 days. Additionally, to investigate the effect of rapamycin on cell death after SCI, we performed TUNEL staining and compared the number of TUNEL-positive cells between the vehicle- and the rapamycin-treated mice at 3 days after injury. The number of TUNEL-positive cells was significantly lower in the rapamycin-treated mice compared to the vehicle-treated mice. These results indicated that rapamycin treatment can produce neuroprotective effect to reduce neuronal loss and cell death following SCI.
4.4 Inhibition of mTOR Improves Locomotor Recovery After Spinal Cord Injury
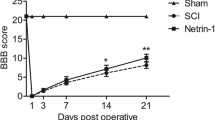
To evaluate the effect of rapamycin treatment on locomotor recovery after SCI, Basso mouse scale (BMS) was measured for 6 weeks [30]. In our result, the rapamycin-treated mice had significantly higher BMS scores than the vehicle-treated mice from 3 to 6 weeks. This data supports the neuroprotection produced by mTOR inhibition can improve locomotor function after SCI.
5 Discussion
5.1 Upregulation of Autophagy in CNS Injury
Previous studies demonstrated the expression of Beclin 1 to increase at lesion sites after traumatic brain injury and cerebral ischemia [9, 18, 31]. In such diseases, expression of LC3 increases at the lesion sites [18, 32–35]. These reports suggest that the autophagic activity increases in response to the neural tissue damage of the brain. Our previous studies first reported the increased expression of Beclin 1 and LC3 in the damaged neural tissue after SCI [25, 26]. Using electron microscopy, we also confirmed that the formation of autophagic vacuoles also increased in the damaged cells of the injured spinal cord [26]. Therefore, autophagy was activated in the damaged neural tissue after SCI.
5.2 Neuroprotective Function of Autophagy
Many studies reported that autophagy has a cytoprotective function against cell death. Autophagy has a cytoprotective function in neurodegenerative diseases [10–13]. Autophagy induced neuroprotection in traumatic brain injury and in neonatal hypoxia-ischemia induced brain injury [9, 36]. In models of Huntington disease, the stimulation of autophagy protects cells against apoptosis [37]. In addition, the inhibition of autophagy increases the apoptosis of neurons and also causes neurodegeneration in mice [10, 11]. One potential mechanism underlying these neuroprotective effects is the blocking of apoptosis by the activation of autophagy [12, 36, 38]. Interestingly, it has been suggested that mTOR inhibition enhances the clearance of mitochondria by inducing autophagy, thereby reducing cytosolic cytochrome c release and downstream caspase activation [24, 39]. Previous studies have demonstrated that inhibition of mTOR upregulates autophagy and shows cytoprotective functions by reducing apoptosis in various disease models, including the myocardial ischemia-reperfusion model [38] and neonatal hypoxia-ischemia-induced brain injury model [36]. In our results, rapamycin promoted autophagy by inhibiting the mTOR signaling and reduced neural tissue damage such as neuronal loss and cell death following SCI. These results suggested autophagy produced neuroprotective effect after SCI.
5.3 Autophagy Modulation as a Therapeutic Target for SCI
Autophagy may be dysregulated in various disorders, including metabolic diseases, neurodegenerative disorders, infectious diseases, and cancer. In several conditions, autophagy is inhibited and this can occur at different stages of the process to enhance disease, whereas in other cases autophagic activity may be permissive towards pathogenesis [24]. Recently, pharmacological approaches to upregulate or inhibit autophagy are receiving considerable attention. For example, autophagy upregulation may be of therapeutic benefit in certain neurodegenerative diseases and trauma [9, 36, 39]. Indeed, our study demonstrated that upregulation autophagy by mTOR inhibitor, rapamycin, resulted in reduction of neural tissue damage and locomotor impairment after SCI [28]. Therefore, the pharmacological modulation of autophagy may have clinical benefits for treatment of patients with SCI. Further studies to clarify the neuroprotective and neuroregenerative mechanisms regulated by autophagy are needed in order to approve the clinical use of pharmacological modulation of autophagy for patients with acute SCI.
5.4 Autophagic Cell Death
The autophagic process can lead to nonapoptotic programmed cell death, which is known as autophagic cell death [8]. Autophagic cell death is morphologically distinct from necrotic cell death and apoptotic cell death [14, 16]. The nucleus is shrunken and fragmented in apoptosis, but in autophagic cell death, the nucleus does not change [14, 18, 31]. Previous studies have shown autophagic cell death to be induced after brain trauma and cerebral ischemia and contributed to neural tissue damage [31, 33]. Our studies demonstrated that most of the nuclei in the TUNEL-positive cells expressed Beclin 1 or LC3 were round, which should normally be observed in autophagic cell death, and they were not either shrunken or fragmented as is observed in apoptotic nuclei [26, 40]. Therefore, these findings suggested autophagic cell death may occur in the injured spinal cord. However, the molecular mechanism defining the features of autophagic cell death is still unknown [8, 41, 42]. Further studies are needed to clarify the molecular mechanism of autophagic cell death in SCI.
6 Conclusion
Our previous studies demonstrated that molecular markers of autophagy such as Beclin 1 and LC3 were significantly upregulated in the injured spinal cord. The increased activity of autophagy was observed in neurons, astrocytes, and oligodendrocytes at the lesion site. Electron microscopy showed an increased formation of autophagic vacuoles in the damaged neural cells. In addition, the rapamycin administration in acute phase of SCI promoted autophagy in the injured spinal cord and reduced neural tissue damage and locomotor impairment. These findings indicated that autophagic activity is increased in damaged neural tissue after SCI. Furthermore the promotion of autophagy by rapamycin treatment can provide neuroprotective effect to improve locomotor function following SCI.
References
Gozuacik D, Kimchi A (2004) Autophagy as a cell death and tumor suppressor mechanism. Oncogene 23:2891–2906
Klionsky D, Emr S (2000) Autophagy as a regulated pathway of cellular degradation. Science 290:1717–1721
Larsen K, Sulzer D (2002) Autophagy in neurons: a review. Histol Histopathol 17:897–908
Ogier-Denis E, Codogno P (2003) Autophagy: a barrier or an adaptive response to cancer. Biochim Biophys Acta 1603:113–128
Levine B, Klionsky D (2004) Development by self-digestion: molecular mechanisms and biological functions of autophagy. Dev Cell 6:463–477
Mele´ndez A, Tallo´czy Z, Seaman M et al (2003) Autophagy genes are essential for dauer development and life-span extension in C. elegans. Science 301:1387–1391
Rubinsztein DC, DiFiglia M, Heintz N et al (2005) Autophagy and its possible roles in nervous system diseases, damage and repair. Autophagy 1(1):11–22. doi:1513[pii]
Tsujimoto Y, Shimizu S (2005) Another way to die: autophagic programmed cell death. Cell Death Differ 12(Suppl 2):1528–1534. doi:10.1038/sj.cdd.4401777
Erlich S, Alexandrovich A, Shohami E et al (2007) Rapamycin is a neuroprotective treatment for traumatic brain injury. Neurobiol Dis 26:86–93
Hara T, Nakamura K, Matsui M et al (2006) Suppression of basal autophagy in neural cells causes neurodegenerative disease in mice. Nature 441(7095):885–889. doi:nature04724 [pii], 10.1038/nature04724
Komatsu M, Waguri S, Chiba T et al (2006) Loss of autophagy in the central nervous system causes neurodegeneration in mice. Nature 441(7095):880–884. doi:10.1038/nature04723
Pan T, Kondo S, Zhu W et al (2008) Neuroprotection of rapamycin in lactacystin-induced neurodegeneration via autophagy enhancement. Neurobiol Dis 32:16–25
Sarkar S, Ravikumar B, Floto RA et al (2009) Rapamycin and mTOR-independent autophagy inducers ameliorate toxicity of polyglutamine-expanded huntingtin and related proteinopathies. Cell Death Differ 16(1):46–56. doi:10.1038/cdd.2008.110
Kitanaka C, Kuchino Y (1999) Caspase-independent programmed cell death with necrotic morphology. Cell Death Differ 6(6):508–515. doi:10.1038/sj.cdd.4400526
Scarlatti F, Granata R, Meijer AJ et al (2009) Does autophagy have a license to kill mammalian cells? Cell Death Differ 16(1):12–20. doi:cdd2008101 [pii], 10.1038/cdd.2008.101
Clarke PG (1990) Developmental cell death: morphological diversity and multiple mechanisms. Anat Embryol 181(3):195–213
Matsui Y, Takagi H, Qu X et al (2007) Distinct roles of autophagy in the heart during ischemia and reperfusion: roles of AMP-activated protein kinase and Beclin 1 in mediating autophagy. Circ Res 100(6):914–922. doi:10.1161/01.RES.0000261924.76669.36
Rami A, Langhagen A, Steiger S (2008) Focal cerebral ischemia induces upregulation of Beclin 1 and autophagy-like cell death. Neurobiol Dis 29:132–141
Suzuki C, Isaka Y, Takabatake Y et al (2008) Participation of autophagy in renal ischemia/reperfusion injury. Biochem Biophys Res Commun 368(1):100–106. doi:10.1016/j.bbrc.2008.01.059
Liang XH, Jackson S, Seaman M et al (1999) Induction of autophagy and inhibition of tumorigenesis by Beclin 1. Nature 402(6762):672–676. doi:10.1038/45257
Kihara A, Kabeya Y, Ohsumi Y et al (2001) Beclin-phosphatidylinositol 3-kinase complex functions at the trans-Golgi network. EMBO Rep 2(4):330–335. doi:10.1093/embo-reports/kve061
Mizushima N (2004) Methods for monitoring autophagy. Int J Biochem Cell Biol 36:2491–2502
Kabeya Y, Mizushima N, Ueno T et al (2000) LC3, a mammalian homologue of yeast Apg8p, is localized in autophagosome membranes after processing. EMBO J 19:5720–5728
Rubinsztein DC, Codogno P, Levine B (2012) Autophagy modulation as a potential therapeutic target for diverse diseases. Nat Rev Drug Discov 11(9):709–730. doi:10.1038/nrd3802
Kanno H, Ozawa H, Sekiguchi A et al (2009) Spinal cord injury induces upregulation of Beclin 1 and promotes autophagic cell death. Neurobiol Dis 33:143–148
Kanno H, Ozawa H, Sekiguchi A et al (2011) Induction of autophagy and autophagic cell death in damaged neural tissue after acute spinal cord injury in mice. Spine (Phila Pa 1976) 36(22):E1427–E1434. doi:10.1097/BRS.0b013e3182028c3a
Kanno H, Ozawa H, Sekiguchi A et al (2009) The role of autophagy in spinal cord injury. Autophagy 5(3):390–392. doi:7724 [pii]
Sekiguchi A, Kanno H, Ozawa H et al (2012) Rapamycin promotes autophagy and reduces neural tissue damage and locomotor impairment after spinal cord injury in mice. J Neurotrauma 29(5):946–956. doi:10.1089/neu.2011.1919
Kanno H, Ozawa H, Sekiguchi A et al (2012) The role of mTOR signaling pathway in spinal cord injury. Cell Cycle 11(17):3175–3179. doi:10.4161/cc.21262
Basso DM, Fisher LC, Anderson AJ et al (2006) Basso Mouse Scale for locomotion detects differences in recovery after spinal cord injury in five common mouse strains. J Neurotrauma 23(5):635–659. doi:10.1089/neu.2006.23.635
Diskin T, Tal-Or P, Erlich S et al (2005) Closed head injury induces upregulation of Beclin 1 at the cortical site of injury. J Neurotrauma 22:750–762
Liu CL, Chen S, Dietrich D et al (2008) Changes in autophagy after traumatic brain injury. J Cereb Blood Flow Metab (Official J Int Soc Cereb Blood Flow Metab) 28(4):674–683. doi:10.1038/sj.jcbfm.9600587
Adhami F, Liao G, Morozov YM et al (2006) Cerebral ischemia-hypoxia induces intravascular coagulation and autophagy. Am J Pathol 169(2):566–583. doi:10.2353/ajpath.2006.051066
Uchiyama Y, Koike M, Shibata M (2008) Autophagic neuron death in neonatal brain ischemia/hypoxia. Autophagy 4(4):404–408
Wen YD, Sheng R, Zhang LS et al (2008) Neuronal injury in rat model of permanent focal cerebral ischemia is associated with activation of autophagic and lysosomal pathways. Autophagy 4(6):762–769
Carloni S, Buonocore G, Balduini W (2008) Protective role of autophagy in neonatal hypoxia-ischemia induced brain injury. Neurobiol Dis 32:329–339
Ravikumar B, Vacher C, Berger Z et al (2004) Inhibition of mTOR induces autophagy and reduces toxicity of polyglutamine expansions in fly and mouse models of Huntington disease. Nat Genet 36:585–595
Khan S, Salloum F, Das A et al (2006) Rapamycin confers preconditioning-like protection against ischemia-reperfusion injury in isolated mouse heart and cardiomyocytes. J Mol Cell Cardiol 41:256–264
Ravikumar B, Berger Z, Vacher C et al (2006) Rapamycin pre-treatment protects against apoptosis. Hum Mol Genet 15:1209–1216
Kanno H, Ozawa H, Sekiguchi A et al (2009) Spinal cord injury induces upregulation of Beclin 1 and promotes autophagic cell death. Neurobiol Dis 33(2):143–148. doi:S0969-9961(08)00217-9 [pii], 10.1016/j.nbd.2008.09.009
Kroemer G, Levine B (2008) Autophagic cell death: the story of a misnomer. Nat Rev Mol Cell Biol 9(12):1004–1010. doi:10.1038/nrm2529
Galluzzi L, Vitale I, Abrams JM et al (2012) Molecular definitions of cell death subroutines: recommendations of the Nomenclature Committee on Cell Death 2012. Cell Death Differ 19(1):107–120. doi:10.1038/cdd.2011.96
Conflict of Interest The authors declare that they have no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2014 Springer Japan
About this chapter
Cite this chapter
Kanno, H., Ozawa, H. (2014). Autophagy in Spinal Cord Injury: Pathogenic Roles and Therapeutic Implications. In: Uchida, K., Nakamura, M., Ozawa, H., Katoh, S., Toyama, Y. (eds) Neuroprotection and Regeneration of the Spinal Cord. Springer, Tokyo. https://doi.org/10.1007/978-4-431-54502-6_3
Download citation
DOI: https://doi.org/10.1007/978-4-431-54502-6_3
Published:
Publisher Name: Springer, Tokyo
Print ISBN: 978-4-431-54501-9
Online ISBN: 978-4-431-54502-6
eBook Packages: MedicineMedicine (R0)