
Abstract
The association between endometriosis and epithelial ovarian cancer has been supported by years of epidemiologic research. Approximately 1.0 % of women with endometriosis may undergo malignant transformation. The malignant transformation is believed to progress in a stepwise fashion through an intermediary endometriotic lesion, atypical endometriosis. The greatest risk is associated with epithelial ovarian cancer of endometrioid and clear cell histology. Endometriosis and ovarian cancer may share a common pathogenic mechanism: hyperestrogenism, excess oxidative stress, and inflammation derived from repeated hemorrhage and iron, contributing to ovarian tumorigenesis. The iron-induced signals can contribute to carcinogenesis via three processes: step 1, by increasing oxidative stress, which facilitates the accumulation of somatic mutations, contributing to endometriosis-associated ovarian cancer initiation; step 2, by creating an estrogen-dependent microenvironment, supporting endometrioid adenocarcinoma progression; and step 3, by surviving stressful periods, thereby contributing to clear cell carcinoma progression. In conclusion, some endometriosis lesions may predispose to ovarian cancer, but future studies are needed to know the exact mechanisms of endometriosis-associated ovarian cancer.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
1 Introduction
Endometriosis is a benign hormone-dependent condition and a common gynecologic disorder, with an estimated frequency of approximately 10 % among women of reproductive age. This disease often results in a serious clinical problem because of its potential for adverse sequelae, including severe dysmenorrhea, chronic pelvic pain, infertility, and possibly developing ovarian cancer [1]. The exact etiology and pathogenesis of endometriosis have yet to be elucidated. It may mainly cause retrograde menstruation, implantation of menstrual tissue, and peritoneal metaplasia in a woman with an improper immune response and a genetic predisposition to developing endometriotic lesions. Thus, the pathogenesis of endometriosis is multifactorial, including the role of genetics, hormonal factors, environmental factors, and immune system.
The pathogenesis of endometriosis has been an area of active investigation, including retrograde menstruation theory, coelomic metaplasia theory, embryonic rest theory, lymphovascular metastasis theory, stem cell theory, and others [2]. Several studies exploring the differential expression of genes between autologous eutopic and ectopic endometrium from patients with endometriosis or between eutopic endometrium from women with or without endometriosis may provide a better understanding of the pathogenesis and pathophysiology of the disorder. The genome-wide profiling and pathway-based enrichment analysis revealed that genes related to cell cycle, growth factors, signal transduction, transcription factors, hormones, cytokines, chemokines and (pro)inflammation, proteases, cell adhesion and motility, stress response and detoxification, immune response, and metabolism were affected in the pathogenesis process of endometriosis [3–16].
Furthermore, it is generally assumed that histologically benign endometriotic lesions may be caused by the genetic defects that are permissive for malignant transformation. Studies have documented loss of heterozygosity and mutations of tumor suppressor genes in endometriosis (see Sect. 29.3). This disorder exhibits high genetic instability that is involved in the cell phenotype changes that take place during cancer progression [17]. Endometriosis shows a monoclonal pattern in origin, suggesting that individual glands of the lesion are derived from single precursor cells. Also, the genome-wide transcriptome of endometriosis does resemble that found in ovarian cancer.
2 Epidemiologic Research
Epithelial ovarian cancers have been classified into four major histologic subtypes: serous (∼60 %), endometrioid (∼10–20 %), clear cell (<10 %), and mucinous (<5 %). Serous, endometrioid, clear cell, and mucinous ovarian tumors histologically resemble the phenotypes of the fallopian tube, proliferative endometrium, gestational endometrium, and endocervix/gastrointestinal tract, respectively. Comparing the profile of epithelial ovarian cancer between Japanese and Caucasians, clear cell carcinomas (27.6 vs. <10 %) are more common in Japan, possibly with fewer serous adenocarcinomas (40.7 vs. 60 %). One possibility is that the Japanese may exhibit a lower proportion of serous adenocarcinoma compared to the United States population. This may reflect a proportional change.
The investigators have focused on latest knowledge of the genetic and environmental factors affecting the development of epithelial ovarian cancer and outline future challenges in its pathogenesis research [18]. The time trend analyses of incidence between 1973 and 2005 in the United States exhibited a decline by 27 % in epithelial ovarian cancer incidence [19, 20]. The incidence trend of ovarian cancer in the United States is similar to the trends observed in most of the European countries. In contrast, an increase in epithelial ovarian cancer rates has been reported in Japan. It is generally accepted that oral contraceptive (OC) use reduces the risk of ovarian cancer and endometrial cancer. Although the exact reasons for the higher ovarian cancer incidence rates in Japan are unknown, the trends may be due to changes in risk factors, such as diet and environmental factors and the low prevalence of OC use (2–3 %) in Japan. Although some part of the pathogenesis has been unveiled, the complete events of genetic and epigenetic changes associated with epithelial ovarian cancer remain to be identified.
The association between endometriosis and malignant transformation has often been described in the medical literature. A literature search of MEDLINE (online PubMed database) was conducted for published articles from 1966 to October 2010 using the keywords endometriosis combined with malignant transformation [21]. The search revealed an increase in reports describing endometriosis-associated malignant transformation. Overall, more than 400 articles were included following a process of independent review of each article and six were graded as good quality [22–27]. Numerous epidemiologic studies have shown an association between endometriosis and ovarian cancer [28, 29]. Epidemiologic studies have shown an increased risk of epithelial ovarian cancer, especially endometrioid and clear cell histologies, among women with endometriosis. Brinton et al. examined the records of 20,686 women hospitalized with endometriosis between 1969 and 1983 [22]. Standardized incidence ratios (SIRs) of cancers were calculated to compare the cancer incidence of the study cohort with that of the general population. After adjustment for age, period, and comorbidities, the hazards ratio was 1.9 for the endometriosis group compared with the control group, indicating that this cohort had an increased overall risk of ovarian cancer. They also found further increases in ovarian cancer risk among women with long-standing histories of ovarian endometrioma (SIR, 4.2) [22]. The same group reported that patients with endometriosis had the risk (4.19-fold) compared with the general population if they presented with primary infertility [24].
There is one unique epidemiologic study in Japan, supporting the hypothesis that ovarian endometrioma increases the subsequent risk of developing ovarian cancer [30]. A cohort of 6,398 women with a clinically documented ovarian endometrioma enrolled between 1985 and 1995 in the prefecture-wide Shizuoka Cohort Study on Endometriosis and Ovarian Cancer Programme has prospectively analyzed, with follow-up through 2002. During follow-up of up to 17 years of the ovarian endometrioma cohort, 46 incident ovarian cancers were identified, yielding that the ovarian cancer risk was elevated significantly among women with ovarian endometrioma (SIR, 8.95). The elevated risk of developing ovarian cancer was mainly restricted to women with ovarian endometrioma diagnosed after age 40 (advancing age). Tumor size 9 cm or greater in diameter was an independent predictive factor of patients with development of ovarian cancer [31]. This analysis was restricted to those with a clinically diagnosed ovarian endometrioma. Therefore, it has been proposed that ovarian endometrioma has been identified as a possible risk factor for ovarian cancer.
Surveillance of endometriosis might result in a number of newly diagnosed cases of ovarian cancer [20]. It is generally accepted that the incidence of malignant transformations ranges between 0.7 and 1.0 % in women with endometriosis in Japan. Although this finding is consistent with the results of six studies that support a positive association between endometriosis and risk of ovarian cancer [22–27], Kobayashi’s group found an SIR of 8.95, compared with other studies reporting SIR less than 5.0. These data provide novel and exciting possibilities. A number of factors contribute to the results including ethnic disparities and differences in genetic predisposition. A significantly increased risk may be found for Japanese. Ovarian endometrioma may have higher cancer risk than pelvic endometriosis. Ovarian cancer in Japan is a growing concern because long-term ovarian cancer trends in incidence show rising rates.
3 Ovarian Cancer Susceptibility Genes
Although the etiology and the ovarian carcinogenesis still need clarification, the link between ovarian carcinogenesis and (epi)genetic mutations is well established [18]. The investigators have utilized genome-wide gene expression analysis and association studies to identify a specific gene signature distinguishing ovarian cancer from controls and which served as a molecular signature for complicated histologies. Recent high-throughput whole genome or targeted sequencing studies have also identified numerous somatic mutations across the whole exome in a variety of neoplasms.
High-grade serous ovarian carcinomas develop rapidly without a definite precursor lesion. Multiple genetic and epigenetic changes are involved in the molecular pathogenesis of serous adenocarcinoma, for example, high-grade serous carcinomas are characterized by the tumor suppressor gene TP53 mutations. They also have germline or somatic loss-of-function mutations in BRCA1 or BRCA2 or promoter methylation of BRCA1. Mucinous adenocarcinoma most probably arises via an adenoma-borderline tumor-carcinoma sequence. KRAS mutation (up to 75 %) and lack of TP53 mutations are common in mucinous tumors. Mutations of Wnt/CTNNB1 (beta-catenin) are common in endometrioid adenocarcinoma. Loss-of-function mutations of PIK3CA (phosphatidylinositol-4,5-bisphosphate 3-kinase, catalytic subunit alpha)/PTEN (phosphatase and tensin homolog) are common in low-grade endometrioid carcinoma [18]. In contrast, high-grade endometrioid carcinomas harbored TP53 mutations and lacked CTNNB1, PIK3CA, or PTEN mutations [18]. Mutations of PIK3CA are observed most frequently in clear cell carcinoma. Recent studies implicated a tumor suppressor gene ARID1A (AT-rich interactive domain 1A (SWI-like)) as frequently disrupted in endometriosis-associated ovarian cancer and clear cell and endometrioid adenocarcinomas. ARID1A plays a role in chromatin remodeling, which leads to cell cycle arrest and cell death in the event of DNA damage. The loss-of-function mutations of ARID1A may result in susceptibility to carcinogenesis through a defect in the repair or replication of damaged DNA. All atypical endometriosis and 86 % of non-atypical endometriosis lost ARID1A expression. ARIDA expression was retained in areas of endometriosis from sites distant from the malignant lesion [32]. These data suggest that loss of ARID1A expression occurs as a very early event in the endometriosis-atypical endometriosis sequence [33]. In endometriosis-associated ovarian cancer, clear cell carcinomas harbor frequent mutations of ARID1A and PIK3CA genes and moderate mutations of PPP2R1A (protein phosphatase 2, regulatory subunit A, alpha) and KRAS [32, 33], while endometrioid cancer harbors mutations of PTEN, CTNNB1, and KRAS [34, 35]. The investigators failed to identify one potential driver mutation in endometriosis-associated ovarian cancer samples. The development of cancer takes place in a multi-step process during which cells acquire a series of mutations, including ARID1A, PPP2R1A, PIK3CA, PTEN, KRAS, or Wnt/CTNNB1. These mutations may be significant factor for endometriosis-associated ovarian carcinogenesis, but various questions have yet to be answered. This model postulates the existence of additional mutations that establish carcinogenesis after acquisition of these mutations. Future studies will represent the remarkable genetic research achievements in the pathogenesis of endometriosis-associated ovarian cancer.
4 Pathogenesis of Endometriosis-Associated Ovarian Cancer
Epidemiologic studies account for the fact that endometriosis has been associated with an increased risk of epithelial ovarian cancer. Genome-wide studies demonstrate that endometriosis shares several genetic characteristics with ovarian cancer. The same pathophysiology (immune alterations, excess oxidative stress and inflammation, estrogen excess, and steroid hormone interaction) orchestrates the progression of endometriosis and its transformation to ovarian cancer. These facts show that some endometriosis has been shown to undergo malignant transformation. Ovarian cancer precursor lesions are known to be atypical endometriosis, which was identified in ~50 % of these histologic subtypes. Many investigators agree that the potential of invasive epithelial malignancies arises in atypical endometriosis [36–38]. Malignant transformation of endometriosis is not a single entity; rather it is a term defining a group of histologically distinct tumors. Each histologic subtype is clinically and genetically unique. The malignant transformation of endometriosis is classified into three groups: (i) epithelial ovarian cancers (endometrioid adenocarcinoma and clear cell carcinoma), (ii) other Müllerian-type tumors, including Müllerian-type mucinous borderline tumor and serous borderline tumor, and (iii) sarcomas such as adenosarcoma and endometrial stromal sarcoma in the female pelvic cavity [21]. Epithelial ovarian cancer is a popular tumor of malignant transformation [39].
Genome-wide studies have facilitated the genetic basis of pathogenesis and pathophysiology of endometriosis and endometriosis-associated ovarian cancer owing to the advent of new network-based analysis methods. Several investigators identified the endometriosis susceptibility genes and pathways that may be potential pathophysiology of endometriosis progression [3–16]. The endometriosis susceptibility genes were grouped into pathways or networks based on functional annotation. Interestingly, current molecular studies have sought to link endometriosis with endometriosis-associated ovarian cancer through pathways or networks related to inflammation, oxidative stress, and hyperestrogenism [40].
5 Inflammation and Immunity
Previous epidemiologic observations suggest that a number of factors that suppress ovulation or menstruation, including gravidity, breast feeding, oral contraception, and gynecologic surgery including hysterectomy and tubal ligation, reduced the risk of ovarian cancer. Endometriosis, perineal talc use, and asbestos exposure increase the risk, while aspirin or NSAIDs use decreases the risk. Ovulation, endometriosis, and talc use may be associated with inflammatory responses of the ovarian surface epithelium and pelvic peritoneum, contributing to ovarian tissue remodeling, proliferation, and tumorigenesis. These risk factors support that persistent pelvic inflammation may play a role in ovarian cancer risk [41]. In general, chronic inflammation has been implicated in a variety of cancers, including gastric cancer (Helicobacter pylori infection), colorectal cancer (ulcerative colitis and Crohn’s disease), lung cancer (tobacco smoking-associated chronic inflammation), malignant mesothelioma and lung cancer (asbestos exposure), hepatocellular carcinoma (hepatitis B and C infection), ovarian cancer (a long history of endometriosis), and others.
Recent advances in innate immunity illuminate the molecular mechanism underlying inflammation-induced carcinogenesis. Innate immunity is made possible by a network of pattern-recognition receptors (PRRs), which include the toll-like receptors (TLRs), Nod-like receptors (NLRs), RIG-like receptors (RLRs), and cytosolic DNA receptors. TLRs mediate interactions between environmental stimuli and innate immunity and trigger inflammatory signals. TLRs are involved in not only the host defense against microbial infections but also stimulation of tumor cell growth and carcinogenesis. Overexpression of PRRs in endometriosis stimulates chronic inflammation pathways, accelerates endometriosis proliferation, and subsequently causes carcinogenesis. Yamada et al. discussed the role of innate immunity in the pathogenesis of endometriosis-associated ovarian cancer, with respect to endogenous ligands, their PRRs, and their signaling pathways [42].
6 Oxidative Stress
Increased generation of reactive oxygen species (ROS) is implicated in the pathogenesis of a variety of human diseases, which include cancer, atherosclerosis, diabetes, neurodegenerative diseases, cardiovascular disease, and aging. Repetitive hemorrhage and the accumulation of heme and iron within endometriotic cysts and peritoneal cavity play a role in the development of ovarian cancer through the formation of ROS under a Fenton reaction [43, 44]. Excessive iron increases cancer risk by free radical-induced chromosomal instability. Persistent oxidative stress induced by endometriosis-dependent hemorrhage might be associated with carcinogenesis.
Recent studies have noted a set of genes that distinguished clear cell carcinoma from non-clear cell carcinoma and confirmed specific expression of a transcription factor, hepatocyte nuclear factor-1beta (HNF-1beta), in clear cell carcinoma, and genetic alteration may be involved in oxidative stress [45]. HNF-1beta is significantly upregulated in ovarian clear cell carcinoma and rarely expressed in non-clear cell carcinoma specimens [46]. Of the clear cell carcinoma susceptibility genes, 87 % are redox-related genes, including anti-oxidative and detoxification enzymes [45]. Forty-one percent of the genes upregulated in clear cell carcinoma samples are downstream targets of HNF-1beta [47]. HNF-1beta is thought to play a role in anti-apoptosis, detoxification, survival, cell cycle regulation, and glycogen synthesis. Sixty percent of the endometriosis cases also exhibited the overexpression of HNF-1beta [48]. Endometriosis has evolved adaptive mechanisms to cope with oxidative stress. Excess hemorrhage and iron can induce high levels of oxidative stress that may have deleterious effects on endometriotic cell growth. Endometriotic cells exhibit a higher production of HNF-1beta to detoxify ROS and survive under oxidative stress conditions. HNF-1beta also plays key roles in triggering DNA damage response without causing cell death and regulating timely cell cycle arrest. HNF-1beta upregulation is sufficient to accumulate the iron-induced genomic instability, which may be enhanced and accumulated with increasing cell passage. Genomic instability might be increased even further upon exposure to iron, ultimately resulting in carcinogenesis. Endometriotic cells have developed efficient ways to cope with oxidative stress and seemingly survive stressful periods by launching a minimal set of protection mechanisms and by temporarily bringing several key genes such as HNF-1beta. These data allow us to speculate that excess oxidative stress might be implicated in the development of endometriosis-associated clear cell carcinoma.
7 Estrogen
Endometriosis and endometrioid adenocarcinoma share a common hormonal mechanism. Hyperestrogenism is a common finding with development of estrogen-dependent lesions and is a significant risk factor for the development of cancer from endometriosis [49]. Endometrioid adenocarcinoma of the ovary and endometrium develops in the setting of excess endogenous and exogenous estrogen exposure. Estrogen drives cell proliferation and activates the PI3K and MAPK proliferative pathways, which are frequently dysregulated in cancer. Estrogen is supposed to participate in the early stages of endometrial tumorigenesis, through the accumulation of random genetic errors and increased telomerase activity. Genomic and nongenomic estrogen receptor (ER) signaling pathways play a role in the onset and development of tumors arising from or outside the reproductive system. Endometrioid adenocarcinoma of the ovary is predominantly positive for ER; however, the molecular link between estrogen and endometrial carcinogenesis remains poorly understood.
In contrast, clear cell carcinoma specifically exhibits negative ER expression and estrogen independency. The iron-mediated ROS oxidatively modifies genomic DNA and, subsequently, ER depletion may be observed, possibly through DNA methylation of the promoter region, histone deacetylation, heme and iron binding, chromatin remodeling, and ubiquitin ligase activity [50, 51]. ER is thought to be inactivated mainly through aberrant DNA methylation [52]. Loss of estrogen function may be a turning point in clear cell carcinoma progression and aggressiveness. Endometriosis-associated ovarian cancer has a dual pathway in carcinogenesis, estrogen-dependent ovarian carcinogenesis with an endometrioid morphology, and estrogen-independent, oxidative stress-dependent carcinogenesis with the clear cell morphology [53].
8 Conclusion
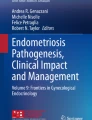
The endometriosis contains abundant iron due to repeated episodes of hemorrhage. Iron is a mutagenic and carcinogenic compound and causes oxidative stress due to generation of ROS. The iron-induced ROS signaling cascades can contribute to carcinogenesis via three major processes: step 1, by increasing oxidative stress, which facilitates the accumulation of somatic mutations and promotes DNA mutagenesis, histone modification, chromatin remodeling, and gene products activation/inactivation, thus contributing to endometriosis-associated ovarian cancer initiation; step 2, by creating a microenvironment that supports sustained growth, angiogenesis, migration, and invasion of cancer cells via estrogen-dependent mechanisms, thus supporting tumor progression of endometrioid adenocarcinoma; and step 3, by surviving stressful periods via temporarily HNF-1beta overexpression, thereby contributing to clear cell carcinoma progression (Fig. 29.1). The high incidence of malignant transformation in high-risk women with endometriosis (advancing age and tumor size 9 cm or greater in diameter) further supports intensive targeted surveillance.

The carcinogenic pathways. Endometriosis may contribute to carcinogenesis via three processes: step 1, by increasing oxidative stress, which facilitates the accumulation of somatic mutations, contributing to endometriosis-associated ovarian cancer initiation; step 2, by creating an estrogen-dependent microenvironment, supporting endometrioid adenocarcinoma progression; and step 3, by surviving stressful periods via temporarily HNF-1beta overexpression, thereby contributing to clear cell carcinoma progression
References
Giudice LC, Kao LC. Endometriosis. Lancet. 2004;364:1789–99.
Figueira PG, Abrão MS, Krikun G, Taylor HS. Stem cells in endometrium and their role in the pathogenesis of endometriosis. Ann N Y Acad Sci. 2011;1221:10–7.
Arimoto T, Katagiri T, Oda K, Tsunoda T, Yasugi T, Osuga Y, Yoshikawa H, Nishii O, Yano T, Taketani Y, Nakamura Y. Genome-wide cDNA microarray analysis of gene-expression profiles involved in ovarian endometriosis. Int J Oncol. 2003;22:551–60.
Bischoff F, Simpson JL. Genetics of endometriosis: heritability and candidate genes. Best Pract Res Clin Obstet Gynaecol. 2004;18:219–32.
Hu WP, Tay SK, Zhao Y. Endometriosis-specific genes identified by real-time reverse transcription-polymerase chain reaction expression profiling of endometriosis versus autologous uterine endometrium. J Clin Endocrinol Metab. 2006;91:228–38.
Burney RO, Talbi S, Hamilton AE, Vo KC, Nyegaard M, Nezhat CR, Lessey BA, Giudice LC. Gene expression analysis of endometrium reveals progesterone resistance and candidate susceptibility genes in women with endometriosis. Endocrinology. 2007;148:3814–26.
Zafrakas M, Tarlatzis BC, Streichert T, Pournaropoulos F, Wölfle U, Smeets SJ, Wittek B, Grimbizis G, Brakenhoff RH, Pantel K, Bontis J, Günes C. Genome-wide microarray gene expression, array-CGH analysis, and telomerase activity in advanced ovarian endometriosis: a high degree of differentiation rather than malignant potential. Int J Mol Med. 2008;21:335–44.
Honda H, Barrueto FF, Gogusev J, Im DD, Morin PJ. Serial analysis of gene expression reveals differential expression between endometriosis and normal endometrium. Possible roles for AXL and SHC1 in the pathogenesis of endometriosis. Reprod Biol Endocrinol. 2008;6:59.
Guo SW. Epigenetics of endometriosis. Mol Hum Reprod. 2009;15:587–607.
Kobayashi H, Yamada Y, Kanayama S, Furukawa N, Noguchi T, Haruta S, Yoshida S, Sakata M, Sado T, Oi H. The role of iron in the pathogenesis of endometriosis. Gynecol Endocrinol. 2009;25:39–52.
Pelch KE, Schroder AL, Kimball PA, Sharpe-Timms KL, Davis JW, Nagel SC. Aberrant gene expression profile in a mouse model of endometriosis mirrors that observed in women. Fertil Steril. 2010;93:1615–27.
Borghese B, Barbaux S, Mondon F, Santulli P, Pierre G, Vinci G, Chapron C, Vaiman D. Research resource: genome-wide profiling of methylated promoters in endometriosis reveals a subtelomeric location of hypermethylation. Mol Endocrinol. 2010;24:1872–85.
Evian Annual Reproduction (EVAR) Workshop Group 2010, Fauser BC, Diedrich K, Bouchard P, Domínguez F, Matzuk M, Franks S, Hamamah S, Simón C, Devroey P, Ezcurra D, Howles CM. Contemporary genetic technologies and female reproduction. Hum Reprod Update. 2011;17:829–47.
Nasu K, Kawano Y, Tsukamoto Y, Takano M, Takai N, Li H, Furukawa Y, Abe W, Moriyama M, Narahara H. Aberrant DNA methylation status of endometriosis: epigenetics as the pathogenesis, biomarker and therapeutic target. J Obstet Gynaecol Res. 2011;37:683–95.
Borghese B, Santulli P, Héquet D, Pierre G, de Ziegler D, Vaiman D, Chapron C. Genetic polymorphisms of DNMT3L involved in hypermethylation of chromosomal ends are associated with greater risk of developing ovarian endometriosis. Am J Pathol. 2012;180:1781–6.
Wu Y, Strawn E, Basir Z, Halverson G, Guo SW. Promoter hypermethylation of progesterone receptor isoform B (PR-B) in endometriosis. Epigenetics. 2006;1:106–11.
Munksgaard PS, Blaakaer J. The association between endometriosis and ovarian cancer: a review of histological, genetic and molecular alterations. Gynecol Oncol. 2012;124:164–9.
Kurman RJ, Shih IM. Molecular pathogenesis and extraovarian origin of epithelial ovarian cancer–shifting the paradigm. Hum Pathol. 2011;42:918–31.
Goodman MT, Shvetsov YB. Incidence of ovarian, peritoneal, and fallopian tube carcinomas in the United States, 1995–2004. Cancer Epidemiol Biomarkers Prev. 2009;18:132–9.
Haruta S, Furukawa N, Yoshizawa Y, Tsunemi T, Nagai A, Kawaguchi R, Tanase Y, Yoshida S, Kobayashi H. Molecular genetics and epidemiology of epithelial ovarian cancer. Oncol Rep. 2011;26:1347–56.
Higashiura Y, Kajihara H, Shigetomi H, Kobayashi H. Identification of multiple pathways involved in the malignant transformation of endometriosis. Oncol Lett. 2012;4:3–9.
Brinton LA, Gridley G, Persson I, Baron J, Bergqvist A. Cancer risk after a hospital discharge diagnosis of endometriosis. Am J Obstet Gynecol. 1997;176:572–9.
Ness RB, Cramer DW, Goodman MT, Kjaer SK, Mallin K, Mosgaard BJ, Purdie DM, Risch HA, Vergona R, Wu AH. Infertility, fertility drugs, and ovarian cancer: a pooled analysis of case–control studies. Am J Epidemiol. 2002;155:217–24.
Brinton LA, Lamb EJ, Moghissi KS, Scoccia B, Althuis MD, Mabie JE, Westhoff CL. Ovarian cancer risk associated with varying causes of infertility. Fertil Steril. 2004;82:405–14.
Borgfeldt C, Andolf E. Cancer risk after hospital discharge diagnosis of benign ovarian cysts and endometriosis. Acta Obstet Gynecol Scand. 2004;83:395–400.
Ness RB. Endometriosis and ovarian cancer: thoughts on shared pathophysiology. Am J Obstet Gynecol. 2003;189:280–94.
Purdie DM, Bain CJ, Siskind V, Russell P, Hacker NF, Ward BG, Quinn MA, Green AC. Hormone replacement therapy and risk of epithelial ovarian cancer. Br J Cancer. 1999;81:559–63.
Somigliana E, Vigano’ P, Parazzini F, Stoppelli S, Giambattista E, Vercellini P. Association between endometriosis and cancer: a comprehensive review and a critical analysis of clinical and epidemiological evidence. Gynecol Oncol. 2006;101(2):331–41.
Dinulescu DM, Ince TA, Quade BJ, Shafer SA, Crowley D, Jacks T. Role of K-ras and Pten in the development of mouse models of endometriosis and endometrioid ovarian cancer. Nat Med. 2005;11:63–70.
Kobayashi H, Sumimoto K, Moniwa N, Imai M, Takakura K, Kuromaki T, Morioka E, Arisawa K, Terao T. Risk of developing ovarian cancer among women with ovarian endometrioma: a cohort study in Shizuoka. Jpn Int J Gynecol Cancer. 2007;17:37–43.
Kobayashi H, Sumimoto K, Kitanaka T, Yamada Y, Sado T, Sakata M, Yoshida S, Kawaguchi R, Kanayama S, Shigetomi H, Haruta S, Tsuji Y, Ueda S, Terao T. Ovarian endometrioma–risks factors of ovarian cancer development. Eur J Obstet Gynecol Reprod Biol. 2008;138:187–93.
Wiegand KC, Shah SP, Al-Agha OM, Zhao Y, Tse K, Zeng T, Senz J, McConechy MK, Anglesio MS, Kalloger SE, Yang W, Heravi-Moussavi A, Giuliany R, Chow C, Fee J, Zayed A, Prentice L, Melnyk N, Turashvili G, Delaney AD, Madore J, Yip S, McPherson AW, Ha G, Bell L, Fereday S, Tam A, Galletta L, Tonin PN, Provencher D, Miller D, Jones SJ, Moore RA, Morin GB, Oloumi A, Boyd N, Aparicio SA, Shih IM, Mes-Masson AM, Bowtell DD, Hirst M, Gilks B, Marra MA, Huntsman DG. ARID1A mutations in endometriosis-associated ovarian carcinomas. N Engl J Med. 2010;363:1532–43.
Yamamoto S, Tsuda H, Takano M, Tamai S, Matsubara O. Loss of ARID1A protein expression occurs as an early event in ovarian clear-cell carcinoma development and frequently coexists with PIK3CA mutations. Mod Pathol. 2012;25:615–24.
Kolasa IK, Rembiszewska A, Janiec-Jankowska A, Dansonka-Mieszkowska A, Lewandowska AM, Konopka B, Kupryjańczyk J. PTEN mutation, expression and LOH at its locus in ovarian carcinomas. Relation to TP53, K-RAS and BRCA1 mutations. Gynecol Oncol. 2006;103:692–7.
Palacios J, Gamallo C. Mutations in the beta-catenin gene (CTNNB1) in endometrioid ovarian carcinomas. Cancer Res. 1998;58:1344–7.
Ogawa S, Kaku T, Amada S, Kobayashi H, Hirakawa T, Ariyoshi K, Kamura T, Nakano H. Ovarian endometriosis associated with ovarian carcinoma: a clinicopathological and immunohistochemical study. Gynecol Oncol. 2000;77:298–304.
Ballouk F, Ross JS, Wolf BC. Ovarian endometriotic cysts. An analysis of cytologic atypia and DNA ploidy patterns. Am J Clin Pathol. 1994;102:415–9.
Sato N, Tsunoda H, Nishida M, Morishita Y, Takimoto Y, Kubo T, Noguchi M. Loss of heterozygosity on 10q23.3 and mutation of the tumor suppressor gene PTEN in benign endometrial cyst of the ovary: possible sequence progression from benign endometrial cyst to endometrioid carcinoma and clear cell carcinoma of the ovary. Cancer Res. 2000;60:7052–6.
Brinton LA, Sakoda LC, Sherman ME, Frederiksen K, Kjaer SK, Graubard BI, Olsen JH, Mellemkjaer L. Relationship of benign gynecologic diseases to subsequent risk of ovarian and uterine tumors. Cancer Epidemiol Biomarkers Prev. 2005;14:2929–35.
Worley MJ, Welch WR, Berkowitz RS, Ng SW. Endometriosis-associated ovarian cancer: a review of pathogenesis. Int J Mol Sci. 2013;14:5367–79.
Ness RB, Grisso JA, Cottreau C, Klapper J, Vergona R, Wheeler JE, Morgan M, Schlesselman JJ. Factors related to inflammation of the ovarian epithelium and risk of ovarian cancer. Epidemiology. 2000;11:111–7.
Yamada Y, Shigetomi H, Onogi A, Haruta S, Kawaguchi R, Yoshida S, Furukawa N, Nagai A, Tanase Y, Tsunemi T, Oi H, Kobayashi H. New insights into pattern recognition receptors and their ligands in gynecologic pathologies. Hum Immunol. 2011;72:213–8.
Yamaguchi K, Mandai M, Toyokuni S, Hamanishi J, Higuchi T, Takakura K, Fujii S. Contents of endometriotic cysts, especially the high concentration of free iron, are a possible cause of carcinogenesis in the cysts through the iron-induced persistent oxidative stress. Clin Cancer Res. 2008;14:32–40.
Kobayashi H, Yamada Y, Kanayama S, Furukawa N, Noguchi T, Haruta S, Yoshida S, Sakata M, Sado T, Oi H. The role of hepatocyte nuclear factor-1beta in the pathogenesis of clear cell carcinoma of the ovary. Int J Gynecol Cancer. 2009;19:471–9.
Kajihara H, Yamada Y, Kanayama S, Furukawa N, Noguchi T, Haruta S, Yoshida S, Sado T, Oi H, Kobayashi H. Clear cell carcinoma of the ovary: potential pathogenic mechanisms. Oncol Rep. 2010;23:1193–203.
Tsuchiya A, Sakamoto M, Yasuda J, Chuma M, Ohta T, Ohki M, Yasugi T, Taketani Y, Hirohashi S. Expression profiling in ovarian clear cell carcinoma: identification of hepatocyte nuclear factor-1 beta as a molecular marker and a possible molecular target for therapy of ovarian clear cell carcinoma. Am J Pathol. 2003;163:2503–12.
Kobayashi H, Kajiwara H, Kanayama S, Yamada Y, Furukawa N, Noguchi T, Haruta S, Yoshida S, Sakata M, Sado T, Oi H. Molecular pathogenesis of endometriosis-associated clear cell carcinoma of the ovary. Oncol Rep. 2009;22:233–40.
Kato N, Sasou S, Motoyama T. Expression of hepatocyte nuclear factor-1beta (HNF-1beta) in clear cell tumors and endometriosis of the ovary. Mod Pathol. 2006;19:83–9.
Zanetta GM, Webb MJ, Li H, Keeney GL. Hyperestrogenism: a relevant risk factor for the development of cancer from endometriosis. Gynecol Oncol. 2000;79:18–22.
Tanase Y, Yamada Y, Shigetomi H, Kajihara H, Oonogi A, Yoshizawa Y, Furukawa N, Haruta S, Yoshida S, Sado T, Oi H, Kobayashi H. Modulation of estrogenic action in clear cell carcinoma of the ovary. Exp Ther Med. 2012;3:18–24.
Swedenborg E, Power KA, Cai W, Pongratz I, Rüegg J. Regulation of estrogen receptor beta activity and implications in health and disease. Cell Mol Life Sci. 2009;66:3873–94.
Suzuki F, Akahira J, Miura I, Suzuki T, Ito K, Hayashi S, Sasano H, Yaegashi N. Loss of estrogen receptor beta isoform expression and its correlation with aberrant DNA methylation of the 5′-untranslated region in human epithelial ovarian carcinoma. Cancer Sci. 2008;99:2365–72.
Mandai M, Yamaguchi K, Matsumura N, Baba T, Konishi I. Ovarian cancer in endometriosis: molecular biology, pathology, and clinical management. Int J Clin Oncol. 2009;14:383–91.
Acknowledgments
Grant support: Supported by Grant-in-Aid for Scientific Research from the Ministry of Education, Science, and Culture of Japan to the Department of Obstetrics and Gynecology, Nara Medical University (H. Kobayashi).
Conflict of Interest
The authors declare no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2014 Springer Japan
About this chapter
Cite this chapter
Kobayashi, H. (2014). Malignant Transformation of Endometriosis. In: Harada, T. (eds) Endometriosis. Springer, Tokyo. https://doi.org/10.1007/978-4-431-54421-0_29
Download citation
DOI: https://doi.org/10.1007/978-4-431-54421-0_29
Published:
Publisher Name: Springer, Tokyo
Print ISBN: 978-4-431-54420-3
Online ISBN: 978-4-431-54421-0
eBook Packages: MedicineMedicine (R0)