
Abstract
Childhood vaccinations are of substantial public health relevance and have contributed significantly to reduced mortality and morbidity from severe infectious diseases.
Persistent organic pollutants are industrially produced chemicals, which are highly persistent, bioaccumulative, and toxic to humans. As the immunological response to vaccinations is a feasible parameter and represents major immune functions, it is most relevant for the assessment of human immune suppression caused by such agents in large epidemiological studies.
This chapter focuses on the limited number of environmental pollutants for which such vaccination data exists, including polychlorinated biphenyls (PCBs) and perfluorinated alkylate substances (PFAS), which are described individually. In general, elevated exposures to these compounds were associated with reduced humoral immune response to routine childhood immunizations. The prenatal and early postnatal exposure to PCB were most immunotoxic, possible through toxicity toward the developing immune system of young infants, while the contemporary exposure to PFAS reduces the antibody levels in a more direct manner.
The presented results in this chapter might explain some of the wide variation in antibody responses to immunization and support the hypothesis that some people today could be immunocompromised because of their exposure to environmental pollutants. Due to their high persistence, PCBs and PFAS will remain widespread in the environment, but the presented evidence of immunotoxicity indicates that human exposure to these chemicals should be limited to protect the human immune system throughout its lifetime.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others

Keywords
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
1 Vaccinations
The immune system has evolved to combat the environmental influences to which humans are constantly exposed, such as bacteria, viruses, fungi, and parasites. Furthermore, immunization programs have helped the immune system to reach protection through vaccination against life-threatening diseases.
For generations, it has been known that there was no second occurrence after suffering from certain illnesses. The modern history of vaccination began in England in 1796, when Edward Jenner discovered that inoculation of children with cowpox virus prevented smallpox disease (André 2003; Hilleman 2000; Plotkin and Plotkin 2011). Subsequent development of vaccines against various bacteria and viruses led to substantial progress in prevention of infectious diseases, and today vaccinations are widely used and considered one of the greatest successes of medical science. Vaccination has led to the total extinction of smallpox and the nearly elimination of polio, which now only exists in a few remote areas in Asia.
In developed countries, the structured programs of vaccination of small children against severe childhood diseases such as diphtheria, tetanus, polio, pertussis, measles, rubella, and mumps have significantly reduced the mortality of infants as well as the infection-associated morbidity caused by these diseases. Furthermore, vaccinations against viruses such as hepatitis, yellow fever, tick-borne encephalitis, etc. have reduced the risk of traveling in endemic areas (André 2003).
In recent years, vaccines against microorganisms causing cancer, such as the human papillomavirus, have been evolved, and a lot of effort is directed against the development of vaccines against severe infections such as HIV and malaria (Plotkin and Plotkin 2011).
The common goal of vaccinations is to reduce the high risk of mortality or chronic disabilities caused by the natural diseases, which overcomes the side effects of vaccination. Furthermore, establishment of herd immunity, with most individuals in a population vaccinated against diseases, reduces the risk of epidemic outbreaks and thereby also indirectly protects unvaccinated individuals such as small infants and individuals with immunodeficiencies from transmission of the disease.
1.1 Immunological Control of Infections
Humans are constantly in contact with microorganisms, but the vast majority is prevented from causing infections due to intact epithelial barriers on the body’s surface. Microorganisms penetrating these barriers meet fixed mechanisms of the innate immune system, such as the complement system, phagocytosis from macrophages and neutrophils, and inflammatory cytokines, which will overcome most infections before they have caused symptoms. Medical practice is mostly concerned with diseases that results from the small proportion of infections that the innate immune system fails to terminate and for which the spread of the pathogen to secondary lymphoid tissues stimulates an adaptive immune response.
Upon the first encounter with a pathogen, a primary adaptive immune response is raised. This involves an extensive process in which pathogen-specific naïve T- and B-lymphocyte clones are selected, expanded, and differentiated into effector cells within the lymphoid tissue. Effector CD4+ Th1 cells and cytotoxic CD8+ T cells travel from the lymphoid tissue to the infected site and activate macrophages to destroy extracellular pathogens or kill infected human cells. Within the secondary lymphoid tissue, T cells activate pathogen-specific B cells and drive isotype switching and somatic hypermutation to produce high-affinity plasma cells, from whence secreted antibodies then travel to the site of infection.
In addition to successful clearance of the specific pathogen, an adaptive immune response also establishes a long-term protective immunity. The next encounter with a specific pathogen will provoke a faster and stronger response against the pathogen. This is produced by circulating antibodies and clones of long-lived memory B and T cells formed by the primary response and reactivated when confronted with the antigen. As a consequence, the infection is cleared quickly by the secondary response, with few or no symptoms of disease and little mortality from even life-threatening pathogens.
1.2 Immunological Stimulation by Immunizations and Vaccination Efficacy
Vaccinations are given to prime the human body against a specific pathogen, before the pathogen itself is encountered. Successful vaccination involves a range of key immunological processes involved in antibody formation. Establishment of long-lasting protective immunology depends on isotype switch and affinity maturation of B cells in the germinal center and on production of memory T and B lymphocytes, which are maintained throughout life and will be recruited upon renewed exposure to the antigen. Antibody titers can be used to measure any given vaccination’s efficacy (Fig. 8.1). An antibody concentration >0.1 IU/mL is considered essential to achieve full long-term protection against diphtheria and tetanus in accordance with the public health purpose of routine vaccinations . However, the immunological response to routine prophylactic vaccinations varies substantially, and the reasons for this wide variation are poorly understood apart from well-known immune deficiencies.

Antibody response against tetanus and diphtheria. Antibody response to vaccinations with tetanus and diphtheria. The antibody titers rise during the first weeks after vaccination and then gradually decline to a steady level
1.3 Vaccine Subtypes
Vaccines can be divided into live (attenuated) or inactivated vaccines. Attenuated vaccines cause a nonpathogenic infection (e.g., measles, rubella, mumps, and tuberculosis), mimicking a natural infection through replication of the microorganism within the host and presentation of antigens on MHC class I and II to the adaptive immune system, causing diverse and long-lasting immunity.
Inactivated vaccines consist of either dead microorganisms (killed bacteria or inactivated viruses, e.g., polio, cholera, and rabies) or components of microorganisms. Component vaccines contain purified components of inactivated microorganisms (e.g., influenza), recombinant antigens (e.g., hepatitis B), purified exotoxins processed with formaldehyde to make them nonpoisonous (e.g., tetanus, diphtheria), or conjugated vaccines of carbohydrates linked to a toxoid (e.g., pneumococcus). Component vaccines activate immunity against the specific antigen without copying the challenge of a natural pathogen. Even though adjuvant is added to increase the immunogenicity by stimulation of an inflammatory response and transportation of the antigen to the regional lymph nodes, nonliving vaccines are less effective than living vaccines, and repeated inoculations and boosters are often required to achieve the needed level of protection against microorganisms (Hilleman 2000; Plotkin 2014).
1.4 Use of Vaccination Efficacy for Epidemiological Studies of Immune Function
Findings identifying dose–response relationships, biological plausibility, and mode of action from experimental models of immune dysfunction caused by environmental pollutants may be telling, but they need to be verified in humans to assess the public health risk. Thus, epidemiological studies of immune dysfunction in exposed individuals are needed, as randomized studies of immunotoxicity are ethically unjustifiable. As such, longitudinal studies are preferable as they follow subjects for a sufficient time period to assess the health outcome of environmental pollutants. International guidelines recommend that the evaluation of immune-related health outcomes should be based on validated direct biological measures of exposure and effect and to a smaller extent on self-reported qualities, such as obtained by questionnaires and diaries (van Loveren et al. 1999; WHO 2012). In contrast to the findings from patients with severe defects in the immune system such as inborn errors or HIV infection, common clinical immune test can hardly detect potential mild-to-moderate states of immunodeficiency caused by immunotoxic agents. However, small changes in the immune system can be detected at a population level under the appropriate conditions. Antibody responses to vaccinations with standardized doses of foreign antigens are recommended as the best tool for evaluation of immune suppression, since antibody responses are measurable indicators of major immune system functions. Therefore, data from vaccination responses reflect the overall efficacy of the immune system to protect individuals from infections with pathogens beyond the specific vaccinations and represent the strongest evidence of immunosuppression (van Loveren et al. 1999; WHO 2012).
Most relevant for assessment of immunotoxic effects are primary immune responses to antigens to which the immunized persons have not previously encountered. This includes standardized pediatric immunizations for assessment of developmental immunotoxicity and vaccines against infections without prior exposure in adults (such as hepatitis B in non-epidemic areas) (Dietert 2008). Furthermore, well-known vaccines with availability to standardized methods for antibody assessment and extensive experience on vaccine efficacy are most suitable (Dietert 2008; Luster et al. 2005; van Loveren et al. 1999; WHO 2012).
2 Persistent Organic Pollutants
Toxic chemicals like groups of polychlorinated biphenyls (PCBs) and perfluorinated alkylate substances (PFAS) are considered persistent organic pollutant as noted under the Stockholm Convention as they are highly persistent and bioaccumulative in the environment. Many are now phased out from production due to their toxic effects, but are still widespread and found in humans, animals, and the environment. Besides being linked to human hepatotoxicity, developmental toxicity, hormonal effects, and a carcinogenic potency, some compounds have been found to cause immune dysfunction.
Immunotoxicology is defined as the study of adverse effects on the immune system resulting from occupational, environmental, or therapeutic exposure to agents suspected of toxicity toward the immune system. Due to its systemic distribution, the immune system is a moving toxicological target for interactions with organic pollutants (Dietert 2008). As human studies regarding quantitative exposure data and dose–response relationships are very limited, to expand our knowledge base, large epidemiological studies addressing the importance of environmental pollutants for human health have been carried out.
Immunological toxicity includes immune dysfunction and activation causing asthma , allergies, and autoimmune diseases as well as immune suppression with increased incidence or severity of infections and cancer. The immunosuppressive capacity of PCBs and PFAS has been investigated using cohort studies of vaccination efficacy conducted in children vaccinated according to their national vaccination program. These studies have addressed both the prenatal and postnatal exposure to potential immunotoxicants to establish their effect on both developmental and mature immunity.
When investigating childhood immunotoxicity , it is important to notice that the human immune system is developing throughout the fetal stage as well as postnatal. In the early gestational stage, hematopoietic stem cell formation, tissue migration, and progenitor cell expansion take place. The bone marrow and thymus are colonized late in prenatal life, while the development of the thymus includes both the late gestational period as well as early postnatal life. At birth, the child is still dependent on transferred immunity from the mother, as critical maturation of child’s capacity for immune responses and immunological memory is ongoing throughout the first year of life. Of special interest to vaccination studies, an infant can achieve adult levels of antibodies by approximately the end of the first year and can maintain a concentrated level of antibodies for several years (Dietert 2008; Holladay and Smialowicz 2000; Holsapple et al. 2004; Luster et al. 2005; WHO 2012).
Due to the timing of the development of immunity, the susceptibility of the immune system to environment pollutants may be greater during fetal and early postnatal development than later in life. As some persistent pollutants are transferred to the fetus during pregnancy, it is important to examine any long-lasting effects these chemicals may cause during this period of life as they could lead to irreversible dysfunctions. Furthermore, young children are most important for assessment of immunotoxicity in humans, as young children, apart from their increased dose sensitivity of immune-modulating drugs, have a short history of environmental exposures and lack the personal confounders found in adults (WHO 2012).
2.1 Polychlorinated Biphenyls
Polychlorinated biphenyls (PCBs) are organic compounds consisting of 209 different isomeric congeners with variable chlorination of a biphenyl group, which displays individual physicochemical properties depending on their particular chlorine substitution pattern (Safe 1994).
The production of PCBs, lasted until the late 1970s when it was banned in most Western countries, but many PCBs are resistant to degradation processes due to their inflammability, chemical stability, and lipophilic nature. They have been used as insulators in electrical equipment and fire retardants and persist widespread in global ecosystems. They are still found in air, water, and soil, as well as in fish , birds, animals, and humans, with a tendency to bioaccumulate in food chains and cause high tissue concentrations in top predator species (Atlas and Giam 1981; Bacon et al. 1992; Kannan et al. 1989; Safe 1994; Skaare et al. 2000).
Their long experimental half-lives and tendency to bioaccumulate in adipose tissues have raised concern of the possible hazards of PCBs to humans. One structural aspect considered to be very important in both biostability and toxicological properties of PCBs is the planarity of the congener. PCBs are divided into coplanar non-ortho PCBs and noncoplanar mono-, di-, tetra-, or hydra-ortho-substituted PCBs according to their chemical structure. The recent concern about immunotoxicity of PCBs is largely based on the dioxin -like coplanar congeners, which share a structural similarity with 2,3,7,8-tetrachlorodibenzo-p-dioxin (TCDD) and might produce similar health effects, including metabolic, reproductive, developmental, and immunotoxic responses (Van den Berg et al. 2006).
Most biological and toxic effects of the dioxin-like PCB congeners are mediated through the aryl hydrocarbon receptor (AhR), a cytosolic receptor protein that regulates the induction of cytochrome P450 enzymes (Safe 1994). The AhR is found in many cells of the immune system and shows high affinity for coplanar and mono-ortho-substituted PCB congeners as well as for TCDD (Safe 1994). In contrast, the non-dioxin-like ortho-substituted PCB congeners exhibit low affinity for the AhR and mediate toxicity via a less clearly described mechanism that involves altered signal transduction pathways and interruption of intracellular Ca2+ homeostasis (Fischer et al. 1998).
Dietary intake of especially fish and animal fats is assumed to be the main source of human exposure to PCB, and humans retain dozens of different PCB congeners in their adipose tissues, blood, and milk (Domingo and Bocio 2007; Liem et al. 2000; Schecter et al. 1994). Populations whose diet includes consumption of PCB-contaminated fish or seafood are still particularly affected, although concentrations of these substances in humans in general are declining (Dallaire et al. 2004; Fängström et al. 2005; Schecter et al. 2005).
Studies have shown that PCBs and dioxins cross the placenta and reach the fetus (Covaci et al. 2002). Additionally, children are exposed to PCBs by the mother through breastfeeding and from dietary intake when older (Brouwer et al. 1998).
2.1.1 Vaccination Efficacy
Due to their wide distribution and long half-lives of several years, chronic low-level PCB exposures remain a significant public health concern. Several studies have investigated the importance of PCB for humoral immune response to routine childhood immunizations in birth cohorts (summarized in Table 8.1). Vaccinations included attenuated virus vaccines of mumps, measles, and rubella, toxoid vaccines of tetanus and diphtheria, and the bacterial polysaccharide–protein conjugated vaccines of Haemophilus influenzae type b (Hib).
Weisglas-Kuperus et al. and Støvlevik et al. found negative effects of in utero PCB exposure on antibody levels against mumps, measles, and rubella at 3–3.5 years of age (Stølevik et al. 2013; Weisglas-Kuperus et al. 2000). In line with this, studies by Heilmann et al. in two cohorts showed reduced antibody responses against tetanus and diphtheria at age 5 years and 7.5 years in children with high PCB levels prenatally and early postnatal (Fig. 8.2). The serum PCB concentration at 18 months was especially significant in regard to the decrease in antibody concentrations, with an estimated 18 % lower diphtheria toxoid antibody level and estimated 22 % lower tetanus toxoid antibody level at age 7 years for each doubling of the PCB exposure at 18 months of age (Heilmann et al. 2006, 2010). In contrast to these findings, Jusko et al. did not show any associations of prenatal PCB exposure and antibody responses to immunizations with tetanus, diphtheria, and Hib at 6 months of age (Jusko et al. 2010).

Dose–effect PCB level in mother and antibody response in child. Dose–effect response between total PCB concentration in maternal serum and antibody responses to childhood vaccinations at age 18 months. Broken lines indicate the 95 % CI (Heilmann et al. 2006, reprinted with permission)
The levels of antibodies varied substantially, but most of the children had antibody concentrations well within the range assumed to provide long-term protection against the infectious diseases vaccinated against. However, in the largest Faroese study conducted by Heilmann et al., 26–37 % of children had diphtheria and tetanus toxoid antibody concentrations below the limit for clinically protection of 0.1 IU/ml before the booster vaccination at 5 years of age. The odds of an anti-diphtheria antibody concentration below a clinically protective level of 0.1 IU/L at age 5 years increased by about 30 % for a doubling of PCB concentrations in milk and 18-month serum (Heilmann et al. 2010). These findings were not reported elsewhere; however, the time from vaccination to antibody measurement differed, and the PCB levels in the Dutch, Slovakian, or Norwegian cohorts were lower than among the Faroese mothers and children due to the traditional habit of eating pilot whale blubber in the Faroese Islands (Grandjean et al. 1995; Weihe et al. 1996). Although the Faroese population has a substantially increased PCB exposure, these data suggest that possible adverse influences on the immune function may well occur also at lower exposure ranges prevalent worldwide.
Even though the published studies are not consistent regarding the effect of PCB to immune responses after specific vaccines, data from these studies taken together points to an adverse effect of PCB exposure on antibody responses to routine childhood vaccinations . Overall, these effects are consistent for both attenuated virus vaccinations and bacterial toxoid vaccinations, suggesting a depression of several components of the immune system.
Discrepancies between studies might be caused by differences in sample sizes and vaccines used (including adjuvants) and dissimilarities in determination of PCB exposure. The time of assessment of antibody response also have an impact. Jusko et al. explain their lack of associations between prenatal PCB exposure and antibody responses at 6 months to the immaturity of the immune system in young infants. However this study has general flaws in the assessment of the vaccination responses. The number of vaccinations differed from 1 to 2 in this study, and the timing of both vaccinations and collection of blood samples for antibody responses varied within the study population. As the vaccination responses were measured very shortly after vaccination, the resulting antibody levels might reflect the difference in individual immunization responses as well as the interindividual variation in timing of the blood sample collection.
Furthermore, the differences in findings from the vaccination studies suggest that the estimated effect on antibody concentrations depends on the time window that analysis represents. Data regarding prenatal PCB exposure have shown associations with some vaccinations, but not others. In the prospective follow-up studies, the highest levels of immunosuppressive associations were caused by serum levels of PCB at 18 months in the Faroese study. This suggests that PCB levels in the fetal stage and early childhood coincide with a highly vulnerable stage of immune system development and that the antibody response may be influenced by accumulated PCB burden from placental transfer and lactation during the early postnatal period.
2.1.2 Immunological Parameters in Humans
In line with the findings regarding childhood vaccinations , exposure to PCBs during pregnancy is found to be associated with immune-related health outcomes and immune functionality parameters in small children. Several studies report that PCB-exposed children have more childhood infections during infancy, preschool, and school age, including respiratory tract infections, gastroenteritis, exanthema subitum, recurrent middle ear infections, and chicken pox (Dallaire et al. 2004; Stølevik et al. 2011, 2013; Weisglas-Kuperus et al. 2000, 2004).
High prenatal PCB exposure in utero and early postnatal has been associated with a decreased thymus size among neonates born in an area with high environmental load of PCBs in Eastern Slovakia, suggesting that infant immune development might be altered by in utero exposure to PCB (Jusko et al. 2012). Mostly nonplanar PCBs were investigated, but concentrations of nonplanar PCBs are moderately correlated with dioxin -like activity in several populations. Therefore, the results could be supported by experimental studies in pregnant mice exposed for TCDD, in which offspring revealed decreases in thymic weight and cellularity (Fine et al. 1989). In addition, in vitro studies of TCDD have suggested a change in the kinetics of thymocyte maturation with skewing of the thymocyte differentiation toward the CD8+ phenotypically more mature TcR αβ+ T cells following exposure to PCBs and dioxins (Lai et al. 1998).
In addition to toxic effects on the thymus, high maternal and cord blood PCB levels have been associated with increased numbers of leukocytes, lymphocytes, and T cells, including cytotoxic T cells, memory T cells, TcR αβ+ T cells, and activated T cells, in infants and small children (Belles-Isles et al. 2002; Weisglas-Kuperus et al. 2000), although this was not confirmed by others (Glynn et al. 2008; Stølevik et al. 2013).
Additionally, a recent substudy within the Norwegian vaccination cohort linked high maternal PCB exposure during pregnancy to representation of immune-related genes at the transcriptomic levels in cord blood, which were also correlated to measles vaccination responses at 3 years of age. The involved genes include regulation of intracellular signaling cascades, lymphocyte activation and T-cell proliferation, cytokine production, and antigen presentation (Hochstenbach et al. 2012), which may further indicate immunosuppressive effects of prenatal exposure to PCBs.
The present findings associating early exposure to PCBs and reduced antibody response to immunizations together with increased risk of infections, decreased thymic volume, and altered composition of T-lymphocyte subsets are all in accordance with the proposed immunosuppressive properties of dioxins and dioxin-like PCBs. The findings of PCB-related impaired resistance to infections and impairment of lymphocyte function and antibody responses have also been demonstrated in animals (Ross et al. 1996). These results suggest that further efforts are needed to minimize the hazard from PCB exposure.
2.2 Perfluorinated Alkylate Substances
Perfluorinated alkylate substances (PFAS) are a group of chemicals with many important industrial and manufacturing applications, which are used widely in surfactants and repellents in food packaging and textile impregnation (Vestergren and Cousins 2009). PFAS comprise a heterogeneous class of chemicals consisting of an alkyl chain (4–14 carbons), which is partially or fully fluorinated and have different functional groups attached. As a group, they display unique characteristics such as chemical and thermal stability, low surface free energy, and surface-active properties.
The most studied compounds to date are perfluoroalkyl sulfonic acids and perfluoroalkyl carboxylic acids. Among these, perfluorooctane sulfonic acid (PFOS) and perfluorooctanoic acid (PFOA) are of greatest concern due to their high level of persistence in the environment.
Perfluorooctane sulfonyl fluorides and perfluoroalkyl carboxylic acids have been produced with increasing intensities since the 1950s. The production of PFOS and related compounds were phased out by the major global manufacturer in 2002, resulting in a rapid decrease in release of these substances; the use of PFOS also is now restricted in the USA and the European Union due to their persistency and toxicity. The production of perfluoroalkyl carboxylic acids is however still ongoing, although several major PFOA-producing companies have committed to reduce their emissions. The historical releases of PFOS, PFOA, and related agents to land, air, and ground and surface water during production and use have caused dispersal to the global environment, especially in the oceans. Additionally, both PFOS and PFOA can be generated through environmental degradation processes of commercially synthesized precursors (Paul et al. 2009; Wang et al. 2014).
As several PFAS are highly persistent substances due to a strong carbon–fluorine bond, they remain a major environmental concern. PFAS are commonly detected in wildlife and have been demonstrated to bioaccumulate in fish all over the globe (Suja et al. 2009). It has been shown that the longer the perfluorinated carbon chains (>C5), the stronger the persistence and strength of binding to proteins is and the more bioaccumulative they become (Martin et al. 2003).
Analyses of occupational and nonoccupational human blood samples from all over the world contain PFAS at detectable levels, in which PFOS is the most dominant compound followed by PFOA and perfluorohexane sulfonic acid (PFHxS) (Calafat et al. 2007; Kannan et al. 2004; Toms et al. 2014; Weihe et al. 2008). Analyses conducted by the Centers for Disease Control and Prevention in the USA show that PFOS and PFOA are detectable in virtually all Americans (Calafat et al. 2007), with children often showing higher serum concentrations than adults (Kato et al. 2009). Studies of retired workers from PFAS production facilities show a long elimination half-life of 5.4 years for PFOS, 3.8 years for PFOA, and 8.5 years for PFHxS (Olsen et al. 2007).
Dietary intake is suspected to be the dominant cause of human PFAS exposure, and elevated concentrations of PFAS are especially associated with consumption of seafood and meat as PFAS pile up in proteins (Berger et al. 2009, 2014; Fromme et al. 2009; Haug et al. 2010). However, PFAS have also been detected in other food items, where they could be transferred from packaging or preparation with PFAS-contaminated applications in addition to bioaccumulation. Dust in the indoor environment may also be an important contributor to PFAS exposure (Fromme et al. 2009). Early-life exposure occurs through placental transfer from the mother during pregnancy as well as through lactation postnatal (Liu et al. 2011; Needham et al. 2011; Vestergren and Cousins 2009). Therefore, fetuses and infants are exposed to these compounds at critical developmental stages of the immune system.
2.2.1 Vaccination Studies
A study by Grandjean et al. has investigated the influence of PFAS on antibody responses after childhood immunizations (Grandjean et al. 2012). The study focused on the homogenous fishing community of the Faroe Islands in the North Atlantic Sea, where frequent intake of marine food is associated with increased exposures to PFAS (Weihe et al. 2008). A birth cohort of 587 consecutive singleton births was included and followed for 7 years. All children were vaccinated according to the official Faroese vaccination program, which includes vaccinations against diphtheria and tetanus at age 3, 5, and 12 months and a booster vaccination at age 5 years. Exposure to PFAS was assessed prenatally from analyses of serum from the mother during pregnancy and from the child at age 5 years before the booster vaccination, and antibody responses were measured at age 5 years prebooster, approximately 4 weeks after the booster, and at age 7 years. Similar to findings from other locations, the highest serum concentrations of PFAS were PFOS, PFOA, and PFHxS, which all were interrelated within the sample, but showed only weak associations between prenatal and postnatal exposures.
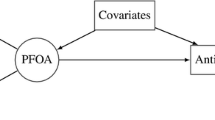
Antibody responses against diphtheria and tetanus were conducted at age 5 years before the booster, approximately 4 weeks after the booster, and at age 7 years. Among PFAS in maternal pregnancy serum, PFOS showed the strongest negative correlations with antibody concentrations at age 5 years. In a structural equation model adjusting for age, sex, and type of booster vaccination, a twofold greater concentration of the three major PFAS in child serum at age 5 years was associated with a halving of the antibody concentration (Fig. 8.3). Furthermore, a twofold increase in PFOS and PFOA concentrations at age 5 years was associated with odds ratios 2.38 and 4.20 for having antibody concentrations below the clinically protective level of 0.1 IU/mL for tetanus and diphtheria at age 7 years, respectively. Data presented in this study suggest a decreased effect of routine childhood vaccines in children aged 5 and 7 years with elevated exposures to PFAS. This may reflect a more general immune system deficit caused by exposure to PFAS (Grandjean et al. 2012).

Dose–effect between PFOS exposure and antibody response. Dose–effect response between PFOS exposure at age 5 years and antibody responses to childhood vaccinations with diphtheria at 7 years. Lines indicate the 95 % CI. The vertical bars on the horizontal scale indicate individual observations (Grandjean et al. 2012, with permission)
Based on the human immunotoxicity data from the Faroese cohort, calculations of benchmark doses have been conducted. It relies on the serum PFAS measurements at age 5 and the serum concentrations of specific antibodies 2 years later. Under different linear assumptions regarding dose dependence of the effects, benchmark dose levels were about 0.13 ng/mL serum for PFOS and 0.03 ng/mL serum for PFOA (Grandjean and Budtz-Jørgensen 2013). These doses are below most serum concentrations reported in recent population studies (Calafat et al. 2007; Kannan et al. 2004; Toms et al. 2014; Weihe et al. 2008). When converted to approximate exposure limits for drinking water, current limits appear to be several hundredfold too high in light of the observed immunotoxicity associated with PFAS exposure (Grandjean and Budtz-Jørgensen 2013). Furthermore, the human exposure to PFAS exceeds in several locations.
The Faroese results have been supported by the only other study regarding PFAS exposure and childhood vaccinations conducted in Norway by Granum et al. Prenatal PFAS exposure and antibody responses to childhood vaccinations at age 3 years were analyzed in 56 children. Vaccination included tetanus and Haemophilus influenzae type b given at ages 3, 5, and 12 months and measles and rubella given at 15 months of age. Increased concentrations of PFOA, PFHxS, perfluorononanoate (PFNA), and PFOS were significantly associated with reduced levels of anti-rubella antibodies in children at 3 years of age, with the highest estimated strength of association for PFNA and the lowest for PFOS. No significant associations were found between the concentrations of PFAS and antibody response to the other vaccines (Granum et al. 2013). Although a discrepancy of results regarding the influence of PFAS and tetanus response exists between the two studies, this study in a very limited number of children in general supports that prenatal exposure to PFAS may suppress responses to some childhood vaccines.
Furthermore, a study of humoral immune response to the seasonal influenza vaccination in 403 adults exposed to PFOA through contaminated drinking water in the USA has recently been published by Looker et al. The authors found evidence of a reduced antibody response 3 weeks after immunization with the influenza strain A/H3N2 in adults with higher PFOA concentrations. This response was reflected in titer rise, titer ratio, and long-term seroprotection after vaccination, although not seroconversion. No associations were found for PFOS exposure or for the response to the influenza serotypes A/H1N1 (swine flu) and influenza B. Even though these results are very supportive of the immunosuppressive effect of PFAS, especially since the antibody responses involved a mixture of primary and secondary reactions as all participants had titers for some of these common viruses prior to the immunization (Looker et al. 2014).
2.2.2 Immunological Parameters in Humans
Epidemiologic data related to PFAS exposure and immunotoxicity in humans are limited. The effect of prenatal PFAS exposure has been investigated with regard to specific childhood infections. In a Danish study of 14,000 children, prenatal exposure to PFOS and PFOA at approximately 8 weeks of pregnancy was not associated with increased risk of infectious diseases leading to hospitalization in the first 8 years of childhood (Fei et al. 2010). Similar to this, no associations were found between PFAS exposure during pregnancy and occurrence of middle ear infection in 18-month-old Japanese children (Okada et al. 2012). However, a positive association between prenatal exposure to PFAS and the self-reported number of episodes of common cold and gastroenteritis, but not middle ear infection, during the first 3 years of life was found in a small Norwegian study (Granum et al. 2013). In adults, no associations were found between PFAS levels and recent self-reported cold or influenza episodes (Looker et al. 2014).
However, occurrence of specific common infections may be a less sensitive or appropriate test of the presence of immune system dysfunction than immunization responses, as these infections are very prevalent and multiple social and demographic factors could affect the results.
The C8 Health Project investigated immune markers in blood from healthy individuals exposed to PFOA-contaminated drinking water for at least 1 year due to residency in the vicinity of a PFOA manufacturing site in the USA. High serum levels of PFOA were significantly associated with lower serum concentrations of C-reactive protein, total IgA, and total IgE (in females only), though not with IgG levels. Furthermore, increasing concentrations of PFOA showed a positive relationship with total antinuclear antibodies, which may indicate an increase in the risk of autoimmune diseases (Fletcher et al. 2009).
Corresponding to this, small changes in serum immunoglobulin levels have been reported in workers with occupational exposure to PFOA (Costa et al. 2009). Although supportive of immunosuppression, these basic tests cannot be considered as either sensitive or specific for immunotoxicity or predictive enough of an adverse effect of the immune system (van Loveren et al. 1999).
2.2.3 Animal Models of Immunotoxicity
Although confirmation of the findings from immunization studies in human studies is sparse, immunotoxicity of PFAS has been demonstrated in rodent, avian, and reptilian models as well as in mammalian and nonmammalian wildlife, affecting both cellular and humoral immunity (DeWitt et al. 2012).
High-dose dietary treatment of mice with PFOS or PFOA has been shown to cause atrophy of the thymus and spleen, decreased thymocyte and splenocyte counts, as well as significantly reduced numbers of bone marrow cells and myeloid cells, pro-/pre-B cells, immature B cells, and early mature B cells. These adverse effects were reversed partially or completely after withdrawal of these compounds (Qazi et al. 2012; Yang et al. 2000).
Furthermore, oral PFOS and PFOA exposure in mice has been found to cause severe suppression of the adaptive immune system in several studies. Findings include decreased numbers of immunoglobulin-producing splenic cells and a dose-dependent reduction in plasma levels of specific IgM and IgG upon immunization with horse or sheep red blood cells in PFOA-exposed mice. The immunosuppressive effect of PFOA appeared to recover following the administration of normal feeding (Dewitt et al. 2008; Yang et al. 2002).
Additionally, immune suppression has been found in mice exposed to PFOS in doses equivalent to the high end of nonoccupational exposure levels in humans. Alteration included especially suppression of specific IgM production by the plaque-forming cell response, a functional assay revealing the attack, and destruction of an antigen by antibodies. Production of both T-cell-dependent and T-cell-independent antibodies was suppressed, suggesting that B cells or antigen-presenting cells might be the specific target of PFOS (Peden-Adams et al. 2008). PFOS exposure in mice has also been associated with reduced host defense to influenza A virus infection, resulting in increased weight loss and reduced survival (Guruge et al. 2009). Additionally, cytokine expression and signaling related to inflammation and T-cell responses are altered by exposure to PFAS (DeWitt et al. 2012).
The importance of in utero exposure to PFAS and immunotoxicity has been investigated in two mice studies with different conclusions. Prenatal PFOS exposure was shown to suppress T-cell-dependent IgM antibody responses upon immunization in male offspring (Keil et al. 2008), although this was not confirmed for PFOA by others (Hu et al. 2010).
Taken together, experimental studies support an increased susceptibility to pathogens due to exposure to PFAS.
2.2.4 Molecular Mechanisms Involved in Immunosuppression by PFAS
The molecular mode of action of PFAS-induced immune suppression has been investigated by examining essential cell populations as well as cell signaling and activation. IgM secretion by B lymphocytes is controlled through production of IL-6. The onset of inflammatory gene expression is driven by the nuclear transcription factor NF-κB, whose transcriptional activity is regulated at multiple levels. In B cells, engagement of CD40 by its ligand leads to signaling through c-Jun and NF-κB, with subsequent IL-6 production (Baccam et al. 2003). This process is critical for humoral responses to T-dependent antigens and results in B-cell proliferation, differentiation, and IL-6 stimulation of immunoglobulin production (Pérez-Melgosa et al. 1999).
Current evidence suggests that the immunotoxic mechanisms of PFAS involve interaction with peroxisome proliferator-activated receptors (PPARs) as well as an PPAR-independent pathways (DeWitt et al. 2009, 2012). In vitro stimulation of human peripheral blood leukocytes with lipopolysaccharide (LPS) in the presence of PFAS for 24–72 hours showed a dose-dependent suppression of TNF-α and IL-6 production. Furthermore, in vitro exposure to PFAS inhibited production of the regulatory cytokines IL-4 and IL-10. The immunotoxic effect of PFOS was PPAR independent through interference with LPS-induced I-κB degradation, NF-κB transactivation, and DNA binding. In contrast, PFOA acted through PPAR to prevent p65 phosphorylation and NF-κB-mediated transcription (Corsini et al. 2011). Both mechanisms of action could theoretically lead to reduced antibody secretion by B lymphocytes, although further evidence for this is needed.
3 Perspectives
Vaccination is a mainstay in modern prevention of infectious diseases. While antibody responses of the average child to routine prophylactic immunizations can vary substantially, the reasons for poor responses are poorly understood, though exposure to environmental pollutants may account for at least some of the variation.
The presented studies provide epidemiological evidence for an association between exposure to persistent organic pollutants and a reduced humoral immune response to routine childhood vaccinations . Specifically, PCB reduces the immune response perinatally and early postnatal and is suspected to be toxic to the development of thymic function. PFAS, whereas, reduce the antibody levels in a more direct manner. The results are supported by animals and cellular studies, although a clear mechanism of action has not yet been demonstrated for all compounds.
The children examined came from population-based birth cohorts and were overall in good health. Although the changes in antibody response are subtle, they could become clinically important when the immune function is challenged by other risk factors such as preterm birth, chronic infections, increasing age, or competing diseases. Furthermore, high exposure levels in populations at risk may hinder a long-term protective immune response and increase the risk of a child not being protected against severe infections, despite a full schedule of vaccinations . In addition, even slight impairments could be important at a population level, e.g., if the herd immunity fails and epidemics of highly infectious and pathogenic infections brake out. In countries without access to routine pediatric immunizations, tetanus, diphtheria, measles, mumps, and rubella still give rise to increased levels of childhood mortality and morbidity.
In addition, one should keep in mind that antibody responses to standardized antigen stimulations reflect the overall efficacy of the immune system in relation to infections, including antigen presentation and T- and B-lymphocyte function. Therefore, the presented immune suppression may also increase children’s susceptibility to common infections, as have been suggested for PCB in some human studies. Therefore, even the small changes in immune function, suggested by the presented vaccination data, could be clinically important and might affect both the general health of children and the degree of protection against infectious diseases that vaccination provides.
Some of the immunotoxic effects from the immunization studies are revealed in children exposed to immunotoxicants through perinatal and early postnatal exposure, while others are associated with concentrations at the time of vaccination. The immune function returns to normal following exposure to immunosuppressive drugs in adults, especially if the drugs do not affect precursor or stem cells. However, the special concerns of low-level exposure to immunotoxicants during the development of the immune system are that developmental immunity may be more sensitive to the dose of immunotoxicants and that an early-life insult prenatally or early postnatal might cause immune defects on a permanent basis, leading to reduced host resistance in children and adults.
4 Conclusion
In conclusion, vaccination efficacy is found to be the most relevant parameter for assessment of immune suppression by environmental persistent pollutants. Results arising from vaccination studies in children support the hypothesis that some people today could be immunocompromised because of exposure to environmental pollutants such as PCBs and PFAS. In contrast to investigations from the presented study, human populations will often be exposed to a mixture of immunomodulating agents, which may in combination cause even more severe effects on the immune system than seen in these studies. While PCBs have been banned since the 1970s and are now found at reduced levels, the production of PFAS has just recently been limited. The persistence of these compounds means that they will still be widespread in the environment and in humans for a long period of time. However, the presented findings suggest that efforts must be stepped up to reduce exposure levels to protect the human immune systems from these as well as other potent immunotoxicants.
References
André FE (2003) Vaccinology: past achievements, present roadblocks and future promises. Vaccine 21:593–595
Atlas E, Giam CS (1981) Global transport of organic pollutants: ambient concentrations in the remote marine atmosphere. Science 211:163–165
Baccam M, Woo S-Y, Vinson C, Bishop GA (2003) CD40-mediated transcriptional regulation of the IL-6 gene in B lymphocytes: involvement of NF-kappa B, AP-1, and C/EBP. J Immunol 170:3099–3108
Bacon CE, Jarman WM, Costa DP (1992) Organochlorine and polychlorinated biphenyl levels in pinniped milk from the Arctic, the Antarctic. Chemosphere 24:779–791
Belles-Isles M, Ayotte P, Dewailly E, Weber J-P, Roy R (2002) Cord blood lymphocyte functions in newborns from a remote maritime population exposed to organochlorines and methylmercury. J Toxicol Environ Health A 65:165–182
Berg V, Nøst TH, Huber S et al (2014) Maternal serum concentrations of per- and polyfluoroalkyl substances and their predictors in years with reduced production and use. Environ Int 69:58–66
Berger U, Glynn A, Holmström KE, Berglund M, Ankarberg EH, Törnkvist A (2009) Fish consumption as a source of human exposure to perfluorinated alkyl substances in Sweden – analysis of edible fish from Lake Vättern and the Baltic Sea. Chemosphere 76:799–804
Brouwer A, Ahlborg UG, van Leeuwen FX, Feeley MM (1998) Report of the WHO working group on the assessment of health risks for human infants from exposure to PCDDs, PCDFs and PCBs. Chemosphere 37:1627–1643
Calafat AM, Kuklenyik Z, Reidy JA, Caudill SP, Tully JS, Needham LL (2007) Serum concentrations of 11 polyfluoroalkyl compounds in the U.S. Population: data from the National Health and Nutrition Examination Survey (NHANES) 1999–2000. Environ Sci Technol 41:2237–2242
Corsini E, Avogadro A, Galbiati V, Dell’Agli M, Marinovich M, Galli CL, Germolec DR (2011) In vitro evaluation of the immunotoxic potential of perfluorinated compounds (PFCs). Toxicol Appl Pharmacol 250:108–116
Costa G, Sartori S, Consonni D (2009) Thirty years of medical surveillance in perfluooctanoic acid production workers. J Occup Environ Med 51:364–372
Covaci A, Jorens P, Jacquemyn Y, Schepens P (2002) Distribution of PCBs and organochlorine pesticides in umbilical cord and maternal serum. Sci Total Environ 298:45–53
Dallaire F, Dewailly E, Muckle G, Vézina C, Jacobson SW, Jacobson JL, Ayotte P (2004) Acute infections and environmental exposure to organochlorines in Inuit infants from Nunavik. Environ Health Perspect 112:1359–1365
Dewitt JC, Copeland CB, Strynar MJ, Luebke RW (2008) Perfluorooctanoic acid-induced immunomodulation in adult C57BL/6J or C57BL/6N female mice. Environ Health Perspect 116:644–650
DeWitt JC, Shnyra A, Badr MZ et al (2009) Immunotoxicity of perfluorooctanoic acid and perfluorooctane sulfonate and the role of peroxisome proliferator-activated receptor alpha. Crit Rev Toxicol 39:76–94
DeWitt JC, Peden-Adams MM, Keller JM, Germolec DR (2012) Immunotoxicity of perfluorinated compounds: recent developments. Toxicol Pathol 40:300–311
Dietert RR (2008) Developmental immunotoxicology (DIT): windows of vulnerability, immune dysfunction and safety assessment. J Immunotoxicol 5:401–412
Domingo JL, Bocio A (2007) Levels of PCDD/PCDFs and PCBs in edible marine species and human intake: a literature review. Environ Int 33:397–405
Fängström B, Strid A, Grandjean P, Weihe P, Bergman A (2005) A retrospective study of PBDEs and PCBs in human milk from the Faroe Islands. Environ Health 4:12
Fei C, McLaughlin JK, Lipworth L, Olsen J (2010) Prenatal exposure to PFOA and PFOS and risk of hospitalization for infectious diseases in early childhood. Environ Res 110:773–777
Fine JS, Gasiewicz TA, Silverstone AE (1989) Lymphocyte stem cell alterations following perinatal exposure to 2,3,7,8-tetrachlorodibenzo-p-dioxin. Mol Pharmacol 35:18–25
Fischer LJ, Seegal RF, Ganey PE, Pessah IN, Kodavanti PR (1998) Symposium overview: toxicity of non-coplanar PCBs. Toxicol Sci 41:49–61
Fletcher T, Steenland K, Savitz D (2009) C8 Science Panel: Status Report: PFOA and immune biomarkers in adults exposed to PFOA in drinking water in the mid Ohio valley. Available: http://www.c8sciencepanel.org/index.html. Accessed on Dec 2014
Fromme H, Tittlemier SA, Völkel W, Wilhelm M, Twardella D (2009) Perfluorinated compounds–exposure assessment for the general population in Western countries. Int J Hyg Environ Health 212:239–270
Glynn A, Thuvander A, Aune M, Johannisson A, Darnerud PO, Ronquist G, Cnattingius S (2008) Immune cell counts and risks of respiratory infections among infants exposed pre- and postnatally to organochlorine compounds: a prospective study. Environ Health 7:62
Grandjean P, Budtz-Jørgensen E (2013) Immunotoxicity of perfluorinated alkylates: calculation of benchmark doses based on serum concentrations in children. Environ Health 12:35
Grandjean P, Weihe P, Needham L, Burse V, Patterson DJ, Sampson E, Jørgensen P, Vahter M (1995) Relation of a seafood diet to mercury, selenium, arsenic, and polychlorinated biphenyl and other organochlorine concentrations in human milk. Environ Res 71:29–38
Grandjean P, Andersen EW, Budtz-Jørgensen E, Nielsen F, Mølbak K, Weihe P, Heilmann C (2012) Serum vaccine antibody concentrations in children exposed to perfluorinated compounds. JAMA 307:391–397
Granum B, Haug LS, Namork E et al (2013) Pre-natal exposure to perfluoroalkyl substances may be associated with altered vaccine antibody levels and immune-related health outcomes in early childhood. J Immunotoxicol 10:373–379
Guruge KS, Hikono H, Shimada N, Murakami K, Hasegawa J, Yeung LWY, Yamanaka N, Yamashita N (2009) Effect of perfluorooctane sulfonate (PFOS) on influenza A virus-induced mortality in female B6C3F1 mice. J Toxicol Sci 34:687–691
Haug LS, Thomsen C, Brantsaeter AL et al (2010) Diet and particularly seafood are major sources of perfluorinated compounds in humans. Environ Int 36:772–778
Heilmann C, Grandjean P, Weihe P, Nielsen F, Budtz-Jørgensen E (2006) Reduced antibody responses to vaccinations in children exposed to polychlorinated biphenyls. PLoS Med 3:e311
Heilmann C, Budtz-Jørgensen E, Nielsen F, Heinzow B, Weihe P, Grandjean P (2010) Serum concentrations of antibodies against vaccine toxoids in children exposed perinatally to immunotoxicants. Environ Health Perspect 118:1434–1438
Hilleman MR (2000) Vaccines in historic evolution and perspective: a narrative of vaccine discoveries. Vaccine 18:1436–1447
Hochstenbach K, van Leeuwen DM, Gmuender H et al (2012) Toxicogenomic profiles in relation to maternal immunotoxic exposure and immune functionality in newborns. Toxicol Sci 129:315–324
Holladay SD, Smialowicz RJ (2000) Development of the murine and human immune system: differential effects of immunotoxicants depend on time of exposure. Environ Health Perspect 108(Suppl):463–473
Holsapple MP, Paustenbach DJ, Charnley G, West LJ, Luster MI, Dietert RR, Burns-Naas LA (2004) Symposium summary: children’s health risk–what’s so special about the developing immune system? Toxicol Appl Pharmacol 199:61–70
Hu Q, Strynar MJ, DeWitt JC (2010) Are developmentally exposed C57BL/6 mice insensitive to suppression of TDAR by PFOA? J Immunotoxicol 7:344–349
Jusko TA, De Roos AJ, Schwartz SM et al (2010) A cohort study of developmental polychlorinated biphenyl (PCB) exposure in relation to post-vaccination antibody response at 6-months of age. Environ Res 110:388–395
Jusko TA, Sonneborn D, Palkovicova L, Kocan A, Drobna B, Trnovec T, Hertz-Picciotto I (2012) Pre- and postnatal polychlorinated biphenyl concentrations and longitudinal measures of thymus volume in infants. Environ Health Perspect 120:595–600
Kannan N, Tanabe S, Ono M, Tatsukawa R (1989) Critical evaluation of polychlorinated biphenyl toxicity in terrestrial and marine mammals: increasing impact of non-ortho and mono-ortho coplanar polychlorinated biphenyls from land to ocean. Arch Environ Contam Toxicol 18:850–857
Kannan K, Corsolini S, Falandysz J et al (2004) Perfluorooctanesulfonate and related fluorochemicals in human blood from several countries. Environ Sci Technol 38:4489–4495
Kato K, Calafat AM, Wong L-Y, Wanigatunga AA, Caudill SP, Needham LL (2009) Polyfluoroalkyl compounds in pooled sera from children participating in the National Health and Nutrition Examination Survey 2001–2002. Environ Sci Technol 43:2641–2647
Keil DE, Mehlmann T, Butterworth L, Peden-Adams MM (2008) Gestational exposure to perfluorooctane sulfonate suppresses immune function in B6C3F1 mice. Toxicol Sci 103:77–85
Lai ZW, Fiore NC, Gasiewicz TA, Silverstone AE (1998) 2,3,7,8-Tetrachlorodibenzo-p-dioxin and diethylstilbestrol affect thymocytes at different stages of development in fetal thymus organ culture. Toxicol Appl Pharmacol 149:167–177
Liem AK, Fürst P, Rappe C (2000) Exposure of populations to dioxins and related compounds. Food Addit Contam 17:241–259
Liu J, Li J, Liu Y, Chan HM, Zhao Y, Cai Z, Wu Y (2011) Comparison on gestation and lactation exposure of perfluorinated compounds for newborns. Environ Int 37:1206–1212
Looker C, Luster MI, Calafat AM, Johnson VJ, Burleson GR, Burleson FG, Fletcher T (2014) Influenza vaccine response in adults exposed to perfluorooctanoate and perfluorooctanesulfonate. Toxicol Sci 138:76–88
Luster MI, Johnson VJ, Yucesoy B, Simeonova PP (2005) Biomarkers to assess potential developmental immunotoxicity in children. Toxicol Appl Pharmacol 206:229–236
Martin JW, Mabury SA, Solomon KR, Muir DCG (2003) Bioconcentration and tissue distribution of perfluorinated acids in rainbow trout (Oncorhynchus mykiss). Environ Toxicol Chem 22:196–204
Needham LL, Grandjean P, Heinzow B et al (2011) Partition of environmental chemicals between maternal and fetal blood and tissues. Environ Sci Technol 45:1121–1126
Okada E, Sasaki S, Saijo Y et al (2012) Prenatal exposure to perfluorinated chemicals and relationship with allergies and infectious diseases in infants. Environ Res 112:118–125
Olsen GW, Burris JM, Ehresman DJ, Froehlich JW, Seacat AM, Butenhoff JL, Zobel LR (2007) Half-life of serum elimination of perfluorooctanesulfonate, perfluorohexanesulfonate, and perfluorooctanoate in retired fluorochemical production workers. Environ Health Perspect 115:1298–1305
Paul AG, Jones KC, Sweetman AJ (2009) A first global production, emission, and environmental inventory for perfluorooctane sulfonate. Environ Sci Technol 43:386–392
Peden-Adams MM, Keller JM, Eudaly JG, Berger J, Gilkeson GS, Keil DE (2008) Suppression of humoral immunity in mice following exposure to perfluorooctane sulfonate. Toxicol Sci 104:144–154
Pérez-Melgosa M, Hollenbaugh D, Wilson CB (1999) Cutting edge: CD40 ligand is a limiting factor in the humoral response to T cell-dependent antigens. J Immunol 163:1123–1127
Plotkin S (2014) History of vaccination. Proc Natl Acad Sci U S A 111:12283–12287
Plotkin SA, Plotkin SL (2011) The development of vaccines: how the past led to the future. Nat Rev Microbiol 9:889–893
Qazi MR, Nelson BD, DePierre JW, Abedi-Valugerdi M (2012) High-dose dietary exposure of mice to perfluorooctanoate or perfluorooctane sulfonate exerts toxic effects on myeloid and B-lymphoid cells in the bone marrow and these effects are partially dependent on reduced food consumption. Food Chem Toxicol 50:2955–2963
Ross P, De Swart R, Addison R, Van Loveren H, Vos J, Osterhaus A (1996) Contaminant-induced immunotoxicity in harbour seals: wildlife at risk? Toxicology 112:157–169
Safe SH (1994) Polychlorinated biphenyls (PCBs): environmental impact, biochemical and toxic responses, and implications for risk assessment. Crit Rev Toxicol 24:87–149
Schecter A, Stanley J, Boggess K et al (1994) Polychlorinated biphenyl levels in the tissues of exposed and nonexposed humans. Environ Health Perspect 102(Suppl):149–158
Schecter A, Päpke O, Tung KC, Joseph J, Harris TR, Dahlgren J (2005) Polybrominated diphenyl ether flame retardants in the U.S. population: current levels, temporal trends, and comparison with dioxins, dibenzofurans, and polychlorinated biphenyls. J Occup Environ Med 47:199–211
Skaare JU, Bernhoft A, Derocher A et al (2000) Organochlorines in top predators at Svalbard–occurrence, levels and effects. Toxicol Lett 112–113:103–109
Stølevik SB, Nygaard UC, Namork E et al (2011) Prenatal exposure to polychlorinated biphenyls and dioxins is associated with increased risk of wheeze and infections in infants. Food Chem Toxicol 49:1843–1848
Stølevik SB, Nygaard UC, Namork E et al (2013) Prenatal exposure to polychlorinated biphenyls and dioxins from the maternal diet may be associated with immunosuppressive effects that persist into early childhood. Food Chem Toxicol 51:165–172
Suja F, Pramanik BK, Zain SM (2009) Contamination, bioaccumulation and toxic effects of perfluorinated chemicals (PFCs) in the water environment: a review paper. Water Sci Technol 60:1533–1544
Toms L-ML, Thompson J, Rotander A et al (2014) Decline in perfluorooctane sulfonate and perfluorooctanoate serum concentrations in an Australian population from 2002 to 2011. Environ Int 71:74–80
Van den Berg M, Birnbaum LS, Denison M et al (2006) The 2005 World Health Organization reevaluation of human and Mammalian toxic equivalency factors for dioxins and dioxin-like compounds. Toxicol Sci 93:223–241
Van Loveren H, Germolec D, Koren HS et al (1999) Report of the bilthoven symposium: advancement of epidemiological studies in assessing the human health effects of immunotoxic agents in the environment and the workplace. Biomarkers 4:135–157
Vestergren R, Cousins IT (2009) Tracking the pathways of human exposure to perfluorocarboxylates. Environ Sci Technol 43:5565–5575
Wang Z, Cousins IT, Scheringer M, Buck RC, Hungerbühler K (2014) Global emission inventories for C4-C14 perfluoroalkyl carboxylic acid (PFCA) homologues from 1951 to 2030, Part I: production and emissions from quantifiable sources. Environ Int 70:62–75
Weihe P, Grandjean P, Debes F, White R (1996) Health implications for Faroe islanders of heavy metals and PCBs from pilot whales. Sci Total Environ 186:141–148
Weihe P, Kato K, Calafat AM, Nielsen F, Wanigatunga AA, Needham LL, Grandjean P (2008) Serum concentrations of polyfluoroalkyl compounds in Faroese whale meat consumers. Environ Sci Technol 42:6291–6295
Weisglas-Kuperus N, Patandin S, Berbers GA, Sas TC, Mulder PG, Sauer PJ, Hooijkaas H (2000) Immunologic effects of background exposure to polychlorinated biphenyls and dioxins in Dutch preschool children. Environ Health Perspect 108:1203–1207
Weisglas-Kuperus N, Vreugdenhil HJI, Mulder PGH (2004) Immunological effects of environmental exposure to polychlorinated biphenyls and dioxins in Dutch school children. Toxicol Lett 149:281–285
WHO (2012) Guidance for immunotoxicity risk assessment for chemicals, IPCS harmonization project document; No. 10 World Health Organization, Geneva. ISBN 978 92 4150 330 3
Yang Q, Xie Y, Depierre JW (2000) Effects of peroxisome proliferators on the thymus and spleen of mice. Clin Exp Immunol 122:219–226
Yang Q, Abedi-Valugerdi M, Xie Y, Zhao X-Y, Möller G, Dean Nelson B, DePierre JW (2002) Potent suppression of the adaptive immune response in mice upon dietary exposure to the potent peroxisome proliferator, perfluorooctanoic acid. Int Immunopharmacol 2:389–397
Acknowledgments
The research summarized in this chapter has been supported by National Institute of Environmental Health Sciences, NIH (ES012199 and ES021993), the National Science Foundation (OCE-1321612), the US Environmental Protection Agency (R830758), the Danish Council for Strategic Research (09–063094), and the Danish Environmental Protection Agency as part of the environmental support program DANCEA (Danish Cooperation for Environment in the Arctic). The authors are solely responsible for the conclusions expressed in this chapter, which do not necessarily reflect the position of any of the funding agencies. We thank Katie T. Herz for editorial comments.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2016 Springer-Verlag Wien
About this chapter
Cite this chapter
Kielsen, K., Shamim, Z., Ryder, L.P., Grandjean, P., Heilmann, C. (2016). Vaccination Efficacy and Environmental Pollution. In: Esser, C. (eds) Environmental Influences on the Immune System. Springer, Vienna. https://doi.org/10.1007/978-3-7091-1890-0_8
Download citation
DOI: https://doi.org/10.1007/978-3-7091-1890-0_8
Published:
Publisher Name: Springer, Vienna
Print ISBN: 978-3-7091-1888-7
Online ISBN: 978-3-7091-1890-0
eBook Packages: Biomedical and Life SciencesBiomedical and Life Sciences (R0)