
Abstract
Epilepsy surgery for drug-resistant childhood epilepsy is not new. However, brain imaging, surgical and anaesthetic techniques have improved to the extent that they are now as much safer and realistic option than they were in the past. Further, the range of surgical candidates is wide, and previous concepts about likely surgical candidates are now challenged as children with previously thought widespread or apparent multifocal disease are evaluated. Outcomes for seizure freedom range from 40 to 80 % depending on the underlying aetiology and the extent of resection. However, the aims of surgery may include seizure reduction in some and improvement in neurodevelopment and behaviour in others, which are less predictable. Epilepsy surgery in children is no longer a last resort. Children thought to be likely candidates should be evaluated early in their natural history to optimise outcomes in the long term.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
Introduction
Epilepsy is a chronic neurological condition characterised by recurrent epileptic seizures where an epileptic seizurecan be defined as a transient occurrence of signs and/or symptoms due to abnormal, excessive or synchronous neuronal activity in the brain [20]. Five percent of the population will have a seizure during their lifetime. About 50 million people worldwide have epilepsy, and nearly two out of every three new cases are discovered in developing countries. Epilepsy is about twice as common in children as in adults, with a rate of 7/1,000 in childhood and only 3.3/1,000 in adults.
Anti-epileptic drugs (AEDs) are the first-line treatment, and seizures will be well controlled by medications in approximately two out of three children with epilepsy. Unfortunately, up to one third of children will not respond optimally to medical treatment, with either continued seizures or unacceptable side effects. Furthermore, there is a high rate of cognitive and behavioural disorders associated with early onset epilepsy. A proportion of these children may be candidates for epilepsy surgery, the removal or modification of part of the brain with the specific aim of treating epilepsy. This is not a new concept; it has been used in the management of epilepsy for over 100 years. However, it is only relatively recently that surgery has gained momentum as a realistic choice in the management of epilepsy in children.
The epidemiology of epilepsy differs between adults and children. Intractable epilepsy in adults is frequently caused by temporal lobe epilepsy (TLE). Temporal lobe resection for the treatment of TLE has provided an excellent option for patients. Excision of the seizure focus generates high expectations for seizure control, minimal loss of function and low morbidity [14, 44]. However, TLE is not a particularly common disorder in children. The underlying pathologies of paediatric epilepsy tend instead to involve extratemporal regions and present in a more diffuse manner. Furthermore, early life seizures more commonly arise secondary to a developmental disorder. These epilepsies can be catastrophic in onset, with developmental regression and related concerns that play a significant role in decision making [2]. This combination of factors results in a group of patients presenting with surgically remediable epilepsy in childhood who exhibit distinctly different characteristics from the typical adult presentation.
Many advances have occurred over the past 25 years since the early reports of successful epilepsy surgery in a highly selected paediatric population. There are increasing data on the benefit of epilepsy surgery in a wider range of carefully evaluated children [1, 27]. Improvements in seizure frequency and management are well documented, but consistent evidence of definable social and cognitive progress in this population has been elusive. A better understanding of the scope of positive and negative outcomes is essential. Expectations of benefit play a critical role in the decision-making process of not only on whom to operate but also when. Fortunately, numerous advances in presurgical evaluation, surgical methods and monitoring technology have improved decision making, procedural options and outcomes.
Evolving Methods and Perspectives
Candidate Selection: Expanding Criteria
Since the late nineteenth century, surgery has been utilised as a treatment for medically refractory epilepsy and recognised as possibly relevant in children over the past 50 years. Depending on the specific procedure, current chances of seizure remission following resective surgery of the epileptogenic focus in adults are typically in the range of 60–70 % [14] and the risk of complications and associated morbidity remains low. Many referrals for epilepsy surgery in the paediatric population are for catastrophic onset epilepsies. Initial reluctance to consider children as candidates for epilepsy surgery has been shown to be unfounded [10]. Success rates in children also vary with the specific procedure and the causative pathology but can be impressive, with low morbidity and mortality rates when candidates are evaluated and treated in specialist paediatric centres. It is currently estimated that 127 children in every 1,000,000 present with drug-resistant epilepsy each year, of which one in five will be appropriate candidates for a surgical procedure [5].
Surgery is considered for drug-resistant epilepsy in children when an assessment indicates that there will be a significant improvement in seizure control in the absence of an unacceptable loss of function. Meeting the first requirement of these criteria would appear straightforward; drug-resistant epilepsy is that which does not respond to medical intervention. Nonetheless, adult definitions have not necessarily been relevant to the childhood population. Over time it has become evident that the traditional view of drug resistance –failure of two drugs over 2 years – is not applicable in many, particularly those with seizure onset within the first 2 years of life [4]. More recently, the ILAE has put forward a modified definition of treatment failure:‘adequate trials of two tolerated and appropriately chosen AED schedules (whether as monotherapies or in combination) that fail to achieve sustained seizure freedom’. In this report, treatment response is defined as seizure freedom lasting at least three times the longest seizure-free interval prior to a new intervention [33]. This would take into consideration even the very young with more catastrophic onset epilepsy.
Additional uncertainty surrounds the developmental delay, cognitive decline and social costs associated with unremitting seizures in children [11]. Considerable concern that developmental losses may become less remediable over time adds a sense of potential urgency to the decision [16, 17]. This is further exacerbated by the catastrophic nature of seizures in some young children.
Historically, impaired intellectual function has been interpreted to mean widespread brain disorder predictive of a poor surgical outcome. Consistent with this belief, criteria for consideration of epilepsy surgery have included normal IQ in some circumstances [38]. However, outcome studies in children suggest that impaired IQ is not synonymous with poor seizure outcome. If a child’s cognitive disabilities are at least in part a consequence of ongoing seizures, there is additional potential for improvement in their achievements following surgery with seizure control. There are also a number of studies that have shown significant gains in IQ testing over time after attaining seizure-free status with epilepsy surgery [2, 21, 45]. These children present a compelling argument for a greater sense of urgency to proceed with epilepsy surgery.
Children with epilepsy frequently have coexistent psychiatric disorders. More than half of children with both seizures and a structural brain abnormality will have a psychiatric disorder. Thus the rate of psychiatric disorder in children coming in for surgical evaluation is particularly high. This has been demonstrated in children with either extratemporal [9] or temporal lobe epilepsy [37]. Unfortunately, the group of children with relevant cognitive and behavioural comorbidities may not experience significant improvement in these disabilities following epilepsy surgery [21, 37]; some diagnoses may indeed evolve. Although some children gain additional psychiatric diagnoses following epilepsy surgery despite an improvement in seizure control, there is no indication that the surgery increases this risk. Appropriate counselling of families is essential prior to surgery in order to highlight this but it is evident that existing psychiatric disorders do not represent a contraindication to surgery.
Surgical Techniques for Childhood Epilepsies
Surgery is considered for drug-resistant epilepsy when an assessment indicates the potential for significant improvement in seizure control in the absence of an unacceptable loss of function. Outcomes are optimal when seizures are demonstrated to arise from one well-defined area that can be removed without functional compromise. This was initially restricted to a temporal lobectomy procedure performed in adults; however, studies showed that many of the adults who benefitted from this intervention had epilepsy since early childhood, suggesting the potential for similar surgery in children [51].
At this time it is well recognised that the complete resection of a single discrete seizure focus in a non-eloquent region of cortex provides an excellent option for seizure treatment at any age. However, the increasing scope of paediatric patients presenting for surgery includes children with syndromes where seizures may be perceived to be generalised or multifocal in onset. Both the site of onset and pathogenesis differentiate paediatric from adult epilepsy [26] (Tables 1and 2). Advances in neuroimaging and neuroanaesthesia have reduced the morbidity and further widened the spectrum of surgical candidates. Improved MRI techniques for structural imaging, as well as more options for functional assessment, have informed preoperative analysis. Advances in surgery such as image-guided techniques, prolonged video EEG and invasive monitoring with stimulation for eloquent cortex have significantly improved surgery outcomes [12]. These techniques can facilitate the goal of complete removal of a seizure focus with preservation of function and fewer complications for a greater range of patients.
Surgical options are considered in two categories: resective and functional. Hemispherectomy and multilobar procedures are the procedures most commonly undertaken in children, especially in the very young [18, 26]. Extratemporal resection for focal cortical dysplasia and developmental tumours is more common in older children with good results [1, 19, 27, 29].
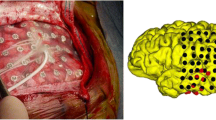
The most common causes of drug-resistant seizures in children are cortical malformations [24]. A number are too diffuse to be addressed with a single resective procedure. However, when restricted to a single hemisphere, variable degrees of resection have been shown to be successful. Although large areas of malformation may be easily recognised (Fig. 1), others are more subtle but the introduction and utilisation of higher resolution MR imaging has made it increasingly clear that cortical dysplasia is an extremely common cause of childhood epilepsy. When these lesions can be identified and are not in eloquent cortex, surgical excision is a highly effective option. Unfortunately, these lesions are found at a surprisingly high frequency in areas of critical, functional cortex. Thus a complete evaluation of both the structure and functionality of the region of interest is essential before surgery can be considered [26, 34].

MRI (a) and EEG (b) of an infant presenting with seizures in the neonatal period. The MRI shows left hemimegalancephaly; the EEG seizure onset in the left hemisphere. The child underwent a left functional hemispherectomy at 4 months of age, leading to seizure freedom
The types of seizures seen in the early onset epilepsies are more a reflection of the age of presentation than the underlying pathology. For example, infantile spasms are events that occur in infants as an age-specific response to a range of pathologies involving a single discrete malformation, multiple foci or a diffuse area of the brain. Thus an apparent generalised event can reflect the immaturity of the environment as opposed to indicating pathology. In cases where the underlying pathology is discrete and identifiable, prompt surgery may provide the best treatment option. The developmental regression that occurs in the presence of unremitting seizures is typically devastating, and earlier surgery is associated with better postsurgical developmental outcomes [28]. In addition, the very young brain retains the ability to alter its functional architecture in response to surgical excision and thus preservation of eloquent cortex is less of a concern.
Early onset epilepsy, especially those related to particular pathologies such as Sturge-Weber syndrome, tuberous sclerosis (Fig. 2), hemispheric syndromes and extensive focal cortical dysplasia, can present with generalised or multifocal features both in clinical presentation and EEG characteristics. However, with underlying focal/lateralised pathology, they are likely to have focal onset and can break traditional concepts of epilepsy surgery [28]. Further with more advanced analysis of epileptic activity, increasingly complex excisions are being evaluated for TS that can be highly successful [49].

MRI and ictal EEG of a 15-month old with focal seizures, the result of tuberous sclerosis. Ictal EEG showed seizure onset from the right frontal region (F4). Although there are multiple tubers seen on MRI, there is a large calcified tuber in the left frontal region (arrowed). Removal of the right frontal tuber led to seizure freedom for 3 years
A procedure considered far more frequently in children than in adults is hemispheric disconnection. This is due in part to the spectrum of underlying pathology as well as to the catastrophic and progressive nature of these diagnoses. For example, seizures are common in Sturge-Weber syndrome, a sporadically occurring disorder with leptomeningeal angioma and associated facial capillary haemangioma (port-wine stain). Seizures can be difficult to control especially if they commence before 1 year as they do in over half of the children. When the seizures do not respond to medical treatment and the process is hemispheric and unilateral, then a hemispherectomy can be a highly beneficial intervention. These children typically present with a hemiparesis that may progress with seizures. Timing of surgery is an issue as some studies indicate a better outcome with early resective surgery [8, 32]. The several different types of hemispherectomy procedures considered under these circumstances have been shown to have similar outcomes [27].
Another paediatric disorder treated with hemispherectomy is Rasmussen Encephalitis (RE). RE is a rare presumed autoimmune disorder involving unilateral hemispheric inflammation and in many relentless epileptic encephalopathy (Fig. 3). Seizures are frequently intractable and progression of the disease leads to cortical hemiatrophy and contralateral hemiparesis. Hemispherectomy is the only cure. It improves epilepsy and halts the cognitive regression, but results in a dense hemiparesis and hemianopia. The most challenging aspect of the treatment debate involves the timing of surgery, as outcomes are reported as better with earlier intervention but not all children may progress to the level of disability achieved by surgery [6]. Hemispherectomies are also considered in children with extensive malformations when the pathology appears to be limited to one side of the brain.

Sequential MRI of the brain of an 8 year old who presented with R focal motor seizures, and subsequently developed increasing frequency to Epilepsia partialis continua with increasing right hemiparesis. Although atrophy of the left hemisphere is seen on the first scan (a), this has progressed on the second scan 12 months later (b) suggestive of Rasmussen encephalitis
Options are more limited when a seizure focus cannot be identified or when a recognised focus is inextricably linked with essential eloquent cortex. When the child’s epilepsy is intractable and debilitating but the cause is not amenable to resection, functional surgical interventions may be considered. The intent of these procedures is to disrupt seizure propagation and contain the abnormal activity as much as possible. Corpus callosotomy, the severing of the connecting fibres between the two hemispheres of the brain, is one such procedure. The goal is to restrict epileptic activity to one hemisphere. This procedure has provided significant relief for ‘drop’ attacks that cause injury, markedly improving quality of life [36, 41]. Although drop attacks are the seizure type most consistently treated in this manner, improvement in other generalised seizures may also be experienced in individuals following surgery.
Multiple subpial transections is another palliative technique used where the surgical focus may be associated with functional cortex. The theory is that the process involves transection of the transverse fibres most implicated in seizure propagation while preserving the vertical functional pathways of the cortex. The technique has also been used in combination with respective surgery where the focus involves eloquent cortex [47] The technique has also been helpful in drug-resistant cases of Landau-Kleffner syndrome, an acquired epileptic aphasia associated with continuous spike-wave of slow sleep. In the absence of a discrete lesion, subpial transections are performed over Wernnicke’s area (and deep into the sylvian fissure, under cortigographic guidance) on the EEG driving side in order to disrupt the epileptic focus while retaining relative preservation of the functional cortex [3, 39].
Timing of Surgery: The Role of Plasticity
The decision of the optimal timing of surgical treatment is often challenging, as the risk–benefit assessment requires clinical experience and multidisciplinary input. There are reasons specific to early life brain development why surgery should be considered promptly in the natural history of paediatric epilepsy. The first years of life are a critical period for the development of cognitive abilities. Studies demonstrate that the presence of seizures leads to cognitive impairment independently of underlying pathology [40]. When ongoing epileptic activity is at least in part responsible for cognitive dysfunction, improved outcome would be expected if and when seizure freedom can be achieved. Thus surgical intervention can be urgent in infants with catastrophic epilepsy unresponsive to medical intervention in order to try to prevent developmental regression or arrest. These candidates for epilepsy surgery need to be identified early in the process of the disease to prevent the possibility of worsening developmental outcomes that could be seen with delayed time to surgery.
There have been indications of ongoing reluctance to refer children for surgery. This barrier has resulted in many children experiencing an unnecessary wait for a possible curative procedure [26]. Epilepsy surgery in children under 3 years of age offers suitable candidates a good chance of significantly improved seizure outcome which compares with rates in older cohorts [16, 18] yet only a third of eligible children are referred within 2 years of diagnosis [26]. This is especially unfortunate since outcomes for cognitive testing, social determinants and motor recovery are all improved by earlier interventions that give the developing brain ample opportunity to develop compensatory function [12].
While the remarkable plasticity of the immature brain is a liability with progressive seizures, it is clearly an asset to epilepsy treatment outcomes. The child’s brain is capable of significant reorganisation of neurological function after insult and surgery, highlighting the importance of early surgical intervention to prevent developmental arrest or regression [23]. Delay to surgery is associated with increased psychosocial, behavioural and educational problems. There are deficits not only associated with the presence of seizures but also with the existence of competitive, dysfunctional brain that can interfere with compensatory function in more functional brain regions [40]. Functional plasticity is particularly noted in the pattern of recovery of linguistic competence following dominant hemispherectomy in children with acquired epilepsy [7]. In congenital hemispheric disorders associated with epilepsy, the contralateral hemisphere is likely to develop dominance. When acquired disorders such as RE involve the dominant hemisphere, surgery at a younger age may provide a better opportunity for transfer of language function due to this increased plasticity. However, when disease progression is slow and deficits less profound, determining the optimum timing for surgery can be very challenging.
Another complication of the aspect of timing relates to the determinants of why children with epilepsy have such a high rate of cognitive disorders. There is evidence supporting hypotheses that seizures and altered cognition independently occur in the presence of the developmental brain pathologies that cause seizures. When the interaction between epilepsy and cognitive disability is uncertain, the necessity of surgery to prevent harm becomes less obvious [13].
Presurgical Evaluation
Management of epilepsy requires a multidisciplinary approach throughout the preoperative, perioperative and postoperative periods [12]. An appropriate team can properly address not only seizure management but also critical comorbidities such as safety, independence, mobility, emotional and behavioural issues, cognition, education and learning. The quality of life of patients and families is greatly enhanced by identifying and managing these additional risk factors.
Improved referral patterns are essential to optimising surgical outcomes [12]. Due to the need for appropriate technology, experience and expertise, children with drug-resistant epilepsy benefit when referred to comprehensive epilepsy centres rather than isolated surgical units. Children with behavioural or developmental regression in the setting of drug-resistant seizures should be referred with greater urgency for presurgical evaluation. Certain subgroups of surgical candidates should be referred to an experienced surgical unit equipped with multidisciplinary personnel with access to advanced technologies such as PET, SPECT and functional MRI. These subgroups would include particularly young children or those at greater risk for complications and morbidity, such as when a seizure focus is difficult to localise or in a potentially eloquent region where invasive EEG monitoring may be required.
Advances in structural imaging have led to improvements in identification of the areas responsible for seizure onset. As might be expected, surgical outcomes are improved when the pathological assessment of the resected region shows an abnormality [52]. Newer techniques in MRI imaging have improved the presurgical structural analysis such that the areas of abnormal cortex are more likely to be closely identified. 3D analysis, specific protocols of ultra-thin slices and additional types of echo sequences have greatly increased the sensitivity and specificity of MRI [22].
In order to optimise post-surgical outcome, it is not only critical to assess the brain being considered for resection, but also that the remaining brain is structurally normal. This is especially important when considering a wide resection or hemispherectomy, although subtle contralateral abnormalities may not be a contraindication to surgery [25]. Advances in functional imaging with fMRI have improved safety of resection by identifying areas of cortical function. When the presence of a structural lesion correlates with a specific electrographic seizure focus, the decision for surgical potential may be easy. In the absence of such helpful associations, non-invasive functional imaging may provide information about the likely area responsible. These studies can take the form of ictal and interictal single-photon emission computed tomography (SPECT) or interictal positron emission tomography (PET) [30].
At a minimum, surgical candidates should be evaluated with an interictal EEG that includes sleep monitoring, preferably video EEG monitoring, an MRI with a specified epilepsy protocol, and an age-appropriate neuropsychological and developmental assessment [12]. However, even with newer functional modalities invasive EEG monitoring may be necessary if a focus is particularly difficult to identify or if the interaction with eloquent cortex is indeterminate. Surgical decisions are mainly based on non-invasive monitoring with aid of functional imaging as needed. There is recognised need for invasive monitoring in selected cases, particularly when there is a delineated focus on EEG but MRI is either lesion-negative or the extent of the lesion cannot be defined. When more extensive assessment is indicated, then a child should be transferred to a specialist surgical centre with experience of such techniques.
Outcomes
The primary objective of epilepsy surgery is seizure freedom, or at the very least reduction of seizures. It may also be aimed at improving other important aspects of neurodevelopment and quality of life. While complete resection of a seizure focus is the best predictor of seizure freedom, developmental outcomes have proven more difficult to quantify. Outcome goals need to be assessed with an individual focus, as population goals may be less appropriate to the spectrum of children appropriate for surgery. Now that low IQ, mental illness and very young age are not considered contraindications to a surgical approach, children being evaluated have an even greater range of developmental status specifically related to their underlying condition.
Nonetheless, relief from seizures remains the defined goal of epilepsy surgery. A number of classification schemes are used to assess outcome. The Engel classification system, originally devised in 1987, is the most commonly used scale (see Table 3) [50]. It identifies significant decreases in seizure number, but also allows for quantification of worthwhile improvement independent of decreased frequency. A change in severity of seizures, or decrease in a particularly troublesome seizure type such as drop attacks, can be reflected in this lifestyle-relevant category. This aside, categories are quite broad, and can be difficult to apply to some of the catastrophic onset epilepsies.
Epilepsy surgery is targeted towards seizure freedom or where possible, although in some with more complex epilepsy reduction in seizures may be the aim (Engel Grade I or II). Overall clinical outcomes appear to be dependent on several factors but the most important determinant of whether seizure freedom will be achieved postoperatively remains whether the resection of the seizure focus is complete [19, 34]. Currently, surgical outcome in children following focal resections is similar to that in adults, with seizure-free rates in the range of 75–80 %, particularly in patients with well-circumscribed lesions where complete lesion resection without sacrifice of functional brain is possible [46]. Children undergoing temporal lobe resection are more likely to achieve seizure freedom (85 %) [45] than those undergoing extratemporal resection (60 %) [29]. Seizure remission rates after surgery for extratemporal apparent non-lesional epilepsy are less favourable, typically due to the challenges of accomplishing a complete resection [34].
While all assessed groups demonstrate worthwhile levels of seizure reduction, cognitive, social and behavioural improvements remain more difficult to quantify. A reduction in the burden of ongoing epilepsy should confer psychosocial benefit and improve quality of life in children. Furthermore, surgical intervention at an earlier age could be expected to have a greater role in preventing cognitive dysfunction than would that in older patients. However, there are minimal published data to support these concepts. Accurate assessment of cognition, behaviour, psychosocial adaptation and quality of life are crucial for an understanding of paediatric epilepsy surgery candidates [12]. Children with ongoing seizures can experience a widening gap in IQ learning relative to their peers with consequent decrease in. Thus the maintenance of IQ in children following surgery could be interpreted as success.
Improvements in cognitive outcomes have been shown in early IQ/DQ in very young children after surgery. Younger children, the group that has highest deficits going into surgery, show the most benefit [35, 43]. Postoperative developmental trajectories are maintained with a stable velocity and importantly accelerated development may occur in seizure-free patients [21]. Furthermore, surgery for TLE performed in childhood results in additional long-term benefits in cognitive development with improved IQ seen beyond 6 years following surgery, related to seizure freedom and wean from medication [45].
The mechanisms underlying short-term and long-term cognitive advances may differ. Whereas short-term improvements may relate to the immediate cessation of seizure activity, long-term improvements have also been shown to be not only associated with seizure control but also removal of AEDs and increased grey matter volumes [45]. A wean from AEDs is a common goal following epilepsy surgery, particularly for parents who already perceive benefits of this objective. However, this may be yet another complex decision since recent tendencies towards less aggressive medication withdrawal are thought to be a contributing reason for improving outcomes following paediatric epilepsy surgery [27].
Patients with acquired disorders treated with a hemispherectomy consistently do better on follow up than children with congenital disorders, especially malformations. Postoperative seizure freedom in the group with developmental pathology is closer to 30 %, in contrast to those with acquired pathology who enjoy complete seizure remission over 80 % of the time [15]. Although most patients with more extensive surgery tend towards more moderate improvement, there are also gains in the social and cognitive outcomes of children after hemispherectomy. Immediate cognitive gains are reported in all groups following surgery, particularly in circumstances where the presence of seizures limits the child’s exposure to social and environmental stimuli [48]. In studies with higher presurgical scores, there is less improvement in cognitive development; however, long-term outcomes are quite favourable in some groups [15, 42]. In patients treated with hemispherectomy for RE, language is significantly more impaired for left (presumed dominant) than right hemispherectomy and cognitive measures change little between surgery and follow up [42].
Significant behavioural improvements however are consistently appreciated post-hemispherectomy in children with unmanageable aggressive and explosive behaviours prior to surgery. This situation is most frequently noted in children with congenital hemiplegic syndromes the result of developmental pathologies whose postoperative seizure profile is the least encouraging of the groups [15]. This suggests that a realistic appraisal of prognosis requires an assessment of underlying pathology as patients with acquired or progressive disorders will have a differing prognosis than patients with congenital disorders both for seizure and behaviour outcome.
Conclusions
Advances in evaluation and surgery mean that wider spectrum of children are amenable to safe surgical resection. Not only can resective surgery for focal epilepsy in children result in similar levels of seizure remission to that seen in adults, surgery can provide a critical option to improve outcomes for a wide variety of paediatric epilepsies. Possible candidates can and should be identified early in their natural history and evaluated. All children with intractable epilepsy and evidence of a focal structural brain abnormality should be considered as possible candidates. This must actively include children under the age of 2 years, particularly those children with epilepsies that are likely to have a poor progress for seizure control. Furthermore, children with focal-onset epilepsy and a history of medication resistance should be considered even where a structural brain abnormality is not demonstrated, as further evaluation with advanced techniques may reveal that surgery is a possibility. Much can be gained from early referral when surgery may be deemed an appropriate option – much can be lost in the long term by delaying.
References
Ansari SF et al (2010) Surgery for extratemporal nonlesional epilepsy in children: a meta-analysis. Childs Nerv Syst 26(7):945–951
Battaglia D et al (2006) Cognitive assessment in epilepsy surgery of children. Childs Nerv Syst 22:744–759
Benifla M et al (2006) Multiple subpial transections in pediatric epilepsy: indications and outcomes. Childs Nerv Syst 22:992–998
Berg AT, Levy SR, Testa FM, D’Souza R (2009) Remission of epilepsy after 2 drug failures in children: a prospective study. Ann Neurol 65(5):510–519
Berg AT et al (2009) Frequency, prognosis and surgical treatment of structural abnormalities seen with magnetic resonance imaging in childhood epilepsy. Brain 132:2785–2797
Bien CG et al (2005) Pathogenesis, diagnosis and treatment of Rasmussen encephalitis: a European consensus statement. Brain 128:454–471
Boatman D et al (1999) Language recovery after left hemispherectomy in children with late-onset seizures. Ann Neurol 46(4):579–586
Bourgeois M et al (2007) Surgical treatment of epilepsy in Sturge-Weber syndrome in children. J Neurosurg 106(1):20–28
Colonnelli MC et al (2012) Psychopathology in children before and after surgery for extratemporal lobe epilepsy. Dev Med Child Neurol 54:521–526. doi:10.1111/j.1469-8749.2012.04293.x, first published on-line14 Apr 2012
Cross JH (1999) Update on surgery for epilepsy. Arch Dis Child 81:356–359
Cross JH (2002) Epilepsy surgery in childhood. Epilepsia 43(S3):65–70
Cross JH et al (2006) Proposed criteria for referrral and evaluation of children for epilepsy surgery: recommendations of the subcommission for pediatric epilepsy surgery. Epilepsia 47(6):952–959
D’Argenzio L et al (2011) Cognitive outcome after extratemporal epilepsy surgery in childhood. Epilepsia 52(11):1966–1972
de Tisi J et al (2011) The long-term outcome of adult epilepsy surgery, patterns of seizure remission, and relapse: a cohort study. Lancet 378:1388–1395
Devlin AM et al (2003) Clinical outcomes of hemispherectomy for epilepsy in childhood and adolescence. Brain 126:556–566
Duchowny M et al (1998) Epilepsy surgery in the first three years of life. Epilepsia 39(7): 737–743
Dunkley C, Cross JH (2006) NICE guidelines and the epilepsies: How should practice change? Arch Dis Child 91:525–528
Dunkley C et al (2011) Epilepsy surgery in children under 3 years. Epilepsy Res 93:96–106
Edwards JC et al (2000) Seizure outcome after surgery for epilepsy due to malformaiton of cortical development. Neurology 55(8):1110–1114
Fisher RS et al (2005) Epileptic seizures and epilepsy: definitions proposed by the International League Against Epilepsy (ILAE) and the International Bureau for Epilpesy (IBE). Epilepsia 46(4):470–472
Freitag H, Tuxhorn I (2005) Cognitive function in preschool children after epilepsy surgery: rationale for early intervention. Epilepsia 46(4):561–567
Gaillard WD et al (2009) Guidelines for imaging infants and children with recent-onset epilepsy. Epilepsia 50(9):2147–2153
Gleissner U et al (2005) Greater functional recovery after temporal lobe epilepsy surgery in children. Brain 128:2822–2829
Guerrini R, Dobyns WB, Barkovitch AJ (2007) Abnormal development of the human cerebral cortex: genetics, functional consequences and treatment options. Trends Neurosci 31(3):154–162
Hallbook T et al (2010) Contralateral MRI abnormalities in candidates for hemispherectomy for refractory epilepsy. Epilepsia 51(4):556–563
Harvey S, Cross JH, Shinnar S, Mathern BW (2008) Defining the spectrum of international practice in pediatric epilepsy surgery patients. Epilepsia 46(1):146–155
Hemb M et al (2010) Improved outcomes in pediatric epilepsy surgery: the UCLA experience. Neurology 74:1768–1775
Jonas R et al (2005) Surgery for symptomatic infant-onset epileptic encephalopathy with and without infantile spasms. Neurology 64:746–750
Kan P, Van Orman C, Kestle JRW (2008) Outcomes after surgery for focal epilepsy in children. Childs Nerv Syst 24:587–591
Knowlton RC et al (2008) Functional imaging: II. Prediction of epilepsy surgery outcome. Ann Neurol 64:35–41
Kossoff EH, Buck C, Freeman JM (2002) Outcomes of 32 hemispherectomies for Sturge-Weber sundrome worldwide. Neurology 59(11):1735–1738
Kramer U, Kahana E, Shorer Z, Ben-Zeev B (2000) Outcome of infants with unilateral Sturge-Weber syndrome and early onset seizures. Dev Med Child Neurol 42:756–759
Kwan P et al (2010) Definition of drug resistant epilepsy: consensus proposal by the ad hoc Task Force of the ILAE Commission on Therapeutic Strategies. Epilepsia 51(6):1069–1077
Lerner JT et al (2009) Assessment and surgical outcomes for mild type I and severe type II cortical dysplasia: a critical review and the UCLA experience. Epilepsia 50(6):1310–1335
Loddenkemper T et al (2007) Developmental outcome after epilepsy surgery in infancy. Pediatrics 119(5):930–935
Maehara T, Shimizu H (2001) Surgical outcome of corpus callosotomy in patients with drop attacks. Epilepsia 42(1):67–71
McLellan A et al (2005) Psychopathology in children with epilepsy before and after temporal lobe resection. Dev Med Child Neurol 47:666–672
Mohamed A et al (2001) Temporal lobe epilepsy due to hippocampal sclerosis in pediatric candidates for epilepsy surgery. Neurology 56(12):1643–1649
Morrell F et al (1995) Landau-Kleffner syndrome: treatment with subpial intracortical transection. Brain 118:1529–1546
Muter V, Taylor S, Vargha-Khadem F (1997) A longitudinal study of early intellectual development in hemiplegic children. Neuropsychologia 35(3):289–298
Nei M, O’Connor M, Liporace J, Sperling MR (2006) Refractory generalized seizures: response to corpus callosotomy and vagal nerve stimulation. Epilepsia 47(1):115–122
Pulsifer MB et al (2004) The cognitive outcome of hemispherectomy in 71 children. Epilepsia 45(3):243–254
Roulet-Perez E et al (2010) Impact of severe epilepsy on development: recovery potential after successful early epilepsy surgery. Epilepsia 51(7):1266–1276
Sadek A, Gray WP (2011) Chopping and changing: long-term results of epilepsy surgery. Lancet 378:1360–1362
Skirrow C et al (2011) Long-term intellectual outcome after temporal lobe surgery in childhood. Neurology 76(15):1330–1337
Spencer S, Huh L (2008) Outcomes of epilepsy surgery in adults and children. Lancet Neurol 7:525–537
Spencer SS et al (2002) Multiple subpial transection for intractable partial epilepsy: an international meta-analysis. Epilepsia 43(2):141–145
Thomas SG et al (2010) Cognitive changes following surgery in intractable hemispheric and sub-hemispheric pediatric epilepsy. Childs Nerv Syst 26:1067–1073
Weiner HL et al (2006) Epilepsy surgery in young children with tuberous sclerosis: results of a novel approach. Pediatrics 117(5):1494–1502
Wieser HG et al (2001) Proposal for a new classification of outcome with respect to epileptic seizures following epilepsy surgery. Epilepsia 42(2):282–286
Wyllie E et al (1988) Subdural electrodes in the evaluation for epilepsy surgery in children and adults. Neuropediatrics 19(2):80–86
Yoon HH et al (2003) Long-term seizure outcome in patients initially seizure-free after resective epilepsy surgery. Neurology 61(4):445–450
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2012 Springer-Verlag Wien
About this chapter
Cite this chapter
Follett, P.L., Vora, N., Cross, J.H. (2012). Paediatric Intractable Epilepsy Syndromes: Changing Concepts in Diagnosis and Management. In: Akalan, N., Di Rocco, C. (eds) Pediatric Epilepsy Surgery. Advances and Technical Standards in Neurosurgery, vol 39. Springer, Vienna. https://doi.org/10.1007/978-3-7091-1360-8_2
Download citation
DOI: https://doi.org/10.1007/978-3-7091-1360-8_2
Published:
Publisher Name: Springer, Vienna
Print ISBN: 978-3-7091-1359-2
Online ISBN: 978-3-7091-1360-8
eBook Packages: MedicineMedicine (R0)