
Abstract
Correction of Pectus Excavatum by using the Minimal Access Repair of Pectus Excavatum (MARPE) produces excellent thoracic remodeling results in children and adolescents for whom this technique was originally designed. Placing a retrosternal bar in older adolescents or adults, who have less malleable ribcages, often fails to elevate depressed sternum enough thus producing unsatisfactory outcomes. Moreover, placing an implanted bar in the ribcage generates tension forces that may lead to complications such as severe or prolonged postoperative pain and/or bar displacement or rotation. Using two or more metal bars to counteract the sternum resistance may enhance thorax remodeling but requires more surgical wounds or larger ones, which worsens the cosmetic outcome of this intervention.
The modified MARPE technique for correction of Pectus Excavatum in adults, is based on the idea that in order to achieve similar results to those attained in younger patients, the rigidity of the ribcage should be reduced before inserting the pectus bar; a goal that can be easily achieved by performing transverse section of the sternum. Osteotomy reduces thoracic rigidity thus facilitating immediate correction of the deformity, while reducing postoperative pain and implant displacements. Further relevant differences between our technique and the standard procedure are: use of short and mildly bent pectus bars and their insertion with bilateral endoscopic control through minimal periareolar or submammary skin incisions, with yields good esthetic results.
Access provided by CONRICYT-eBooks. Download chapter PDF
Similar content being viewed by others


Keywords
Technical Highlights
The main technical highlights of this procedure are:
-
(a)
Short and flat bars are used (curved only at the ends).
-
(b)
Bilateral perimammilar incisions in males and sub-mammary incisions in females are used for insertion of both the introducer and the pectus bar, which provide good esthetic results. Incisions at the axillary lines are requuired in cases of depression of the lower end of the sternum.
-
(c)
Use of angular lens to examine the pleural cavities and to monitor the whole procedure, which enhances the safety of this intervention.
-
(d)
Transverse sternotomy performed with endoscopic monitoring of the mammary vessels. This section allows for immediate correction of the deformity and reduces postoperative pain as well as the probability of implant migration.
-
(e)
Instruments and implant are inserted according to the steps described for the standard MARPE technique.
-
(f)
The bar is bilaterally fixed to the costal arcs by means of steel wire, without stabilizer plates.
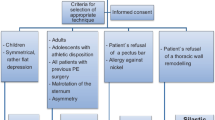
Indications
-
Symmetric Pectus Excavatum in adults
-
Symmetric Pectus Excavatum in older adolescents
-
Very severe Pectus Excavatum in adults, relatively asymmetric or complex (utilization of longer bars. Incisions at axillary lines).
Preoperative General Considerations
-
1.
The basic preoperative work-up includes: antero-posterior and lateral chest films, electrocardiogram and general laboratory investigations.
-
2.
Quantitative estimations of the deformity, such as the Haller index or volumetric studies have low impact on the decision of establishing the indication for surgery or on the planning of the intervention.
-
3.
Computed tomogram (CT) with three-dimensional reconstruction offers attractive images which are interesting from the academic point of view, but do not provide additional relevant information.
-
4.
Photographic documentation of the deformity before and after correction is recommended, taking frontal, lateral and oblique pictures from both sides of patients while they are in the supine and standing positions.
-
5.
Procedures are conducted under general anesthesia with selective intubation with double lumen tube. In case that this intubation procedure is not feasible, simple intubation can be used, with low ventilation volumes is sufficient.
-
6.
Although sternotomy markedly reduces postoperative pain, postoperative analgesia protocols are recommended, which include epidural analgesia during the first few days and intravenous analgesic treatment on subsequent days.
-
7.
Antibiotic prophylaxis with cephalosporin, is administered 30 min before skin incision and maintained until the fifth postoperative day
-
8.
Antithrombotic prophylaxis should be administered with low molecular weight heparin at standard doses.
Special Instruments
The surgical instruments for general thoracic surgery and following special intruments:
-
1.
Pectus surgical instruments set with bars, bar bending tools and dissectors (Biomet Microfixation Pectus Bar, Jacksonville, Florida). Stabilizer plates are not needed.
-
2.
Scope of 5 mm or 10 mm with 30° and flexible endoscopic ports (Flexipath 12 mm).
-
3.
Costotome and/or Lebsche knife (Codman and Shurtleff, Inc, Bridgewater, MA, USA).
-
4.
Multifilament Dall-Milles steel cable system and cable grip (Stryker Orthopaedics, Mahwah, NJ, USA) or monofilament stainless steel sternotomy wire.
Surgical Technique
The patient is placed in the supine position with a small interscapular roll and with the arms in abduction.
Incisions 2–3 cm long are performed on the internal margins of both areolas in male patients or on the submammary creases in female patients. The distance between both areolas is measured and a metal bar is selected that is four centimeters longer than that distance. The bar is then bent with a mild curvature at the both ends.
The mammary fat and pectoral muscles are displaced and flexible ports are inserted in both the hemithorax. Flexible ports allow for simultaneous parallel insertion of the scope and instruments. Both pleural cavities are then explored with a 30° scope.
A skin incision of 2 cm is made on the sternum, through which the pre-sternal tissue is dissected until the surface of the sternum is reached. Then the entire sternum thickness is sectioned with a costotome and/or a Lebsche knife. The right mammary vessels are monitored through scope, while the left vessels are preserved by stopping the sectioning procedure as soon as bone resistance is perceived to drop.
The pectus introducer is inserted through the right skin incision into the subpectoral layer and is moved forward until the highest point of the anterior arch is reached. At this point, it enters the right pleural cavity and is moved towards the contralateral hemithorax. The midline is crossed behind the depressed sternum ventral to the pericardium under endoscopic vision. At that moment, the scope is passed to the left hemithorax to monitor the entrance of the introducer in the left pleural cavity and its exit to the subpectoral space. At this point the introducer is advanced and a corresponding submuscular tunnel is created on the left side.
A cotton tape is tied to the end of the dissector and the dissector is withdrawn back to exit the ribcage. This cotton tape preserves the trajectory and facilitates insertion of a second broader introducer that widens the tunnel. The pectus bar is pulled through the anterior mediastinum from one incision to the other into the submuscular pockets and is finally turned and fixed to the ribs using steel wires without stabilizer plates. Our preference is for the Dall-Milles steel cable system and cable tensor.
After evacuation of the thoracic cavities, the wound is closed in layers.
Procedure Overview (Figs. 41.1, 41.2, 41.3, 41.4, 41.5, and 41.6)

Peri-mammilary incisions in male patients or in the submammary creases in female patients and an additional 2 cm incision to perform the sternotomy are made

Bilateral insertion of ports after which a sternotomy is performed under endoscopic vision of the right mammary vessels

The introducer is inserted through the right perimammilary incision. The introducer has crossed midline and exits the left pleural space and left chest wall in a symmetric manner. The scope is switched from one side to the other for this maneuver. A cotton tape is tied to the introducer and retrieved

The cotton band is used to help guide the bar into its final position

The pectus bar is flipped and set into the desired position

Both ends of the pectus bar are attached to the ribs with multifilament wires using a Dall-Milles steel cable system tied around the rib
Postoperative Management
Patients are extubated in the operation room and transferred to the recovery room for the first few hours, where the analgesic treatment is adjusted and a chest film is taken. After transfer to the wards, respiratory physiotherapy is provided after 24 h and mobilization after 48 h postoperatively. Patients are discharged on the 5th day with pain medication which consists of non-steroidal anti-inflammatory drugs. Relative rest for 2 weeks is recommended. Patients are advised to avoid sport activities in general for 6 months and competitive or contact sports for 1 year.
Removal of the pectus bar after 3 years is recommended; however, it can be removed earlier, once the sternal fracture is consolidated in its new position.
Comments
Correction of Pectus Excavatum by using the Minimal Access Repair of Pectus Excavatum (MARPE) produces excellent thoracic remodeling results in children and adolescents for whom this technique was originally designed. Placing a retrosternal bar in older adolescents or adults, who have less malleable ribcages, often fails to elevate depressed sternum enough thus producing unsatisfactory outcomes. Moreover, placing an implanted bar in the ribcage generates tension forces that may lead to complications such as severe or prolonged postoperative pain and/or bar displacement or rotation. Using two or more metal bars to counteract the sternum resistance may enhance thorax remodeling but requires more surgical wounds or larger ones, which worsens the cosmetic outcome of this intervention.
The modified MARPE technique for correction of Pectus Excavatum in adults, is based on the idea that in order to achieve similar results to those attained in younger patients, the rigidity of the ribcage should be reduced before inserting the pectus bar; a goal that can be easily achieved by performing transverse section of the sternum. Osteotomy reduces thoracic rigidity thus facilitating immediate correction of the deformity, while reducing postoperative pain and implant displacements. Further relevant differences between our technique and the standard procedure are: use of short and mildly bent pectus bars and their insertion with bilateral endoscopic control through minimal periareolar or submammary skin incisions, with yields good esthetic results.
For the success of this technique patients with chondromanubrial sternal depression or inelastic depression extensively involving the whole sternal body and both anterolateral rib cages (platythorax) are not eligible candidates for this intervention and should therefore be considered for an open surgical repair. Patients with rigid though asymmetric or extensive deformities however, can benefit from transverse sternotomy but need longer bars, which can only be inserted through lateral wounds.
Procedure Related Images (Figs. 41.7, 41.8, 41.9, 41.10, 41.11, 41.12, 41.13, 41.14, 41.15, 41.16, 41.17, 41.18, 41.19, 41.20, 41.21 and 41.22)

The 2–3 cm long perimmamilar incisions made in male patients or on the submammary creases in female patients provide easy access to insert the bar. An additional 2 cm incision is made in order to perform the sternotomy

The sternotomy is safely performed under endoscopic monitoring of the right mammary vessels. Transverse sternal osteotomy reduces tension of the rib cage if the sternum is rigid and depressed

The introducer is inserted through the right perimammilary incision in the subpectoral layer and is moved forward just above the anterior ribs until the location to insert the bar is reached. At this point it is inserted into the intrapleural space and is moved in a transverse direction into the mediastinum in order to create the retrosternal tunnel

The introducer has crossed midline and exits the left pleural space and left chest wall in a symmetric manner

The cotton tape preserves the trajectory and guides insertion of a second thicker dissector that widens the tunnel and of the metal implant

A short metal bar is selected and bent with a mild curvature at the ends

The cotton band is used to help guide the bar into its final position

The pectus bar is rotated and secured with steel wires. Both wings of the pectus bar are attached to the ribs with multifilament wires using a Dall-Milles steel cable system tied around the rib. Postoperative X-rays demonstrating the bar secured with a monofilament metal wire (a) -which was introduced through the bar hole (see arrow)- or with multifilament wire (b) embracing rib and prosthesis at its serrated end border (see arrow)

Once the pleural cavities are aspirated, the wound is closed in layers using simple interrupted sutures, such as 3–0 absorbable and 4–0 non-absorbable monofilament for subcutaneous tissue and skin, respectively

Pre- and postoperative (4th postoperative day) images of the deformity repair in an adult male patient. Note that this patient has Poland’s syndrome with absence of the left pectoralis major and minor muscles. Although this anomaly limits the final esthetic result of the intervention, adequate contour of the chest wall is achieved and scars are well concealed
Suggested Reading
Pérez D, Cano JR, Quevedo S, López L. New minimally invasive technique for correction of pectus carinatum. Eur J Cardiothorac Surg. 2011;39(2):271–3.
Pérez D, Cano JR, Quevedo S, López L. Videothoracoscopic repair of pectus excavatum with sternal transection for adult patients with nonelastic deformity. J Thorac Cardiovasc Surg. 2011;142(4):942–3.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2017 Springer-Verlag Berlin Heidelberg
About this chapter
Cite this chapter
Pérez, D., Torrent, G., Quevedo, S. (2017). Minimally Access Repair of Pectus Excavatum- with Sternotomy in Adults. In: Saxena, A. (eds) Chest Wall Deformities. Springer, Berlin, Heidelberg. https://doi.org/10.1007/978-3-662-53088-7_41
Download citation
DOI: https://doi.org/10.1007/978-3-662-53088-7_41
Published:
Publisher Name: Springer, Berlin, Heidelberg
Print ISBN: 978-3-662-53086-3
Online ISBN: 978-3-662-53088-7
eBook Packages: MedicineMedicine (R0)