
Abstract
Patients with severe lower-extremity trauma present multiple challenges to surgeons, physiatrists, rehabilitation specialists, and family members. Often there is considerable debate surrounding limb salvage or to proceed with early amputation. Prior to the LEAP study (Lower Extremity Assessment Project), high-level evidence assisting the clinician in this decision was lacking. This chapter details the findings of the LEAP study and other studies examining combat-related injuries and provides the surgeon and other members of the treatment team valuable information and guidance in the management and counseling of the trauma patient with severe limb-threatening trauma.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
22.1 Introduction
More than three out of five accidental injuries in the USA are to the musculoskeletal system. Costs associated with the care of these injuries have been estimated to be $849 billion or 7.7 % of the US gross domestic product (GDP) in the year 2004. Musculoskeletal disease and injury continue to account for the majority of both lost wages and hospital bed days in the USA [1]. We must improve the care of these injuries so that we may help patients rehabilitate from injury and prevent future morbidity.
A small but resource-heavy subset is the high-energy trauma patient with a mangled extremity [2]. The evaluation and subsequent management of this patient group can be a great source of stress for both the patient and the treating surgical team. The decision-making processes are difficult and can be controversial, and the clinical evidence for these decisions has been largely based upon small case series and historical Level V evidence [3]. These data have influenced the treatment of limb-threatening trauma and have potentially led to large numbers of limb amputations with severe lower-extremity trauma where limb salvage may have been technically possible but not recommended [4, 5]. As medical and surgical technology, skills, procedures, and concepts have evolved, so has our ability to salvage limbs previously thought to be unsalvageable. Particular areas of advancement include soft-tissue handling, less invasive fracture management, microvascular repair, and soft-tissue coverage [6–13]. Limb-salvage protocols have been evaluated, and many of them have influenced our current treatment strategies [14, 15]. These studies and others reviewing complicated limb trauma have suggested that early amputation may be preferable due to the mental and physical toll limb salvage can levy on patients [16–18]. Most studies have included small numbers of patients, and their results have correspondingly not yielded definitive results [6, 7, 18, 19].
In an effort to provide evidence for clinicians to rely upon when making amputation versus salvage decisions, a large multicenter, prospective, observational study was undertaken entitled the Lower Extremity Assessment Project (LEAP) [20–22]. Utilizing data from this project and more recent data from military services involved with combat-related injuries, several areas of the amputation – limb-salvage debate – have been explored. Evidence from this trial and others is presented in the following chapter to assist treatment teams in these difficult and complex situations. The goals of this chapter are to present the data from this study and provide a framework for surgical treatment teams to employ when evaluating the high-energy trauma patient with a mangled extremity.
22.2 Traumatic Primary Amputations: Considerations and Completions
The patient presenting with a complete or near-complete traumatic amputation as the result of high-energy trauma requires an evaluation consistent with the latest recommendations of the American College of Surgeons and the principles of Advanced Trauma Life Support [23–25]. Once the patient’s life-threatening issues have been stabilized, attention can then be focused on the injured extremity. It is perhaps best to have the orthopedic surgeon present prior to any surgical intervention. It is typically this surgeon who will follow the patient through subsequent recovery and functional gain with the affected extremity. In addition, any further surgical interventions are likely to be performed by an orthopedic surgeon.
Standard open wound protocols should be followed in accordance with open fracture principles surrounding the acute zone of injury (see Chap. 20). Once the patient is physiologically stable, the zone of injury on the affected limb is defined in the surgical suite, and the limb is deemed appropriate for definitive amputation, and appropriate surgical steps are taken according to the desired amputation level and planned technique (i.e., bone cut lengths, muscle flap coverage, myodesis planning).
In the orthopedic trauma setting, there are three primary lower-extremity amputations we consider appropriate: below-the-knee, above-the-knee, and, in some select cases, through-the-knee. In the high-energy trauma patient, more often than not, the heel pad has been traumatized over the hind foot making the Syme amputation less optimal and rarely used option (Fig. 22.1). The hip disarticulation is also rarely used except for the most severe proximal injuries. This usually includes those with massive soft-tissue injury and/or an obvious vascular and complete sciatic nerve transection. The indications and techniques for the above three primary amputations have been well described [26] and are not the focus of this chapter. However, when contemplating an amputation through-the-knee, the surgeon must critically evaluate the soft-tissue envelope around this tenuous area. If there is any evidence that the zone of injury includes this area, most especially the proximal gastroc-soleus musculature, then there should be strong consideration to proceed with an amputation level above-the-knee. Data from the LEAP study [20, 22, 27] has suggested that through-the-knee amputations do not perform as well as above-the-knee amputations in the mangled extremity patient. This finding was most likely attributed to the condition of the soft-tissue envelope in their patient cohort and to difficulties with prosthetic fitting. In the absence of compromised soft-tissues in this area and in the properly selected patient with experienced prosthetics support, a through-the-knee amputation has been shown to provide good muscular balance and has a low risk for the late development of joint contractures [28].

This 28-year-old male was involved in a high-speed motorcycle crash and sustained significant forefoot and midfoot trauma. The heel pad was severely damaged in this case which happens commonly in these injury patterns. This makes subsequent reconstrutive efforts difficult with amputation levels below the midsection of the tibia (i.e., Syme amputations)
Severe upper extremity injuries, which present as complete or near-complete amputations, warrant special consideration and evaluation by a surgeon who is familiar with reconstruction procedures in this area. The decision-making process in the mangled upper extremity can be challenging, especially when limb salvage becomes an option [29]. Primary amputation may not be in the best interest of some patients as it has been suggested that a sensate hand with minimal prehensile function can outperform a prosthesis [30]. Standard principles of wound care should be employed until appropriate consultation can be obtained. When definitive surgical intervention is required, preservation of length is critical and can decrease the energy needed for the patient to suspend their prosthesis (Fig. 22.2). Furthermore, the increased surface area of the limb can help with load distribution, prosthesis propulsion in space, and counterpressure with task performance [26].

This 16-year-old female was involved in a high-speed motor vehicle crash in which the vehicle rolled multiple times. She sustained a traumatic amputation of the forearm including the entire radius and ulna. The proximal soft-tissue involvement was extensive, and she underwent a proximal amputation leaving 14 cm of residual humerus. She was ultimately fit with a myoelectric hand
Absolute indications for primary limb amputation have been suggested in the literature with varying algorithms. Generally, these indications have included a patient presenting with a total or near-total leg amputation or complete tibial or sciatic nerve transection in an adult [14, 31, 32]. Relative indications have included two or more of the following: concurrent severe ipsilateral foot injury, large intercalary soft-tissue or bone loss, warm ischemia time of greater than 6 h, and severe concurrent multiple injuries (Table 22.1) [8, 15, 31, 33–35]. Uniformly, however, these studies indicate that the clinician’s judgment at the time of initial evaluation is critical; amputation decision-making should employ a multitude of factors. We also advise seeking multispecialty input with this difficult decision (i.e., orthopedics, plastic surgery, general surgery). In one study, a combined approach led to 89 % of patients achieving a successful viable limb, and only 11 % went on to secondary amputation [31].
22.2.1 Outcome of Traumatic Primary Amputations
There is little in the literature reporting the long-term outcome of traumatic amputations. Recently, Dougherty published a study evaluating the outcomes of 123 transtibial amputees from the Vietnam War – 65 % of which were victims of land mines and booby traps. He found that with isolated amputations, these patients led relatively normal lives. However, when concomitant injuries were sustained by these patients, their SF-36 scores lowered, and their incidence of psychological illness increased [36]. Smith et al. [37] published a descriptive study describing outcomes of 20 patients with unilateral transtibial amputations. They found that SF-36 scores were lower than normal age-matched scores in the categories of physical function and role limitations because of physical health problems and pain. Aside from those two sections, scores from the normal population were not significantly different. Lerner et al. [38, 39] evaluated three groups of patients: posttraumatic fracture nonunion, chronic refractory osteomyelitis, and lower-extremity amputation. In their group of 109 patients, they found that the chronic osteomyelitis patients were the most adversely affected among the three groups. Interestingly, 85 % of the amputee patients believed they had been “mentally scarred” by their orthopedic problem, but despite that complaint, they had minimal restriction in lifestyle and activity – a direct contrast to the poorer functioning osteomyelitis group.
In 2004, a study was published which reviewed 161 trauma-related amputation patients that were participants in the LEAP study [27]. This study found no differences in outcomes between the above-the-knee amputees and the below-the-knee amputees. The exception to this finding was with walking speeds in which the below-the-knee group performed better. A key finding in this study was the significantly poorer outcomes of patients that had undergone a through-the-knee amputation. The poorer outcome was associated with worse walking speeds and also less physician-measured satisfaction in terms of clinical, functional, and cosmetic recoveries of their patients. As we noted earlier, we believe the surgeon must critically evaluate the zone of injury prior to proceeding with a through-the-knee amputation. Furthermore, when faced with the decision to proceed with an above-the-knee amputation, surgeons should take whatever steps are necessary to preserve femoral length [40]. It was recently shown that retained length of the femur significantly improves temporospatial and kinematic gait outcomes. Careful attention to the adductors, either with preservation or reconstruction, can benefit this group of patients and improve their mobility.
The outcome of isolated traumatic lower-extremity amputations is mixed but can generally be associated with residual disability and lower outcome scores than the general population. While Dougherty’s [41] study of transtibial amputations demonstrated relatively normal scores with a select population with an isolated lower-extremity injury, other studies indicate substantially poorer outcomes. In another study by Dougherty examining more proximal transfemoral amputations, substantial disability was found in patient follow-up [36]. Smith et al. [37] and the LEAP study [27] also identified significant disability with traumatic amputations in follow-up. These studies indicate that when lower-extremity injuries are among a constellation of traumatic injuries, which they often are, outcomes demonstrate increased disability. An extensive rehabilitation program offered at the treating US Army hospital may have influenced the better outcomes identified in Dougherty’s transtibial amputation study. This finding and those of the LEAP study underscore the need to have high-energy traumatic amputation patients closely followed and managed by a multidisciplinary team including surgeons, rehabilitation physicians, nurses, prosthetists, and therapists. It is also the surgeon’s responsibility to inform patients of expected outcomes and ensure that unrealistic expectations are not confusing patients during their recovery. These discussions can allay patient fears and allow the patient, their families, and support networks to adjust to the trauma and plan ahead for expected changes.
22.3 The Subtotal Amputation Injury: Limb Salvage or Amputation
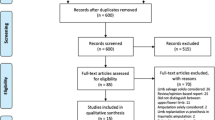
The high-energy trauma patient with a subtotal amputation to an extremity presents immediate challenges to the trauma team. The Lower Extremity Assessment Project (LEAP) was a prospective cohort study of 601 patients who had been admitted to eight Level I trauma centers for the treatment of severe lower-extremity injuries below the distal part of the femur [21]. This study sought to provide evidence for clinicians to use when faced with this dilemma and has recently published 7-year follow-up data [20]. The singular study has produced multiple projects investigating various facets of the lower-extremity injured patient, and many are discussed in the ensuing sections. Inclusion criteria for the LEAP study are listed in Table 22.2 and highlight the severity of trauma evaluated in this study as well as the breadth of injuries included. Please refer to Case 1 in Figs. 22.3a, 22.4, and 22.5c and Case 2 in Figs. 22.6a and 22.7c for limb-salvage and amputation examples.

This 20-year-old female sustained severe right lower leg trauma after being run over by a personal watercraft. (a–d) Initial surgical evaluation and debridement with subsequent external fixation. (c) Extensive soft-tissue loss and intact neurovascular bundle posterior to the tibia fracture. At this time, we confirmed our decision to salvage the limb. This wound had a vacuum-assisted closure device until the plastic surgery team could evaluate and ultimately place a tissue flap over the wound (Case and photographs courtesy of David P. Barei, MD)

(a, b) Anterior-posterior and lateral radiographic views of the injured lower extremity. Note significant soft-tissue shadow highlighting the extensive damage. This patient was fortunate and did not sustain substantial bone loss. (c, d) Provisional external fixation was employed to restore length, alignment, and rotation to the injured limb. (e, f) One year post-injury radiographs demonstrating complete union of both the tibia and fibula (Case and photographs courtesy of David P. Barei, MD)

(a–c) Clinical follow-up demonstrating good result of limb salvage with this patient. She was able to gain excellent range of motion and had an outstanding support network aiding her in the recovery process (Case and photographs courtesy of David P. Barei, MD)

This 40-year-old female was involved in a severe motorcycle crash. In Figures (a–c) profound soft-tissue and osseous damage was sustained. Emergency department evaluation demonstrated the foot be avascular. The patient underwent emergent operative intervention and underwent an acute above-the-knee amputation (d). She returned to the operating suite several times over the ensuing days for further debridement and, ultimately, a disarticulation of the hip joint. Radiographs for this patient are shown in Fig. 22.7

(a–c) Radiographs of the patient pictured in Fig. 22.6a
22.3.1 Factors Influencing Initial Salvage Decisions
Initial decisions for the acute trauma patient with a severely injured lower extremity include immediate amputation (i.e., within the first 24 h) or delayed (i.e., secondary procedure with the first hospitalization) [8, 14, 15, 17, 42, 43]. There are a multitude of factors influencing this decision: those related directly to the leg injury itself, the extent and severity of associated injuries, the physiologic reserve of the patient, and their social support network. The training and experience of the attending surgeon may also play a role in the decision-making process [44].
Mackenzie et al. published the results of a survey pertaining to surgeons and their decision to amputate or reconstruct traumatized lower extremities. This study highlighted various factors that different specialties (general surgeons and orthopedic surgeons) deemed most important to consider in the critical decision of amputation versus salvage (Table 22.3). Interesting perspectives representative of specialty-specific training and goals were identified. Namely, the general surgeons tended to emphasize the overall physiologic condition and reserve of the patient as a whole (the injury-severity scale, limb ischemia), whereas the orthopedic surgeon emphasized functional outcome prognosis (nerve integrity, soft-tissue coverage, limb ischemia). The study conclusions suggest that the main factor influencing surgeons on the question of salvageable limbs is apparent soft-tissue damage: muscle injury, absence of sensation, arterial injury, and vein injury. Patient factors were found to play much less of a role, although alcohol consumption and socioeconomic status were noted to be of some influence [44].
22.3.2 Lower-Extremity Injury-Severity Scales and Scores: Tools for Assisting Surgeons with Salvage or Amputation Decisions
Lower-extremity injury-severity scores were developed by clinicians to assist surgical teams in making the often difficult initial decision of whether to attempt limb salvage or amputate a severely traumatized extremity. Surgeons have hypothesized that patients who undergo initial salvage attempts but subsequently require later amputation have worse outcomes than those who have early amputation. This makes intuitive sense and was shown to be correct in the LEAP study [16] and highlights the importance of early and accurate selection on which patients should proceed with a limb amputation during their first hospitalization.
Several studies [31, 33, 45–47] have examined the application of high-energy lower-extremity trauma scoring systems to patients with severe lower-extremity trauma. The LEAP study [21] contained the largest patient cohort of 565 prospectively evaluated high-energy lower-extremity injured patients. Each patient in this study had five well-known injury-severity scoring systems applied to their case in an effort to determine the clinical utility of each system [45]. The five systems evaluated were the Mangled Extremity Severity Score (MESS) [29, 48], the Limb Salvage Index (LSI) [32], the Predictive Salvage Index (PSI) [34], the Nerve Injury, Ischemia, Soft-Tissue Injury, Skeletal, Shock, and Age of Patient Score (NISSSA) [49], and the Hannover Fracture Scale (HFS) [50]. Table 22.4 represents the components of each injury-severity scale with the addition of a newer scale that was developed in India to predict hospital days required, flap requirements, rate of infection, and the number of secondary procedures required. This scale also incorporates patient comorbidities but emphasized primarily the evaluation of type IIIB open tibia fractures [51]. It was not assessed in the LEAP trial but is included for the sake of completeness. See Tables 22.5, 22.6, 22.7, 22.8, and 22.9 for details on each extremity trauma scale.
When reviewing the initial studies for each of these instruments, reports indicated both high sensitivity and specificity for their respective scores [29, 32, 34, 48, 49]. However, when these scoring instruments have been evaluated subsequently by other clinicians, the initial results have been unable to reproduce (Table 22.10) with widely varying sensitivity and specificity values. The differences among these instruments (typically a higher specificity) demonstrate that they may be more helpful to treatment teams in determining which injuries may support entry of the injured extremity into a limb-salvage pathway [45] and not to which extremities should undergo immediate amputation. The sensitivities were generally low in the LEAP study demonstrating that their accuracy at predicting which extremities may eventually require amputation is poor and certainly should not be relied upon to make acute treatment decisions. Furthermore, in the face of low test sensitivity, placing too much emphasis upon these scores may delay an inevitable amputation risking complications in patient care potentially resulting in sepsis and even death [42].
Bosse et al. and Bonanni et al. [33, 45] were unable to recommend any scale for independent use in determining the fate of an injured limb. With the initial presentation of a trauma patient, they concluded that lower-extremity injury-severity scales have limited usefulness and that scores at or above respective amputation thresholds should be used cautiously in decision-making with high-energy trauma patients. Their utility is in providing a list of the factors to consider when making the clinical decision.
22.3.3 Lower-Extremity Injury-Severity Scales and Scores: Predicting Functional Outcomes of Salvaged Limbs After Limb-Threatening Trauma
It has been hypothesized that lower-extremity injury-severity scores may have utility in the accurate prediction of functional outcome in the limbs that underwent salvage after severe trauma. This important and useful question has been studied recently in a number of studies [33, 46, 52, 53]. Ly et al. [53] evaluated the clinical and functional outcomes of the patient cohort in the LEAP study as determined by the Sickness Impact Profile [54, 55] and the patients’ scores on the MESS, PSI, and LSI lower-extremity injury-severity scores. They found no correlation among these instruments with patient clinical or functional outcomes. A unique point that this study investigated was the specific evaluation of functional scores on patients in whom the injury-severity threshold scores had recommended an amputation, but the patients had undergone limb-salvage instead. Very interestingly, these “amputation-recommended” patients had outcome scores that were no worse than those patients who had salvaged limbs and had injury-severity scores indicating that amputation was not recommended. Durham et al. [46] studied 30 limbs that had undergone limb salvage and had similar findings as Ly et al. Based upon phone interviews and clinic visits where return to work, impairment, and disability were assessed, they also concluded that none of the extremity injury scales could predict functional outcome.
22.3.4 Lower-Extremity Injury-Severity Scales and Scores: Summary
Whenever evaluating patients and deciding upon optimal care for their injured limb, due caution should be exercised when interpreting the lower-extremity injury-severity scales. This holds true with both initial management and extrapolating ultimate functional outcomes with patients. It is the author’s opinion that these lower-extremity scoring systems should still play a role in the management decisions for some patients but should simply be used as one data point among many in the complex processes surrounding the care of the high-energy trauma patient.
22.3.5 Outcomes in Patients Undergoing Limb Salvage or Amputation for Limb-Threatening Injuries
In 2002, Bosse et al. [21] and LEAP study group published their initial report on a prospective cohort of 569 patients that had sustained high-energy lower-extremity trauma from March 1994 to June 1997. The patients in this study had either undergone limb salvage or amputation and were followed prospectively for 24 months and then reported on again at 7-year follow-up [20].
The initial report demonstrated that patients had similar functional outcomes regardless of whether they underwent limb reconstruction/salvage or amputation. The results also indicated that although the outcomes were similar, both groups had substantial levels of disability, and only half had returned to work at 2 years post-injury. Indeed, patients in both groups were able to show significant improvement over the study period, but an important overreaching finding of the study was the profound disability and persistently low psychosocial-functioning subscale [54, 56].
This study was also able to enlighten surgeons on particular factors not related to the injury itself that may predispose some trauma patients to a poorer or less than optimal outcome. These included a lower level of education, poverty, lack of private health insurance, smoking, and involvement with disability-compensation litigation [21]. The elucidation of these factors provides areas for treatment teams to intervene and assist patients in achieving a better outcome. We advocate for the early involvement and intervention by psychosocial and vocational rehabilitation specialists. Their function in the patient’s recovery we believe is imperative and a key component for a better functional outcome. With their expertise, they can directly address the variables listed above and change or even prevent adverse outcomes.
In addition to the listed factors above, self-efficacy and an involved social support network are important determinants of outcome and should be emphasized in rehabilitation [57–59]. The orthopedic surgeon evaluating this patient in the outpatient setting can be instrumental in this area and help empower the social support network to assist the patient through both the difficult physical and mental recoveries. The orthopedist is also likely the only clinician who can help determine the activity level of the patient in the postoperative time frame and, with this knowledge and assistance from the social workers and disability specialists, can help make vocational retraining possible. Both of the above functions should help facilitate the patient’s return to work as excessive delay in this area could potentially lead to poorer outcomes [60, 61].
Longer-term follow-up on the LEAP patient cohort was published at 7 years post-injury [20]. Perhaps unexpectedly, one-half of the patients in the LEAP study remained “severely” disabled and one-quarter were “very severely” disabled [54, 55]. Only one-third of the patients had outcome scores similar to the general population. As found in the initial LEAP 2-year results, there were no significant differences identified among limb-salvage and amputation groups. This follow-up study confirmed and added other factors that were found to be predictive of poor outcomes in the LEAP patient cohort: older age, female gender, nonwhite race, lower education level, living in a poor household, current or previous smoking history [62], low self-efficacy, poor self-reported health status before the injury, and involvement with the legal system in an effort to obtain disability payments. Conclusions drawn from this study warrant attention from treatment teams and do not necessarily involve the acute surgical management of this traumatized population. The optimization of recovery in these patients should emphasize the involvement of professionals who can address certain areas of recovery beyond the operating theater, namely, job retraining, intensive rehabilitative therapy, and education [63–65]. Furthermore, educating patients and their families on realistic and typical expected outcomes is important, as many patients will foster unrealistic expectations. The presence and mental fixation on these unrealistic expectations may predispose patients to poorer outcomes and generalized dissatisfaction with their condition and care [20, 60, 61].
22.3.6 Outcomes of the Mangled Foot and Ankle
A specific subset of patients within the LEAP study that underwent limb salvage with mangled foot and ankle trauma was recently reported upon [66]. This cohort included 174 patients with severely injured foot or hindfoot injuries. The spectrum of injuries included mostly complex foot trauma and tibial pilon fractures. Salvage was undertaken in 116 patients and 58 had an immediate BKA. Assessed outcomes included primarily the Sickness Impact Profile, walking speed, rehospitalizations related to injury complications, time to full weightbearing, visual analog pain scale, and return to work. At 2-year follow-up, the authors found that the limb-salvage group, those that had free tissue transfers and/or ankle fusions, had significantly poorer outcomes than the standard BKA group with standard skin flap design closure. This relationship was not found with standard soft-tissue coverage in the salvage group, which highlights the priority of careful soft-tissue management, specifically that around the vulnerable heel pad [67]. The greatest deficit identified in these study groups revolved around the psychosocial aspect of the limb-salvage group. This demonstrates, as shown in the LEAP study as well, the immense psychological toll these injuries exhibit upon patients during their recovery and onwards.
Another recent study reviewed the outcome of 63 military service members with 89 mangled lower limbs resulting from blast injuries sustained in a combat environment [68]. This study, along with that of Ellington et al. [66], showed that open fractures of the hindfoot were associated with higher rates of amputation, 29 % in this study with six of those conducted for chronic pain 18 months following the injury. The authors also noted higher rates of amputation when the trauma was associated with a vascular injury. At final follow-up, 74 % of the injured limbs still had persisting pain and disability related to injury. Only 14 % of the service members were ultimately fit to return to their preinjury duties.
Adding to the mangled lower-extremity data set from a combat theater, 90 % of patients in another study (91 of 102 patients) sustained open calcaneal fractures [69] from a blast-type mechanism. With an average of 4 years follow-up, 42 % of this cohort went on to amputation. Fifteen percent of these were done in a delayed fashion. This study highlighted several factors predictive of eventual amputation: blast-type mechanism, plantar wound location and size, and escalating Gustilo-Anderson classification type. It is also quite interesting to note that the authors reported statistically significant lower visual analog scores (2.1 compared to 4.0) in the amputation group than the limb-salvage group.
22.3.7 Complications in the Treatment of Severe Lower-Extremity Trauma
The management of limb-threatening trauma is challenging and complications can be significant. Harris et al. [70] reported that among the 149 amputations performed among the LEAP patients, there was a 5.4 % amputation revision rate. There was an overall 24 % complication rate with most of these being reported at 3 months post-injury. The most common complications were wound infection (34 %) followed by wound dehiscence (13 %). In the 371 limb-salvage patients, 3.9 % required a late amputation, which was defined as a limb undergoing amputation after the initial hospitalization. Most complications were noted at 6 months post-injury and included a total of 37.7 % of this group. Again, the most common complication noted was wound infection (23.2 %). The complications of osteomyelitis and nonunions were, not surprisingly, seen predominantly in the salvage group and entailed 8.6 % and 31 %, respectively.
Soft-tissue coverage associated with limb salvage and reconstruction is also associated with significant complications and has been reported to occur in 53 % of flap procedures within the LEAP patient cohort. Operative intervention was required in 87 % of these patients [71]. Rehospitalization, often a setback in recovery, occurred in one-third of LEAP study patients and involved the limb-salvage/reconstruction group more than the amputation group.
When complications become unsalvageable or limb-salvage techniques fail for various reasons, some patients may opt for an elective amputation rather than proceed with further efforts. Choosing an elective amputation in this situation is a particularly sensitive issue and certainly one of the most difficult decisions to make for the patient. The time already invested in recovery and the lure of anticipated functional gain can make this decision all the more challenging. Quon et al. [72] reviewed a small cohort of patients undergoing elective amputations for a functionally impaired lower limb that limited those patients’ ability to do their everyday activities. They identified three key factors in their patients’ decisions: pain, function, and participation. While the study subjects voiced differing reasons within these categories, basic tenets of the study related to patients feeling the leg was potentially holding them back and that amputating the leg may afford them decreased pain, improved function with daily activities, and future participation in hobbies or activities they were previously forced to give up due to the trauma.
Complications in the management of this severely injured group of patients are sadly unavoidable. It is in our and our patients best interest to understand the nature of the complications and how then to best avoid them. From the initial evaluation and subsequent follow-up of these patients, treatment teams should not underestimate the difficult nature of the recovery process and the potential for complications and secondary procedures. Further, a future area of research may be warranted with investigation into when salvage efforts have stalled and patients may be better suited with an elective amputation over continued salvage techniques. As clinicians we have a duty to inform patients on all treatment options, and perhaps early involvement of an amputation team may help some patients opt for an earlier amputation rather than struggle with the ostensibly successful limb salvage with an unpredictable recovery.
22.3.8 Psychological Distress in Patients with Severely Injured Lower Extremities
Accompanying the significant challenges with physical recovery and impairment is an often underappreciated source of morbidity with orthopedic trauma patients – psychological distress and mental illness [73, 74]. This is especially evident in the high-energy lower-extremity trauma patient where limb salvage and amputations are being debated and subsequent recoveries managed. During the course of the LEAP study, patients were evaluated for psychological distress [75] utilizing the Brief Symptom Inventory [76, 77]. At 2 years post-injury, 42 % of the patients screened positive for a psychological disorder, yet only 22 % had reported receiving any mental health services. Almost 20 % of the study group reported severe phobic anxiety and/or depression. The authors of the study were able to identify factors that were likely to be associated with patients that had psychological distress. These included poorer physical function, younger age, nonwhite race, poverty, a likely drinking problem, neuroticism, a poor sense of self-efficacy, and limited social support. Interestingly, some of these same factors have been attributed to chronic pain syndromes which could certainly exacerbate any coexisting psychological distress these patients may be suffering from [78].
Another study utilizing the LEAP study participants worked to characterize the relationships between pain, psychological distress, and physical function in the early and later stages of recovery [79]. They reported that the presence of depression and anxiety, at any detectable level, led to decreased levels of function during recovery after injury. Complimenting this data set, a study by Castillo et al. [80] showed that during the early phases of recovery, levels of pain were able to predict corresponding levels of anxiety and depression symptoms. Stronger relationships were seen with anxiety and pain throughout the recovery stages. Based upon these and other studies, it is quite clear that the patient with severe lower-extremity trauma would benefit significantly from interventions specifically aimed at decreasing negative emotions, especially anxiety, in the recovery period.
As emphasized previously, the orthopedic surgeon is most likely going to be the primary coordinator of care with these patients in the postoperative period during their lengthy functional recoveries. Along with recognizing the physical dysfunction and instituting appropriate referrals for therapy and job retraining, the treating surgeon must also be astute enough to evaluate and screen these traumatized patients for psychological distress. If mental distress is suspected or identified, appropriate consultation or referral should be initiated to a provider trained in this area. Furthermore, by understanding and recognizing potential risk factors for psychological distress and thus poorer outcomes with this patent population (i.e., drinking problems, poor social support network, or poor self-efficacy), prophylactic referrals can be made early in the patient’s recovery. Ultimately, for patients to be given the best chance for the most favorable outcome, the physical and psychological needs of this population should to be addressed simultaneously [75]. Adding directed therapy toward these areas could prove to decrease acute pain associated with recovery and improve overall functional gains.
22.3.9 Societal Costs Associated with Limb Salvage and Amputation
An argument we have heard and understand is that of the cost of limb salvage and its toll on society in comparison to a “quick amputation and be done with it” attitude… “let the patient get on with their life.” The cost burden of the limb-salvage and amputation debate was recently reported [2], and the results directly counter what many have argued in the past. At 2 years of follow-up, both groups had essentially the same healthcare costs. However, projected lifetime costs were $509,000 for amputees and $163,000 for limb-salvage patients (2002 US dollar figures) – over a threefold difference. The difference was mainly attributed to the repair and replacement costs associated with prostheses for the amputation population, which had an estimated 40–45 years of life remaining. In regard to complications, they found a 46 % increase in costs if patients had required a rehospitalization – a finding that underscores the importance of clinicians having a solid understanding of risk factors for both complications and poorer outcomes.
22.4 The Open Fracture with Severe Nerve Injury
The management of severe limb-threatening injuries is challenging and often requires difficult decisions to be made acutely. Predicting the outcome of patients with this type of trauma (Table 22.2) has proved challenging, and the utility of limb-salvage predictive scores has been shown to be limited. A repetitive and concerning theme in the scientific literature surrounding limb salvage and amputation is the severe open fracture with associated nerve injury and purported poor results of 60–100 % disability with this type of injury [81–83]. This scenario represents a unique conundrum in the decision-making process.
The loss of foot plantar sensation has been ingrained into the trauma surgeon’s psyche as a major, if not sometimes the primary predictor of acute amputation. In fact, MacKenzie et al. [44] showed that nearly 40 % of orthopedic surgeons place nerve integrity and plantar sensation as the primary determinant in the decision to amputate or reconstruct (Table 22.3). Often, this decision is made based on initial emergency room evaluation even though this sometimes rudimentary exam has been shown to be unpredictable [35]. The influence of nerve integrity on the trauma community has been borne out by its direct and independent inclusion into three of the major limb-salvage prediction scales: the LSI, NISSSA, and HFS (Tables 22.4, 22.6, 22.8, and 22.9).
The insensate foot was evaluated among 55 patient cohort of the LEAP study [84]. This group presented to the emergency department with an insensate foot and underwent either amputation (26 patients) or limb salvage (29 patients). The insensate-salvage group was also matched and compared with a sensate-salvage group as a control group in the study. The authors identified some interesting and important findings directly impacting commonly held beliefs pertaining to limb-salvage versus amputation debates and predicted outcomes. First and foremost, patients that had absent plantar sensation demonstrated substantial impairment at final follow-up. However, their outcomes were similar and appeared to be unaffected whether undergoing amputation or limb salvage. Second and perhaps most interesting, the patients with the insensate foot on presentation that underwent limb salvage did not have worse outcomes than the matched cohort with intact sensation that underwent limb salvage. This included no differences in final plantar sensation or the need for late amputation. In fact, 67 % of the patients in the insensate foot group regained normal foot sensation over the study period – a highlight that supports increased diligence in treatment decisions utilizing emergency department nerve exams. Ultimately, the 2-year outcome of patients that had undergone limb salvage with an insensate foot did not appear to be influenced or adversely affected by the presence or absence of plantar sensation [84].
More recently, Beltran et al. [85] reviewed 32 open type III tibia fractures with a total of 43 peripheral nerve injuries (peroneal or tibial) sustained in a combat environment. Complimenting the LEAP data, this study specifically investigated nerve injuries sustained with high-energy mechanisms such as seen in military combat. With nearly 2-year follow-up, 89 % of injured motor nerves were functional, and 93 % of sensory nerve injuries were functional as well. Full return of function was seen in 37 % of the motor nerve injuries and in 25 % of sensory nerves. The authors conclude that improvement can be expected in 50 % of motor nerve injuries and in 27 % of sensory nerve injuries.
The decisions in these analyses and others are often based upon emergency department evaluation and not upon direct surgical observation. The initial evaluation demonstrating a loss of plantar sensation can easily be attributed to a transient neurapraxia from compression or stretch and/or temporary ischemia, which can be reversible. Furthermore, in the combat situation, both blast injuries and high-velocity gunshot wounds can cause local tissue cavitation leading to nerve dysfunction. The intraoperative finding of complete nerve transection or segmental neural element loss could be suggestive of an absolute indication for primary limb amputation, especially in light of associated vascular injuries or other severe traumas. However, it is important to note that often clinicians treat patients with insensate feet in the clinical setting, namely, in the diabetic and spinal cord injury patient populations [84]. In the surgical suite, we do not advocate invasive surgical exploration of nerve structures in the lower extremity when they are not already exposed secondary to the trauma itself. This practice is associated with unwarranted tissue damage and should be avoided. With evidence to support return of both motor and sensory functions including plantar sensation during recovery, the reliance specifically upon plantar sensation and nerve function in general in the lower extremity during the initial physical exam finding should be avoided in the amputation decision-making process.
22.5 Summary
The high-energy lower-extremity trauma patient presents many challenges to treatment teams. Past literature has not been overly supportive of limb salvage and often makes the point that early amputation is advantageous to save patients from lengthy suffering [15, 17]. However, as technology and surgical concepts have evolved, so have our abilities to salvage limbs previously thought to be candidates only for amputation. These salvaged limbs, although demonstrating generally poor outcomes, have been shown to have equivalent results to limbs treated with primary amputation [20–22] and entail an equivalent of 2-year healthcare costs and substantial savings over the long term.
Often, given the option of limb salvage or amputation, most patients opt to save their extremity rather than undergo an amputation. While data presented here and in the LEAP data show equivalent results among the salvage/amputation groups, it should be noted that most of the data were derived from care patients had received at Level I trauma centers. It has been argued that these centers, with their experienced trauma staff, may impart different outcomes than patients treated elsewhere [86].
We believe that limb salvage is a reasonable goal for clinicians and patients at experienced Level I trauma centers. The LEAP data and other studies present sufficient evidence to support this conclusion. The early involvement of post-acute-care services, such as therapists, rehabilitation specialists, psychologists, and many others, is imperative for the optimization of patient outcomes and potentially holds the highest value in recovery efforts. Diligence, thoughtful care, and presenting realistic expectations will allow these traumatized patients to achieve their best recovery and functional outcomes.
References
Andersson G, American Academy of Orthopaedic Surgeons. United States Bone and Joint Initiative: The Burden of Musculoskeletal Diseases in the United States (BMUS), Third Edition, 2014. Rosemont, IL. Available at http://www.boneandjointburden.org. Accessed on 15 July 2015.
MacKenzie EJ, Jones AS, Bosse MJ, Castillo RC, Pollak AN, Webb LX, et al. Health-care costs associated with amputation or reconstruction of a limb-threatening injury. J Bone Joint Surg Am. 2007;89(8):1685–92.
Wright JG. A practical guide to assigning levels of evidence. J Bone Joint Surg Am. 2007;89(5):1128–30.
Dillingham TR, Pezzin LE, MacKenzie EJ. Incidence, acute care length of stay, and discharge to rehabilitation of traumatic amputee patients: an epidemiologic study. Arch Phys Med Rehabil. 1998;79(3):279–87.
Dillingham TR, Pezzin LE, MacKenzie EJ. Limb amputation and limb deficiency: epidemiology and recent trends in the United States. South Med J. 2002;95(8):875–83.
Godina M. Early microsurgical reconstruction of complex trauma of the extremities. Plast Reconstr Surg. 1986;78(3):285–92.
Francel TJ, Vander Kolk CA, Hoopes JE, Manson PN, Yaremchuk MJ. Microvascular soft-tissue transplantation for reconstruction of acute open tibial fractures: timing of coverage and long-term functional results. Plast Reconstr Surg. 1992;89(3):478–87; discussion 88–9.
Caudle RJ, Stern PJ. Severe open fractures of the tibia. J Bone Joint Surg Am. 1987;69(6):801–7.
Anglen J, Kyle RF, Marsh JL, Virkus WW, Watters III WC, Keith MW, et al. Locking plates for extremity fractures. J Am Acad Orthop Surg. 2009;17(7):465–72.
Collinge CA, Sanders RW. Percutaneous plating in the lower extremity. J Am Acad Orthop Surg. 2000;8(4):211–6.
Haidukewych GJ. Innovations in locking plate technology. J Am Acad Orthop Surg. 2004;12(4):205–12.
Haidukewych GJ, Ricci W. Locked plating in orthopaedic trauma: a clinical update. J Am Acad Orthop Surg. 2008;16(6):347–55.
Gorman PW, Barnes CL, Fischer TJ, McAndrew MP, Moore MM. Soft-tissue reconstruction in severe lower extremity trauma. A review. Clin Orthop Relat Res. 1989;243:57–64.
Lange RH. Limb reconstruction versus amputation decision making in massive lower extremity trauma. Clin Orthop Relat Res. 1989;243:92–9.
Hansen Jr ST. The type-IIIC tibial fracture. Salvage or amputation. J Bone Joint Surg Am. 1987;69(6):799–800.
Smith DG, Castillo R, MacKenzie E, Bosse MJ, Group TLS. Functional outcomes of patients who have late amputation after trauma is significantly worse than for those who have early amputation. Orthopaedic trauma association 2003 annual meeting; 10/9/2003; Salt Lake City, UT2003.
Hansen Jr ST. Overview of the severely traumatized lower limb. Reconstruction versus amputation. Clin Orthop Relat Res. 1989;243:17–9.
Georgiadis GM, Behrens FF, Joyce MJ, Earle AS, Simmons AL. Open tibial fractures with severe soft-tissue loss. Limb salvage compared with below-the-knee amputation. J Bone Joint Surg Am. 1993;75(10):1431–41.
Francel TJ. Improving reemployment rates after limb salvage of acute severe tibial fractures by microvascular soft-tissue reconstruction. Plast Reconstr Surg. 1994;93(5):1028–34.
MacKenzie EJ, Bosse MJ, Pollak AN, Webb LX, Swiontkowski MF, Kellam JF, et al. Long-term persistence of disability following severe lower-limb trauma. Results of a seven-year follow-up. J Bone Joint Surg Am. 2005;87(8):1801–9.
Bosse MJ, MacKenzie EJ, Kellam JF, Burgess AR, Webb LX, Swiontkowski MF, et al. An analysis of outcomes of reconstruction or amputation after leg-threatening injuries. N Engl J Med. 2002;347(24):1924–31.
MacKenzie EJ, Bosse MJ, Kellam JF, Burgess AR, Webb LX, Swiontkowski MF, et al. Characterization of patients with high-energy lower extremity trauma. J Orthop Trauma. 2000;14(7):455–66.
Alexander RH, Proctor HJ, American College of Surgeons, Committee on Trauma. Advanced trauma life support program for physicians: ATLS. 5th ed. Chicago: American College of Surgeons; 1993.
Trauma ACoSCo. Advanced trauma life support for doctors ATLS: manuals for coordinators and faculty. 8th ed. Chicago: American College of Surgeons; 2008.
Trauma ACoSCo. Advanced trauma life support for doctors: student course manual. 6th ed. Chicago: American College of Surgeons; 1997.
Pinzur M. Amputations in trauma. In: Browner BD, Jupiter J, Levine A, Trafton P, Krettek C, editors. Skeletal trauma: basic science, management, and reconstruction, vol. 2. 4th ed. Philadelphia: Saunders/Elsevier; 2009. p. 2 v. xxv, 2882, I56 p.
MacKenzie EJ, Bosse MJ, Castillo RC, Smith DG, Webb LX, Kellam JF, et al. Functional outcomes following trauma-related lower-extremity amputation. J Bone Joint Surg Am. 2004;86-A(8):1636–45.
Pinzur MS, Smith DG, Daluga DJ, Osterman H. Selection of patients for through-the-knee amputation. J Bone Joint Surg Am. 1988;70(5):746–50.
Johansen K, Daines M, Howey T, Helfet D, Hansen Jr ST. Objective criteria accurately predict amputation following lower extremity trauma. J Trauma. 1990;30(5):568–72; discussion 72–3.
Pinzur MS, Angelats J, Light TR, Izuierdo R, Pluth T. Functional outcome following traumatic upper limb amputation and prosthetic limb fitting. J Hand Surg Am. 1994;19(5):836–9.
Dagum AB, Best AK, Schemitsch EH, Mahoney JL, Mahomed MN, Blight KR. Salvage after severe lower-extremity trauma: are the outcomes worth the means? Plast Reconstr Surg. 1999;103(4):1212–20.
Russell WL, Sailors DM, Whittle TB, Fisher Jr DF, Burns RP. Limb salvage versus traumatic amputation. A decision based on a seven-part predictive index. Ann Surg. 1991;213(5):473–80; discussion 80–1.
Bonanni F, Rhodes M, Lucke JF. The futility of predictive scoring of mangled lower extremities. J Trauma. 1993;34(1):99–104.
Howe Jr HR, Poole Jr GV, Hansen KJ, Clark T, Plonk GW, Koman LA, et al. Salvage of lower extremities following combined orthopedic and vascular trauma. A predictive salvage index. Am Surg. 1987;53(4):205–8.
Lange RH, Bach AW, Hansen Jr ST, Johansen KH. Open tibial fractures with associated vascular injuries: prognosis for limb salvage. J Trauma. 1985;25(3):203–8.
Dougherty PJ. Long-term follow-up of unilateral transfemoral amputees from the Vietnam war. J Trauma. 2003;54(4):718–23.
Smith DG, Horn P, Malchow D, Boone DA, Reiber GE, Hansen Jr ST. Prosthetic history, prosthetic charges, and functional outcome of the isolated, traumatic below-knee amputee. J Trauma. 1995;38(1):44–7.
Lerner RK, Esterhai Jr JL, Polomano RC, Cheatle MD, Heppenstall RB. Quality of life assessment of patients with posttraumatic fracture nonunion, chronic refractory osteomyelitis, and lower-extremity amputation. Clin Orthop Relat Res. 1993;295:28–36.
Lerner RK, Esterhai Jr JL, Polomono RC, Cheatle MC, Heppenstall RB, Brighton CT. Psychosocial, functional, and quality of life assessment of patients with posttraumatic fracture nonunion, chronic refractory osteomyelitis, and lower extremity amputation. Arch Phys Med Rehabil. 1991;72(2):122–6.
Bell JC, Wolf EJ, Schnall BL, Tis JE, Tis LL, Potter BK. Transfemoral amputations: the effect of residual limb length and orientation on gait analysis outcome measures. J Bone Joint Surg Am. 2013;95(5):408–14.
Dougherty PJ. Transtibial amputees from the Vietnam War. Twenty-eight-year follow-up. J Bone Joint Surg Am. 2001;83-A(3):383–9.
Bondurant FJ, Cotler HB, Buckle R, Miller-Crotchett P, Browner BD. The medical and economic impact of severely injured lower extremities. J Trauma. 1988;28(8):1270–3.
Dirschl DR, Dahners LE. The mangled extremity: when should it be amputated? J Am Acad Orthop Surg. 1996;4(4):182–90.
MacKenzie EJ, Bosse MJ, Kellam JF, Burgess AR, Webb LX, Swiontkowski MF, et al. Factors influencing the decision to amputate or reconstruct after high-energy lower extremity trauma. J Trauma. 2002;52(4):641–9.
Bosse MJ, MacKenzie EJ, Kellam JF, Burgess AR, Webb LX, Swiontkowski MF, et al. A prospective evaluation of the clinical utility of the lower-extremity injury-severity scores. J Bone Joint Surg Am. 2001;83-A(1):3–14.
Durham RM, Mistry BM, Mazuski JE, Shapiro M, Jacobs D. Outcome and utility of scoring systems in the management of the mangled extremity. Am J Surg. 1996;172(5):569–73; discussion 73–4.
O'Sullivan ST, O'Sullivan M, Pasha N, O'Shaughnessy M, O'Connor TP. Is it possible to predict limb viability in complex Gustilo IIIB and IIIC tibial fractures? A comparison of two predictive indices. Injury. 1997;28(9–10):639–42.
Helfet DL, Howey T, Sanders R, Johansen K. Limb salvage versus amputation. Preliminary results of the Mangled Extremity Severity Score. Clin Orthop Relat Res. 1990;256:80–6.
McNamara MG, Heckman JD, Corley FG. Severe open fractures of the lower extremity: a retrospective evaluation of the Mangled Extremity Severity Score (MESS). J Orthop Trauma. 1994;8(2):81–7.
Tscherne H, Gotzen L. Fractures with soft tissue injuries. Berlin/New York: Springer; 1984. vi, 164 p. p.
Rajasekaran S, Naresh Babu J, Dheenadhayalan J, Shetty AP, Sundararajan SR, Kumar M, et al. A score for predicting salvage and outcome in Gustilo type-IIIA and type-IIIB open tibial fractures. J Bone Joint Surg Br. 2006;88(10):1351–60.
Lin CH, Wei FC, Levin LS, Su JI, Yeh WL. The functional outcome of lower-extremity fractures with vascular injury. J Trauma. 1997;43(3):480–5.
Ly TV, Travison TG, Castillo RC, Bosse MJ, MacKenzie EJ. Ability of lower-extremity injury severity scores to predict functional outcome after limb salvage. J Bone Joint Surg Am. 2008;90(8):1738–43.
Bergner M, Bobbitt RA, Carter WB, Gilson BS. The sickness impact profile: development and final revision of a health status measure. Med Care. 1981;19(8):787–805.
Bergner M, Bobbitt RA, Kressel S, Pollard WE, Gilson BS, Morris JR. The sickness impact profile: conceptual formulation and methodology for the development of a health status measure. Int J Health Serv. 1976;6(3):393–415.
de Bruin AF, de Witte LP, Stevens F, Diederiks JP. Sickness impact profile: the state of the art of a generic functional status measure. Soc Sci Med. 1992;35(8):1003–14.
Berkman L, Glass T. Social integration, social networks, social support, and health. In: Berkman L, Kawachi I, editors. Social epidemiology. New York: Oxford University Press; 2000.
MacKenzie EJ, Morris Jr JA, Jurkovich GJ, Yasui Y, Cushing BM, Burgess AR, et al. Return to work following injury: the role of economic, social, and job-related factors. Am J Public Health. 1998;88(11):1630–7.
MacKenzie EJ, Bosse MJ. Factors influencing outcome following limb-threatening lower limb trauma: lessons learned from the Lower Extremity Assessment Project (LEAP). J Am Acad Orthop Surg. 2006;14(10 Spec No):S205–10.
O'Toole RV, Castillo RC, Pollak AN, MacKenzie EJ, Bosse MJ. Surgeons and their patients disagree regarding cosmetic and overall outcomes after surgery for high-energy lower extremity trauma. J Orthop Trauma. 2009;23(10):716–23.
O'Toole RV, Castillo RC, Pollak AN, MacKenzie EJ, Bosse MJ. Determinants of patient satisfaction after severe lower-extremity injuries. J Bone Joint Surg Am. 2008;90(6):1206–11.
Castillo RC, Bosse MJ, MacKenzie EJ, Patterson BM. Impact of smoking on fracture healing and risk of complications in limb-threatening open tibia fractures. J Orthop Trauma. 2005;19(3):151–7.
Archer KR, MacKenzie EJ, Bosse MJ, Pollak AN, Riley 3rd LH. Factors associated with surgeon referral for physical therapy in patients with traumatic lower-extremity injury: results of a national survey of orthopedic trauma surgeons. Phys Ther. 2009;89(9):893–905.
Archer KR, Castillo RC, Mackenzie EJ, Bosse MJ. Gait symmetry and walking speed analysis following lower-extremity trauma. Phys Ther. 2006;86(12):1630–40.
Castillo RC, MacKenzie EJ, Archer KR, Bosse MJ, Webb LX. Evidence of beneficial effect of physical therapy after lower-extremity trauma. Arch Phys Med Rehabil. 2008;89(10):1873–9.
Ellington JK, Bosse MJ, Castillo RC, MacKenzie EJ, Group LS. The mangled foot and ankle: results from a 2-year prospective study. J Orthop Trauma. 2013;27(1):43–8.
Lawrence SJ, Singhal M. Open hindfoot injuries. J Am Acad Orthop Surg. 2007;15(6):367–76.
Ramasamy A, Hill AM, Masouros S, Gibb I, Phillip R, Bull AM, et al. Outcomes of IED foot and ankle blast injuries. J Bone Joint Surg Am. 2013;95(5), e25.
Dickens JF, Kilcoyne KG, Kluk MW, Gordon WT, Shawen SB, Potter BK. Risk factors for infection and amputation following open, combat-related calcaneal fractures. J Bone Joint Surg Am. 2013;95(5), e24.
Harris AM, Althausen PL, Kellam J, Bosse MJ, Castillo R. Complications following limb-threatening lower extremity trauma. J Orthop Trauma. 2009;23(1):1–6.
Pollak AN, McCarthy ML, Burgess AR. Short-term wound complications after application of flaps for coverage of traumatic soft-tissue defects about the tibia. The Lower Extremity Assessment Project (LEAP) Study Group. J Bone Joint Surg Am. 2000;82-A(12):1681–91.
Quon DL, Dudek NL, Marks M, Boutet M, Varpio L. A qualitative study of factors influencing the decision to have an elective amputation. J Bone Joint Surg Am. 2011;93(22):2087–92.
Crichlow RJ, Andres PL, Morrison SM, Haley SM, Vrahas MS. Depression in orthopaedic trauma patients. Prevalence and severity. J Bone Joint Surg Am. 2006;88(9):1927–33.
Singh G, Harkema JM, Mayberry AJ, Chaudry IH. Severe depression of gut absorptive capacity in patients following trauma or sepsis. J Trauma. 1994;36(6):803–8; discussion 8–9.
McCarthy ML, MacKenzie EJ, Edwin D, Bosse MJ, Castillo RC, Starr A. Psychological distress associated with severe lower-limb injury. J Bone Joint Surg Am. 2003;85-A(9):1689–97.
Derogatis LR, Melisaratos N. The Brief Symptom Inventory: an introductory report. Psychol Med. 1983;13(3):595–605.
Derogatis LP. BSI: brief symptom inventory. 3rd ed. Minneapolis: National Computer Systems; 1993.
Castillo RC, MacKenzie EJ, Wegener ST, Bosse MJ. Prevalence of chronic pain seven years following limb threatening lower extremity trauma. Pain. 2006;124(3):321–9.
Wegener ST, Castillo RC, Haythornthwaite J, Mackenzie EJ, Bosse MJ, Group LS. Psychological distress mediates the effect of pain on function. Pain. 2011;152(6):1349–57.
Castillo RC, Wegener ST, Heins SE, Haythornthwaite JA, Mackenzie EJ, Bosse MJ, et al. Longitudinal relationships between anxiety, depression, and pain: results from a two-year cohort study of lower extremity trauma patients. Pain. 2013;154(12):2860–6.
Lusskin R, Battista A. Evaluation and therapy after injury to peripheral nerves. Foot Ankle. 1986;7(2):71–81.
Aldea PA, Shaw WW. Management of acute lower extremity nerve injuries. Foot Ankle. 1986;7(2):82–94.
Bateman JE. Trauma to nerves in limbs. Philadelphia: Saunders; 1962. p. 443.
Bosse MJ, McCarthy ML, Jones AL, Webb LX, Sims SH, Sanders RW, et al. The insensate foot following severe lower extremity trauma: an indication for amputation? J Bone Joint Surg Am. 2005;87(12):2601–8.
Beltran MJ, Burns TC, Eckel TT, Potter BK, Wenke JC, Hsu JR, et al. Fate of combat nerve injury. J Orthop Trauma. 2012;26(11):e198–203.
MacKenzie EJ, Rivara FP, Jurkovich GJ, Nathens AB, Egleston BL, Salkever DS, et al. The impact of trauma-center care on functional outcomes following major lower-limb trauma. J Bone Joint Surg Am. 2008;90(1):101–9.
Krettek C, Seekamp A, Kontopp H, Tscherne H. Hannover Fracture Scale '98 – re-evaluation and new perspectives of an established extremity salvage score. Injury. 2001;32(4):317–28.
Tscherne H, Oestern HJ. A new classification of soft-tissue damage in open and closed fractures (author’s transl). Unfallheilkunde. 1982;85(3):111–5.
Gustilo RB, Anderson JT. Prevention of infection in the treatment of one thousand and twenty-five open fractures of long bones: retrospective and prospective analyses. J Bone Joint Surg Am. 1976;58(4):453–8.
Gustilo RB, Mendoza RM, Williams DN. Problems in the management of type III (severe) open fractures: a new classification of type III open fractures. J Trauma. 1984;24(8):742–6.
Winquist RA, Hansen Jr ST, Clawson DK. Closed intramedullary nailing of femoral fractures. A report of five hundred and twenty cases. J Bone Joint Surg Am. 1984;66(4):529–39.
Johner R, Wruhs O. Classification of tibial shaft fractures and correlation with results after rigid internal fixation. Clin Orthop Relat Res. 1983;178:7–25.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2016 Springer-Verlag Berlin Heidelberg
About this chapter
Cite this chapter
Cross, W.W., Swiontkowski, M.F. (2016). Outcome and Management of Primary Amputations, Subtotal Amputation Injuries, and Severe Open Fractures with Nerve Injuries. In: Pape, HC., Sanders, R., Borrelli, Jr., J. (eds) The Poly-Traumatized Patient with Fractures. Springer, Berlin, Heidelberg. https://doi.org/10.1007/978-3-662-47212-5_22
Download citation
DOI: https://doi.org/10.1007/978-3-662-47212-5_22
Publisher Name: Springer, Berlin, Heidelberg
Print ISBN: 978-3-662-47211-8
Online ISBN: 978-3-662-47212-5
eBook Packages: MedicineMedicine (R0)