
Abstract
Lymphogranuloma venereum (LGV) has been renamed several times in the past and was known as tropical bubo, climatic bubo, poradenitis inguinalis, Durand-Nicolas-Favre disease, lymphopathia venereum and the fourth, fifth or sixth diseases. The causative agent of LGV is Chlamydia trachomatis genovar L. Worldwide, LGV is thought to account for 2–10 % of genito-ulcerative diseases in tropical climate areassuch as India and Africa. In Europe, North America and Australia, LGV is endemic mainly among HIV coinfected men who have sex with men. The first choice of treatment is an uninterrupted 21-day course of doxycycline 100 mg b.i.d.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
- Lymphogranuloma Venereum (LGV)
- Tropical Climate Areas
- Climatic Bubo
- Exanthema Subitum
- Rectal Chlamydial Infection
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
FormalPara Key Points-
Lymphogranuloma venereum (LGV) is a sexually transmitted infection (STI) caused by C. trachomatis genovar L (that primarily involves the lymphatics of the anogenital region).
-
Left untreated, LGV can lead to irreversible lymph oedema and fibrotic sequelae.
-
The disease is endemic in the tropical regions of Africa, Asia and South America.
-
In 2004, it was found endemic in the Western world among men who have sex with men (MSM) with high-risk sexual behaviour.
-
The standard algorithm to diagnose LGV is to first exclude C. trachomatis infection in suspected individuals via a commercially available routine nucleic acid amplification test (NAAT). In case this routine test is positive, genovar L has to be confirmed via an “in house” C. trachomatis genovar-specific C. trachomatis NAAT.
-
Apart from HIV and STI screening, HCV testing should be offered to all LGV patients.
-
The goal of therapy is to eradicate the pathogen.
-
Late sequelae do not respond to antibiotic treatment and need to be managed surgically.
-
Subjects who have had sexual contact with an LGV patient should be examined, tested for chlamydial infection and promptly treated.
-
To exclude reinfections, STI screening during a follow-up visit 3 months after an LGV diagnosis should be offered.
Definition and Epidemiology
Lymphogranuloma venereum (LGV) has been renamed several times in the past and was known as tropical bubo, climatic bubo, poradenitis inguinalis, Durand-Nicolas-Favre disease, lymphopathia venereum and the fourth, fifth or sixth diseases. However, the name LGV is currently the standard name and should be distinguished from granuloma inguinale, a bacterial STI caused by Klebsiella granulomatis.
The causative agent of LGV is Chlamydia trachomatis genovar L. Worldwide, LGV is thought to account for 2–10 % of genito-ulcerative diseases in tropical climate areas such as India and Africa. In Europe, North America and Australia, LGV is endemic mainly among HIV coinfected men who have sex with men (MSM, homo- and bisexual men) and is for the large part caused by genovar L2b. Heterosexual transmission of this MSM-associated L2b strain has been described.
The degree of infectiousness and the reservoir of disease have not been accurately defined, but heterosexual transmission has been attributed largely to asymptomatic female carriers, and in the MSM population, asymptomatic rectal infection and/or penile infection is the likely source of onward transmission.
Basic Concepts of Pathogenesis
Chlamydia trachomatis types L1, L2 and L3 are the causative pathogens. Additional variants have been described such as L2b, the strain currently found in MSM. Genovar L strains are invasive organisms that disseminate via underlying connective tissue and spread to regional lymph nodes. As a result, most LGV infections cause (systemic) symptoms in contrast to infections with C. trachomatis genovars A–K that remain confined to the mucosa and are asymptomatic in many cases. The incubation period of LGV is 1–4 weeks.
Clinical Presentation
Depending on the site of inoculation, LGV can cause inguinal disease (usually after inoculation of the genitalia) or the anorectal syndrome (usually after inoculation via the rectum). The disease course usually follows three separate stages (Table 57.1).
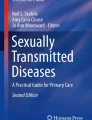
In the current LGV epidemic among MSM, proctitis is the primary manifestation of infection, usually presenting within a few weeks of sexual contact. It is characterised by severe symptoms of painful anorectal ulcers (Fig. 57.1) and bloody and/or purulent anal discharge. Tenesmus and constipation are also seen due to the mucosal and perirectal oedema. Anoscopic examination may reveal a granular or haemorrhagic proctitis with purulent exudate, mucosal ulceration and tumorous masses (Fig. 57.2). LGV proctitis is usually not accompanied by inguinal lymphadenopathy; but diagnostic imaging techniques may demonstrate pelvic node involvement. There is a debate about the proportion of asymptomatic LGV cases among MSM. In UK cohorts, almost all LGV infections appear to be symptomatic, in contrast to Dutch studies where a significant proportion of asymptomatic infections have been detected.


Anorectal lymphogranuloma venereum (LGV) with perianal ulceration


Anorectal lymphogranuloma venereum (LGV) with discharge, mucosal inflammation and oedema (same patient as in Fig. 57.1)
The primary lesions are small painless papules or pustules that may erode to form a herpetiform ulcer. They usually heal within 1 week and often go unnoticed. In the secondary stage 2–6 weeks after onset of primary lesion, painful inflamed inguinal and/or femoral lymph nodes, usually one sided, arise (Fig. 57.3). These “buboes” may become fluctuant and rupture in every third patient (Fig. 57.4). Inguinofemoral lymphadenopathy is mainly seen when the inoculation site is located on the external genitalia, which is the case in many male patients. In contrast, women more often have primary involvement of the rectum, upper vagina, cervix or posterior urethra; as these regions drain to the deep iliac or perirectal nodes, inguinofemoral lymphadenopathy is not seen. The resultant intra-abdominal or retroperitoneal lymphadenopathy may lead to symptoms of lower abdominal pain or low back pain. Constitutional symptoms, such as low-grade fever, chills, malaise, myalgias and arthralgias, may present during the second stage of disease. A rare presentation is the pharyngeal syndrome affecting the mouth and throat. Cervical lymphadenopathy and buboes can occur.


Inguinal lymphogranuloma venereum (LGV) with a bubo in the groin area


Late-stage inguinal lymphogranuloma venereum (LGV) with fistulae (From Dr. R. Hu, Dermatological Service, Paramaribo, Suriname)
The third stage of disease in LGV is often called the “anogenitorectal syndrome” and is more often present in women. Patients initially develop proctocolitis followed by perirectal abscess, fistulas, strictures and stenosis of the rectum, possibly leading to “lymphorrhoids” (haemorrhoid-like swellings of obstructed rectal lymphatic tissue). Without treatment, chronic progressive lymphangitis leads to chronic oedema and sclerosing fibrosis, resulting in strictures and fistulas of the involved region, which can ultimately lead to elephantiasis, esthiomene (the chronic ulcerative disease of the external female genitalia) and the frozen pelvis syndrome. If left untreated, LGV proctitis can lead to rectal strictures, with subsequent sequelae of soiling, pain, constipation and the possible development of megacolon.
Differential Diagnosis
LGV proctitis can mimic chronic inflammatory bowel diseases like Crohn’s disease, both clinically and in the pathological substrate. It is therefore often misdiagnosed by gastroenterologists confronted with MSM presenting with proctitis symptoms. The clinical and histologic picture of early LGV proctocolitis is similar to that seen in inflammatory bowel disease and LGV proctitis has been mistaken for Crohn’s disease. This has led to delay in the correct diagnosis and suboptimal treatment.
Since LGV is characterised by a diversity of presentations (depending on the inoculation site and the different stages of disease evolution), it is extremely difficult to establish a definitive diagnosis by clinical examination alone. As a result, it can be a challenge to differentiate LGV from other dermatological and sexually transmitted diseases (Table 57.2).
The clinician often misses the primary inoculation site. If present, it may simulate genital herpes, primary syphilis, chancroid or traumatic ulceration and bacterial, candidal or traumatic balanoposthitis. A mucopurulent urethritis noted in a few instances of LGV is often mistaken for non-specific urethritis or gonorrhoea.
The second stage of LGV manifests as regional lymphadenitis and perilymphangitis with bubo formation and is often confused with buboes caused by chancroid, syphilis, genital herpes, plague, tularaemia, tuberculous lymphadenitis, cat-scratch disease, septic lymphadenitis, Hodgkin’s disease, incarcerated inguinal hernia or psoas abscess.
In the tertiary stage, genital elephantiasis may mimic filariasis, tuberculosis, fungal or parasitic infection, granuloma inguinale (pseudo-elephantiasis) or transient vulvar elephantiasis with toxaemia of pregnancy. The rectal strictures of LGV may resemble those caused by trauma, actinomycosis, tuberculosis, schistosomiasis or adenocarcinoma of the rectum.
General Principles of Treatment
Systemic antibiotic therapy is the cornerstone in the treatment of LGV infection. Despite a paucity of robust evidence regarding the efficacy of therapy for any rectal chlamydial infections (LGV or non-LGV), 3 weeks of oral doxycycline 100 mg twice daily to treat LGV is recommended (Centers for Disease Control and Prevention (CDC) 2004; Clinical Effectiveness Group of the British Association for Sexual Health and HIV (CEG/BASHH) 2006; Workowski et al. 2010). Doxycycline is contraindicated in pregnancy and breastfeeding.
Early and prompt treatment is essential to prevent ongoing transmission, serious complications and mutilating sequelae. The low incidence of the disease, its complex presentation and the natural history marked by spontaneous remissions and exacerbations have precluded any rigorous evaluation of management. Nevertheless, sporadic trials in the treatment of LGV have shown successful use of tetracyclines (especially doxycycline) and erythromycin. Early and prompt antibiotic treatment shortens the duration of buboes, ulcers, sinuses and rectal discharges. Prolonged treatment (at least for 3 weeks) is the norm and more than one course of therapy or alternating some of the antibiotics may be necessary for chronic cases. The vast majority of recent MSM case reports have observed complete responses to 3-week doxycycline therapy; shorter courses may not eradicate the organism. It has been shown that L biovar C. trachomatis RNA can persist for up to 16 days in LGV proctitis patients treated with doxycycline.
The following antibiotic chemotherapy recommendations have been made for uncomplicated LGV infections:
-
Doxycycline, 100 mg orally b.i.d. × 21 days, or erythromycin, 500 mg orally q.i.d. × 21 days, or azithromycin, 1 g orally once weekly × 21 days (Workowski et al. 2010).
-
Doxycycline, 100 mg orally b.i.d. × 14 days, or erythromycin, 500 mg orally, q.i.d. × 14 days, or tetracycline, 500 mg orally, q.i.d. × 14 days, or sulphadiazine, 1 g orally q.i.d. × 14 days (WHO 2003).
-
For pregnant and lactating women or children below 8 years, erythromycin stearate is prescribed (Banor et al. 1953). In children, the dose is 7.5–12.5 mg/kg/dose q.i.d. for 14 days.
Other mentioned antibiotic modalities which have been successfully used in treating acute bubonic LGV and LGV proctocolitis are minocycline, 300 mg orally initially, followed by 200 mg b.i.d. for 10 days. Azithromycin regimens have been suggested but the dosage and duration of therapy are not known.
Surgical Treatment
Fluctuant buboes are aspirated through the surrounding unaffected skin with a wide-bore needle and not incised. Perianal and perirectal abscesses must be surgically drained. Rectal strictures are dilated either manually or with elastic bougies at weekly intervals. When the stricture is impassable, a preparatory ileocolostomy followed by proctocolectomy is a justifiable procedure. Chronic intractable ulcerative lesions of the rectum may be treated by suitable single-stage surgical procedures, such as full skin cover by direct flaps, myocutaneous flaps or sliding flaps (floating island). A urethral stricture can be dilated with Lister’s or Clutton’s bougies.
The chronic manifestations of tertiary LGV such as rectovaginal fistulae, genital elephantiasis, vulvar growths, esthiomene or rectal strictures and stenosis do not respond to antibiotic therapy and require surgical intervention and plastic reconstruction. Polypoid excrescences of the vulva, pedunculated tumours or elephantiasic vulvae require local excision and partial or total vulvectomy.
Management of Patients with Proctitis
It is recommended to screen all MSM who report receptive anal sexual practices in the previous 6 months for anorectal C. trachomatis infection with a commercially available nucleic acid amplification test (NAAT). Subsequently, MSM with anorectal C. trachomatis infection are then screened for LGV proctitis using a genovar L-specific “in house” developed NAAT. In the recent MSM LGV epidemic, incident cases of both HIV and hepatitis C have been observed, and serological testing should be offered for both infections after appropriate window periods have elapsed according to relevant local guidelines. The prevalence of HIV among LGV cases ranges from 67 to 100 % in 13 descriptive studies (Rönn and Ward 2011). Tests for STI, including HIV (if not already known HIV positive), hepatitis B and hepatitis C should be offered before starting therapy.
Given the high incidence of STIs in MSM with proctitis complaints, the CDC recommends presumptive therapy in MSM with a high index of suspicion (Workowski et al. 2010) rather than waiting for positive cultures that can take more than a week to return (Box 57.1). Delay in treatment can lead to potential complications and “lost to follow-up” infections.
Box 57.1. Proctitis Syndromic Treatment Guidelines for High-Risk Individuals with Anal Complaints (Adapted from de Vries et al. 2013)
Syndromic treatment of a symptomatic proctitis or confirmed non-LGV C. trachomatis proctitis:
-
Doxycycline 100 mg p.o., 2d.d. 7 days
Syndromic treatment of a suspected N. gonorrhoea proctitis (e.g. based on Gram-negative intracellular diplococci) or confirmed N. gonorrhoea proctitis:
-
Ceftriaxone 500 mg i.m. single dose
PLUS
-
Doxycycline 100 mg p.o., 2d.d. for 7 days
Syndromic treatment of LGV proctitis or confirmed LGV proctitis:
-
Doxycycline 100 mg p.o., 2d.d. for 21 days
OR
-
Erythromycin 500 mg p.o., 4d.d. for 21 days
Follow-Up
Patients are followed up clinically until signs and symptoms resolve. This may occur within 3–6 weeks. All patients diagnosed with LGV should be followed up at the end of treatment, to ensure resolution of symptoms and signs of infection, to check that adequate partner notification has been completed, to address any patient concerns and to arrange suitable follow-up testing for syphilis and blood-borne viruses including hepatitis B and C and HIV.
Doxycycline failure in LGV has been reported in 3 out of 75 treated patients (Rodríguez-Domínguez et al. 2014). If the recommended 21-day course of doxycycline is completed, a test of cure for LGV seems indicated only in those with persistent complaints. It should be noted that doxycycline can also cause gastrointestinal symptoms like mucous discharge and diarrhoea. A routine microbiological test of cure is usually not done.
Partner Management
It is essential that sex partner notification be initiated when the diagnosis is made. Partners who have had sexual contact with an LGV patient, should be promptly treated for LGV according to the above-mentioned therapy advice. STI testing should be offered to all sexual contacts within the last 3 months (or in case of symptomatic patients within 30 days before the onset of the patient’s symptoms). Moreover, empiric antibiotic therapy should be recommended to partners, until STI has been excluded in the partner.
Prevention
Patients diagnosed with LGV should be counselled regarding prevention of other STIs including HIV and hepatitis C. Moreover, regular sexual health screening including HIV testing should be offered, condom use should be demonstrated and promoted, hepatitis A and B vaccination for MSM offered, and patients at risk of HIV infection should be advised of the availability of post-exposure prophylaxis for HIV. In particular, HIV-positive MSM should be made aware of recent trends in hepatitis C epidemiology and warned of the risks of unprotected anal sex, serosorting, recreational drug use and mucosally traumatic sexual practices such as fisting. Enema use prior to receptive anal sex should be discouraged since it is associated with rectal chlamydial infections and especially LGV proctitis. Although sharing of equipment was rare, it is prudent to advise against sharing any such equipment and to wash equipment thoroughly after use.
Sexual contacts must be traced and promptly treated. Patients on antibiotic therapy should be monitored for recurring symptoms over a period of 6 months following antibiotic treatment. Doctors and other health care workers must observe proper safeguards such as wearing gloves when touching infected sites or handling soiled dressings or other contaminated items. Health-seeking behaviour and health education of those at risk should be encouraged.
Future Perspectives
In the ongoing LGV epidemic, there is a need for better and cheaper screening tools to detect cases in larger groups of individuals at risk. This is of importance to prevent complications in the individual patient and to halt transmission in the community. Physicians should consider LGV in case MSM present with inguinal lymphadenopathy, genital ulceration or proctitis complaints. If chronic inflammatory bowel syndromes like Crohn’s disease are considered, especially in MSM, LGV proctitis should always be excluded. Shorter antibiotic courses than the present ones of 21 days are needed to increase patient compliance to the treatment but require large controlled clinical trials. Lastly, a deeper understanding of the microbial and immunological background of LGV infection in relation to HIV could shed light on the considerable number of asymptomatic LGV cases found.
Abbreviations
- B.i.d.:
-
Bis in die/two times a day
- C:
-
Chlamydia
- LGV:
-
Lymphogranuloma venereum
- MSM:
-
Men who have sex with men
- NAAT:
-
Nucleic acid amplification test
- Q.i.d.:
-
Quater in die/four times a day
- STI:
-
Sexually transmitted infection
References
Banor Jr L, et al. Erythromycin treatment of lymphogranuloma venereum. In: Welch H et al., editors. Antibiotics annual 1953-54. New York: Medical Encyclopedia; 1953. p. 475–9.
Centers for Disease Control and Prevention (CDC). Lymphogranuloma venereum among men who have sex with me--etherlands, 2003–2004. MMWR Morb Mortal Wkly Rep. 2004;53(42):985–8.
Clinical Effectiveness Group of the British Association for Sexual Health and HIV (CEG/BASHH). 2006 National guideline for the management of lymphogranuloma venereum (LGV) of the British Association of Sexual Health and HIV (BASHH). 2006. http://www.bashh.org/documents/92/92.pdf.
de Vries HJ, Reddy BS, Khandpur S. Chapter 41. Lymphogranuloma venereum. In: Gupta S, Kumar B, editors. Sexually transmitted infections. 2nd ed. New Delhi: Elsevier; 2012. p. 506–21.
de Vries HJ, Zingoni A, White JA, Ross JD, Kreuter A. 2013 European Guideline on the management of proctitis, proctocolitis and enteritis caused by sexually transmissible pathogens. Int J STD AIDS. 2013;18;25(7):465–474.
Guidelines for the management of sexually transmitted infections, WHO 2003. Downloadable from: http://apps.who.int/iris/bitstream/10665/42782/1/9241546263_eng.pdf. Accessed 26 June 2013.
Rodríguez-Domínguez M, Puerta T, Menéndez B, González-Alba JM, Rodríguez C, Hellín T, Vera M, González-Sainz FJ, Clavo P, Villa M, Cantón R, Del Romero J, Galán JC. Clinical and epidemiological characterization of a lymphogranuloma venereum outbreak in Madrid, Spain: co-circulation of two variants. Clin Microbiol Infect. 2014;20(3):219–25.
Rönn MM, Ward H. The association between lymphogranuloma venereum and HIV among men who have sex with men: systematic review and meta-analysis. BMC Infect Dis. 2011;11:70.
Workowski KA, Berman S, Centers for Disease Control and Prevention (CDC). Sexually transmitted diseases treatment guidelines, 2010. MMWR Recomm Rep. 2010;59(RR-12):1–110.
Further Reading
Davis TW, Goldstone SE. Sexually transmitted infections as a cause of proctitis in men who have sex with men. Dis Colon Rectum. 2009;52:507–12.
de Vries HJ, Van der Bij AK, Fennema JS, et al. Lymphogranuloma venereum proctitis in men who have sex with men is associated with anal enema use and high-risk behavior. Sex Transm Dis. 2008;35(2):203–8.
de Vries HJ, Smelov V, Middelburg JG, Pleijster J, Speksnijder AG, Morré SA. Delayed microbial cure of lymphogranuloma venereum proctitis with doxycycline treatment. Clin Infect Dis. 2009;48(5):e53–6.
de Vries HJ. Sexually transmitted infections in men who have sex with men. Clin Dermatol. 2014;32(2):181–8.
de Vries HJ, Zingoni A, Kreuter A, Moi H, White JA. 2013 European guideline on the management of lymphogranuloma venereum. J Eur Acad Dermatol Venereol. 2014 doi: 10.1111/jdv.12461. [Epub ahead of print].
de Vrieze NH, de Vries HJ. Lymphogranuloma venereum among men who have sex with men. An epidemiological and clinical review. Expert Rev Anti Infect Ther. 2014 Jun;12(6):697–704.
de Vrieze NH, van Rooijen M, Speksnijder AG, de Vries HJ. Urethral lymphogranuloma venereum infections in men with anorectal lymphogranuloma venereum and their partners: the missing link in the current epidemic? Sex Transm Dis. 2013;40(8):607–8.
Hathorn E, et al. What is the appropriate treatment for the management of rectal Chlamydia trachomatis in men and women? Sex Transm Infect. 2012;88:352–4.
Hill SC, Hodson L, Smith A. An audit on the management of lymphogranuloma venereum in a sexual health clinic in London, UK. Int J STD AIDS. 2010;21(11):772–6.
Korhonen S, Hiltunen-Back E, Puolakkainen M. Genotyping of Chlamydia trachomatis in rectal and pharyngeal specimens: identification of LGV genotypes in Finland. Sex Transm Infect. 2012;88(6):465–9.
Luk NM. Lymphogranuloma venereum. In: Kuen-kong LO, et al., editors. Social hygiene handbook, handbook of dermatology and venereology. Lisbon Social Hygiene Service, Department of Health; 1996. p. 1–14.
Martin DH, et al. A controlled trial of single dose of azithromycin for the treatment of chlamydial urethritis and cervicitis. The Azithromycin for Chlamydial infections study group. N Engl J Med. 1992;327:921–95.
McLean CA, Stoner BP, Workowski KA. Treatment of lymphogranuloma venereum. Clin Infect Dis. 2007;44 Suppl 3:S147–52.
Najafi JA, et al. Surgical aspects of inguinal lymphogranuloma venereum. Mil Med. 1979;144:697–9.
Peuchant O, Baldit C, Le Roy C, Trombert-Paolantoni S, Clerc M, Bébéar C, de Barbeyrac B. First case of Chlamydia trachomatis L2b proctitis in a woman. Clin Microbiol Infect. 2011;17(12):E21–3.
Pinsk I, Saloojee N, Friedlich M. Lymphogranuloma venereum as a cause of rectal stricture. Can J Surg. 2007;50(6):E31–2.
Prakash S, et al. Problematic ulcerative lesions in sexually transmitted diseases: surgical management. Sex Transm Dis. 1986;13:127–30.
Soni S, Srirajaskanthan R, Lucas SB, Alexander S, Wong T, White JA. Lymphogranuloma venereum proctitis masquerading as inflammatory bowel disease in 12 homosexual men. Aliment Pharmacol Ther. 2010;32(1):59–65.
Sowmini CN, et al. Minocycline in the treatment of lymphogranuloma venereum. J Am Vener Dis Assoc. 1976;2:19–22.
Spaargaren J, Fennema HS, Morré SA, de Vries HJ, Coutinho RA. New lymphogranuloma venereum Chlamydia trachomatis variant, Amsterdam. Emerg Infect Dis. 2005;11(7):1090–2.
Vall-Mayans M, Caballero E, Sanz B. The emergence of lymphogranuloma venereum in Europe. Lancet. 2009;374(9686):356.
van der Bij AK, Spaargaren J, Morre SA, Fennema HS, Mindel A, Coutinho RA, de Vries HJ. Diagnostic and clinical implications of anorectal lymphogranuloma venereum in men who have sex with men: a retrospective case-control study. Clin Infect Dis. 2006;42:186–94.
van der Ham R, de Vries HJ. Lymphogranuloma venereum, where do we stand? Clinical recommendations. Drugs Today (Barc). 2009;45 Suppl B:39–43.
Verweij SP, Ouburg S, de Vries H, Morré SA, van Ginkel CJ, Bos H, Sebens FW. The first case record of a female patient with bubonic lymphogranuloma venereum (LGV), serovariant L2b. Sex Transm Infect. 2012;88(5):346–7.
Ward H, Martin I, Macdonald N, Alexander S, Simms I, Fenton K, French P, Dean G, Ison C. Lymphogranuloma venereum in the United Kingdom. Clin Infect Dis. 2007;44:26–32.
Wright LT, et al. The treatment of lymphogranuloma venereum with terramycin. Antibiot Chemother. 1951;1:193–7.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2015 Springer-Verlag Berlin Heidelberg
About this chapter
Cite this chapter
de Vries, H.J.C. (2015). Lymphogranuloma Venereum. In: Katsambas, A.D., Lotti, T.M., Dessinioti, C., D’Erme, A.M. (eds) European Handbook of Dermatological Treatments. Springer, Berlin, Heidelberg. https://doi.org/10.1007/978-3-662-45139-7_57
Download citation
DOI: https://doi.org/10.1007/978-3-662-45139-7_57
Publisher Name: Springer, Berlin, Heidelberg
Print ISBN: 978-3-662-45138-0
Online ISBN: 978-3-662-45139-7
eBook Packages: MedicineMedicine (R0)