
Abstract
Mycological examination is the diagnostic procedure necessary to confirm a fungal disease, from the Greek word “mykes” meaning mushroom. The mycological test is also necessary to document the complete cure response to treatment, as clinical recovery is often followed by a relapse if the fungus has not been completely eliminated from the skin (mycological cure). The diagnosis of a fungal infection is considered simple from a clinical point of view, but the report of unusual presentations, misdiagnosed or sometimes neglected, has increased worldwide causing extensive and long-standing disease. General immunosuppressive treatment for inflammatory chronic diseases and acquired immune depression syndrome are frequently complicated with fungal superinfections, both from common strain and rare or opportunistic fungal species, such as cryptococcosis, histoplasmosis, sporotrichosis, blastomycosis, and aspergillosis. In the immunocompetent patient, dermatophytes are the main fungal infection, being the primary pathogen. Clinical presentation has also changed with time, from the classic ringworm appearance (tinea) to more veiled eczematous undefined patches, simulating more frequent diseases, such as atopic or contact eczema, seborrheic dermatitis, impetigo, rosacea, and lupus erythematosus. A general common attitude to prescribe combination treatments and/or corticosteroid topics before confirming the diagnosis (“ex adjuvantibus”) is one of the possible causes of further dermatophyte pathomorphosis and misdiagnosis, named tinea incognita or tinea atypica.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
FormalPara Key Points-
Mycoses are diseases caused by fungi, present in the soil, air, contaminated food, animals, and humans. Fungi are classified according to the microscopy appearance and by the method of reproduction in culture. Therefore, laboratory testing is necessary to confirm the diagnosis in all conditions.
-
Superficial localized infection can be diagnosed rapidly by taking fresh unstained material (skin, nails, hairs) to be examined by direct microscopy after potassium hydroxide (KOH) clarification. This procedure is usually rapid and easy to handle even in general practice, if provided with a light microscopy.
-
Fungal culture is necessary to identify the fungus and to confirm the vitality of the strain. When a local or systemic antifungal treatment is performed, culture is necessary to assess effective recovery or current infection. It requires specific training and great expertise, reserved to specialized mycology laboratories.
-
False-negative results are possible; therefore, biopsy and histology are indicated if direct microscopy and culture are negative and clinical suspicion is high.
-
Wood’s lamp examination has very limited indication, detecting the natural luminescence of only few pathogens, mainly Microsporum spp., Malassezia furfur, and Corynebacterium minutissimum.
-
Molecular techniques, such as DNA hybridization and PCR, are useful to prompt diagnosis, detecting even small amounts of fungi, but are expensive procedures, limited to the research or reference laboratories for the diagnosis of rare fungal infections, which are difficult or dangerous to cultivate in vitro.
-
Great simplification of the fungal identification process is expected from the introduction of the assay mass spectrometry in routine laboratory.
General Principles
Mycological examination is the diagnostic procedure necessary to confirm a fungal disease, from the Greek word “mykes” meaning mushroom. The mycological test is also necessary to document the complete cure response to treatment, as clinical recovery is often followed by a relapse if the fungus has not been completely eliminated from the skin (mycological cure). The diagnosis of a fungal infection is considered simple from a clinical point of view, but the report of unusual presentations, misdiagnosed or sometimes neglected, has increased worldwide causing extensive and long-standing disease. General immunosuppressive treatment for inflammatory chronic diseases and acquired immune depression syndrome are frequently complicated with fungal superinfections, both from common strain and rare or opportunistic fungal species, such as cryptococcosis, histoplasmosis, sporotrichosis, blastomycosis, and aspergillosis. In the immunocompetent patient, dermatophytes are the main fungal infection, being the primary pathogen. Clinical presentation has also changed with time, from the classic ringworm appearance (tinea) to more veiled eczematous undefined patches, simulating more frequent diseases, such as atopic or contact eczema, seborrheic dermatitis, impetigo, rosacea, and lupus erythematosus. A general common attitude to prescribe combination treatments and/or corticosteroid topics before confirming the diagnosis (“ex adjuvantibus”) is one of the possible causes of further dermatophyte pathomorphosis and misdiagnosis, named tinea incognita or tinea atypica.
The etiology of a fungal infection is rapidly proved with laboratory testing and possible in a general office if provided with very basic light microscopy. Besides, few dermatologists and laboratory physicians are trained to recognize dermatophytes. Final identification of the species requires culture facilities and further expertise, which should be referred to a mycology laboratory.
False-negative results are possible, especially if the specimen is not correctly taken, and more invasive assessment should be performed before ruling out the diagnosis of a fungal disease. Biopsy specimens for histopathology examination with PAS or silver staining are indicated when clinical suspicion is high. Sensitivity of culture alone is about 32 %, while histology reaches 85 %, especially in onychomycosis.
A specific fluorescent dye named calcofluor-white might be used, because it binds selectively to the fungal cell wall chitin (apple green fluorescence), but a fluoroscope is necessary.
A molecular approach has been proposed, but the tool is expensive; a plethora of different methods has been proposed without conclusive validation and therefore has never gained much popularity. Direct staining with monoclonal antibody labeled with fluorescent dyes has been proposed to detect rare and small amounts of fungi in the clinical specimens, mainly Pneumocystis carinii in bronchoalveolar lavage.
The perspective in clinical mycology laboratories is the fast fungal identification by assay mass spectrometry (matrix-assisted laser desorption ionization time-of-flight (MALDI-TOF) mass spectrometer (MS)) from clinical cultures. Spectral databases (biotype library) of different fungal species have been realized by several independent researchers, and preliminary results confirm the usefulness of the tool, with a sensitivity of 91.9 % on skin isolates, which is hoped to become routine in the immediate future.
Biology and Morphology of the Fungi
Fungal microscopy identification requires an extensive knowledge of fungi biology as a whole, whose principles are magisterially described in the reference book by Grigoriu et al. (1987) and are somewhat synthesized as follows.
Fungi are classified with the lower plants (category, cryptogams; phylum, thallophytes), although devoid of chlorophyll and incapable of photosynthesis, and they are:
-
Heterotrophic, meaning they subside on organic substances for survival and are unable to directly elaborate mineral elements, such as green plants. They are provided with several enzyme systems able to digest organic substances (keratin) and to de novo synthesize toxins and antibiotics.
-
Aerobic, developing at different temperatures varying from one species to another, but usually ranging between 20 and 37 °C, preferring neutral pH and several degrees of humidity, while dryness is poorly tolerated. Direct light exposure has different effects among species, fostering or inhibiting growth.
-
Eukaryotes, with well-differentiated cytoplasm and nuclei. They consist of a thallus or aerius mycelium, which is a matted network of branching tubes called hyphae, filled with the living substance, continuously expanding with growing tips. The thallus accomplishes both vegetative and reproductive functions: from the central starting point of the colony, the hyphae develop centrifugally in all directions obtaining nourishment from the environment, with the young elements at the periphery and aging dead elements at the center. When the vegetative expanding apparatus has accumulated sufficient nourishment and the environment is favorable, the reproductive phase might take place, which can be either sexual (perfect fungi) or asexual. A limited number of fungal species do not have a documented sexual way of reproduction and for this reason are called imperfect fungi.
A number of classifications have been proposed on the basis of the thallus’ different characteristic and sexual reproduction ways, to consent a precise nomenclature and identification, whose simplest ones are illustrated in Table 123.1.
-
On the basis of thallium morphology, it is possible to distinguish among septate and not septate fungi. A single cell generates a type of thallus with intercommunicating filaments (hyphae), named coenocytic filaments, without subdivision and therefore called aseptate hyphae. Other thalli are made of septated hyphae, which indicate the presence of regular periodical septal division in the filaments, provided with central pores allowing the passage of nutrients from one segment to the other. Another type of thallus consists of isolated cells, solely and elongated or attached one to the other, forming fragile, eventually branching chains but without intercommunication, therefore called pseudomycelium.
-
The principal way of fungal reproduction in pathologic material is asexual, producing a variety of spores (Table 123.2) responsible for fungal dissemination in the environment. The aspect of pathogenic fungi might differ from the parasitic state to the culture optimal saprophytic state. In fact, mycelia fungi do not usually deserve fruiting bodies in the pathologic materials, and species identification is possible only in culture specimens. Yeasts might bud in vivo, while the so-called dimorphic fungi are typically found as yeast cells in pathologic material, producing mycelia filaments in cultures.
Table 123.2 Distinctive morphological characteristics of fungal spores
Basic Concepts Related to the Pathogens
From a practical medical point of view, the pathogenic fungi for humans are:
-
Dermatophytes (whose mycological diagnosis is extensively treated in this chapter)
-
Yeasts and yeastlike fungi (whose laboratory diagnosis requires specialized equipment and expertise, and only basic concepts are expressed in this chapter)
-
Some dimorphic and opportunistic fungi, becoming pathogen under peculiar circumstances (whose diagnosis is not developed in this chapter)
Dermatophyte Infections
Dermatophytes are actually classified among the ascomycetes and represent a closely related group of fungi, whose main pathogens for humans are the Trichophyton, Microsporum, and Epidermophyton genera. They are ubiquitous and are characterized by the ability to use keratin as a nutrient source, therefore evolving a dependency on humans and/or animals for the survival and dissemination of their species. They are noninvasive, as they colonize the keratinized stratum corneum, which is a nonliving tissue. However, the presence of the fungus and its metabolic products usually induces an inflammatory eczematous response in the host, counteracting the parasitism. More severe reactions might be related to the species and strain of dermatophyte causing the infection, but also from host predisposing condition, such as skin barrier alterations or previous skin diseases.
-
The superficial dermatophyte infections affect the outer layers of the skin, the nails, and hairs. Growing fungi produce typically branched and compartmented septate filaments (hyphae) and arthrospores, which break off from the hyphae at the septate level and represent the main ways of propagation and species conservation. Each segment forms a physiological unit.
-
In culture, the characteristic morphology of the reproductive spores (micro- and macroconidia) and accessory features consent species identification.
Guidelines for Proper Specimen Collection in Dermatophyte Infections
Specimen collection is a delicate moment and is the first cause of false-negative results. It should be adapted to the site affected and type of material, including skin scrapings, broken hairs, nail clippings, corneal scraping, and body fluids such blood, CSF, urine, sputum, as well as discharge or pus from lesions.
All specimens must be transported to the laboratory without delay to prevent bacterial overgrowth. Some laboratories suggest refrigeration if a long delay is expected, especially for body fluids and discharged materials, but it is recommended only for a short period.
Skin scales scrapings are best taken from the leading edge of the rash, after the skin has been cleaned with soaks of 0.9 % saline solution to remove cream residuals. Disinfection with alcohol or ether is often advocated but is not necessary and might remove the upper scales which are the most infested. Gently remove the surface skin using a blade or curette and place the material in a sterile container or a black paper envelope (Fig. 123.1).


Correct execution of the scales sample from the active borders of an erythematous scaling round-shaped lesion (top-left inset); correct execution of the hair sample from discolored and few millimeter broken-off hairs plucked with a pair of eyebrow tweezers (top-right inset). The native preparation is put on a smear and a drop of a clearing solution is added (down-left inset); staining with blue or black ink preparations might be useful to highlight hyphae and arthrospores or yeasts presence (downright inset)
Hairs should be gently pulled out with a pair of tweezers, choosing those broken off at the surface (black dots) or few millimeters from the follicle, discolored and lusterless, surrounded by a whitish sheath, or covered by scales (Fig. 123.1). Parasitized hairs are removed easily and painless. A toothbrush can be used to collect scales from the infected scalp.
Nail clippings are usually taken from the ventral surface scaly deposits, using a blunt curette or a blade. If the nail plate is widely detached and full of debris, the distal end should be cut with a pair of scissors and discarded to find the fresh infected nail. Depending on the site of involvement, the lateral and/or proximal surface of the nail plate should also be scraped (Fig. 123.2).


Correct site of sampling depending on the clinical form of onychomycosis
Examination by Direct Microscopy
The most common and first step laboratory examination is to examine fresh unstained materials (native preparation), such as scales, hairs, and nails. Part of the material is placed on a clean slide and eventually split to very fine dust with the aid of a blade. Body fluids, content of vesicles, and pustules can be also directly placed on the smear. Keratinized material and cell walls are opaque at microscopy, and some chemical solutions (Table 123.3) must be added to dissolve keratinocytes and make the material transparent, a process that is called “clearing.” Certain laboratories add glycerin to delay the preparation drying out and have more time to perform the slide lecture. One or two drops of the clearing agent is put on the collected material on the slide and then covered with a cover slip (Fig. 123.1). The most used clearing solution is potassium hydroxide (KOH) in 10–40 % concentrations. It is very cheap and stable on light and does not need particular conservation or caution, and the preparation is rapidly ready. Time to clearing depends on the material type and thickness, the hairs being rapidly destroyed by KOH and therefore examined in 20 min, 1 h at most; the skin scales usually are examined within 3 h, while the nails are more resistant, sometimes requiring 24 h and addition of new clearing solution or physiologic solution, because one of the major disadvantages with KOH is precipitation and formation of crystals. Additional staining with methylene blue, Parker blue, or black ink do not replace direct examination (Fig. 123.1), but it is sometimes useful to highlight the chitin in the fungal cell walls. Fixation and staining with lactophenol cotton blue (LPCB) is preferred to observe yeasts, fungal accessories, and fruiting structures, especially from culture specimen.
The microscopic examination is first performed under a low-power lens (100×) run carefully along the slide to find fields of interests (Fig. 123.3). Once the fungus is detected, the high-power lens (200 or 400x) observation allows for true hyphae confirmation and distinction from pseudohyphae, as well as arthrospores selection from yeasts.


Skin scraping: under low-power light microscopy, selection of a field of interest (top-left inset; 100×); major definition of hyphae and arthrospores characteristics at higher power observation (top-right inset; 400×). Parasitized hairs: sheath of arthrospores surrounding the hair shaft in an ectothrix arrangement and hyphae presence in the scales (bottom-left inset; 100×); hyphae and arthrospores inside the hair root and shaft in endothrix parasitism (bottom-right inset; 400×)
Fungal elements are sometimes difficult to find, and a negative result does not rule out fungal infection. Microscopy should be repeated, possibly with fresh material or giving more time to clearing and repeating the observation with great perseverance.
Direct Microscopic Examination Pitfalls
Specific training is necessary to avoid the many possible sources of errors in mycology, as in any other laboratory procedure.
-
Mistakes in sample collection: insufficient material, inadequate site of sampling, and contamination.
-
Insufficient clearing and hasty observation yield most false-negative results.
-
Artifacts (Fig. 123.4): the mycelia filaments and arthrospores have to be distinguished from:
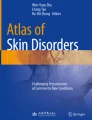
Fig. 123.4 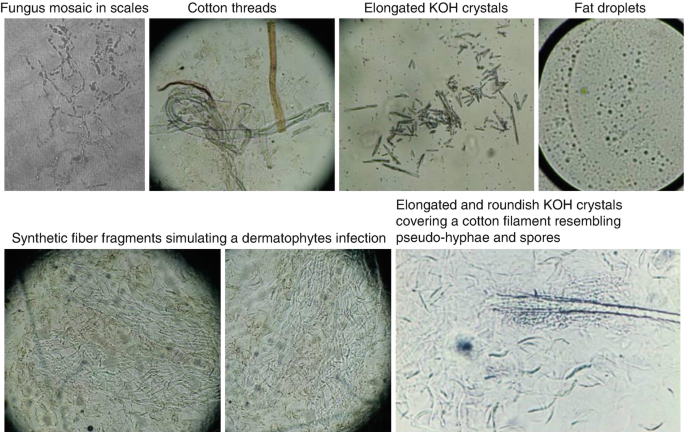
Microscopic examination artifacts
-
Fungus mosaics: a network made of refractive small filaments or crystals, irregular in shape and diameter, whose chain arrangement is very similar to the mycelia and might mislead a nonexpert investigator. They are cell debris containing cholesterol crystals due to a reaction of the intercellular substance with potassium hydroxide. Usually the mosaics are located at the limits of the cells and disappear if a drop of glycerol or physiologic solution is added to the preparation. The higher-power observation (100×) enables the distinction from the fungal hyphae, which are regular in caliber and shape, septated, connected together continuously.
-
Cotton threads, other vegetal filaments and fur brittles, which are usually woven or twisted on their axis and irregular in caliber, tufted at the extremities.
-
Polyhedral or elongated crystals: refractive bodies differing in appearance one from the other and not connected together. It is the dehydrated clearing agent that usually causes this artifact, and a drop of distilled water added directly to the smear makes them to disappear.
-
Fat droplets, refractive roundish or oval bodies, enclosed by a double membrane frequently due to the previous use of cosmetic creams, persisting on the skin although disinfected. Cleaning with water and soap before examination is advisable.
-
-
Filamentous bacteria: some Actinomycetales bacteria and particularly the Streptomyces genus are able to produce a network of branching filaments very similar to the fungal mycelia, but smaller in dimensions (0.5–0.8 μm).


Yeast Infections
Yeasts and yeastlike are a subtype of fungal species characterized by clusters of round or oval cells. They divide and propagate budding out similar cells from their surface. Some yeasts are capable of producing filaments, which remain part of the single original cell, not connected with other elements and called pseudohyphae. They are usually saprophytic, but a pathogenic potential might arise in the presence of several favoring conditions. The main yeasts causing human superficial skin infections, whose diagnosis might be confirmed in a general laboratory provided with a light microscopy, are:
-
Candida species and Torulopsis glabrata
-
Malassezia species
Specimen Collection and Examination by Direct Microscopy
Basic concepts and procedures are similar to dermatophyte mycological examination, and only useful additional information for the general practice is addressed in the following paragraphs.
Candida spp. infection can be confirmed by swabs and by scrapings. The pathologic material (scales, pustules, white deposits, and secretions) is cleared with KOH between the slide and the cover slip. Urine can be examined without clarification, and blood is seeded directly on the medium for culture. Under the microscope, the presence of pseudohyphae and round, oval yeasts forms might be sufficient to confirm the type of infection (Fig. 123.5), but when dealing with opportunistic infections, culture execution is recommended to confirm pathogenicity instead of simple colonization. Detection of yeasts should be interpreted in close cooperation with clinicians, and equivocal or unusual findings should be verified by repeated laboratory tests. Superinfection of skin lesions in the course of several diseases is very frequent, and Candida detection is not sufficient to ascribe its etiologic role. Histology is sometimes necessary to distinguish primary infection from superinfection.


Candida yeast cells and pseudohyphae in a groin intertrigo (400×)
Malassezia spp. infection is better documented by stripping off the skin surface with an adhesive tape (scotch test), as the scales are very subtle and superficial. The scotch is then stuck on a glass slide and examined using potassium hydroxide (KOH), eventually stained with blue or black ink preparation. The abundant presence of the fungal filamentous form budding from the yeast cells in a pattern called “spaghetti with meatballs” is very peculiar and diagnostic (Fig. 123.6).


Skin scotch test after KOH + Parker’s blue clarification positive for Malassezia furfur pseudohyphae and clusters of yeastlike cells (400×)
Fungal Culture
General Principles of the Correct Procedure and Fungal Identification
Culture is necessary to correctly identify most of the fungal species but requires great expertise, and only very specialized laboratories are reliable.
Specimen collection is similar to the previously described technique for direct examination, but sterile materials should be used, because the transferring process of the pathologic samples (scales, hairs, nails) is a delicate moment, at high risk of contamination. Every subsequent passage should be performed under sterile conditions. The specimen must be placed on a sterile plate, subdivided into small particles with the aid of a sterile dissecting needle or a razor blade and collected with a previously flamed platinum loop to be seeded on the culture medium (Fig. 123.7). A distance of about 1 cm should be maintained between each inoculum on the medium surface. The test tubes or Petri dishes must be taken from fridge cool to room temperature, and the mouth of the tube or the dish plate must be flamed with a Bunsen burner to sterilize it.


Culture technique: transferring process of the pathologic material on different medium containers
The most commonly used culture medium is Sabouraud’s dextrose agar added with cycloheximide and chloramphenicol to avoid mold contamination. Time to colony growth on Sabouraud’s agar is a first discrimination of the type of fungus: filamentous fungi grow very slowly, along several weeks (3 weeks or more), incubated at 25–30 °C. Yeasts produce fast growing colonies (24–48 h). A number of other organic and synthetic culture media have been proposed (Table 123.4), whose laboratory preparation has been simplified by the use of prompt dehydrated media, which only need the addition of a fixed amount of distilled water, sterilization, and portioning on test tubes or Petri dishes.
A selective dermatophytes medium (DTM) is available for practitioner’s use in the office, which does not require special conservation or care. Dermatophyte growth is indicated from the medium’s color change to orange. Unfortunately, this kind of test is expensive and does not allow for subsequent fungal identification.
Once the colonies have grown, identification relies on both gross and microscopic features. Colony morphology and growth dynamics may vary considerably with the culture medium used (type of glucose, peptone, pH) and other conditions such as the degree of humidity and temperature. It is therefore essential to maintain constant conditions in the laboratory and to use the same components for the media preparation. Well-established and reference features are based on Sabouraud’s medium, and it is advisable to always perform at least one culture on that medium when other culture media are used.
Candida species cannot be identified either by direct microscopy or by culture macro- and microscopic features. The final species determination relies on the germ tube tests (rapid production of chlamydospores) and on sugar fermentation and assimilation tests, as well as nitrogen utilization (Table 123.5).
Candida strains resistant to antifungals have been detected (35–39); therefore, the antifungal susceptibility test should be performed, especially in nosocomial settings and in immunocompromised patients.
Culture of Malassezia species is not easy to obtain and usually not necessary. The Sabouraud’s agar medium is added with a layer of olive oil to favor Malassezia caramel-colored colonies growth.
Gross Morphology Examination
The colony morphology examination has a relative value, because gross features are changeable and similar to related fungi (Figs. 123.8 and 123.9). Observation includes the reverse side of the tubes or Petri dishes, because some features may differ greatly.


Gross morphology of dermatophyte colonies


Gross morphology of Candida colonies on Sabouraud’s agar
Surface of the colony: convex or flat; elevated with a central button, convoluted with regular folds or vermiculate, with radial branching.
Aspect of the colony: plaster-like or waxy, glabrous or wooly, granular, dusty, creamy.
Color: grayish or creamy, orange, red, purple, pink, cafè au lait, dark brown, black, dark or olive green. The pigmentation density usually varies as it diffuses in the medium and might greatly change on the reverse side of the colony.
Consistency: soft and friable or so hard that it is difficult to detach with the platinum loop.
Culture Microscopic Examination
Once the gross morphology observation is completed, a specimen of the culture is taken with a platinum loop and put on a slide, cleared with one or two drops of KOH or stained with lactophenol cotton blue, which stains the fungal elements in blue, and covered with a cover slip.
The first step of the culture microscopic examination is to reveal if the specimen contains hyphal fungi (septate or not septate) or yeasts (pseudohyphae, budding cells). In the case of yeasts, it is not usually possible to complete identification under the microscope, and therefore a switch to other techniques is necessary, as previously mentioned (implantation on selective medium, sugar fermentation and assimilation test, nitrogen utilization).
The second step is the detailed description of the mycelia elements configurations (Tables 123.6 and 123.7). Some hyphae are very straight, others sinuous, slender, or thick, with periodical enlargement of single enchained elements and/or swelling at the tips of the filaments. These specialized, ornamental or accessory structures, arising from a single cell modification into a thick-walled resting cell, with a very peculiar morphology aid in species identification: spiral and racquet hyphae are commonly seen in Trichophyton mentagrophytes; pectinate body occurs in Microsporum audouinii; chandelier hyphae occur in Trichophyton schoenleinii and Trichophyton violaceum infections, and nodular organ characterize Trichophyton mentagrophytes and Microsporum canis.
Although suggestive, the accessory structures are changeable, and the most important elements to note are the presence of fruiting bodies (spores, chlamydospores, asci, aleuriospores, etc.). In the case of dermatophytes, the micro- and macroconidia configurations, arrangement, and shape make identification certain. Additional biochemical tests may be helpful in distinguishing T. rubrum from T. mentagrophytes: milk agar medium favors T. mentagrophytes growth, while T. rubrum is restricted; T. mentagrophytes is urease positive while T. rubrum is urease negative.
Culture Pitfalls
A negative culture may arise because:
-
The condition is not due to fungal infection.
-
The specimen was not collected properly, especially as regards sterile procedure and eventual bacterial contamination.
-
Antifungal treatment had been used prior to collection of the specimen.
-
There was a delay before the specimen reached the laboratory.
-
The laboratory procedures were incorrect.
-
The organism grows very slowly.
It is advantageous to collect several samples from the patient, to eventually repeat the cultural examination when a fungal infection appears likely, preferably prior to treatment.
Another major problem is false-positive results due to contamination, especially molds development in nail specimens. Molds are ubiquitous and their etiologic role in onychomycosis is very controversial. Onychomycosis due to opportunistic fungi, especially Scopulariopsis brevicaulis, have no specific clinical features, and simple isolation from the nails is not sufficient to assess infection. As a general rule, the suspected pathogen fungus must be detected at least in three different samples of the pathologic material, obtained from several different sites, plated out on at least three different media, including Sabouraud’s agar + actidione.
Other Complementary Examinations in Mycology
Wood’s Lamp Examination
This very simple examination introduced in medical mycology in 1925 by Margarot and Devèz is no more very popular in routine use, requiring a source of ultraviolet rays filtered with a 9–10 % nickel salt sheet of glass (366 nm wavelengths allowed to pass). The examination is performed in a dark room and natural luminescence phenomenon is limited to microsporum species (green fluorescence), pityriasis versicolor (yellow green), and erythrasma (reddish fluorescence). It is otherwise useful to rapidly distinguish the malassezia infection from other skin coloring changes such as vitiligo and to detect tinea capitis during epidemics, especially in schools.
Histological Examination
Biopsy and histological examination does not replace native preparation and usually is unnecessary in superficial fungal infections, but it is sometimes performed to exclude major skin diseases and superinfections, especially if dealing with yeasts. Histological examination allows for primary candidiasis to be distinguished from superinfection, by the presence of a parakeratotic horny layer, stuffed with PAS-positive yeast cells and pseudohyphae.
It is otherwise mandatory to confirm the clinical suspect of rare deep-seated or disseminated fungal diseases, such as actinomycosis, cryptococcosis, histoplasmosis, and other infections. It is also effective to confirm a pathologic role of opportunistic fungi and their relation with the infected tissue. Histology is superior to the other methods in its negative predictive value. The combination of direct microscopy plus histology was 97.8 % sensitive with 98 % negative predictive value and remains the most sensitive diagnostic approach for onychomycosis.
The specific request must be clearly indicated to the pathologist, because simple hematoxylin-eosin stains give more information on the tissue reaction pattern than on the fungal presence and require a very careful examination. It rarely enables a more precise diagnosis than simple mycosis and the fungus cannot be identified as a rule. The most used stains are Hotchkiss-McManus stain (Periodic Acid Schiff reagent, PAS) in all conditions, May-Grunwald-Giemsa and Gram stain to visualize very fine Gram-positive filaments (actinomycosis, nocardiosis), and methenamine silver nitrate staining by Gomori’s method, which is particularly useful to fungal membrane detection.
Electron Microscopy
The extensive use of both transmission and scanning electron microscopy is devoted to research on the morphology and physiology of the various pathogenic fungi. It does not play a role in diagnostic procedures.
Future Perspectives
Mycology is sometimes considered an obsolete assessment, because clinical diagnosis is usually simple and antifungal treatment highly efficacious. Laboratory exam has relied on direct examination for such a long time that interest on research and implementation has been limited for decades. The sensibility of the traditional mycological examinations is not very high and conditioned from the investigator’s expertise. The diagnostic error accounts for about 30 % of the cases. Therefore, last decade’s research has devoted a certain interest to faster, more sensitive, and culture-independent techniques. The molecular biology techniques, especially the polymerase chain reaction (PCR) and in situ hybridization for fungal identification, are highly sensitive but expensive and require complex post-amplification procedures to differentiate relevant fungal types. At the moment, research is limited to deep-seated and disseminated fungal infections (blood infections, drug-resistant Candida and Aspergillus species) or to severe special site infections (fungal keratitis). Preliminary data using real-time polymerase chain reaction high-resolution melting analysis (PCR-HRM) suggest the capacity to detect and differentiate yeasts from filamentous fungi and to discriminate among relevant species of yeasts.
Current limitation of the molecular assays is the lack of methodological standardization and validation, with continuous new method proposals whose results interpretation are not always clear and reproducible.
New impulse to collect samples and make correct fungal identification arises from the assay mass spectrophotometry, which seems to be a cost-effective rapid tool and will probably be largely adopted as routine laboratory determination in an immediate future.
Wide consensus and validation from large prospective studies are necessary to allow widespread adoption of these assays into the clinical setting, but the basic approach with direct microscopy remains the clue to the diagnosis of superficial skin fungal infections.
Reference
Grigoriu D, Delacretaz J, Borelli D. Medical mycology. Toronto: Hans Huber Publishers; 1987.
Further Reading
Alshawa K, Beretti JL, Lacroix C, Feuilhade M, Dauphin B, Quesne G, et al. Successful identification of clinical dermatophyte and Neoscytalidium species by matrix-assisted laser desorption ionization-time of flight mass spectrometry. J Clin Microbiol. 2012;50(7):2277–81.
Ansar A, Farshchian M, Nazeri H, Ghiasian SA. Clinico-epidemiological and mycological aspects of tinea incognito in Iran: a 16-year study. Med Mycol J. 2011;52(1):25–32.
Atzori L, Pau M, Aste N, Aste N. Dermatophyte infections mimicking other skin diseases: a 154-person case survey of tinea atypica in the district of Cagliari (Italy). Int J Dermatol. 2012;51(4):410–5.
Bašková L, Buchta V. Laboratory diagnostics of invasive fungal infections: an overview with emphasis on molecular approach. Folia Microbiol. 2012;57(5):421–30. Praha.
Bejdák P, Lengerová M, Paloušová D, Volfová P, Kocmanová I, Mayer J, Ráčil Z. Detection and identification of filamentous fungi causing mycoses using molecular genetic methods. Klin Mikrobiol Infekc Lek. 2012;18(4):109–14.
Bugli F, Cacaci M, Martini C, Torelli R, Posteraro B, Sanguinetti M, Paroni SF. Human monoclonal antibody-based therapy in the treatment of invasive candidiasis. Clin Dev Immunol. 2013;2013:403121.
Faergemann J, Fredriksson T, Herczka O, Krupicka P, Björklund KN, Sjökvist M. Tinea incognito as a source of an “epidemic” of Trichophyton violaceum infections in a dermatologic ward. Int J Dermatol. 1983;22(1):39–40.
Giri S, Kindo AJ. A review of Candida species causing blood stream infection. Indian J Med Microbiol. 2012;30(3):270–8.
Goldschmidt P, Degorge S, Benallaoua D, Semoun O, Borsali E, Le Bouter A, et al. New strategy for rapid diagnosis and characterization of keratomycosis. Ophthalmology. 2012;119(5):945–50.
Gray LD, Roberts GD. Laboratory diagnosis of systemic fungal diseases. Infect Dis Clin North Am. 1988;2(4):779–803.
Ive FA, Marks R. Tinea incognito. Br Med J. 1968;3(5611):149–52.
Karimzadegan-Nia M, Mir-Amin-Mohammadi A, Bouzari N, Firooz A. Comparison of direct smear, culture and histology for the diagnosis of onychomycosis. Australas J Dermatol. 2007;48(1):18–21.
Kourkoumpetis TK, Fuchs BB, Coleman JJ, Desalermos A, Mylonakis E. Polymerase chain reaction-based assays for the diagnosis of invasive fungal infections. Clin Infect Dis. 2012;54(9):1322–31.
Krajewska-Kulak E, Niczyporuk W, Lukaszuk C, Bartoszewicz M, Roszkowska I, Edyta M. Difficulties in diagnosing and treating tinea in adults at the department of dermatology in Bialystok (Poland). Dermatol Nurs. 2003;15(6):527. -30, 534.
Lawry MA, Haneke E, Strobeck K, Martin S, Zimmer B, Romano PS. Methods for diagnosing onychomycosis: a comparative study and review of the literature. Arch Dermatol. 2000;136(9):1112–6.
Lewis 2nd JS, Wiederhold NP, Wickes BL, Patterson TF, Jorgensen JH. Rapid emergence of echinocandin resistance in candida glabrata resulting in clinical and microbiologic failure. Antimicrob Agents Chemother. 2013;57(9):4559–61.
Liu D, Cloe S, Baird R, Pedersen J. Application of PCR to the identification of dermatophyte fungi. Med Microbiol. 2000;49:493–7.
Ma CF, Li FQ, Shi LN, Hu YA, Wang Y, Huang M, Kong QQ. Surveillance study of species distribution, antifungal susceptibility and mortality of nosocomial candidemia in a tertiary care hospital in China. BMC Infect Dis. 2013;13(1):337.
Marcos JY, Pincus DH. Fungal diagnostics: review of commercially available methods. Methods Mol Biol. 2013;968:25–54.
Margarot J, Devèz P. La lumière de Wood en dermatologie. Ann Derm Syph. 1929;10:581.
Mazuelos EM, García AI. Microbiological aspects of the cryptococcosis in the post-HAART era. Enferm Infecc Microbiol Clin. 2010;28 Suppl 1:40–5.
Nenoff P, Erhard M, Simon JC, Muylowa GK, Herrmann J, Rataj W, Gräser Y. MALDI-TOF mass spectrometry – a rapid method for the identification of dermatophyte species. Med Mycol. 2013;51(1):17–24. doi:10.3109/13693786.2012.685186. Epub 2012 May 10.
Ni W, Huang Q, Cui J. Disseminated cryptococcosis initially presenting as cellulitis in a patient suffering from nephrotic syndrome. BMC Nephrol. 2013;14:20.
Olson TC, Bongartz T, Crowson CS, Roberts GD, Orenstein R, Matteson EL. Histoplasmosis infection in patients with rheumatoid arthritis, 1998–2009. BMC Infect Dis. 2011;11:145.
Paloušová D, Lengerová M, Volfová P, Bejdák P, Kocmanová I, Mayer J, Ráčil Z. Invasive fungal infections in immunocompromised patients with focus on aspergillosis and its causative agents. Klin Mikrobiol Infekc Lek. 2012;18(4):96–101.
Paul AY, Aldrich S, Scott RS, Ellis MW. Disseminated histoplasmosis in a patient with AIDS: case report and review of the literature. Cutis. 2007;80(4):309–12.
Richardson MD. Changing patterns and trends in systemic fungal infections. J Antimicrob Chemother. 2005;56 Suppl 1:i5–11.
Robert R, Pihet M. Conventional methods for the diagnosis of dermatophytosis. Mycopathologia. 2008;166(5–6):295–306.
Romano C, Maritati E, Gianni C. Tinea incognito in Italy: a 15-year survey. Mycoses. 2006;49(5):383–7.
Sanglard D, Odds FC. Resistance of Candida species to antifungal agents: molecular mechanisms and clinical consequences. Lancet Infect Dis. 2002;2(2):73–85.
Schubach A, Barros MB, Wanke B. Epidemic sporotrichosis. Curr Opin Infecjt Dis. 2008;21(2):129–33.
Seyfarth F, Wiegand C, Erhard M, Gräser Y, Elsner P, Hipler UC. Identification of yeast isolated from dermatological patients by MALDI-TOF mass spectrometry. Mycoses. 2012;55(3):276–80.
Shenoy MM, Teerthanath S, Karnaker VK, Girisha BS, Krishna Prasad MS, Pinto J. Comparison of potassium hydroxide mount and mycological culture with histopathologic examination using periodic acid-Schiff staining of the nail clippings in the diagnosis of onychomycosis. Indian J Dermatol Venereol Leprol. 2008;74(3):226–9.
Skerlev M, Miklić P. The changing face of microsporum spp infections. Clin Dermatol. 2010;28(2):146–50.
Spampinato C, Leonardi D. Candida infections, causes, targets, and resistance mechanisms: traditional and alternative antifungal agents. Biomed Res Int. 2013;2013:204237.
Sunenshine RH, Anderson S, Erhart L, Vossbrink A, Kelly PC, Engelthaler D, Komatsu K. Public health surveillance for coccidioidomycosis in Arizona. Ann N Y Acad Sci. 2007;1111:96–102.
Theel ES, Hall L, Mandrekar J, Wengenack NL. Dermatophyte identification using matrix-assisted laser desorption ionization-time of flight mass spectrometry. J Clin Microbiol. 2011;49(12):4067–71.
Vonberg RP, Gastmeier P. Nosocomial aspergillosis in outbreak settings. J Hosp Infect. 2006;63(3):246–54.
Weinberg JM, Koestenblatt EK, Tutrone WD, Tishler HR, Najarian L. Comparison of diagnostic methods in the evaluation of onychomycosis. J Am Acad Dermatol. 2003;49(2):193–7.
Wolfson JS, Waldron MA, Sierra LS. Blinded comparison of a direct immunofluorescent monoclonal antibody staining method and a Giemsa staining method for identification of Pneumocystis carinii in induced sputum and bronchoalveolar lavage specimens of patients infected with human immunodeficiency virus. J Clin Microbiol. 1990;28(9):2136–8.
Yamaguchi T, Ito S, Takano Y, Umeda N, Goto M, Horikoshi M, et al. A case of disseminated sporotrichosis treated with prednisolone, immunosuppressants, and tocilizumab under the diagnosis of rheumatoid arthritis. Intern Med. 2012;51(15):2035–9.
Acknowledgement
The authors are grateful to Barry Mark Wheaton for the kind revision of the English text.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2015 Springer-Verlag Berlin Heidelberg
About this chapter
Cite this chapter
Atzori, L., Pau, M., Aste, N. (2015). Mycological Examination. In: Katsambas, A.D., Lotti, T.M., Dessinioti, C., D’Erme, A.M. (eds) European Handbook of Dermatological Treatments. Springer, Berlin, Heidelberg. https://doi.org/10.1007/978-3-662-45139-7_123
Download citation
DOI: https://doi.org/10.1007/978-3-662-45139-7_123
Publisher Name: Springer, Berlin, Heidelberg
Print ISBN: 978-3-662-45138-0
Online ISBN: 978-3-662-45139-7
eBook Packages: MedicineMedicine (R0)