
Abstract
Due to demographic changes, the welfare state principle and the solidarity principle are under scrutiny. Social security funds must now consider European labor mobility and immigration. The healthcare market is a growth market. Inpatient rehabilitation, however, does not grow proportionally to the market due to the existing legal framework. The introduction of the Social Code (SGB) Ninth Book (IX) and the definition of disability based on the bio-psycho-social model of the International Classification of Functioning, Disability, and Health (ICF) and the expert assessment of the need for rehabilitation lead to the ICF increasingly being implemented. An effective tool in this setting is the standardized Work Rehabilitation Questionnaire (WORQ), based on the ICF, which is freely available in six languages. Motivation plays a pioneering role in rehabilitation, especially for Return to Work (RTW). The aim of this study was to cross-culturally adapt the WORQ to German and to investigate whether the WORQ in combination with the Diagnostic Tool for Work Motivation (DIAMO) can be used to target suitable rehabilitation measures and improve RTW. First, a cross cultural adaptation of the WORQ is needed in a German rehabilitation setting. This adaptation requires interdisciplinary collaboration between the developers of the WORQ, independent advisors, patients, and other scientists. This study report on the quantitative results and recommendation for clinical practice is discussed in this chapter.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


1 Introduction
Health is not everything – but without health everything is nothing.
-- Arthur Schopenhauer (1788–1860), German philosopher
The improvement in prevention, the rehabilitation process in clinics and outpatient facilities, is necessary to enable work and integration. The current public discussions about the cost explosion in health care, the demographic change, the increase in the statutory retirement age after 2030 (Bofinger et al., 2016, p. 38), demography collective agreements (Zumbeck, 2017, p. 16), and workplace design in line with the concept of ‘Arbeit 4.0’ (Braun, 2016, pp. 13–16) give rise to further considerations about the targeted and more efficient use of the available funds with regard to treatment success (Belzl, 2006). The desire of the Techniker Krankenkasse (TK) to collect and evaluate personal member data by means of fitness bracelets (Becker, 2016, p. 4), shows how up-to-date and important the topic of effective health prevention and rehabilitation by social insurance institutions is. As part of a feasibility study, we evaluated the benefits of the International Classification of Functioning, Disability, and Health (ICF; World Health Organization, 2011) and the holistic bio-psycho-social model for assessing needs and participation in working life for a cross-agency use of each institution for implementation (Bundesministerium für Arbeit und Soziales, 2016, S. 27, 28; Schubert et al. 2014, p. 133). The ICF is a language with an internationally recognized vocabulary standard for uniform communication in interdisciplinary communication (Vreeman and Richoz, 2015). This allows for an assessment of individual needs and the required service provision in the context of dynamic process control (Schubert et al., 2014, p. 133).
In 2018, 411 billion euros were spent on health services in Germany (Statistisches Bundesamt, 2020), which is 4.944 euros per inhabitant. This is an increase of 96 billion euros or 23% compared to 2013 (Statistisches Bundesamt, 2016b; 2020). Figure 5.1 shows the development of health expenditure from 2005 to 2018 in euros.

It should be noted that within health expenditure, according to the Statistisches Bundesamt, only expenditure on the final consumption of health goods, services and investments in the health sector is included (excluding intermediate consumption such as the production of medicines and sales to pharmacies). In addition, research and development costs are included, provided they are carried by the issuers. Expenses for care, occupational health insurance and health measures for reintegration into working life are also considered health expenditure (Statistisches Bundesamt [Destatis], 2017a). Not included are costs for wellness, fitness, or accommodation in nursing homes.
This chapter deals with the framework conditions set out in the Sozialgesetzbuch (SGB), Ninth Book (IX)—Rehabilitation and Participation of Disabled Persons, 2001. Rehabilitation is an interdisciplinary research field of psychology, social psychology, medicine, sociology, ethics, data protection, and law. In 2015, around 7.6 million persons were severely disabled, that is, 9.3% of the total population in Germany, 51% of which were men. Persons who have been granted a degree of disability of 50 % or more by the healthcare authorities and given a valid ID card, are considered to be severely disabled (Statistisches Bundesamt, 2016d). The numbers increase with the increasing life expectancy in Germany. More than one billion people in the world live with some form of disability, of whom nearly 200 million experience considerable difficulties in functioning (World Health Organization, 2011, p. xi). Spending on rehabilitation amounted to € 32.6 billion in 2014 (Reha-Info, 2016, S. 1). Figure 5.2 shows the percentages of expenditures by each carrier.

Expenditure Ratio (in Percentage) of € 32.6 Billion in Rehabilitation Spending in Rehabilitation Institutions in 2014
The participation services are subdivided into four service groups within the meaning of § 5 SGB IX. These are the services for medical rehabilitation, support and supplementary benefits, benefits for participation in the community life as well as benefits for participation in working life, for example, retraining. The costs of the partial hire services will be allocated to them according to the tasks of the individual carriers. The house of rehabilitation providers within the meaning of § 6 SGB IX illustrates this in Fig. 5.3.

House of Rehabilitation Institutions according to § 6 SGB IX
In Germany, the number of inpatient rehabilitation patients decreased by 0.2% in 2015 compared to the previous year. In 2015, 19.2 million rehabilitation patients were hospitalized in hospitals. The 1.153 prevention or rehabilitation facilities differ in ownership or legal form according to public (229), non-profit (300), and private (624) institutions. The 624 private preventive or rehabilitation facilities are dominant in the market (Statistisches Bundesamt, 2016c). The participation of the rehabilitation facilities is approved by the German Pension Insurance for inpatient medical rehabilitation either after having gone through inpatient hospital treatment (e.g. after surgery or chemotherapy) (AHB) (Deutsche Rentenversicherung Bund, 2006), or following the requirements of the statutory accident insurance at the ‘Professional Association’s stationary treatment (BGSW)’ for injuries of the musculoskeletal system according to § 34 SGB VII (Deutsche Gesetzliche Unfallversicherung und Sozialversicherung für Landwirtschaft, Forst und Gartenbau, 2016).
The distribution by facilities, staff and age group in the prevention or rehabilitation facilities is shown in Fig. 5.4. Inpatient treatments include, in the context of accident insurance, the professional association’s stationary treatment (BGSW), e.g. after severe injuries of the musculoskeletal system, and the complex inpatient rehabilitation (KSR), e.g. after a cross-sectional injury (Simmel et al., 2014, pp. 524–529). Pensions for reduced work capacity due to mental disorders more than doubled during the period from 1993 to 2010 (Fig. 5.5). In Germany, the legal framework is designed and implemented by the Sozialgesetzbuch (SGB) or by regulations and guidelines. The importance of the topic stems from the current discussion on demographic change, skills shortages, legislation, prevention, or cost restraints on public budgets.

(Source Statistisches Bundesamt, 2015, table time series updated in 2021, p. 7)
Prevention and Rehabilitation Facilities by Facilitites, Staff and Patients by Age Group 2014.

(Source Adapted from Bering and Schmidt-Ohlemann, 2013, p. 3)
Pensions due to Reduced Earning Capacity.
The rehabilitation, prevention, and participation are interdisciplinary scientific research fields, which overlap with psychology, law, social sciences, medicine, sports science, and business administration. As a result, a definition of the term in this article is essential in order to create a common level of understanding. In 1948, the WHO defined health as follows:
“Health is a state of complete physical, mental and social well-being and not merely the absence of disease or infirmity. The enjoyment of the highest attainable standard of health is one of the fundamental rights of every human being without distinction of race, religion, political belief, economic or social condition.” (World Health Organization, 2011; Klein, 2015, p. 34).
In the delimitation of the health term, the disability term is defined according to the decision of the European Court of Justice Kaltoft ECJ (12/18/2014, case C-354/13):
An illness of an employee is considered a disability when it constitutes
“a limitation which results in particular from physical, mental or psychological impairments which in interaction with various barriers may hinder the full and effective participation of the person concerned in professional life on an equal basis with other workers, and the limitation is a long-term one” (Albert et al. 2016, p. 397).
In the individual European member states, the goals and definitions for the term disability and thus the disability policy are different (Maschke, 2008, p. 5775). In Germany, the Ninth Book of the Social Code—Rehabilitation and Participation of Disabled Persons—(Neuntes Buch SGB IX) defines disability in § 2 (1):
Menschen sind behindert, wenn ihre körperliche Funktion, geistige Fähigkeit oder seelische Gesundheit mit hoher Wahrscheinlichkeit länger als sechs Monate von dem für das Lebensalter typischen Zustand abweichen und daher ihre Teilhabe am Leben in der Gesellschaft beeinträchtigt ist. Sie sind von Behinderung bedroht, wenn die Beeinträchtigung zu erwarten ist. (Neuntes Buch SGB IX, Bundesgesetzblatt i. d. F. of 06/19/2001 BGBl. l, p. 1046, 1047; last changed at 07/26/2016 BGBl. l, pp. 1824, 1837, § 2 (1))
People are disabled if their physical function, mental ability, or mental health is likely to be more than six months away from the typical state of life, and therefore their participation in society is impaired. You are at risk of disability if the impairment is expected. (Own Translation)
In rehabilitation and prevention practice, these and other framework conditions should be directly integrated into practice-oriented and applicable organizational procedures.
The International Classification of Diseases (ICD) has been in existence for more than 100 years, and its amendment, the International Classification of Functioning, Disability, and Health has existed for more than 16 years (Stucki, 2012, p. 1). In order to understand the ICF concept of functioning, it is necessary to compare the definitions made in the previous section. Disability is seen in relation to functioning. The domain ranges from complete functioning to complete disability on a gradual scale as illustrated in Fig. 5.6 (Bickenbach, 2012 p. 5). The ‘functioning’ includes the body functions, body structures, and activities and participation. The integrative bio-psycho-social model of functioning, as illustrated in Fig. 5.7, shows the mutual influences of the individual factors and components (Rauch et al., 2012, p. 9). The terms used in the model are described in more detail in Table 5.1.

Illustration of Functioning, e.g. Hearing According to the ICF

The Integrative Bio-psycho-social Model of Functioning, Disability, and Health
To develop a common understanding of the ICF, a hierarchical coding system has been suggested. The ICF has a hierarchical structure and consists of two parts: “functioning and disability” and “contextual factors”.
These two factors again consist of two components each:
-
“Functioning and disability”
-
Body functions and structures
-
Activities and participation
-
-
“Contextual factors”
-
Environmental factors
-
Person-related factors (not yet defined)
-
The categories are subdivided according to the chapter heading (item of the first level) down into the item of the fourth level (Table 5.2) (Rauch et al., 2012, p. 11).
The ICF model and category system aim to make it clear that the interactions between the individual factors and components can lead to imbalances, for example, after an accident, a cancer diagnosis, or a job loss. This can lead to a prolonged absence from work. As a result, professional contacts can be reduced, and the work rhythm that gives structure to everyday life can change or break down considerably, and eventually material losses can occur. Health is thus not only an attribute of a person but affects the entire social and environmental context of the person. The following Fig. 5.8 illustrates a version of the bio-psycho-socio-ecological concept of health following the WHO's definition of health (see above) .

The Bio-psycho-socio-ecological Concept of Health
The basis for this model is to ease ‘return to work’ (RTW), such as re-entry into working life after a long period of unemployment or sickness absence. This multi-scientific knowledge of psychology, neurobiology, medicine and integrative therapy forms the basis for health coaching (Hartz & Petzold, 2014, p. 61). In doing so, the volitional competencies required to face this challenge are promoted, for example, by restrictions of physical functioning. Education and professional status seem to play a central role in the perception of the job situation. Obviously, perceived job risks may increase the health risk of workers.
In order to find a suitable individual ‘return to work’ approach, the German-speaking Work Rehabilitation Questionnaire—WORQ (Finger et al., 2013) was developed for the first time in Germany. The aim of the questionnaire is to standardize information about the person, the professional situation, rehabilitation, and function. With this information, a multifunctional team (e.g. doctors, physiotherapists, osteopaths, psychologists, and nutritionists) should use this questionnaire individually as a communication and documentation basis for rehabilitation and RTW to enable development processes. The advantage of the multimodal concepts in rehabilitation is being guided by the statutory accident insurance controlling the treatment of the injured and referring to a professional accident clinic to protect individuals from disability (Bethge, 2011, p. 145). As part of the rehabilitation documentation, the ‘Integration of ICF documentation tools into the rehabilitation cycle’ was developed, which with the WORQ can form a documentation basis by means of the ICF (Glassel et al., 2012, p. 467). As part of the rehabilitation, the data on the questionnaires WORQ and Diagnostic Tool for Work Motivation (DIAMO) (Fiedler et al., 2008) have not yet been collected in Germany. The WORQ has been translated in Switzerland to Swiss-German, therefore only for the German-speaking region (Swiss Paraplegic Research/ICF Research Branch).
The adaptation of the WORQ was preceded by a literature search on rehabilitation test procedures used in Germany. The identification of tests measuring rehabilitation motivation and treatment expectation or work motivation is listed in Table 5.3.
The development of the WORQ was based on the ICF core set for vocational rehabilitation consisting of 90 categories, of which 13 are included in the Brief ICF Core Set (Finger et al., 2013). The WORQ has been cross-culturally adapted to several languages, and for German speaking persons, it has been adapted to German-Switzerland and German-Germany (see www.myworq.org; Finger et al., 2013, 2015; Finger and Escorpizo 2016a, b; Veith-Tezeren et al., 2017b, c). The German-Germany adaptation was carried out as part of a research project to improve rehabilitation and RTW, guided by a quality management approach, i.e. SWOT analysis and the Continuous Improvement Cycle (see Figs. 5.9 and 5.10).

Continuous Improvement Cycle

Strengths and Weaknesses (SWOT Analysis) of WORQ
The WORQ enables self-assessed patient reports and clinician rated assessments. The results can be used to tailor the rehabilitation process also in relation to other relevant therapies. Combinations with other questionnaires within psychology, pain therapy, physiotherapy, and sociology are also possible. The strength lies in the ICF language and in the WORQ since it has been cross-culturally adapted to the legal and cultural framework in different languages. In Germany, with approximately 646.000 employed persons from different countries (Statistisches Bundesamt, 2017b), language barriers are common in the rehabilitation facilities.
2 Method
The two clinics participating in this study were the Berufsgenossenschaftliche Unfallklinik (BGU), Frankfurt am Main, which is part of the hospital group of statutory accident insurance gGmbH and a private non-profit company, while the HKB-Klinik GmbH & Co., Klinik Rabenstein (KR) is a private clinic (Veith-Tezeren, 2017a). The cross-cultural adaptation of the WORQ German-Germany (GG; self-report long version and brief versions) was carried out with the participation of the authors of the original test following standard procedures of a cultural adaptation regarding questionnaires (e.g. experts, lay participants and patients). The questionnaires used in this study were thus the DIAMO (Fiedler et al., 2008) and WORQ GG. The standardized work motivation questionnaire DIAMO has closed questions and utilizes a so-called item wording effect, a methodological artefact used in empirical social research (Fiedler et al., 2008, p. 481).
Sample
The aim of this study was to cross-culturally adapt the WORQ to German and to investigate the relationship between the WORQ and the DIAMO as well as their association with different rehabilitation measures. The BGU clinic only accepts rehabilitation patients from accident insurance companies or privately insured persons, while the CR is open to all insured persons if the diagnosis is approved for treatment. Power calculations for t-tests with an α-error probability of 0.05 and a power of 0.8 and able to detect an average effect of d = 0.5 resulted in a sample size of N = 128, or N = 64 in each clinic. The power calculations for the correlations was based on an α-error probability of 0.05 and a power of 0.8 capable of revealing a mean effect of | r | = 0.3 resulting in a sample size of N = 82.
Adaptation WORQ–German-Germany
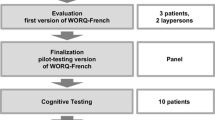
The first pre-test of the WORQ GG in Germany at the KR revealed that the educational system and vocational training, as well as the social welfare system of Switzerland, differ from those in Germany. Language barriers also led to problems of understanding that could only be resolved in a one-to-one interview, which meant that the study had to be based on interviews. Cross-cultural adaptations of the WORQ German Swiss self-report and brief versions to WORQ GG started by recruiting three patients and three neutral persons after the first pre-test survey in the KR by expert groups. The exchange of information on the WORQ GG took place through personal meetings and discussions, through voting on the results via e-mails and via telephone conferences. Particular attention was paid to the differences in school and vocational qualifications between the USA, Switzerland, and Germany. The patient group, two women and one man, concluded at the ratio of two to one, that the WORQ German-Swiss was too long. In addition, the question sequence was criticised. The group of neutral persons, two women and two men, concluded at the ratio of three to one, that the WORQ GG was not too long. The expert group of six people, three women and three men, focused on the cross-cultural adaptation of Part 1 in the WORQ GG. Particularly on understanding the content of the questions and on the length, as the existing WORQ GG should be limited to not more than six pages. The order of the questions in the brief and SR versions of the WORQ GG was changed so that they were compatible with the order within the ICF coding system. In Part 2 of the WORQ GG questionnaire, only linguistic adjustments were made.
Statistical Analysis
Data were analysed using LimeSurvey, G*Power and R Version 3.3.3. Missing values resulting from unanswered questions were supplemented by a mean value imputation. An independent samples t-test was used to analyse group differences. The t-test assumes a normal distribution of the examined variables in both groups. This can be assumed for a sample size greater than N = 30 in both groups (Gravetter & Wallnau, 2009, p. 204). Pearson correlation coefficient was used to analyse the association between two variables. Associations between the work motivation of the rehabilitation patients using DIAMO and ICF impairments using WORQ were explored.
3 Results
A total of 163 participants aged between 18 and 65 years took part in the study (mean age 47.9 years), consisting of 117 men and 45 women (one participant did not indicate gender). Table 5.4 shows the martial status of the participants.
Education
40% of the participants had a lower secondary school diploma (Hauptschule) forming the largest group, while 33% had a higher secondary school degree (Realschule), and 13% had Abitur or general university entrance qualification (Hochschulreife). The number of other school qualifications were less than 10%. Figure 5.11 shows the distribution of education among the participants.

Distribution of Education
Vocational Qualifications
The vocational qualifications are illustrated in Fig. 5.12. Most notably is that 63 participants have completed a certificate of apprenticeship, while 28 participants have obtained an academic degree.

Vocational Qualifications of Respondents
Occupational Relationships in the Main Activity
Most of the participants were employed (87%) as displayed in Fig. 5.13. The BGU exclusively provide treatment for persons undergoing rehabilitation in connection with their occupation, by accident, occupational disease, or an impending occupational disease.

Employment Relationships in the Main Activity
Degree of Employment
54 participants worked full-time, while many were not able to work due to being in rehabilitation or due to health reasons. The details can be seen in Fig. 5.14.

Degree of Employment
Duration of Disability
The duration of occupational disability in years can be seen in Fig. 5.15. Most of the participants have had occupational issues for one and a half years.

Duration of Disability (WORQ SR GG)
Reliability Analysis
The WORQ GG showed a Cronbach’s Alpha value of 0.94 with a sample size of 163 participants and 36 items, representing high internal consistency. This is also acceptable compared to the Cronbach’s Alpha value of 0.88 in Finger et al. (2013, p. 507) having a sample size of 74.
Mean Complaint Level
The mean level of complaints from part 2 of the WORQ is displayed for BGU (Fig. 5.16), KR (Fig. 5.17) and BGU and KR combined (Fig. 5.18) (BGU). The figures display the increase in complaint intensities from left to right. The combined scores show that pain is the most severe symptom complaint, followed by general stamina, sleeping function and moving in another way.

Mean Complaint Type, items in the BGU on the WORQ SR GG

Mean Complaint Type, items in the Klinik Rabenstein on the WORQ SR GG

Mean Complaints on the WORQ SR GG items
The participants in the BGU clinic scored above the mean value of 5 for eight categories of which moving in another way was highest, while the participants in KR clinic reported fewer complaints above the mean value of 5 (pain and sleeping function). Comparing the BGU and KR reveals the former scores higher in all selected categories (Table 5.5).
Group Comparison by Gender of all Items According to WORQ SR GG
The comparison of men and women indicates that women seem to score higher than men (Table 5.6).
Correlation Analysis of 11 DIAMO Dimensions with 36 items (34 dimensions) WORQ SR GG
The results of the correlational analysis between the 11 DIAMO and the 34 WORQ GG dimensions are described below.
-
The DIAMO target inhibition correlates with the WORQ GG item ‘d240, handling stress and other psychological requirements’ (r = 0.33)
-
The DIAMO target inhibition correlates with the WORQ GG item ‘d3503, talking to a person’ (r = 0.31).
-
The DIAMO target inhibition correlates with the WORQ GG item ‘d3150 communicating as a receiver of hand signs or gestures’ (r = 0.3).
-
The DIAMO dimension failure avoidance correlates with the WORQ GG item ‘d3150, communicating as a recipient of gestures or gestures’ (r = 0.29).
-
The DIAMO dimension work incentive and desire for change (AV) correlates with the WORQ GG item ‘d210, adopt a single task’ (r = 0.29).
-
DIAMO target inhibition correlates with the WORQ GG item ‘b164, higher cognitive functions’ (r = 0.28).
-
The DIAMO dimension work incentive and desire for change (AV) correlates with the WORQ GG item ‘d475, driving a vehicle’ (r = 0.27).
-
The DIAMO dimension work incentive and desire for change (AV) correlates with the WORQ GG item ‘d540, dressing oneself’ (r = 0.27).
-
The DIAMO load factor (BL) in the workplace correlates with the WORQ GG item ‘b164, Higher cognitive functions’ (r = 0.27).
-
The DIAMO target inhibition correlates with the WORQ GG item ‘d160, focus attention’ (r = 0.27).
-
The DIAMO dimension settings for work correlates with the WORQ GG item ‘d430, lifting and carrying objects’ (r = 0.27).
-
The DIAMO dimension settings for work correlates with the WORQ GG item ‘d475, driving a vehicle’ (r = 0.26).
-
The DIAMO dimension settings for work correlates with the WORQ GG item ‘d540, dressing’ (r = 0.26).
-
The DIAMO target inhibition correlates with the WORQ GG item ‘b126, functions of temperament and personality’ (r = 0.26).
-
The DIAMO target inhibition correlates with the WORQ GG item ‘d177, making decisions’ (r = 0.26).
-
The DIAMO load factor (BL) in the workplace correlates with the WORQ GG item ‘d3503, talking to a person’ (r = 0.26).
Correlations Between Age and DIAMO
The correlational analysis between age and DIAMO reveals the following findings:
-
The work attitudes (EA) correlate negatively with age (r = -−0.29).
-
The target activity (ZA) correlates negatively with age (r = -−0.34).
-
The work incentive and desire for change (AV) correlates negatively with age (r = -−0.28).
Finally, an exploratory correlation analysis was carried out between the Depression Core Set in the WORQ SR GG with DIAMO and a significant correlation between target inhibition and Psychiatric Core Set (r = 0.303).
Comparing BGU and KR on DIAMO
The DIAMO factor ‘attitude to work’ (t (152,99) = 2.80, p = 0.006) differs between participants at the BGU (mean = 3.80) and KR (mean = 3.44). The factor ‘target activity’ differs also between (t (152,31) = 2.63, p = 0.009; BGU, mean = 3.98; KR, mean = 3.68) as well as ‘work desire change request’ (t (144.86) = 2.026, p = 0.04; BGU, mean = 3.07; KR, mean 2.85).
4 Discussion
The results of the WORQ SR GG and the DIAMO show that both questionnaires can be used to target suitable rehabilitation measures. For data protection reasons, the collected data could only be evaluated at the group level. An individual analysis in electronic form, administered at regular intervals, could contribute to improving RTW for each participant through optimizing communication and documentation and gaining new insights. On the basis of the current results, there seem to be differences between the rehabilitation programs at the BGU and KR. Common to all programs is that insufficient sleep, which is often compensated by medication, has more impact on functioning compared to the other ICF categories.
The association between the target inhibition of the DIAMO and the item ‘dealing with stress and other mental demands’ of the WORQ SR GG, indicates that a stronger focus on coping strategies within the rehabilitation setting must be addressed, so that the patients’ re-entry-into-the-work process can be facilitated. Any implementation of new interventions should carefully consider the mental models of patients representing the whole setting.
The gender and age-specific relationships between the complaints arising from the ICF questionnaires, the WORQ SR GG and the DIAMO work motivation questionnaire need to be further investigated. The focus could be on the contextual factors. The workplace-specific conditions in companies could be further investigated for factors that favour or inhibit RTW. The prolonged sickness absence of employees from the work process leads to many social and financial challenges in the age of accelerated adjustment (Arbeit 4.0). Thus, the likelihood that workplace processes, work requirements, and departmental structures have changed noticeably at the time of reentry into employment may have considerably increased during individuals’ sick leave or rehabilitation process. Especially in the current phase of corporate restructuring, it is therefore important for rehabilitants to stay in contact with the workplace during the entire rehabilitation process and to be informed of and, if necessary, to be involved in first-hand changes in one’s own workplace. This promotes the commitment to the company, which represents a gain for the company in the current situation of skill shortages. On the other hand, a high fluctuation of employees leads to rising costs, simply because of the long training periods required.
Taking into account the results of the present study, participants from BGU and KR might benefit from a number of obvious proposed measures with regard to the average severity of their worst complaints. These are suggested in Table 5.7 in descending order, with no claim to completeness.
Sleep is one of the most important prerequisites for mental and physical health. The need for restful sleep was indicated by participants at both clinics. In the current sample, lack of sleep seems to affect symptoms of pain, general stamina, function to move in a different way, and the function muscle strength, also negatively contributing to tensions in the family and at work. The effects of sleep disorders can negatively affect cognitive functions such as concentration, pain, sensation of pain, and spontaneous pain (Schuh-Hofer et al. 2016) as well as heart problems, weakening of the immune system, fat cells, stomach, joints and muscles (Schuh-Hofer et al., 2016). See Fig. 5.19 for a summary.

(Source Adapted from Myers, 2014 p. 108)
Possible Effects of Sleep Deprivation.
5 Conclusion
It was not examined whether the differences between the rehabilitation programs of the BGU and the KR lead to different RTW results. This might be explored in a long-term WORQ study. In addition, the introduction of the ZAZO (Zielanalyse and Zieloperationalisierung, standing for target analysis and operationalisation) training concept in the clinics could address the specific needs of each group in a customer-oriented manner. In doing so, information influencing RTW could be analysed more precisely. A number of further research questions are connected with the investigations carried out in the present work, e.g.:
-
Effects on job satisfaction among male and female rehabilitees after RTW
-
Tailoring occupational rehabilitation for part-time employees over the age of 65 with regard to RTW
-
Impact of school education or vocational training on RTW? Age-specific industry differences in RTW
In a long-term study, the integration of the WORQ SR GG into the rehabilitation process would most likely lead to further evidence-based improvements of the whole rehabilitation process. The latter could support the planned amendments to the SGB IX on 01.01.2023.
References
Albert, N.G., (trans.) Erber, G., & Peniston, W. (2016). Lesbian Decadence: Representations in art and literature of fin-de-siècle France. New York: Harrington Park Press.
Becker, K.B. (09. Februar 2016). Kassen wollen Daten von Fitness-Armbändern nutzen. Der Patientenbeauftragte der Bundesregierung pocht aber auf Freiwilligkeit, die Ärzte lehnen den Vorstoß strikt ab. Süddeutsche Zeitung, 4.
Belzl, H. (2006). Physiotherapie nach Verletzung. Trauma und Berufskrankheit, 8(Suppl 1), 87–89.
Bering, R., & Schmidt-Ohlemann, M. (2013). Implementierung der Internationalen Klassifikation der Funktionsfähigkeit, Behinderung und Gesundheit (ICF) zur Klassifizierung von psychischen Beeinträchtigungen. Deutsche Vereinigung für Rehabilitation DVfR, November (S. 1–17).
Bethge, M. (2011). Erfolgsfaktoren medizinisch-beruflich orientierter orthopädischer Rehabilitation. Rehabilitation, 50(03), 145–151.
Bickenbach, J. (2012). Was ist die Funktionsfähigkeit und warum ist sie von Bedeutung. In: J. Bickenbach (Hrsg.), Die ICF-Core-Sets. Manual für die klinische Anwendung. Programmbereich Gesundheit (1. Aufl., S. 4–7). Bern: H. Huber.
Bofinger, P., Feld, L. P., Schmidt, C. J., Schnabel, I., & Wieland, V. (2016). Zeit für Reformen. Jahresgutachten 2016/17. Bonifatius GmbH Druck-Buch-Verlag.
Braun, M. (2016). Arbeit 4.0 menschengerecht gestalten. Schwerpunkt. Betriebliche Prävention, 2016(01), 13–18.
Bundesministerium für Arbeit und Soziales. (Hrsg.). (2016). Rehabilitation und Teilhabe behinderter Menschen. https://www.bmas.de/SharedDocs/Downloads/DE/PDF-Publikationen/a990-rehabilitation-und-teilhabe-deutsch.pdf?__blob=publicationFile. Accessed 11 Feb 2020.
Deck, R., Zimmermann, M. & Raspe, H. (2008). FREM-17. In Diagnostische Verfahren in der Rehabilitation (Diagnostik für Klinik und Praxis, Bd. 5, S. 98–100). Göttingen: Hogrefe.
Deutsche Rentenversicherung Bund. (Hrsg.). (22. August 2006). Anforderungsprofil für eine stationäre Einrichtung zur medizinischen Rehabilitation mit 100 Rehabilitationsplätzen und Zulassung zum AHB-Verfahren, Dezernat 8023, Zusammenarbeit mit Reha-Einrichtungen, Medizin/Psychologie, Abteilung Rehabilitation, Deutsche Rentenversicherung Bund. http://www.deutsche-rentenversicherung.de/BraunschweigHannover/de/Inhalt/2_Rente_Reha/02_Reha/05_Fachinformationen/03_Infos_Reha_Einrichtungen/profil_zulassung_ahb_I.pdf.pdf?__blob=publicationFile&v=3. Accessed 11 Feb 2020.
Deutsche Gesetzliche Unfallversicherung und Sozialversicherung für Landwirtschaft, Forst und Gartenbau (Hrsg.). (01. Juli 2016). Berufsgenossenschaftliche Stationäre Weiterbehandlung (BGSW). Anforderungen. http://www.dguv.de/medien/landesverbaende/de/med_reha/documents/bgsw2.pdf. Accessed 11 Feb 2020.
ECJ. (12/18/2014, case C-354/13). ECLI:EU:C:2014:2463, http://curia.europa.eu/juris/document/document.jsf?docid=160935&doclang=EN. Accessed 14 Dec 2019.
Faller, H., & Vogel, H. (2008). FEZ. In Diagnostische Verfahren in der Rehabilitation: Bd. 5. Diagnostik für Klinik und Praxis (S. 87–89). Göttingen: Hogrefe.
Fiedler, R. G., Ranft, A., Greitemann, B., & Heuft, G. (2008). DIAMO. In: Diagnostische Verfahren in der Rehabilitation: Bd. 5. Diagnostik für Klinik und Praxis (S. 364–367). Göttingen: Hogrefe.
Finger, M., & Escorpizo, R. (2016a). Work Rehabilitation Questionnaire Self-Report, ICF Research Branch. Swiss Paraplegic Research. http://www.myworq.org/quest/nrs/WORQ_SR_NR_German.pdf. Accessed 11 Febr 2020.
Finger, M., & Escorpizo, R. (2016b). Work Rehabilitation Questionnaire Self-Report. Brief. Swiss Paraplegic Research. http://www.myworq.com/quest/nrs/WORQ-Brief_SR_NR_German.pdf. Accessed 11 Febr 2020.
Finger, M. E., Bie, R. de, Nowak, D., & Escorpizo, R. (2015). Development and testing of an ICF-based questionnaire to evaluate functioning in vocational rehabilitation: The Work Rehabilitation Questionnaire (WORQ). Chapter 23. In: R. Escorpizo, S. Brage, D. Homa & G. Stucki (Hrsg.), Handbook of vocational rehabilitation and disability evaluation. Application and implementation of the ICF: Handbooks in health, work, and disability (S. 495–520). Cham: Springer.
Finger, M. E., Escorpizo, R., Bostan, C., & Bie, R. D. (2013). Work rehabilitation questionnaire (WORQ): Development and preliminary psychometric evidence of an ICF-based questionnaire for vocational rehabilitation. Journal of Occupational Rehabilitation, 24, 498–510.
Glassel, A., Rauch, A., Selb, M., Emmenegger, K., Luckenkemper, M., & Escorpizo, R. (2012). A Case Study on the Application of International Classification of Functioning, Disability and Health (ICF)-based tools for vocational rehabilitation in spinal cord injury. Work (Reading, Mass.), 41(4), 465–474.
Grawetter, F., & Wallnau, L. (2009). Statistics for the behavioral sciences. Belmont: Wardsworth.
Hartz, P., & Petzold, H. G. (2014). Das Gesundheitscoaching. In P. Hartz & H. G. Petzold (Hrsg.) Wege aus der Arbeitslosigkeit. MINIPRENEURE; Chancen um das Leben neu zu gestalten – zur Bewältigung von Langzeitarbeitslosigkeit. Integrative Modelle in Psychotherapie, Supervision und Beratung (Aufl. 2014). Wiesbaden: Springer VS.
Klein, C. (2015). Psychosoziales Gesundheitsmanagement für Führungskräfte. Igel Verlag RWS.
Maschke, M. (2008). Vergleich der Definitionen in europäischen Behindertenpolitiken. In K.-S. Rehberg & D. Giesecke (Hrsg.), Die Natur der Gesellschaft. Verhandlungen des 33. Kongresses der Deutschen Gesellschaft für Soziologie in Kassel 2006: Bd. 33. Verhandlungen des … Kongresses der Deutschen Gesellschaft für Soziologie (S. 5773–5784). Frankfurt/Main: Campus.
Myers, D.G. (2014). Psychologie. Berlin, Heidelberg: Springer.
Neuntes Buch Sozialgesetzbuch - Rehabilitation und Teilhabe behinderter Menschen -. SGB IX. (Bundesgesetzblatt i. d. F. vom 2001 BGBl. l, S. 1046, 1047; zul. geä. am 2016 BGBl. l, S. 1824, 1837). In Bundesgesetzblatt (§ 2). https://dejure.org/gesetze/SGB_IX/2.html. Accessed 11 Feb 2020.
Nübling, R., Hafen, K., Kriz, D., Herwig, J., Töns, N., & Bengel, J. (2008). PAREMO. In: Diagnostische Verfahren in der Rehabilitation: Bd. 5. Diagnostik für Klinik und Praxis (S. 101–104). Göttingen: Hogrefe.
Nübling, R., & Scholz, H. (2008). FPTM. In: Diagnostische Verfahren in der Rehabilitation: Bd. 5. Diagnostik für Klinik und Praxis (S. 93–97). Göttingen: Hogrefe.
Rauch, A., Lückenkemper, M., & Cieza, A. (2012). Einführung in die Internationale Klassifikation der Funktionsfähigkeit, Behinderung und Gesundheit. In: J. Bickenbach (Hrsg.), Die ICF-Core-Sets. Manual für die klinische Anwendung. Programmbereich Gesundheit (1. Aufl., S. 8–20). Bern: Huber.
Reha-Info. (1/2016). Die Rehabilitation, 55, 1–8. Reha-Info zur Zeitschrift Die Rehabilitation. https://www.bar-frankfurt.de/service/reha-info/reha-info-archiv/reha-info-2016/reha-info-012016/editorial.html. Accessed 14 Dec 2019.
Schneider, W., Basler, H.-D., & Beidenherz, B. (2008). FMP. In: Diagnostische Verfahren in der Rehabilitation: Bd. 5. Diagnostik für Klinik und Praxis (S. 90–92). Göttingen: Hogrefe.
Schubert, Michael, Penstorf, Carola, Seel, H., Morfeld, M., Bade, S., Gleisberg, D., Jonßen, L. et al. (Bundesarbeitsgemeinschaft für Rehabilitation e. V. (BAR), (Hrsg.). (2014). Abschlussbericht zum Projekt „Prüfung von aktuellem Stand und Potential der Bedarfsermittlung von Leistungen zur Teilhabe am Arbeitsleben unter Berücksichtigung der ICF (Machbarkeitsstudie)“. http://www.bar-frankfurt.de/fileadmin/dateiliste/Startseite/Abschlussbericht_end_x.pdf. Accessed 14 Dec 2019.
Schuh-Hofer, S., Schäfer-Voß, S., & Treede, R. D. (2016). Schlaf und Schmerz. Aktuelle Neurologie, 43, 249–255.
Simmel, S., Beickert, R., & Bühren, V. (2014). Traumarehabilitation der Deutschen Gesetzlichen Unfallversicherung. Besondere Heilverfahren in den BG-Unfallkliniken. Deutscher Ärzte-Verlag, 11(3), 524–529. Trauma rehabilitation of the German Social Accident Insurance Special rehabilitation measures in the BG-trauma centers.
SGB. (2001). Sozialgesetzbuch (SGB) Neuntes Buch (IX) - Rehabilitation und Teilhabe behinderter Menschen -. SGB IX. http://www.gesetze-im-internet.de/sgb_9_2018/. Accessed 14 Dec 2019.
Statistisches Bundesamt. (2015, Tabelle Zeitreihe aktualisiert in 2021). Gesundheit 2014. Diagnosedaten der Patienten und Patientinnen in Vorsorge- oder Rehabilitationseinrichtungen. Fachserie 12, Reihe 6.2.2. Wiesbaden. https://www.destatis.de/DE/Publikationen/Thematisch/Gesundheit/VorsorgeRehabilitation/DiagnosedatenVorsorgeReha2120622147004.pdf?__blob=publicationFile. Accessed 11 Feb 2020.
Statistisches Bundesamt. (2016a). Gesundheitsausgaben. Gesundheitsausgaben im Jahr 2014 bei 328 Milliarden Euro. https://www.destatis.de/DE/ZahlenFakten/GesellschaftStaat/Gesundheit/Gesundheitsausgaben/Gesundheitsausgaben.html. Accessed 11 Feb 2020.
Statistisches Bundesamt. (2016b). Gesundheitsausgaben im Jahr 2014 bei 328 Milliarden Euro. Wiesbaden. https://www.destatis.de/DE/PresseService/Presse/Pressemitteilungen/2016/03/PD16_080_23611.html. Accessed 11 Feb 2020.
Statistisches Bundesamt. (2016c). 19,2 Millionen Patienten 2015 stationär im Krankenhaus behandelt. Wiesbaden (283/16).
Statistisches Bundesamt. (2016d). 7,6 Millionen schwerbehinderte Menschen leben in Deutschland. 381/16. Wiesbaden. https://www.destatis.de/DE/PresseService/Presse/Pressemitteilungen/2016/10/PD16_381_227pdf.pdf;jsessionid=8DFE1237C00E438B6519D785FD49F478.cae2?__blob=publicationFile. Accessed 11 Feb 2020.
Statistisches Bundesamt. (2017a). Gesundheitsausgaben. Gesundheitsausgaben im Jahr 2015 um 4,5% gestiegen. https://www.destatis.de/DE/ZahlenFakten/GesellschaftStaat/Gesundheit/Gesundheitsausgaben/Gesundheitsausgaben.html. Accessed 11 Feb 2020.
Statistisches Bundesamt. (2017b). März 2017: Erwerbstätigkeit mit stabilem Aufwärtstrend. https://www.destatis.de/DE/PresseService/Presse/Pressemitteilungen/2017/05/PD17_145_132.html;jsessionid=86760E79C3C32B6C6606403BEC358AB4.cae3. Accessed 11 Feb 2020.
Statistisches Bundesamt. (2020). Gesundheitsausgaben im Jahr 2018 um 4% gestiegen. https://www.destatis.de/DE/Presse/Pressemitteilungen/2020/05/PD20_164_23611.html. Accessed 22 Apr 2020.
Stucki, G. (2012). Vorwort. In J. Bickenbach (Hrsg.), Die ICF-Core-Sets. Manual für die klinische Anwendung: Programmbereich Gesundheit (1. Aufl., S. 1–3). Bern: Huber.
Veith-Tezeren, C. (2017a). Überprüfung des ICF-basierten WORQ Fragebogens in der Bundesrepublik Deutschland und Evaluation in der beruflichen Rehabilitation. Masterthesis 2018 at FOM Hochschule GmbH, Essen.
Veith-Tezeren, C., Dittrich, W. H., Escorpizo, R. et al. (2017b). Work Rehabilitation Questionnaire Self-Report (WORQ - German-Germany version). http://myworq.org/quest/nrs/WORQ_SR_NR_German_Germany.pdf. Accessed 11 Febr 2020.
Veith-Tezeren, C., Dittrich, W. H., Escorpizo, R., et al. (2017c). Work Rehabilitation Questionnaire Short-Self-Report (WORQ - German-Germany version). http://myworq.org/quest/nrs/WORQ-Brief_SR_NR_German_Germany.pdf. Accessed 11 Febr 2020.
Vreeman, D. J., & Richoz, C. (2015). Possibilities and implications of using the ICF and other vocabulary standards in electronic health records. Physiotherapy Research International: The Journal for Researchers and Clinicians in Physical Therapy, 20, 210–219.
World Health Organization. (2001). International classification of functioning, disability and health: ICF. Geneva: World Health Organization.
World Health Organization. (2011). World report on disability. Geneva: World Health Organization.
Zumbeck, C. (2017). Mit 5 Schritten besser eingliedern. Für ein gutes Betriebliches Eingliederungsmanagement sind Ressourcen wie Wissen, Geld und Zeit nötig. Auch bessere externe Netzwerke und Beratung können die Umsetzung puschen. BEM-PRAXIS. Gute Arbeit (3), 14–16.
Zwerenz, R. (2008). FBTM. In Diagnostische Verfahren in der Rehabilitation: Bd. 5. Diagnostik für Klinik und Praxis (S. 84–86). Hogrefe.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2021 The Author(s), under exclusive license to Springer Fachmedien Wiesbaden GmbH, part of Springer Nature
About this chapter

Cite this chapter
Veith-Tezeren, C., Dittrich, W.H. (2021). Adaptation of an ICF-Based Questionnaire for Vocational Rehabilitation in Germany. In: Johansen, T., H. Dittrich, W. (eds) Occupational Health and Rehabilitation. FOM-Edition(). Springer Gabler, Wiesbaden. https://doi.org/10.1007/978-3-658-33484-0_5
Download citation
DOI: https://doi.org/10.1007/978-3-658-33484-0_5
Published:
Publisher Name: Springer Gabler, Wiesbaden
Print ISBN: 978-3-658-33483-3
Online ISBN: 978-3-658-33484-0
eBook Packages: Business and ManagementBusiness and Management (R0)