
Abstract
The great saphenous vein is by far the most frequently examined and treated vein of all the superficial veins. Furthermore, the majority of venous studies are performed on the great saphenous vein. Duplex ultrasound makes it possible to assess the vein very accurately before and after intervention.
Assessing the great saphenous vein with duplex ultrasound is a relatively new concept with some surgeons still performing surgery without considering the need of a preoperative scan. The first international consensus document appeared in 2006 (Coleridge-Smith et al., Eur J Vasc Endovasc Surg 31:1–10, 2006) with the object of producing a standard ultrasound protocol which would encourage consistency between treatments, doctors and hospitals. This development was welcomed as it was a first step towards standardisation. Since then there have been several recommendations from various international societies in an attempt to improve the examination of the great saphenous vein and the rest of the superficial venous network.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others



Keywords
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
FormalPara Chapter SummaryThe great saphenous vein is by far the most frequently examined and treated vein of all the superficial veins. Furthermore, the majority of venous studies are performed on the great saphenous vein. Duplex ultrasound makes it possible to assess the vein very accurately before and after intervention.
Assessing the great saphenous vein with duplex ultrasound is a relatively new concept with some surgeons still performing surgery without considering the need of a preoperative scan. The first international consensus document appeared in 2006 (Coleridge-Smith et al. 2006) with the object of producing a standard ultrasound protocol which would encourage consistency between treatments, doctors and hospitals. This development was welcomed as it was a first step towards standardisation. Since then there have been several recommendations from various international societies in an attempt to improve the examination of the great saphenous vein and the rest of the superficial venous network.
7.1 Examination Procedure
Every examiner should establish an examination procedure which develops into a well-oiled routine. In this way the entire great saphenous vein can be covered including its tributaries and perforating veins so there is less chance of any vein segments being overlooked.
A good place to begin is in the groin with the subject standing. Here the anatomy of the saphenofemoral junction and its tributaries can be examined in B scan. The competency of the veins in this region should be tested with the Valsalva manoeuvre and at least one other provocation manoeuvre. Duplex mode should be used for this and it is advisable to use colour duplex.
The whole course of the great saphenous vein down the leg should be viewed once in B scan to detect any sudden calibre changes and dilated perforating veins or tributaries. Special attention must be paid to the region of the perforating veins of the adductor canal (formerly Dodd and Hunter) and the paratibial perforating veins (formerly Boyd), as well as the junctions with the anterior and posterior arch veins below the knee. Duplex mode must be switched on repeatedly when running over the course of the great saphenous vein. It is more effective to use PW than colour mode for this because changes in the velocity profile are more obvious (Sect. 7.5.2). Tributaries and perforating veins are better assessed in colour on this first pass. However, they must not divert the examination from the saphenous trunk.
7.2 Objectives of the Examination
The following questions should be answered at the conclusion of the examination:
-
Is there reflux through the saphenofemoral junction?
-
Is the terminal valve competent?
-
Is the preterminal valve competent?
-
Are the superficial inguinal veins competent?
-
Is there any anomaly of the saphenofemoral junction?
-
Is an aneurysm present?
-
Is the great saphenous vein visible in the fascial compartment throughout its length?
-
Is the whole course of the vein interfascial?
-
What is its diameter at the standardised point 10 cm below the junction?
-
Are there any acute changes in saphenous calibre?
-
Is its course typical in relation to topographical anatomy?
-
Is its course more lateral than usual at the groin or thigh?
-
Is there a duplication present over part of its course?
-
Is there an aplastic or hypoplastic segment along its course?
-
Is there evidence of thrombosis or post-phlebitic changes?
-
Is there reflux in the great saphenous vein?
-
Is this reflux well or poorly drained?
-
How many saphenous segments are refluxive?
-
Where is the proximal reflux source?
-
Are any dilated tributaries or perforating veins apparent in the course of the great saphenous vein?
-
Are they involved in the recirculation circuit?
-
Does the reflux leave the great saphenous vein by a tributary or a perforating vein?
-
What is the Hach Class (in the areas it may be used)?
-
Which shunt type is present as defined in the CHIVA strategy?
-
How does the calibre and course of the great saphenous vein behave distal to the end of the reflux?
-
Are there any pathological soft tissue changes surrounding the great saphenous vein?
-
Is the flow in the dilated great saphenous vein antegrade, because it is serving as drainage path for obstructed deep veins (secondary varicose veins, Chap. 15)?
-
Has all or part of the saphenous vein been treated?
7.3 The Saphenofemoral Junction
In the groin the anterior (formerly medialis) and posterior (formerly lateralis) accessory saphenous veins unite with the great saphenous vein to join the common femoral vein. Since these veins will be mentioned very frequently in this chapter, the former nomenclature will be omitted. Likewise the confluence of the great saphenous vein will be referred to as the saphenofemoral junction (SFJ), as recommended in the consensus document (Coleridge-Smith et al. 2006). The region of the proximal great saphenous vein and the confluence of superficial inguinal veins (sometimes called the “crosse”) will be described as the saphenofemoral region.
The saphenofemoral junction is examined with the ultrasound probe lightly pressed against the groin of the standing subject (Fig. 7.1). The anatomy of the saphenofemoral region is examined first in B scan. Next, the effectiveness of the various provocation manoeuvres can be assessed in augmenting antegrade flow and inducing reflux in the superficial and deep veins (Sect. 6.11). Then, the saphenofemoral junction and the anatomy of the confluence of superficial inguinal veins are examined. Flow through the saphenofemoral junction, the superficial tributaries and the great saphenous vein is tested. Particular attention is made in the assessment of valve competence. The terminal valve controls the flow between the common femoral vein and the great saphenous vein and is present in 91 % of cases (Mühlberger et al. 2009). The preterminal valve affects the flow between the saphenofemoral junction, the superficial tributaries and the distal great saphenous vein.

Position of the probe during the examination of the great saphenous vein in a standing subject. 1 Examination of the saphenofemoral junction, 2 measurement of the saphenous vein diameter in the thigh
Copyright: [Author]
The superficial tributaries at the saphenofemoral junction (Sect. 2.4) have many anatomical variants which are important to evaluate using duplex ultrasound because this may influence the treatment approach (Fig. 7.2; see also Sect. 7.3.6). It is helpful during surgery if the surgeon knows how many tributaries are expected and how they connect. Occasionally it is difficult to define whether the surgically exposed vein is the junction of the anterior accessory saphenous vein with the great saphenous vein or the true junction of the great saphenous vein with the common femoral vein. This situation is easily avoided if the operator knows exactly how many tributaries join the great saphenous vein at the saphenofemoral junction and their distribution towards lateral and medial. Furthermore, the division of the epigastric and superficial circumflex iliac veins into two or three branches which join the anterior accessory saphenous vein can likewise make this junction look like the saphenofemoral junction, thus adding to the confusion (Fig. 7.2 C, D, I, L, M, O, P and Sect. 7.3.1).

Views of the different confluence variations of the great saphenous vein, its tributaries and the confluence of the superficial inguinal veins with the common femoral vein according to Lanz and Wachsmuth. 1 Falciform margin of the saphenous hiatus with 2 upper cornu and 3 lower cornu. 4 Deep inguinal lymph nodes. 5 Common femoral vein. 6 Common femoral artery. 7 Femoral branch of the genitofemoral nerve, 8 Cutaneous branch of the femoral nerve. 9 Great saphenous vein. 10 Anterior accessory saphenous vein. 11 Superficial circumflex iliac vein. 12 Superficial epigastric vein. 13 Superficial external pudendal vein. 14 Posterior accessory saphenous vein (legends for letters – see text) (From Platzer (2005); by kind permission of Thieme-Verlag)
Copyright: Thieme
The veins of the confluence of the superficial inguinal veins are:
-
Anterior accessory saphenous vein from distal and lateral (Sects. 7.3.7 and 10.4)
-
Superficial circumflex iliac vein from proximal and lateral (Sect. 7.3.5)
-
Superficial epigastric vein from proximal, confluence quite variable (Sect. 7.3.5)
-
Deep and superficial external pudendal veins from medial (Sect. 7.3.4)
-
Posterior accessory saphenous vein from distal and medial (Sect. 10.5)
Some of these veins may not be present. Many of them, especially the proximally arising superficial circumflex iliac and the superficial epigastric veins, have several sub-tributaries which may join to form a single vein at the saphenofemoral junction or enter the confluence of superficial inguinal veins separately. The same is true of the medially arising superficial and deep external pudendal veins which often join the common femoral or the posterior accessory saphenous vein directly. Furthermore, all or any of these veins may join one another before they enter the confluence of the superficial inguinal veins.
Lanz and Wachsmuth have systematised all the possible anatomical variations of the confluence (Fig. 7.2). They start with the confluence of all the superficial inguinal veins into the common femoral vein (A) and then describe the different variants for the confluence of the individual vessels: B–E for the anterior accessory saphenous vein; F–G for the posterior accessory saphenous vein; H–I for the superficial and deep external pudendal veins, respectively; J–N for the superficial epigastric vein; and O–R for the superficial circumflex iliac vein.
7.3.1 Normal Findings
The great saphenous vein joins the common femoral vein from the anteromedial aspect. As a rule a competent great saphenous vein is not very large, but it is always visible in B scan (Fig. 7.3). However, the calibres even of competent veins may differ widely. Some indication of normal vein size may be deduced from the subject’s body size and the diameter of the rest of his veins, for example, those visible on the back of the hand. On average, the diameter of the great saphenous vein in the saphenofemoral region in a healthy subject who has been standing for a few minutes is 7.5 mm (±1.8 mm), with a range of 3.5–11.0 mm (Mendoza et al. 2013). Fifteen centimetres below the saphenofemoral junction, it becomes smaller and more uniform in size. The great saphenous vein can be overlooked occasionally in a supine subject.



Normal findings of the saphenofemoral junction. (a) B scan in transverse view through the left groin of a thin subject standing. Note that the entire venous network, including the common femoral vein is no more than 2 cm below the surface (scale on the right). The saphenofemoral junction is outlined and seen clearer on the moving image (online material). (b) Colour duplex ultrasound of the same subject during muscular systole demonstrating antegrade flow in the common femoral vein and saphenofemoral junction. (c) B scan of the same subject 1 cm further down where the saphenofemoral junction has separated into a small calibre great saphenous vein and anterior accessory saphenous vein (AASV). (d) Transverse view through the right groin in a standing subject with small calibre veins. During muscular systole, the blue signal in all the superficial veins represents antegrade flow as they join into the saphenofemoral junction. In this subject the pudendal vein curves anteriorly into the back of the great saphenous vein. For this reason the direction of antegrade flow towards the confluence of superficial inguinal veins is towards the probe and therefore appears red. Investigating flow in muscular diastole is important for distinguishing between a normal finding and pathological reflux. If antegrade flow continues in the pudendal vein 1 s after the end of muscular systole, it is pathological. The mouth at the saphenofemoral junction is clearly visible (yellow arrows) (Art. common femoral artery). (e) Transverse view through the right groin with a common drainage of the great saphenous and anterior accessory saphenous veins into the saphenofemoral junction (SFJ). There is a separate drainage of the pudendal vein directly into the common femoral vein. The superficial external pudendal artery is visible crossing the saphenofemoral junction. This is a common finding (online material). (f) Transverse view through the right groin demonstrating a wide saphenofemoral junction in a big man. Despite its relatively large calibre, the junction was competent (SFA superficial femoral artery, DFA deep femoral artery, CFV common femoral vein). (g) Same position as in (f) with colour duplex in muscular systole and antegrade flow (blue). In diastole there was no reflux in the saphenous trunk or through the saphenofemoral junction
Copyright: [Author]
It is common to see the familiar image of a narrow calibre great saphenous vein terminating in a broad mouth at the saphenofemoral junction (Fig. 7.3d). Here the valve leaflets are frequently observed moving with changes in the blood flow (see also Figs. 7.6 and 7.7).
The anterior accessory saphenous vein joins the great saphenous vein from the side at an acute angle in the saphenofemoral region. In transverse view it is seen lateral to the great saphenous vein and vertically above the femoral vein (Fig. 7.3c–e). It is not always visible in B scan. A useful rule is if an imaginary line is drawn along a tangent to the medial edge of the common femoral vein, the great saphenous vein lies medial and the anterior accessory saphenous vein lies lateral (Fig. 7.4) (for anatomical variations, see also Sect. 7.3.2; for reflux in the anterior accessory saphenous vein Sect. 7.3.7; and for its anatomical course Sect. 10.4).

Normal relations of the great saphenous and anterior accessory saphenous veins. This is a transverse view through the left groin of a standing subject slightly below the saphenofemoral junction. The anterior accessory saphenous vein (AASV) lies vertically above the femoral vein and the great saphenous vein lies medially (“alignment” sign)
Copyright: [Author]
The superficial circumflex iliac vein may join either the great saphenous vein or the anterior accessory saphenous vein. It very rarely joins the common femoral vein directly. Using ultrasound it generally appears as a cranial extension of the great saphenous or the anterior accessory saphenous vein. Like the epigastric vein, it may consist of several branches which either unite or join the confluence separately. If one of these veins joins the anterior accessory saphenous vein from a cranial direction, then this junction may be mistaken for the saphenofemoral junction (Fig. 7.5). This mistaken identification is a source of error in surgery which may result in an inappropriate ligation (for reflux from these vessels, see also Sect. 7.3.5).

Diagram of a “pseudo” saphenofemoral junction formed by the confluence of a lateral superficial inguinal tributary like the superficial circumflex iliac vein (SCIV) or epigastric vein (EV) and the anterior accessory saphenous vein (AASV) with the great saphenous vein (GSV) (green circle). The true saphenofemoral junction lies deeper (red circle)
Copyright: [Author]
In B scan a valve cannot always be seen at the saphenofemoral junction. Although this is said to occur in up to 50 % of subjects, the use of more modern ultrasound machines has increased visualisation of the terminal valve to 91 %. In transverse view the valve leaflets can be seen moving during the various provocation manoeuvres (Fig. 7.6). In longitudinal view the valves can be seen in different positions. The terminal valve lies directly in the saphenofemoral region (Fig. 7.7a–c), and the preterminal valve lies below the confluence of superficial inguinal veins (Fig. 7.8), although the anterior accessory saphenous vein may also join distal to this valve. Valve movement can be detected in B scan. Rigid valve cusps indicate disease; however, flexible cusps do not exclude reflux. PW mode or colour duplex must be used to test for the presence of reflux.


Transverse image of the terminal valve at the saphenofemoral junction. (a) During muscular systole the valve leaflets are visible as white lines (arrow). (b) During muscular diastole the valve curves out towards the great saphenous vein when the junction is competent (muscular systole/diastole cycle on online material). (c) The valve (yellow arrows) opens during muscular systole causing movements in the mouth of the saphenofemoral junction (yellow contour). The anterior accessory saphenous vein (AASV) is also seen just before it terminates into the great saphenous vein (GSV). (d) Same groin in muscular diastole where the returning blood tries to re-enter the great saphenous vein. Here the valve leaflets (arrowed) are seen closing back towards the great saphenous vein. (e) Transverse view through the right groin this time with complete incompetence of the great saphenous vein. During muscular systole the valve cusps point towards the deep vein. (f) During muscular diastole in (e), the valves close back towards the great saphenous vein. It is impossible to establish whether reflux exists from the behaviour of the valves in a static B scan alone. In the film (online material), it is more obvious from the movement of the visualised blood that this valve is incompetent
Copyright: [Author]

Longitudinal view through the saphenofemoral junction demonstrating a competent terminal valve. (a) Longitudinal view during a Valsalva manoeuvre causes the valve (arrowed) to curve out into the great saphenous vein (GSV). The epigastric vein is seen in the left of the image (1). (b) A valve leaflet is seen opening during muscular systole. (c) Same subject as in (b) demonstrating a closed valve leaflet curving into the great saphenous vein during a Valsalva manoeuvre (image of a rigid, inflexible valve is seen in Fig. 7.15)
Copyright: [Author]

Longitudinal view through the great saphenous vein immediately below the saphenofemoral junction demonstrating the preterminal valve. (a) Both valve cusps are visible with the classical “swallow’s nest” shape. The valve is seen at rest in the standing subject. (b) The leaflet furthest from the surface is very clearly visible at rest. (c) The valve closes in muscular diastole
Copyright: [Author]
7.3.2 Anatomical Variations of the Saphenofemoral Junction
There are numerous anatomical variations at the saphenofemoral junction. For example, any or all of the superficial inguinal veins may join the common femoral vein directly. Direct drainage occurs frequently with the pudendal vein (Fig. 7.9). If this vein is overlooked during surgery, then it may be the source of a recurrence.

Drainage of the pudendal vein directly into the common femoral vein. (a) Transverse view through the right groin. (b) Same position showing antegrade flow during muscular systole. (c) Transverse view through the left groin. The common femoral artery is circled (red). CFV common femoral vein, GSV great saphenous vein (online material). (d) Transverse view approx. 1 cm further distal. The great saphenous vein is visible as an independent vessel. The drainage of a very large pudendal vein is seen entering the common femoral vein directly (online material). (e) Same position with colour duplex with the probe tilted slightly so that both veins are visible in one image. At the end of muscular systole, there is a short flow reversal in the great saphenous vein (small red signal) until valve closure. However, long-lasting flow is now apparent in the pudendal vein. It is blue because the blood is refluxing away from the probe and pathological because the flow is prolonged and the pudendal vein is very dilated in comparison to the great saphenous vein (online material)
Copyright: [Author]
Duplication of the great saphenous vein at the saphenofemoral junction is very rare, even though this is postulated repeatedly as a cause of recurrence. According to Caggiati (personal communication), this variant does not occur. The great saphenous vein may join the common femoral vein directly at the groin or a few centimetres in either direction. Information on the level of the saphenofemoral junction is helpful to the surgeon but not as important as determining the level of the sapheno-popliteal junction.
In the majority of cases, the anterior accessory saphenous vein terminates in the region of the saphenofemoral junction where it joins the great saphenous vein (Fig. 7.3). Sometimes it may join up to 5 cm further down. It occasionally joins the femoral vein directly immediately adjacent to the great saphenous vein (Fig. 7.10). Very rarely it may join the common femoral vein by passing between the superficial femoral artery and the deep femoral artery (Fig. 7.11). It is equally rare to find a duplication of the anterior accessory saphenous vein in the saphenofemoral region (Fig. 7.12). If these anatomical variations of the anterior accessory saphenous vein are missed preoperatively, they may provide a source of recurrence.

Independent drainage of the anterior accessory saphenous vein (AASV) into the common femoral vein (CFV) (online material). (a) Transverse view through the left groin in a standing subject during muscular systole. There is antegrade flow up the anterior accessory saphenous vein and into the common femoral vein. (b) Transverse view 1 cm further distal from (a) demonstrating the great saphenous vein joining the common femoral vein. The anterior accessory saphenous vein is visible as an independent vessel lateral to the saphenofemoral junction
Copyright: [Author]

Confluence of the anterior accessory saphenous vein (AASV) between the superficial and deep femoral arteries. (a) Diagram of the position of the arteries in relation to the confluence. (b) Measurement in the common femoral vein which is the reflux source. (c) Measurement in the confluence of the anterior accessory saphenous vein which is clearly refluxive. (d, e) Velocity profiles in the two adjacent arteries
Copyright: [Author]

Saphenofemoral junction. Transverse view through the left groin in a standing patient with an incompetent terminal valve and a dilated great saphenous vein (GSV) which turns left at the top of the image. Two competent anterior accessory saphenous veins (AASV) are seen draining separately into the saphenofemoral junction. (a) Region of the drainage points of both anterior accessory saphenous veins. (b) 1 cm further distal
Copyright: [Author]
In most cases the posterior accessory saphenous vein will not form part of the confluence of superficial inguinal veins but will meet the great saphenous vein in the upper thigh.
The tributaries join medially (pudendal vein and much further distal the posterior accessory saphenous vein) and laterally (epigastric and superficial circumflex iliac from cranial, anterior accessory saphenous vein from caudal). Hildebrandt’s diagram provides a simplified classification supplemented by additional information from Mühlberger (Fig. 7.13). Only the pudendal vein drains medially at the saphenofemoral region (Fig. 7.13a). There are laterally joining veins from cranial (epigastric and superficial circumflex iliac veins) and caudal (anterior accessory saphenous vein), which may join above the distal edge of the ostium (dotted line in Fig. 7.13a and fainter in the other images) or below this point. The level at which the anterior accessory saphenous vein joins may be important for positioning the fibre in endoluminal laser treatment. Furthermore, the presence and location of the terminal and preterminal valves should be defined if selective ablation techniques are performed. Some of the anatomical variations are given in Fig. 7.13.


Junctional variations and valves for common or separate inflow from the proximal and lateral tributaries. (a) Standard saphenofemoral junction with tributaries. The pudendal vein is the single medial segment which joins between the terminal and preterminal valves. The lateral segment is shown with a common confluence of a cranial and caudal branch and another valve at the level of its junction with the great saphenous vein. The typical position of a lymph node (LN) lateral to the great saphenous vein is shown. The perpendicular dotted line marks the caudal edge of the ostium. (b) Additional information defining the lateral segment (light green/light purple) and the medial segment (light brown). The lateral segment is divided into cranial (green) and caudal (light purple) parts. (c) Transverse view of the lateral segment distal to the terminal valve (TV). An imaginary dotted line drawn around the front wall of the common femoral vein and passing through the confluence of the great saphenous vein will give the exact point where the great saphenous vein enters the femoral vein. This is known as the fossa ovalis or ostium. (d) Longitudinal view demonstrating the confluence of the lateral cranial segment also distal to the terminal valve. (e) Absent terminal valve. (f) Confluence of the lateral segment consisting of the superficial epigastric, circumflex iliac and anterior accessory saphenous veins. Note that here they are proximal to the terminal valve. (g) In this image the confluence of the lateral and medial segment are both proximal to the terminal valve. (h) All of the superficial inguinal tributaries join between the terminal and the preterminal valves. (i) The lateral cranial tributaries may join separately from one another or together as in this illustration between the terminal and preterminal valves. The anterior accessory saphenous vein is not present. (j) Isolated entry of the superficial epigastric vein (cranial lateral segment). (k) The anterior accessory saphenous vein enters just distal to the preterminal valve (CFA common femoral artery, LN lymph node, TV terminal valve, CIV circumflex iliac vein, SEV superficial epigastric vein, PV pudendal vein, AASV anterior accessory saphenous vein, GSV great saphenous vein) (Drawings Dr. Andreas Hildebrandt, Berlin; by kind permission)
Copyright: Dr. A. Hildebrandt, Berlin
Precise documentation of the saphenofemoral junction should include all the superficial inguinal veins and their relationship and distance from the terminal and preterminal valves. Such information is needed principally for study purposes, but in the context of new treatments which selectively preserve tributaries, pre-procedural documentation may become important.
7.3.3 Reflux from the Common Femoral Vein
The most common source of reflux in the great saphenous vein is the saphenofemoral junction. Here the saphenous trunk is filled refluxively from the common femoral vein. During the Valsalva manoeuvre or muscular diastole, blood flows down from the iliofemoral veins into the great saphenous vein. This can be seen indirectly in B scan from the behaviour of the valves and the dilation of the vein wall during refluxive flow.
The mouth of the great saphenous vein generally appears dilated in B scan (Fig. 7.14). The calibre of the great saphenous vein often increases after the subject has been standing for a few minutes. However, reflux may also occur across the saphenofemoral junction even if the vein is not dilated.

Incompetent saphenofemoral junction of the left leg in B scan. The diameter of the great saphenous vein (GSV) is grossly dilated (c.f. Fig. 7.3) (A common femoral artery, VFC common femoral vein)
Copyright: [Author]
Much information can be gained in B scan:
-
The morphology of the saphenofemoral junction and the proximal great saphenous vein
-
The morphology of the confluence of superficial inguinal veins
-
The presence or absence of thrombus in the common femoral or great saphenous veins (compression manoeuvre, Chaps. 11 and 14)
-
Morphology of the valves
-
Drainage paths of the insonated veins
7.3.3.1 Morphology of the Saphenofemoral Junction and the Confluence of the Superficial Inguinal Veins
The following questions should be answered:
-
Do the superficial inguinal veins join the femoral vein directly or via the great saphenous vein?
-
Which superficial inguinal tributaries are present?
-
Is the saphenofemoral junction dilated?
-
Is there an aneurysm?
Aneurysms of the saphenofemoral region should be identified because of the potential difficulty in surgical treatment. They may be either discrete or fusiform dilatations of the great saphenous vein itself (Fig. 7.15) or dilatations growing out of the vein wall (Fig. 7.16). Surgery on the saphenofemoral junction may be complicated by these thin-walled balloons of blood. They may grow as large as a golf ball and obscure the operating field. Tributaries often flow directly into these aneurysms (Fig. 7.17).

Aneurysm at the confluence of the great saphenous vein and the anterior accessory saphenous vein (AAVS) with incompetence of the terminal valve and a competent preterminal valve (complete, Hach Class I). (a) Transverse view through the left groin demonstrating the saphenofemoral junction (SFJ) during muscular diastole. Blood refluxes from the common femoral vein through the incompetent terminal valve into the great saphenous vein and directly into the laterally positioned anterior accessory saphenous vein. Turbulence can be observed in the aneurysm (white arrows). Although this is during diastole and there is reflux, the valve cusp point towards each other They are not curved back into the great saphenous vein as would be expected with reflux but are rigid (blue arrows) (CFV common femoral vein). (b) Same position after the end of diastole. The erythrocyte sludge has gone, and the valve cusps remain rigid in the same position as during diastole. The narrow lumen between the rigid valve cusps caused a jet-effect which may have led to the development of the aneurysm (online material)
Copyright: [Author]

Aneurysm formed by a bulge in the side wall of the vein. (a) Transverse view through the right groin with an incompetent saphenofemoral junction. The aneurysm looks like a mushroom growing out of the great saphenous vein (GSV). (b) 1 cm further distal the aneurysm (AN) and the great saphenous vein look like two different vessels
Copyright: [Author]

Side aneurysm of the great saphenous vein (GSV) at the saphenofemoral junction. (a) Transverse view through the left groin in B scan. The anterior accessory saphenous vein (AASV) is seen draining into the aneurysm. The superficial external pudendal artery crosses between the aneurysm and the great saphenous vein (online material). (b) Intraoperative photograph of the aneurysm exposed showing its connections with the pudendal (#) and epigastric (+) veins. The forceps are pointing to the normal calibre great saphenous vein just below the band-like superficial external pudendal artery (** anterior accessory saphenous vein)
Copyright: [Author]
Turbulence is normally observed in aneurysms in B scan during provocation manoeuvres. A thrombus in the lumen of an aneurysm is rare (Pascarella et al. 2005). Surprisingly, in contrast to the arterial circulation, there is no relationship between the presence of an aneurysm and the development of a superficial vein thrombosis (Kalodiki et al. 2012). A combination of a weak vein wall and an overload of refluxive blood volume striking the vein wall may encourage aneurysm formation. The resulting flow characteristics seem to prevent thrombus formation.
Even with incompetence the terminal valve is usually seen fluttering. It folds into the great saphenous vein during muscular diastole if reflux is present, or during a Valsalva manoeuvre. If the valve is rigid and immobile, this may suggest a primary valve defect or post-thrombotic scarring (Fig. 7.15).
If the system is poorly drained (Sect. 3.2.3), echoes appear in B scan inside the great saphenous vein immediately after a provocation manoeuvre. These may make the vein appear homogeneous with a similar echogenicity as the surrounding tissue. This depends on the accumulation of erythrocytes and the formation of so-called erythrocyte sludge. If the vein appears heterogeneous, this may indicate turbulence and varying flow velocities (Fig. 7.15). Patients presenting with this turbulence may go on to develop an aneurysm at the saphenofemoral region.
The direction of blood flow can be seen in B scan from the erythrocyte sludge. However, reflux can be seen much more clearly using colour duplex ultrasound. This allows us to answer the following questions:
-
Does the reflux flow from the common femoral vein through the saphenofemoral junction into the superficial veins?
-
Does it fill the great saphenous vein, anterior accessory saphenous vein or both refluxively?
-
Is any other superficial inguinal tributary also refluxive?
-
Is isolated reflux present in a named superficial inguinal tributary?
Reflux from the common femoral vein through the saphenofemoral junction via an incompetent terminal valve is measurable at the saphenofemoral region (Fig. 7.18). This is termed complete incompetence of the great saphenous vein. This finding must be distinguished from the tributary type incomplete incompetence. In this situation the reflux arises from the deep leg veins via an incompetent superficial inguinal tributary. The terminal valve remains competent (Sects. 7.3.4 and 7.3.5).

Incompetent saphenofemoral junction in colour duplex in the patient from Fig. 7.13a). (a) Transverse view through the groin during muscular diastole demonstrating reflux from the common femoral vein (CFV). The blood flows from the deep vein towards the probe (red). Note that the common femoral vein and saphenofemoral junction are both coloured red. (b) Longitudinal view through the junction in the same patient during muscular systole. The blood flow is antegrade in both the deep and superficial veins. (c) Same longitudinal position at the very beginning of muscular diastole. The blood starts to change direction and flows out of the common femoral vein. (d) During muscular diastole the blood flows out of the common femoral vein and into the great saphenous vein. Only with this unequivocal finding is it correct to speak of incompetence of the saphenofemoral junction
Copyright: [Author]
In addition to the reflux from the common femoral vein, it is not uncommon to find a tributary (usually the pudendal vein) which is also refluxive or at least dilated (Fig. 7.19). Antegrade flow will be found in both these veins during muscular systole. The course of the pudendal vein to its termination in the saphenofemoral region may show red representing flow towards the probe. In diastole it is important to clarify whether flow can be observed from the deep vein into the great saphenous vein (red) and whether the pudendal vein presents a long-lasting flow. The colour red or blue depends on the course of the pudendal vein towards the probe. However, it is pathological if this flow is prolonged in diastole. Here it may fill the great saphenous vein refluxively or drain into the common femoral vein through the saphenofemoral junction (Sect. 7.3.6).

Incompetent saphenofemoral junction with a refluxive pudendal vein (online material). (a) Transverse view through the left groin during muscular systole demonstrating antegrade flow in both veins (great saphenous and pudendal). In the pudendal vein antegrade flow towards the probe (red), flow is only visible at the confluence with the great saphenous vein (GSV). (b) At the beginning of muscular diastole, there is clear reflux from the common femoral vein through the saphenofemoral junction. The reflux from the pudendal vein cannot be evaluated at this early timepoint. (c) Towards the end of muscular diastole, it becomes clear that in addition to reflux from the common femoral vein (CFV), the great saphenous vein is also filled refluxively by the pudendal vein
Copyright: [Author]
Sometimes the findings at the saphenofemoral junction are contradictory. It may be competent during the Valsalva manoeuvre and incompetent with another provocation manoeuvre, or vice versa. Occasionally it is incompetent and then competent consecutively using the same manoeuvre twice. When this happens the veins are not usually very dilated. The contradiction may result from the different intensities of the manoeuvres. The calf compression applied or the effort in raising the toes may not have been the same both times. The frequency of the challenge test is also important because this affects the volume of blood which collects in the leg prior to the subsequent manoeuvre. Poorly drained systems may likewise give contradictory results (Sect. 3.2.3). In the latter case, an elevation-dependency manoeuvre may clarify what is happening (Sect. 6.9). As the patient stands up from a period of leg elevation, a long-lasting reflux will be observed in the vein if it is pathological (Lattimer et al. 2013). Competent valves may be found in the common femoral vein which may result in a negative Valsalva reflux but a positive reflux following a calf compression or contraction manoeuvre (Lattimer et al. 2012b). If the contradiction cannot be resolved, then the subject must be called in again for more testing. However, this problem only arises in borderline cases of pathology and in the early stages of incompetence where treatment is rarely required.
The deep femoral vein joins the femoral vein from posterior in the proximal thigh to form the common femoral vein. Normally this confluence cannot be seen during the examination of the saphenofemoral junction. The deep femoral vein may join at an acute angle in which case it will be the same colour (blue) on duplex as the femoral vein. Sometimes a red jet can be seen entering the common femoral vein from posterior (Fig. 7.20a, b). This means that the deep femoral vein joins at right angles. This finding is not pathological.

Confluence of the deep femoral vein in the groin. (a) Transverse view of the left groin showing the common femoral (CFV), deep femoral (DFV) and great saphenous veins (GSV). The deep femoral vein joins below the saphenofemoral junction. Therefore, the great saphenous vein appears separate from the common femoral vein (online material). (b) Longitudinal view in the same subject. (c) Transverse view of the right groin showing the common femoral, deep femoral and great saphenous veins. The deep femoral vein joins immediately opposite the great saphenous vein. It looks as if the deep femoral vein fills the great saphenous vein refluxively (red) because the flow is towards the probe. (d) Longitudinal view in the same subject. The saphenofemoral junction is indicated opposite the confluence of the deep femoral vein (blue arrows)
Copyright: [Author]
A special situation occurs when there is reflux arising from the deep femoral vein which flows directly into the great saphenous vein (Fig. 7.20c, d). In rare cases the deep femoral vein joins immediately opposite the saphenofemoral junction. It meets the femoral vein from behind and its blood flows anteriorly to enter directly into the great saphenous vein. Simple interruption of the saphenofemoral junction in patients with this configuration leads to an improvement in their varicose veins. A cause may be postulated that a systolic jet from the deep femoral vein during activity strikes the valve of the great saphenous vein with enough force to cause damage. After endoluminal procedures that close the great saphenous vein without ligation of the tributaries, recurrence may occur in this unusual configuration because of the relentless jet from the deep femoral vein.
With constant reflux from the common femoral vein into a very dilated pudendal vein, this may result in cross-pelvic communications and shunting (Spontaneous Palma shunt, Chap. 15).
7.3.4 Reflux from the Pudendal Vein
The pudendal vein joins the saphenofemoral junction from the medial side. It may join the great saphenous vein, the saphenofemoral junction or directly into the femoral vein (Fig. 7.9). Occasionally it joins the great saphenous vein from a posterior direction. These variants are helpful to the surgeon. Reflux arising from the pudendal vein when it joins the saphenofemoral junction and takes it to the great saphenous vein can easily be confused with reflux arising from the common femoral vein directly (Fig. 7.21). Colour duplex is better than PW mode for distinguishing these conditions. The pudendal vein may also be described as the medial segment.

Transverse view through the left groin. (a) Velocity profiles in the great saphenous vein just below the saphenofemoral junction demonstrating antegrade flow during systole and retrograde flow after relaxation of the toes (**). (b) During muscular systole antegrade flow is seen in the great saphenous vein with inflow from the pudendal vein (arrowed). (c) During muscular diastole there is no reflux from the common femoral vein. The only reflux present is from the pudendal vein into the great saphenous vein. (d) Flow from the confluence of superficial inguinal veins “at rest”. The subject is standing without moving. Note the constant flow from the pudendal vein. (e) Another image showing a permanent flow (reflux) from the pudendal vein at rest (reflux from the pudendal and epigastric veins on online material)
Copyright: [Author]
7.3.5 Reflux from the Epigastric and Superficial Circumflex Iliac Veins
The epigastric and superficial circumflex iliac veins may also account for incompetence of the great saphenous vein. This is possible in addition to reflux from the saphenofemoral junction (incompetent terminal valve) or independent of it (with competent terminal valve). The two together are also known as the cranial section of the lateral segment (Fig. 7.13).
Both the epigastric and the superficial circumflex iliac veins may also join the anterior accessory saphenous vein first and deliver their reflux either only distally into this vein or through the anterior accessory saphenous vein into the great saphenous vein from the lateral side. Here, as with the pudendal vein, only precise examination can shed light on these different reflux sources (Figs. 7.22 and 7.23).

Reflux with competent terminal valve of the great saphenous vein. (a) Transverse view through the left groin. Reflux from the epigastric vein (EV) into the great saphenous vein (GSV) without incompetence of the saphenofemoral junction. The reflux from the epigastric vein flows away from the probe into the great saphenous vein and is therefore shown in blue (online material) (CFV common femoral vein). (b) Longitudinal view through the same groin. The epigastric vein does not run on this plane and therefore indicated with a dotted line in the upper left of the second image. One valve leaflet is shown in yellow. (c) Longitudinal view in muscular diastole. Reflux from the epigastric vein is seen flowing into the great saphenous vein
Copyright: [Author]

(a) PW measurement in the great saphenous vein immediately below the saphenofemoral junction, * muscular systole giving rise to antegrade flow, ** muscular diastole evidencing reflux. (b) Measurement in the epigastric vein of the same subject demonstrating a long-lasting flow towards the feet and into the saphenofemoral junction. The flow is continuous and prolonged with only a short interruption during muscular systole . (c) Measurements taken at the saphenofemoral junction in the same patient. Here it might be supposed that the reflux comes from the common femoral vein because it was recorded in the immediate vicinity. (d) Measurement in the common femoral vein at the saphenofemoral junction. No reflux is recorded. Flow from the epigastric vein fills the great saphenous vein. The reflux profile from the epigastric vein in (b) coincides with the great saphenous vein in (a). This is an additional support for the conclusion that the blood volume in the great saphenous vein comes from the epigastric vein
Copyright: [Author]
The epigastric vein unlike all the situations described so far (see also Fig. 7.2) is never the last vein to join the junction segment of the great saphenous vein before the saphenofemoral junction. In research in surgical preparations (Mühlberger et al. 2009), the average distance between the confluence of the epigastric vein with the saphenous vein and the confluence of the great saphenous vein with the common femoral vein was found to be 1.2 cm. In only 30 % of epigastric veins was this distance reduced to 0–0.7 cm.
Reflux in the cranial part of the lateral segment must not only be sought in the confluence region. The whole proximal great saphenous vein must be examined systematically for inflows. The groin region proximal of the saphenofemoral junction must be examined for refluxive vessels. They must then be followed to their confluence with the deep veins or refluxive leg veins.
7.3.6 Physiological and Pathological Flow in Groin Tributaries
It is often difficult to determine whether a tributary is refluxive. In these vessels the physiological flow is into the great saphenous vein and towards the foot. Therefore, no conclusion can be drawn from the flow direction alone.
Analysis of the velocity profile is decisive. After manual compression of the calf, the Wunstorf manoeuvre or during the Valsalva manoeuvre, a short, not very rapid, flow in these tributaries is normal. The description “short” in this context needs to be defined. In venous assessment the backflow should last no more than 0.5 or 1 s, depending on the author, if it is physiological. The short backflow in a healthy vein lasts between 0.1 and 0.2 s and represents the time taken for the valve to close. Regarding superficial inguinal tributaries, a precise time cut-off point is less meaningful because these veins drain physiologically into the deep veins during muscular diastole. A variety of components interact in these cases adding further difficulties to a time definition, as can be seen in Figs. 7.24 and 7.25. The concept of “flow volumes” in the diagram should be regarded as a semi-quantitative measure and refers to the area under the velocity profile.

Algorithm for assessing reflux in the saphenofemoral region to determine whether the incompetence of the great saphenous vein (GSV) is complete or incomplete
Copyright: [Author]

Comparison of the velocity profiles between a tributary and the great saphenous vein. (a) Short backflow with small volume in a healthy superficial inguinal tributary. (b) The backflow in this tributary has an identical profile to the great saphenous vein, making it clearly responsible for the reflux into the great saphenous vein. This is regardless of whether the profiles are steep or relatively flat. (c) Reflux volumes in this great saphenous vein are greater than in the tributary, but just as prolonged. Here, the tributary is partly responsible for the reflux and therefore pathological, but it is obvious that the great saphenous vein is filled from several sources. (d) Reflux in this great saphenous vein is shorter than in the tributary (upper) or absent (lower). The tributary in both these cases has a clear pathological flow and must be considered refluxive. It is likely that they are draining through the saphenofemoral junction into the deep veins or the flow is too small to be recognised if it drains down into the increased calibre great saphenous vein
Copyright: [Author]
Healthy tributaries can be seen in B scan as small calibre vessels usually only when they are being specifically targeted. In colour duplex they are easier to find during muscular diastole. A tributary which is obvious during a B scan examination is usually pathological and requires further assessment. If the flow in the tributary is longer than 1 s, its velocity profile must be compared with that of the great saphenous vein.
In poorly drained systems (Sect. 3.2.3), there is often reflux from one of the superficial inguinal tributaries. The identification of a refluxive tributary is important for the prognosis after treatment. The highest reflux source in these patients may be from a pelvic origin. Therefore, whatever endovenous leg procedure is selected, this source is unlikely to be included in the treatment. This may lead to early recurrences in the patient (Sect. 13.3).
It has been shown that female patients with reflux from the superficial inguinal tributaries have high oestradiol levels in the blood of the varicose veins themselves. More surprising was that there were also increased levels of testosterone in comparison to male patients (Oswald 2005). This discovery must be examined with further research for its clinical implications and prognostic significance. Nevertheless, it confirms that gonadal venous blood is present in leg veins which may have originated from a proximal reflux source.
7.3.7 Reflux in the Anterior Accessory Saphenous Vein
The anterior accessory saphenous vein joins the great saphenous vein in the groin. Rarely it joins the common femoral vein directly. Occasionally there is duplication in the region of its termination (Figs. 7.2, 7.3, 7.4, 7.5, 7.6, 7.10, 7.11, and 7.12). An anterior accessory saphenous vein is found in only 50 % of cases (Mühlberger et al. 2009). The average distance between the confluence of the anterior accessory saphenous vein with the great saphenous vein and the saphenofemoral junction is 2 cm. In 90 % of legs, the anterior accessory saphenous vein is joined by one or more tributaries (epigastric or superficial circumflex iliac vein) before it terminates into the great saphenous vein.
Normally the anterior accessory saphenous vein is distinguished from the great saphenous vein because of its lateral position in relation to the great saphenous vein and common femoral vein (Fig. 7.4). However, this anatomy is sometimes not so easy to detect if its course is followed carefully. Occasionally, the vein which appears in the groin from a lateral position may prove to be the great saphenous vein (Sect. 7.4). Aplasia of the proximal section of the great saphenous vein may lead to a mistaken identity.
If there is reflux in the anterior accessory saphenous vein in the groin, there are three possible findings:
-
Reflux from the common femoral vein through the saphenofemoral junction:
-
With a healthy great saphenous vein in its downward course. The proximal great saphenous vein is only incompetent down to the confluence of the anterior accessory saphenous vein, Hach Class I (Figs. 7.26 and 7.28a)
Fig. 7.26 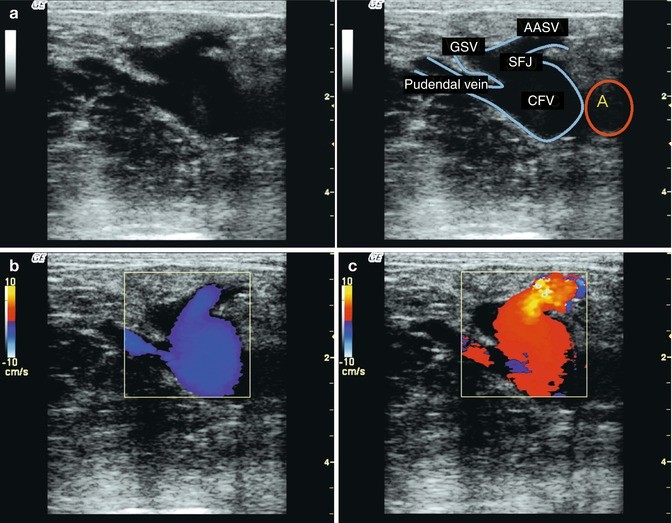
Transverse view through the groin with an incompetent terminal valve and reflux escaping through the accessory anterior saphenous vein. This is complete incompetence of the great saphenous vein, Hach Class I. (a) The saphenofemoral junction (SFJ) is dilated to accommodate the drainage of the great saphenous vein (GSV) and anterior accessory saphenous vein (AASV). There is an incidental finding of independent drainage of the pudendal vein (PV). (b) During muscular systole there is antegrade flow (blue) in the common femoral vein (CFV), the anterior accessory saphenous vein and pudendal vein, but no flow in the great saphenous vein. (c) During muscular diastole there is reflux through the saphenofemoral junction into the anterior accessory saphenous vein. There is no reflux in the lower part of the great saphenous vein (online material)
Copyright: [Author]
-
With an incompetent great saphenous vein where the anterior accessory saphenous vein is a refluxive tributary of the refluxive great saphenous vein (Figs. 7.27 and 7.28b).
Fig. 7.27 
A tortuous and dilated anterior accessory saphenous vein (AASV) in the groin. The saphenofemoral junction (SFJ) is refluxive with the reflux flowing into both the great saphenous vein (GSV) and the anterior accessory saphenous vein. The anterior accessory saphenous vein is so tortuous that it is already visible as an independent vessel in the image of the saphenofemoral junction. It lies lateral to the tangential line through the medial circumference of the common femoral vein (CFV) (see also Fig. 7.4)
Copyright: [Author]
Fig. 7.28 
Possible forms of reflux in the confluence of the anterior accessory saphenous vein using the right groin as an example. (a) Reflux (red arrow) from the common femoral vein through the saphenofemoral junction into the anterior accessory saphenous vein. The great saphenous vein is healthy in its further course with antegrade flow (white arrow). (b) Reflux (red arrow) from the common femoral vein through the saphenofemoral junction which is directed into both the anterior accessory saphenous vein and the lower part of the great saphenous vein. (c) Reflux (red arrow) from the epigastric vein which joins the anterior accessory saphenous vein directly. The great saphenous vein is healthy in its further course downwards with antegrade flow (white arrow). (d) Reflux (red arrow) from the great saphenous vein flowing into the anterior accessory saphenous vein. The saphenofemoral junction and great saphenous vein are competent
Copyright: [Author]
-
-
Reflux from the confluence of superficial inguinal veins into the anterior accessory saphenous vein without reflux of the great saphenous vein or the saphenofemoral junction (Fig. 7.28c).
-
Reflux from the antegrade flow in the great saphenous vein into the anterior accessory saphenous vein. The deep veins are not involved in this type of recirculation (Fig. 7.28d).



It is important to distinguish these findings for the purposes of deciding on a treatment strategy and in making a prognosis. The prognosis is less good with reflux arising from the confluence of the superficial inguinal veins.
7.3.8 Pelvic Venous Reflux Through Franceschi’s P and I Points
When there is reflux arising from within the pelvis, the blood flow escaping into the subcutaneous compartment can be observed at two points (see also Sect. 3.3.6).
The I point is located in a standing subject approximately 1–3 cm above and lateral to the saphenofemoral junction. It is medial to the epigastric veins. If the I point is incompetent, a refluxive round ligament vein will be found above the inguinal ligament in transverse view. Reflux is best observed here during the Valsalva manoeuvre. It is also present, but less obvious, using other provocation manoeuvres.
The P point is located in the lithotomy position with the probe applied at right angles or slightly skewed near the labia. If the P point is incompetent, it is best demonstrated during the Valsalva manoeuvre. There will be a strong reflux signal between the vaginal cavity and the ischiopubic bone (Fig. 7.29).

Image showing reflux at the P point near the left labium. The probe is applied at right angles as shown in the diagram. Reflux is seen passing from the internal pudendal vein to the external pudendal vein
Copyright: [Author]
7.3.9 Reporting the Superficial Inguinal Veins
Examination findings can be documented on a line diagram or template during the examination and described in writing. However, recording the findings in a table is fast and easy to review. A suggested table is shown (Table 7.1).
7.3.10 Clinical Implications of Different Reflux Sources in the Groin
In the pre-ultrasound era, treatment of varicose veins was restricted to stripping of the great saphenous vein including ligation of all superficial inguinal tributaries in a crossectomy. Neovascularisation was considered to be the only cause of recurrence assuming a well-performed initial operation. The introduction of ultrasound allowed new treatment procedures to be developed.
In the early days of endoluminal laser ablation, the confluence of superficial inguinal veins was intentionally left unclosed. Current practice in most units is to leave with a gap of about 2 cm between the lower margin of the ostium and the tip of the laser. However, controversy remains as to the ideal placement of the laser tip with some advocates pursuing a “flush” ablation and others a more “selective” ablation. These different techniques continue because there remains a lack of an agreed definitive solution.
A post-operative ultrasound examination is able to determine the nature of recurrent veins in the groin. For example, an inflow from the epigastric veins without reflux can be distinguished from a neovascularisation wherein newly formed veins develop and connect to the common femoral vein. The former recurrence may arise when reflux from the epigastric veins existed prior to the operation and the crossectomy deprived them of a drainage route (Sects. 13.3.1 and 13.4.1). A similar situation may be seen after ligation of the confluence of superficial inguinal veins when reflux from the pelvis existed prior to the operation. These veins quickly enlarge and develop to find a connection to the distal great saphenous vein which was not initially removed. A recurrence often results (Sect. 13.3.2).
Duplex ultrasound plays an important part in the preoperative diagnosis, accurate documentation and follow-up of the groin regardless of whatever treatment was used. If the source of preoperative reflux is detected precisely in advance, then the optimum treatment for the saphenofemoral region can be selected in accordance with the drainage routes. Options may include closure of the pelvic reflux path or closure of the great saphenous vein distal to the entry point of the pudendal vein to allow drainage.
Stücker summarised the different possibilities of reflux in the groin into three types (Stücker et al. 2013):
-
Type 1: Incompetence of the terminal but sufficiency of the preterminal valve with reflux escaping through anterior accessory saphenous vein
-
Type 2: Sufficiency of the terminal but incompetent preterminal valve with reflux originating in tributaries and not in deep vein
-
Type 3: Incompetence of the terminal and the preterminal valve with reflux emerging from deep vein and descending along the great saphenous vein
7.4 B Scan Examination Along the Great Saphenous Vein
The anatomy of the great saphenous vein has already been described (Sects. 2.4.1, 2.4.2, 2.4.3, 2.4.4, and 2.4.5). The great saphenous vein is generally examined starting at the groin and going down to the foot.
The subject should be standing with the majority of their weight on the contralateral leg whilst holding onto a frame for light support. The test leg should be dependent, slightly externally rotated with the foot lightly resting on the floor and pointing laterally (Fig. 7.1). As a matter of routine, once the superficial inguinal tributaries have been identified and assessed (Sect. 7.3), a compression manoeuvre should be carried out on the saphenofemoral junction and the deep veins to exclude thrombosis (Fig. 7.30).

Compression manoeuvre in the groin. Transverse view of the right groin in a standing subject. The first image shows the normal state of the saphenofemoral junction (SFJ) and the second image the appearances during compression with the probe. The artery is slightly squashed (A) during compression, but the common femoral vein (CFV) and saphenofemoral junction (SFJ) become a narrow slit
Copyright: [Author]
The diameter of the great saphenous vein is often measured to check if the vein is incompetent and for study purposes. The UIP (Union Internationale de Phlebologie) consensus document suggests measuring the vein at the saphenofemoral junction or within the first 3 cm of the great saphenous vein and in the middle of the thigh (Coleridge-Smith et al. 2006). However, these recommendations have not been validated by studies.
Optimum Point for Measuring the Diameter of the Great Saphenous Vein
Current data suggest a second measurement point in the proximal thigh 10–15 cm from the groin (Fig. 7.31, see also Fig. 7.1). In a population of 182 legs, the diameter of the great saphenous vein was measured in the standing subject 2–3 cm and also 10–15 cm below the saphenofemoral junction. Sixty legs had a healthy great saphenous vein, and 122 presented with reflux beginning in the groin. Fifty-one of these were refluxive above the knee only (Hach Class II), and 71 were refluxive above and below the knee (Hach Class III and IV). The diameter did not correlate with age or sex at either measurement point. Correlations were found with weight, moderate correlations between the diameter and the clinical class of CEAP, as well as the refilling time. Although a high correlation was found between the diameters at the groin and in the thigh, the predictive value of the diameter in the proximal thigh was better for the presence of reflux and the clinical class. The great saphenous vein at the proximal thigh was more uniform, easier to measure and more representative as a single measurement point.

Diameter measurements in the great saphenous vein. (a) Transverse views through the right groin (left half of image) and the thigh 10–15 cm below the groin (right half of image) in a normal subject. The great saphenous vein was measured at both points. The diameter in the groin was 0.81 or 0.7 cm depending on which axis was taken. In the thigh it was smaller at 0.56 cm. b: Transverse view through the right groin in a patient with venous insufficiency. The great saphenous vein is elliptical in shape. Gross differences in the measurements were obtained depending on the axis taken (1.4–2.2 cm). The diameter at the thigh was significantly smaller at 0.9 cm. c: Longitudinal view through the course of the proximal great saphenous vein. The left and right halves of the image show the great saphenous vein in continuity. A uniform and reliable measurement point is difficult to obtain because of the progressive reduction in the calibre of the great saphenous vein
Copyright: [Author]
The average diameter in subjects with healthy veins was 7.5 mm (±1.8) at the saphenofemoral junction and 3.7 mm (±0.9) in the proximal thigh. In subjects with reflux, the average diameter was 10.9 mm (±3.9) at the saphenofemoral junction and 6.3 mm (±1.9) in the proximal thigh. The diameter did not correlate with the Hach Class (Mendoza et al. 2013).
Diameter measurements should be taken in a transverse image. It remains controversial whether the probe should be at right angles to the skin or diagonal in position. As shown in Fig. 7.31, the variability demonstrated at the saphenofemoral junction measurement point, the preferred point chosen by most phlebologists, is so great that this is unlikely to provide meaningful information. For studies it is important always to use the same method of measurement and to describe this method exactly.
For the reasons mentioned above, it is preferable to measure the diameter in the thigh, 10–15 cm from the groin, in a segment where the walls of the great saphenous vein run parallel and there are neither inflows nor outflows. The ideal probe position is at about the height of the yellow line in Fig. 7.1.
Interval compression manoeuvres in B scan should be performed to exclude a thrombosis along the course of the great saphenous vein (see also Chap. 11). Furthermore, the course of the vein within its fascia (Sect. 7.4.1) and any aplastic/hypoplastic (Sect. 7.4.2) or duplications (Sect. 7.4.3) should be identified at this stage of the examination.
The great saphenous vein should be examined over its entire course in transverse view so that tributaries and perforating veins are not overlooked. Variations in calibre must always be examined with care. In such cases it is important to check for reflux in the distal segment after the separation of a refluxive tributary. The smaller calibre great saphenous vein below a refluxive tributary is frequently competent; however, this is not necessarily always the case.
7.4.1 Saphenous Eye
Bailly proposed the term “saphenous eye” for the typical appearance of the great saphenous vein in the thigh and calf in transverse view (Bailly 1992 in Appendix 2). The eye consists of the muscle fascia (lower lid), saphenous fascia (upper lid) and the great saphenous vein itself, representing the iris and pupil (Figs. 7.32 and 7.33). The saphenous fascia lies directly on or just above the great saphenous vein. Occasionally a thin additional fascia can be seen in the subcutaneous fatty tissue (Figs. 7.34a and 7.36). This fascia if present separates the subcutaneous tissue into two layers and runs parallel to the muscle fascia.

Variations of the saphenous eye in the thigh. (a) Transverse view through the inner thigh with normal appearance of the saphenous eye. (b) The appearance may be asymmetrical depending on the level of the section and the fat content of the leg. (c) When the fat content is high, there may be a space between the lower lid and the iris. If the saphenous compartment is filled with fat, the great saphenous vein (GSV) does not lie directly on the muscle fascia. (d) If the great saphenous vein is refluxive, the iris will appear very big. In this image the connective tissue anchoring the great saphenous vein, the saphenous ligament (arrowed), is very clear
Copyright: [Author]

The saphenous eye in the lower leg. (a) Transverse view through the left calf, approximately10 cm below the posterior skin crease of the knee. The saphenous eye is harder to identify in the calf, because there is much less fat in this region. The edge of the tibia is on the right of the image (arrows). (b) It is difficult to distinguish the eye clearly from the surrounding tissue in the calf as demonstrated in the left leg of an obese subject. The tibial edge is arrowed. (c) In the calf the fascial compartment helps in differentiating between the saphenous vein and the tributaries. The left image shows a refluxive tributary and great saphenous vein in muscular systole. There is antegrade flow in the great saphenous vein (blue). The right image is during muscular diastole. There is no flow in the great saphenous vein, but the tributaries are filled refluxively. The fascia is just discernible in the lateral part of the compartment to the right of the colour window immediately above the tibial edge (arrowed)
Copyright: [Author]

Junction of the great saphenous vein in continuity with a tributary. (a) Longitudinal view through the inner thigh. The axes of the proximal (refluxive) and distal (competent) great saphenous vein (GSV) usually run in a straight line as shown. The tributary comes off at an angle of varying degrees. A valve leaflet is visible at the junction of the tributary with the great saphenous vein (marked in yellow). The sharp white contour of the great saphenous vein is prominent because it represents a thick vein wall. The tributary in contrast has a thin wall which is much less apparent (saphenous fascia yellow arrows, subcutaneous fascia red arrows). (b) Longitudinal view through the inner thigh demonstrating a refluxive great saphenous vein (#) in continuity with a refluxive tributary . Its further course disappears from the right of the image because it becomes tortuous. The great saphenous vein itself is competent (+) more distal. The large calibre of the great saphenous vein and associated tributary gives the false impression that the distal great saphenous vein is a tributary because it forms an angle with the axis. (c) Another patient demonstrating the junction of the great saphenous vein with a straight continuation of a tributary. During muscular systole there is antegrade flow in all veins. The great saphenous vein is tented up towards the skin, making the antegrade flow in the distal section of the vein appear red because the flow here is towards the probe. The tributary is dilated. (d) During muscular diastole there is gross reflux into the dilated tributary and antegrade flow in the distal great saphenous vein (online material)
Copyright: [Author]
If the upper and lower lid of the saphenous eye cannot be identified in association with a vein in transverse view, it is not the great saphenous vein. Any tortuous structure visible from the exterior is a tributary. The great saphenous vein is straight and cannot become tortuous within its fascial compartment because it is anchored by the saphenous ligament and surrounding connective tissue. Tortuous and dilated veins are always tributaries. This difference is very important for establishing the Hach Class (Sect. 4.1).
To the novice examiner, refluxive tributaries may be taken for the great saphenous vein if they appear to be straight downward continuations (Fig. 7.34).
7.4.2 Aplasia/Hypoplasia of the Great Saphenous Vein
An aplastic or hypoplastic segment of the great saphenous vein is found in 12 % of subjects with healthy veins and 24 % of those with refluxive great saphenous veins (Sect. 2.4.4). A straight or tortuous tributary runs parallel to this aplastic segment in the subcutaneous tissue carrying the blood from distal to enter the patent proximal part of great saphenous vein (or vice versa if there is reflux). In aplastic segments the saphenous eye appears “empty” (Fig. 7.35). However, if the empty saphenous eye is studied histologically, a rudimentary saphenous vein is always found. In case of very thin saphenous vein, many phlebologists use the term hypoplastic (Sect. 2.6.3).

Aplastic segment of the great saphenous vein. (a) An “empty” saphenous eye in the thigh with a dilated tributary directly under the skin. (b) With less fatty tissue the “eye” is smaller. Transverse view above the aplastic segment demonstrating the junction of the great saphenous vein with the extrafascial tributary is seen on the online material. (c) Longitudinal view in the same leg at the point where the tributary leaves the saphenous compartment. No visible vein remains within this saphenous compartment. (d) Longitudinal view though the distal thigh in colour duplex demonstrating a very short aplastic segment. The reflux bypasses the aplastic segment of the refluxive great saphenous vein (arrowed) by running above the vein in a tributary for a short distance. It then rejoins the great saphenous vein further down. A competent great saphenous vein with an aplastic segment is shown on the online material
Copyright: [Author]
7.4.3 Duplication of the Great Saphenous Vein
As described above (Sect. 2.4.3), only those veins which course through the saphenous compartment can be defined as saphenous veins. Thus, there is only a duplication when both the branches run parallel inside this compartment. True duplication is found in 1 % of subjects (Fig. 7.36). A tributary running through the subcutaneous fatty tissue parallel to the great saphenous vein is found in the thigh of 26 % of legs. This is a pseudo duplication, Fig. 7.37. In subjects with healthy veins, the lumen of this accompanying vein is often larger than that of the great saphenous vein itself. In phlebography there was no way of distinguishing whether the course of a vein is intrafascial or extrafascial. Consequently, pseudo and true duplications were classified together which increased the frequency of a duplicate system to 27 % (Sect. 2.4.3).

Subject with a true duplication of the great saphenous vein in the right leg starting 3 cm below the saphenofemoral junction down to the posterior knee crease. (a) Transverse view just above the knee with both great saphenous veins in close proximity. The saphenous ligament (yellow arrow) connects the two veins. An additional layer of connective tissue is visible within the subcutaneous fat (red arrows) online material. (b) Transverse view approximately 10 cm below the groin in the same subject. The saphenous compartment contains both great saphenous veins. Further lateral an anterior accessory saphenous vein is apparent (#). The online material contains two more images of the same subject at the mid and distal thigh. The two veins are slightly further apart at these points but are still within the same compartment and connected together by the saphenous ligament
Copyright: [Author]

Pseudo duplication of the great saphenous vein. Transverse view through the thigh. A second vein is seen running parallel to the great saphenous vein within the subcutaneous fat. This is a straight tributary accompanying the great saphenous vein (online material)
Copyright: [Author]
If the great saphenous vein is refluxive, this does not necessarily mean that both limbs of a duplication are refluxive (Fig. 7.38).

(a) Transverse view through the inner thigh demonstrating a duplication of the great saphenous vein (GSV) in the saphenous compartment with an accompanying tributary . The right vessel of the duplication (#) and the tributary are refluxive (online material). The left vessel (+) is competent (▶ velocity profile at bottom). As the refluxive vessel joins the competent vessel further down, it delivers its reflux into the competent vessel provoking a permanent antegrade flow. That means that blood flow is antegrade in the competent vessel during muscular diastole (right B scan unmarked, left B scan marked). (b) Diagram of the recirculation circuit. The refluxive vessel of the duplication is shown dark red (SSV small saphenous vein)
Copyright: [Author]
7.4.4 Course of the Great Saphenous Vein
The great saphenous vein appears on ultrasound medial to the confluence of the superficial inguinal veins. In disease it is a large vessel coming up from the thigh (Fig. 7.39). The greatest volume of antegrade flow will be observed during provocation manoeuvres. Occasionally the great saphenous vein in the groin can be situated in a medial or lateral position which may cause confusion with the anterior or posterior accessory saphenous veins (Fig. 7.40; see also Sects. 10.4 and 10.5).

Longitudinal view of the normal course of the great saphenous vein (GSV) in the groin in a patient with an incompetent terminal valve. During muscular diastole turbulent flow from the common femoral vein (CFV) is seen entering the great saphenous vein via the saphenofemoral junction (SFJ). The common femoral vein is marked with blue dotted lines because it leaves the plane of this image
Copyright: [Author]

(a) Transverse view through the right groin just below the saphenofemoral junction. A large vein is observed in a lateral position with a smaller less defined vein further medial. The classic assumption would be that the anterior accessory saphenous vein is incompetent (see also Fig. 7.10b) and the great saphenous vein is healthy. With further assessment of the course of the veins, it becomes apparent (online material) that the refluxive vein running laterally in the groin is the great saphenous vein (GSV) and the medial competent vein is the posterior accessory saphenous vein (VSAP). (b) Transverse view through the same leg further proximal in colour duplex. The lateral vein is refluxive (red), the much smaller medial vein (arrow) is not (no signal on colour duplex)
Copyright: [Author]
There are several ways of confirming the identity of the great saphenous vein:
-
If the probe is passed to and fro along the inner thigh in transverse view, the saphenous eye will always be found whether “filled” or “empty” Figs. 7.32 and 7.35). In the distal thigh, there may be a palpable fascial defect which can be felt as a “hole” in the tissue. This is often assumed to be the point where a perforating vein passes through the musculature. However, in B scan it can be seen that this is incorrect. The vein at this point is usually either uniformly dilated (Fig. 7.41a) or demonstrates a focal dilatation along one side of the wall (Fig. 7.41b, c).
Fig. 7.41 
Image of a dilated section of the great saphenous vein in the distal thigh. (a) Longitudinal view through the inner thigh just above the knee demonstrating a dilation of the great saphenous vein. A perforating vein in this region cannot be identified. (b) Longitudinal view in the distal thigh showing the great saphenous vein and a very marked bulge (left) which fills with erythrocyte sludge if the subject stands still for a few seconds (right). Note the increasing prominence of the acoustic shadow (objects in B scan, Chap. 1). (c) Longitudinal view through the distal thigh in a different subject with erythrocyte sludge in an aneurysmally dilated region of the great saphenous vein. Left after the subject has been standing still, middle with extension of the toes, right after muscular diastole
Copyright: [Author]
-
The great saphenous vein is always posterior to the medial condyle of the knee (Fig. 7.48a).
-
One to two hand’s breadths below the knee, the great saphenous vein is always found between the tibial edge and the extensor hallucis longus muscle (Fig. 7.33a–c).
-
At the ankle the great saphenous vein lies on or is slightly anterior to the medial malleolus (Fig. 2.5). This is difficult to demonstrate using ultrasound because the contact area of the probe is minimal. If this area is followed up the leg, the great saphenous should be found a few centimetres above the ankle.

Despite a systematic examination, a great saphenous vein along its typical course may not be identified in some subjects. This happens occasionally after the subject has been standing for some time (Fig. 7.42). In these subjects erythrocyte sludge may settle in the vein filling it with a homogeneous grey colour instead of a black void. This is difficult to differentiate from the surrounding tissue. There are various ways of “clearing” the vein to return it to its echo-free state. These include vein compression with the probe, manual calf compression or the Wunstorf manoeuvre. The main objective is to create flow in the vein to “flush out” the erythrocytes.

(a) Transverse view through the inner thigh demonstrating an almost invisible great saphenous vein. The erythrocyte sludge has eliminated the contrast between the vein and the surrounding tissue. The accompanying tributary could be easily overlooked. (b) After the Wunstorf manoeuvre, both the great saphenous vein and a refluxive tributary are clearly visible
Copyright: [Author]
7.5 Measuring Blood Flow Along the Great Saphenous Vein
Duplex ultrasound offers two ways of measuring blood flow in the great saphenous vein. These are PW (velocity profile analysis) and colour-coded duplex. In contrast to the arteries veins are collapsible tubes without a regular pump from behind. This makes consistent velocity measurements difficult to obtain. Therefore, a semi-quantitative evaluation of the velocity profile is all that is usually possible (Fig. 1.20). The angle of insonation in relation to the course of the vein is not as important as it is with arteries.
7.5.1 Normal Findings
In a standing subject, the great saphenous vein has a poor, hardly measurable, upward flow. Therefore, a provocation manoeuvre will be required to assess flow in this vein (Fig. 7.43a, b; see also Chap. 6).


The antegrade volume flow generated by a provocation manoeuvre varies in every subject. (a) PW measurement in the great saphenous vein 10 cm below the groin during a manual calf compression and release manoeuvre. (b) The same measurement during a Wunstorf manoeuvre. The flow in this case is more prolonged. (c) Colour duplex image in the great saphenous vein 10 cm below the groin; left under a Wunstorf manoeuvre, the flow is antegrade (blue). After the toes are relaxed, there is a short change of colour to red (right), corresponding to the short backflow until the valve closes. (d) A large 6.1 mm diameter competent great saphenous vein in the thigh shown with colour duplex. (e) Measurement of the same vein in PW mode demonstrating antegrade flow with a short backflow. (f) Reflux in the great saphenous vein in the thigh in a vein of only 3.5 mm in diameter
Copyright: [Author]
Muscle contraction of the calf (Wunstorf manoeuvre) or a manual calf compression is sometimes insufficient to provoke adequate flow in a healthy great saphenous vein. This is because the blood leaves the great saphenous vein partially or completely through perforating veins before it reaches the probe (Fig. 7.43b). To measure flow in the proximal thigh, both methods (muscle contraction and manual compression) should therefore be used (Fig. 7.43a, b). Manual compression of the thigh immediately distal of the probe is a useful complement. In healthy veins antegrade flow is observed. The velocity profile is down and away from the probe in PW (Fig. 7.43a, b) On colour duplex the vein is coloured blue (Fig. 7.43c). This antegrade flow may be followed by a short backflow. This is represented in PW as a short upward curve (Fig. 7.43a, b). On colour duplex there is a flicker of red (Fig. 7.43c).
This short backflow is caused by gravity. The blood flows back under the force of gravity until the valve closes. Additionally, as has been reported by Lurie and Kistner, B mode has demonstrated a vortex effect in the sinus of the valve that actually initiates closure of the valve during antegrade flow. Then, retrograde flow of a small volume is necessary to approximate and push the valve cusps back into the lumen thereby closing the valve (Lurie et al. 2003).
Measuring the diameter alone is not enough to judge whether a vein is competent or incompetent. It is not unusual for large calibre veins to be competent (Fig. 7.43d, e) and very small calibre veins to be refluxive (Fig. 7.43f). Special attention must be paid to large calibre veins with exclusively or predominantly antegrade flow, especially during muscular diastole. This may indicate a secondary dilation due to deep venous obstruction (Chap. 15).
In the absence of visible varices, a competent saphenofemoral junction may give a false reassurance of normality with the temptation not to examine the rest of the veins. Even in the absence of significant perforating veins or tributaries in B scan, the flow patterns should still be examined at various points. As a minimum requirement, the great saphenous vein should be assessed at the following points:
-
The point at which the diameter was measured (10–15 cm below the groin)
-
The distal thigh at the level of the perforating veins of the adductor canal (formerly Dodd and Hunter)
-
Below the knee at the height of the paratibial perforating veins (formerly Boyd)
-
Just above the ankle
Occasionally the great saphenous vein forms part of a recirculation circuit without being filled itself in retrograde flow. In this situation it may be filled with refluxive blood from a perforating vein or tributary where it carries this blood in antegrade flow to a refluxive tributary further up the leg. In B scan an increase in diameter is observed with the velocity profile showing antegrade flow during both systole and diastole, usually with a much larger volume flow in diastole (Fig. 9.10). This condition is called antegrade incompetence.
7.5.2 Reflux in the Great Saphenous Vein
When a subject with an incompetent great saphenous vein is standing, antegrade flow during a provocation manoeuvre will be followed by reflux. Usually there is a greater volume of refluxive blood than that observed in antegrade flow. The reflux may be short and rapid (Fig. 7.44a) or slow and long-lasting (Fig. 7.44b), or a combination of these two extremes (Fig. 7.44c). In colour duplex the reflux appears as a red colour in the lumen (Fig. 7.44c, d). If the curve in PW duplex disappears after the short, necessary backflow for valve closure, it is easy to stop observing and overlook a low-volume reflux which continues for much longer (Fig. 7.45).

(a) Transverse view through the inner thigh with a refluxive great saphenous vein. In PW a short antegrade flow is observed (downward curve) followed by a large volume of reflux (upward curve). (b) Transverse view through the inner thigh with a refluxive but poorly drained great saphenous vein. The reflux is slow and long-lasting. This is easily overlooked using colour duplex. (c) Transverse view through the inner thigh in colour duplex. The great saphenous vein maintains a red colour in its lumen for a long time (online material). (d) Longitudinal view through the great saphenous vein with reflux in colour duplex. This image is obtained by angling the measurement window along the great saphenous vein as it runs parallel to the skin
Copyright: [Author]

(a) Transverse view through the thigh using PW mode. After a provocation manoeuvre causing antegrade flow, there is a short, rapid reflux causing valve closure followed by slower, longer-lasting reflux. The first part of the curve is the backflow signalling terminal valve closure in the groin. The second part is much slower and represents the reflux carried from the posterior accessory saphenous vein flowing into the great saphenous vein. This finding would be overlooked if the examination concluded prematurely after recording the short backflow curve. (b) Transverse view through the thigh with backflow causing saphenofemoral junction closure (steep upward curve) followed by prolonged low-volume reflux arising from the epigastric vein (flat upward curve)
Copyright: [Author]
The reflux volume is the blood volume which first flows upwards during a provocation manoeuvre and then flows down again during the relaxation phase of the manoeuvre (Chap. 3). By the definition from the international consensus document (Coleridge-Smith et al. 2006), the retrograde flow must last at least between 0.5 and 1 s before it can be regarded as reflux. The clinical importance of reflux between 0.5 and 1 s has never been fully assessed in a study. It may be sensible to use the 1 s cut-off point to define pathology because shorter flows often correlate with reflux volumes which are very small with questionable clinical significance.
The curve is never unequivocal. Reflux phenomena may occur at volumes similar to the volumes observed in antegrade flow (Fig. 7.46a). Clarification can be obtained by using different provocation manoeuvres (Fig. 7.46b). The examiner must pay special attention in cases where the examination may be painful. In the presence of oedema from chronic venous insufficiency, the great saphenous vein may be only moderately dilated with very little flow observed during provocation. The antegrade and retrograde flow curves in PW mode may be too diminished to be clinically useful. In this situation an elevation-dependency manoeuvre (Sect. 6.9) may be very helpful in clarifying pathology.

Incomplete incompetence of the great saphenous vein filled by reflux from a paratibial perforating vein (formerly Boyd). (a) Examination of the great saphenous vein in the calf below the reflux source from the incompetent perforating vein using manual compression. In B scan note that the reflux duration is relatively short. (b) Examination of the same great saphenous vein using the Wunstorf manoeuvre. The antegrade flow is smaller but the reflux is of much greater volume. There are two peaks. The first reflux curve appears while the forefoot is still elevated. After relaxation more reflux is allowed to flow out from the perforating vein. The Wunstorf manoeuvre appears to be more reliable than manual compression when assessing incompetence in perforating veins
Copyright: [Author]
When the great saphenous vein is dilated, the valves can be seen “open” in muscular systole and “closed” in diastole. Even if the valve appears closed, the vein may still be incompetent (Fig. 7.47).

Valves in a refluxive great saphenous vein. Longitudinal view through the inner thigh in the same subject as seen in Fig 7.44d but further proximal. (a)Observed during muscular systole (left) and muscular diastole (right). The upper valve leaflet in the image appears to be rigid because it does not seem to close across the lumen (online material). (b) Valve wings marked (yellow)
Copyright: [Author]
7.5.2.1 Identifying the Reflux Source of the Great Saphenous Vein
In the vast majority of cases, the great saphenous vein is filled refluxively at a single point like the saphenofemoral junction. However, when looking for proximal reflux sources, there may be other pathological inflows. These include an additional refluxive inguinal tributary, a perforating vein or refluxive flow from the anterior accessory saphenous vein.
Interesting
Most dilated perforating veins in the course of a refluxive great saphenous vein are well drained and not refluxive (Chaps. 3 and 9).
Once the junction of the great saphenous vein with the common femoral vein has been examined (Sect. 7.3), it may be competent or refluxive. If the saphenofemoral junction or a superficial inguinal tributary is incompetent and fills the great saphenous vein, then this will identify the proximal reflux source (Fig. 7.39a).
However, if the saphenofemoral junction is competent, then the vein should be examined from proximal to distal. The probe should be held in transverse view to determine possible reflux sources. These include sites where dilated perforating veins or tributaries join the vein. Usually these inflows are associated with alterations in calibre. The vein is usually smaller in calibre proximal to the inflow compared to further down (Fig. 7.48a).

Reflux source from the proximal paratibial perforating vein (formerly Boyd). (a) Great saphenous vein below the knee proximal of the perforating vein (left) and distal (right). The enveloping saphenous fascia can be seen at both points. There is a clear change in calibre with reflux below the entry of the perforating vein and competency above (additional material online). (b) Transverse view through the calf at the level of the paratibial perforating vein. The junction of the refluxive perforating vein with the great saphenous vein is shown (additional material online)
Copyright: [Author]
Common reflux sources into the great saphenous vein:
-
Posterior accessory saphenous vein. The reflux originates from the small saphenous vein (Fig. 4.9a), the pelvis through the labial veins (Fig. 4.7b) or from the perforating vein at the back of the thigh (Fig. 4.8b).
-
Perforating vein of the adductor canal (formerly Dodd; Fig. 4.8a).
-
Connecting vein between the anterior accessory vein and great saphenous vein in the mid thigh (Fig. 4.7c).
-
Paratibial perforating veins (especially formerly Boyd; Fig. 7.48b).
-
Intersaphenous vein between the small and great saphenous veins in the calf (Fig. 4.9b).
-
Connecting vein between the posterior arch vein and the great saphenous vein in the distal calf (Fig. 4.8c).
Uncommon reflux sources into the great saphenous vein:
-
Perforating vein from the deep femoral vein approx. 5–10 cm below the groin
-
Distal perforating vein of the adductor canal (formerly Hunter)
-
Paratibial perforating vein after thrombosis
-
Perforating vein directly from the tibia after a tibia fracture; Sect. 9.10)
Special attention must be paid to these sites when examining the great saphenous vein from proximal to distal. They may be the main proximal reflux source or an additional source of proximal pathological flow. If this second variant is overlooked prior to a saphenofemoral ligation, then recurrence is inevitable because the refluxive inflow into the great saphenous vein has not been completely eradicated. This commonly occurs with a refluxive perforating vein of the adductor canal (formerly Dodd) or with reflux into the great saphenous vein through the posterior accessory saphenous vein.
A situation may occur called reflux without source (Mendoza 2002 in Appendix 2). This is where the saphenofemoral junction is competent, but many healthy tributaries drain retrograde along the downward course of the great saphenous. This causes an increasing volume of reflux to build up without a definite source. The reflux in this situation does not come from the deep system but only from the tributaries. The diameter of the great saphenous vein and the reflux volume remain small (Fig. 7.49 and Sect. 3.3.4).

Reflux without source according to Cappelli and Franceschi. The terminal valve of the great saphenous vein (GSV) remains competent. Blood from healthy tributaries, including the posterior and anterior accessory saphenous veins, drain progressively into the great saphenous vein in a retrograde fashion. There is no pathological connection with the deep system. The reflux curves are of small volume but progressively increase down the great saphenous vein (shown on the right at three different stages, SSV small saphenous vein) (online material)
Copyright: [Author]
7.5.2.2 Identifying the Reflux Drainage from the Great Saphenous Vein
Reflux may leave the great saphenous vein in several places. Tributaries and perforating veins are usually involved.
Almost all the visible, dilated perforating veins down the course of the great saphenous vein may serve as re-entry points for reflux (Sects. 3.4 and 9.3). If the refluxive section of the great saphenous vein ends at one of these perforating veins, then this can be established as the distal reflux drainage point (Fig. 7.50).

(a) Transverse view through the inner thigh at the height of the perforating vein of the adductor canal (formerly Dodd). The terminal and preterminal valves are incompetent with a refluxive great saphenous vein from the groin. This is draining through the perforating vein back into the deep vein. There are no refluxive tributaries present. This is classified as a complete incompetence of the great saphenous vein (GSV), Hach Class II. This was a concurrent finding during the examination of the leg of a subject with post-traumatic varicose veins in the calf (Fig. 9.14). The groin reflux was not apparent clinically because this recirculation did not include any varicose tributaries. The perforating vein of the adductor canal runs slightly distal. For this reason the image shows the competent great saphenous vein as well as the dilated perforating vein which carries the reflux to the deep vein. The connection between the two is shown with a dotted line as it is not in the plane of this image. The reflux is indicated by yellow arrows. (b) Transverse view through the upper third of the calf. The tibial edge is shown on the left. The great saphenous vein is incompetent above and below the knee with a refluxive tributary (trib) leaving the great saphenous vein just above the proximal paratibial perforating vein (formerly Boyd). This is classified as a complete incompetence of the great saphenous vein, Hach Class III (additional material online). The reflux in the great saphenous vein ends in the perforating vein which carries the majority of the reflux volume back into the deep system. (c) Same position as (b) shown in colour duplex
Copyright: [Author]
Multiple drainage points are not usually visible on phlebography. For this reason Hach always stated that the varicose tributary was the lowest reflux drainage point when using his classification. A draining perforating vein on the great saphenous vein is present in 47 % of legs with incompetence. Additional refluxive tributaries are usually, but not necessarily, associated with this recirculation circuit.
Reflux is drained exclusively through tributaries in 53 % of recirculations involving the great saphenous vein. These then carry their reflux back through perforating veins or the small saphenous vein and into the deep veins. These tributaries are usually clinically visible on the surface of the leg as varicose veins.
In an unpublished study where 82 consecutive legs with great saphenous reflux were examined with duplex (Table 7.2), 48 (59 %) were found to have only one refluxive tributary which drained all the reflux from the great saphenous vein (Fig 7.51a). In 32 % of the legs, there were two refluxive tributaries, in 8 % the vein was drained by 3 tributaries and in 1 % by 4. The most distal tributary in each case was the distal reflux drainage point. The great saphenous veins were all competent below this point, by definition, down to the ankle. An alteration in the calibre of the great saphenous vein is usually found at the distal reflux drainage point (Fig. 7.51c).

Junction of a single tributary draining the great saphenous vein (GSV). (a) Transverse view through the inner thigh demonstrating the refluxive tributary in colour duplex. The refluxive great saphenous vein is visible in the saphenous eye where it fills a tributary. Below this point the great saphenous vein is competent. This is a complete incompetence of the great saphenous vein, Hach Class II. The colour “overloads” the image causing the vein to appear much larger than the one in B scan (black outline) (additional material online). (b) Transverse view below the refluxive tributary. The great saphenous vein is competent and the tributary is refluxive. At the end of muscular systole, the flow in the great saphenous vein is still antegrade (blue) while it is already refluxive (red) in the tributary (Left). When the patient stands still, there is no flow in both these veins (Right) (additional material online). (c) Calibre reduction below the branch point of the refluxive tributary in a patient with complete incompetence of the great saphenous vein in the thigh, Hach Class II. On the left the diameter of the great saphenous vein is 4.8 mm, on the right it is 2.9 mm
Copyright: [Author]
7.5.2.3 Identifying the Number of Refluxive Segments of the Great Saphenous Vein
A refluxive tributary may refill the great saphenous vein lower down where the flow is antegrade causing it to reflux once more (Sect. 4.1.3). Thus, all parts of the great saphenous vein below the first competent segment must be examined. In 16 % of incompetence in the great saphenous vein, there is a competent section between the proximal reflux source and the distal re-entry point. This is where a refluxive tributary takes the reflux away from the great saphenous vein and carries it back into the great saphenous vein further down the leg (Fig. 4.11a).
7.5.2.4 Identifying a Draining Perforating Vein Along the Refluxive Course
For those who use the CHIVA method of treatment, it is important to differentiate the shunt types. If there is a perforating vein draining the refluxive segment of the great saphenous vein (shunt type I), the proximal reflux source should be interrupted. The saphenous vein will then drain via this perforating vein. If there is no perforating vein (shunt type III), manual tributary occlusion will arrest the retrograde flow in the saphenous trunk. This is a shunt type 3 where the proposed treatment is to ablate or ligate only the tributary and leave the saphenofemoral junction intact. Apart from an examination in B scan, a simple test can clarify this situation (Figs. 7.52 and 4.23). A velocity profile is first taken in the proximal region of the refluxive great saphenous vein in PW mode during a Wunstorf manoeuvre. The refluxive tributary close to its junction with the great saphenous vein is then compressed with a finger without compressing the great saphenous vein at the same time (Fig. 4.23). Then, the Wunstorf manoeuvre is repeated. If antegrade flow is present in the proximal great saphenous vein, this confirms that the vein itself is not compressed by the finger. If there are no draining perforating veins between the probe and the compressed tributary, no reflux will be recorded, after the brief antegrade curve. Directly after the digital compression of the tributary is released, reflux will resume (Mendoza 2002 in Appendix 2; Zamboni et al. 2010). In Fig. 7.52, there were two refluxive tributaries which were compressed with two fingers and released one at a time.

Transverse view through the thigh with PW recordings of the velocity profile of the great saphenous vein. The great saphenous vein is refluxive with two draining tributaries which were compressed digitally by the examiner. Starting from the left, movement artefacts occurred only as the subject raised and lowered his toes with the provocation manoeuvre. Tributary occlusion seems to control the saphenous reflux. At the yellow arrow and the red arrow, digital compression of the proximal and distal tributaries were released, respectively. Both resulted in gross saphenous reflux. It may be concluded that there are no draining perforating veins on the great saphenous vein because, if there were, tributary compression would not have controlled the reflux
Copyright: [Author]
7.5.3 Pulsatility Within the Great Saphenous Vein
If the subject sits on the edge of a couch with the legs in a dependent position, antegrade flow will soon commence within an incompetent great saphenous vein. Closer inspection will reveal that this flow is pulsatile (Lattimer et al. 2012a). It was suggested that the more marked the pulsation, the more pathological the chronic venous insufficiency of the leg (Fig. 7.53).

Spontaneous saphenous pulsation, neither dependent on respiration nor synchronous with the cardiac cycle, is a marker for advanced chronic venous insufficiency. Pulsation is detected in the great saphenous vein of a dependent leg in a patient with chronic venous insufficiency after about 1–2 min
Copyright: [Author]
Two out of 44 legs with healthy veins (4.5 %) presented spontaneous pulsation in the great saphenous vein. In contrast 75 % of legs with refluxive great saphenous vein presented pulsation. Pulsation also correlates with clinical findings. In the absence of visible veins or skin alterations, pulsation is found in the great saphenous vein in 4.5 % of cases and in 94.1 % of cases with vein-related skin alterations. The presence of pulsation also correlates with the diameter in the middle third of the thigh. With no pulsation the average diameter of the great saphenous vein was 3.5 mm. With pulsation the average diameter was 7 mm.
References
Coleridge-Smith P, Labropoulos N, Partsch H, Myers K, Nicolaides A, Cavezzi A (2006) Duplex ultrasound investigation of the veins in chronic venous disease of the lower limbs-UIP consensus document, part I. Basic principles. Eur J Vasc Endovasc Surg 31:1–10
Kalodiki E, Stvrtinova V, Allegra C et al (2012) Superficial vein thrombosis: a consensus statement. Int Angiol 31:203–216
Lattimer CR, Azzam M, Kalodiki E, Makris G, Geroulakos G (2012a) Saphenous pulsation on duplex may be a marker of severe chronic superficial venous insufficiency. J Vasc Surg 56(5):1338–1343
Lattimer CR, Kalodiki E, Azzam M et al (2012b) Volume displacements from an incompetent great saphenous vein during a standardised Valsalva manoeuvre. Acta Phlebologica 13(1):25–30
Lattimer CR, Kalodiki E, Azzam M, Geroulakos G (2013) Reflux time estimation on air-plethysmography may stratify patients with early superficial venous insufficiency. Phlebology 28(2):101–108
Lurie F, Kistner RL, Eklof B, Kessler D (2003) Mechanism of venous valve closure and role of the valve in circulation: a new concept. J Vasc Surg 38:955–961
Mendoza E, Blättler W, Amsler F (2013) Great saphenous vein diameter at the saphenofemoral junction and proximal thigh as parameters of venous disease class. Eur J Vasc Endovasc Surg 45(1):76–83
Mühlberger D, Morandini L, Brenner E (2009) Venous valves and major superficial tributary veins near the saphenofemoral junction. J Vasc Surg 49:1562–1569
Oswald M (2005) Our blue wonder. To be read at: www.ourbluewonder.com
Pascarella L, Al-Tuwaijri M, Bergan JJ, Mekenas LM (2005) Lower extremity superficial venous aneurysms. Ann Vasc Surg 19(1):69–73
Platzer W (2005) Taschenatlas der Anatomie. Stuttgart, Thieme
Stücker M, Moritz R, Altmeyer P, Reich-Schupke S (2013) New concept: different types of insufficiency of the saphenofemoral junction identified by duplex as a chance for a more differentiated therapy of the great saphenous vein. Phlebology 28(5):268–274
Zamboni P, Gianesini S, Menegatti E, Tacconi G, Palazzo A, Liboni A (2010) Great saphenous varicose vein surgery without saphenofemoral junction disconnection. Br J Surg 97:820–825
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2014 Springer-Verlag Berlin Heidelberg
About this chapter
Cite this chapter
Mendoza, E., Morrison, N., Lattimer, C.R. (2014). Examination of the Great Saphenous Vein. In: Mendoza, E., Lattimer, C., Morrison, N. (eds) Duplex Ultrasound of Superficial Leg Veins. Springer, Berlin, Heidelberg. https://doi.org/10.1007/978-3-642-40731-4_7
Download citation
DOI: https://doi.org/10.1007/978-3-642-40731-4_7
Published:
Publisher Name: Springer, Berlin, Heidelberg
Print ISBN: 978-3-642-40730-7
Online ISBN: 978-3-642-40731-4
eBook Packages: MedicineMedicine (R0)