
Abstract
Electroencephalography is a commonly used tool for presurgical evaluation of epilepsy patients. In this paper, we present a quantitative evaluation of interictal high frequency oscillations (HFOs) in scalp Electroencephalographies (EEGs) for epileptogenic region localization. We process multichannel EEGs using time-frequency spectral analysis in order to detect HFOs in each EEG channel. Comparison between the results of time-frequency analysis and visual assessment is performed to verify the reliability of time-frequency analysis. Later, \(t\)-test and Pearson correlation analysis are performed to analyze the relationships between ictal HFOs and interictal HFOs. The high correlations between interictal and ictal HFOs imply that interictal HFOs, like ictal HFOs, are valuable in localizing the epileptogenic region. As a result, scalp interictal HFOs are valuable in epileptogenic region localization for presurgical evaluation of epilepsy patients. It holds great potential for reducing the long delay before patients can be referred for surgery.
Access provided by Autonomous University of Puebla. Download conference paper PDF
Similar content being viewed by others


Keywords
1 Introduction
Epilepsy is a common neurologic disorder affecting more than 1 % of the world population. Although antiepileptic drug (AED) is the most popular treatment of epilepsy, 40 % of epilepsy patients are pharmacoresistant. For these patients with pharmacoresistant seizures, surgery is a highly effective treatment instead of AED. However, a successful epilepsy surgery necessitates the accurate delineation of the epileptogenic region. Reliable biomarkers are needed to identify potential surgical candidates and localize the epileptogenic regions as early as possible after AED fails. A commonly used biomarker is the interictal EEG spike, which however is not reliable for localizing the extent of an epileptogenic region because it is difficult to differentiate two types of interictal epileptic discharges: those originating from the ictal onset zone; and those propagated from other regions or irritative regions [5, 11].
High frequency oscillations (HFOs) are oscillatory activities on EEG above 25 Hz. HFOs can be subgrouped into gamma waves, ripples, and fast ripples, etc. A gamma wave is a pattern of neural oscillation in humans with a frequency range between 25 and 100 Hz, though 40 Hz is prototypical. Ripple is HFO in the 80–200 Hz range, reflecting inhibitory field potentials, which synchronize neuronal activity [3]. HFOs of 250–600 Hz, which are referred to as fast ripples (FRs), are pathologic signals reflecting summated action potentials of spontaneously bursting neurons [3].
Clinical studies using direct brain recordings during presurgical evaluation have found ripples and FRs to be valuable in identifying the epileptogenic region [2, 3]. It has also been shown in [5, 11] that HFOs, with or without interictal spikes, are more reliable in identifying epileptogenic region than interictal spikes alone and even more reliable than ictal onset in determining the extent of brain tissue that must be resected.
HFOs in patients with focal epilepsies have been reported with ECoG recordings [9, 10]. In [6], HFOs’ changes have been extracted based on a simple statistics of time-frequency representation. In [8], a reviewer-dependent approach for detection of HFOs has been proposed. In [4], HFOs have been detected using swarmed neural-network features.
Till recently, HFOs analysis has been confined to ECoG, which has limited its utility as a biomarker. Analysis of scalp EEG has demonstrated possibility to detect HFOs from scalp EEGs [1, 7]. In [1], Andrade-Valenca et al. have studied scalp EEGs recordings of 15 patients with focal epilepsy, and analyzed the rates of gamma waves (40–80 Hz) and ripples (\({>}\)80 Hz) by visually rating the number of spikes, gamma waves, and ripples per minute for each channel of scalp EEGs. However, inspecting the bulky multi-channel EEG data visually is very tedious and time-consuming. In another work [7], HFOs in scalp EEGs recorded during slow-wave sleep (CSWS) have been investigated through visual analysis as well as time-frequency spectral analysis. However, the reliability of using the scalp EEG to identify the epileptogenic region is still an open question.
In this paper, we present a quantitative evaluation of HFOs in scalp EEGs in localizing epileptogenic region. Following [7], the quantitative analysis is based on a time-frequency spectral analysis of scalp EEGs recorded from 6 epilepsy patients. Comparison between the results of time-frequency analysis and visual assessment is performed to verify the reliability of time-frequency analysis. Furthermore, we use paired \(t\)-test and Pearson correlation analysis to look for relationships between the frequency-power characteristics of ictal and interictal HFOs. The results of \(t\)-test demonstrate significant differences between ictal and interictal HFOs in both values of peak frequency and corresponding power. This fact implies that the HFOs can be valuable for differentiating the ictal and interictal states. The Pearson correlation analysis shows high correlations between ictal and interictal HFOs. The high correlations imply that interictal HFOs, similar to ictal HFOs, hold potential in localizing the epileptogenic region.
Our results demonstrate the potential of using interictal HFOs of scalp EEGs as a biomarker of noninvasive localization of the epileptogenic region. The HFOs in interictal EEG are quite promising for detecting the epileptogenic region once it is proved to be reliable. The interictal EEGs have many advantages in localizing the epileptogenic region compare to ictal EEGs. They have less muscle artifacts. Moreover, they make it possible to diagnose epilepsy without waiting subsequent seizures and long-term presurgical evaluation. Thus, the findings in this paper would help to justify earlier surgical treatment and thereby reduce the long delay before patients are referred for surgery [2].
2 Methods
2.1 EEGs Recording
The EEGs recording was conducted at the KK Women’s and Children’s Hospital (KKH), Singapore. We recruited those pediatric epileptic patients with informed consent obtained from their guardians. The patients were subject to the standard video-EEG monitoring in the epilepsy monitoring unit (EMU) of KKH. Long-term EEGs were recorded by 32 electrodes placed on scalp according to the international 10–20 system. All data were stored on a hard disk with 256 or 512 sampling rate.
The subjects recruited so far are 27 patients with diagnosis of different types of seizures. We focus only on focal seizure in this study. After careful assessment by the EEG technologist, 6 epileptic patients aged between 5 and 12 years (3 male, 3 female) are selected for this analytic work with 44 seizure events and frequently occurred HFOs in both ictal and interictal states. The related information of the patients are listed in Table 1.
2.2 Visual Assessment of EEGs
Each patient's EEGs are assessed visually. Seizure events are identified from the standard video-EEG system by a EEG technologist. EEGs are marked as ictal or interictal periods. In addition, some of the visible HFOs are also marked. The conventional EEG traces (10 s per page) are initially reviewed to identify the ictal events, as shown in Figs. 1a and 2a. Then, the traces are temporally expanded to 2 s per page in order to study the details of activity faster than 25 Hz (see Figs. 1b and 2b).

Ictal EEGs of P025 (sampling rate 512 Hz): the above row is after 0.5–198 Hz bandpass filtering, the below row is after 20–198 Hz bandpass filtering. a P025 ictal EEGs with 10 s window. b P025 ictal EEGs with 2 s window

Interictal EEGs of P006 (sampling rate 256 Hz): the above row is after 0.5–98 Hz bandpass filtering, the below row is after 20–98 Hz bandpass filtering. a P006 interictal EEGs with 10 s window. b P006 interictal EEGs with 2 s window
In interictal period, the HFOs are relatively clear, as shown in Fig. 2. But due to the large amount of artifacts during ictal state, the HFOs cannot be found easily by visual checking as in Fig. 1. We need to extract HFOs from EEG back ground noises in order to further study HFOs in epileptic EEGs.
2.3 Time-Frequency Analysis
We investigate the time evolution of the high-frequency power spectrum of the ictal and interictal activity by applying the Gabor transform, which is the Fourier transform with a sliding Gaussian window. For EEGs with 256 Hz sampling rate, we apply Fourier transform with a 500 ms wide Gaussian window (contains 128 data points, the frequency resolution is 2 Hz) and 10–100 Hz frequency range to the raw EEG data. For EEGs with 512 Hz sampling rate, we apply Fourier transform with a 250 ms wide Gaussian window (contains 128 data points, the frequency resolution is 4 Hz) and 10–200 Hz frequency range. All computations are performed using a program written in-house for MATLAB 2010a (MathWorks Inc., Natick, MA).
3 Results
3.1 Comparison of Time-Frequency Analysis and Visual Assessment
A typical example of ictal EEGs which contains HFOs is shown in Fig. 1, and a typical example of interictal EEGs containing HFOs is shown in Fig. 2. We show the signal with both 10 and 2 s window respectively. Red circles in the figures are used to mark out the visually inspected HFOs.
For the HFOs marked in Fig. 1, we plot the spectrograms of the corresponding channels: Fp2-F8, F8-T4, T4-T6, as shown in Fig. 3.

Time-frequency spectrograms of EEGs in ictal state of P025, with sampling rate of 512 Hz, and bandpass filtering of 20–198 Hz. a Fp2-F8. b F8-T4. c T4-T6
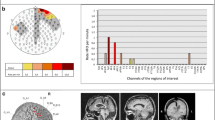
For the HFOs marked in Fig. 2, we plot the spectrograms of the corresponding channels: Fp2-F8, F8-T4, T4-T6, as shown in Fig. 4.

Time-frequency spectrograms of EEGs in interictal state of P006, with sampling rate of 256 Hz, and bandpass filtering of 20–98 Hz. a Fp2-F8. b F8-T4. c T4-T6
HFOs are identified as clearly visible red spectral spots with frequencies faster than 20 Hz that are surrounded by an area of low power. From Figs. 3 and 4, we can find the clear red spots at the same time points of visually marked red circles in Figs. 1 and 2. This indicates that time-frequency analysis obtains reliable results as visual assessment.
3.2 Relationship of Ictal HFOs and Interictal HFOs
We compare the frequencies and power values of the HFO peaks in the spectrograms of interictal period with those of ictal period. For each event (a period of ictal HFOs or interictal HFOs, according to one spectrogram), we pick the point with highest value in the spectrogram, and record the corresponding value (power) and frequency of that point. Then, for each patient with several events, we compute the average value of all events’ power and frequency.
The average peak frequency and corresponding power value of ictal HFOs and interictal HFOs of each patient are shown in the 6th and 7th column of Table 2. The frequencies and powers of the total 6 patients are then analyzed using a paired \(t\)-test and Pearson correlation analysis between ictal HFOs and interictal HFOs.
For paired \(t\)-test, relationships are considered statistically significant if \(p<0.05\). From the result of Table 2, HFOs detected during ictal period have significantly higher frequencies (\(p=0.0328\)) and more power (\(p=0.0423\)) than those detected during interictal period. This provides us evidence that HFOs can be used to differentiate interictal and ictal state for seizure detection.
For Pearson correlation analysis, larger Pearson correlation coefficient (range between [0,1]) implies higher correlation between two data sets. From the result of Table 2, the Pearson correlation coefficients are computed. Results \(\gamma =0.7808\) for frequency and \(\gamma =0.7550\) for power are obtained, which indicates that the frequencies and powers in interictal HFOs and ictal HFOs are highly correlated.
We also demonstrate in Table 2 that the channels involved in ictal HFOs (column 4) and interictal HFOs (column 5) are similar, which indicates that HFOs largely remain in the same region during interictal and ictal periods.
4 Conclusion
In this paper, we presented a quantitative evaluation of interictal scalp EEG for Epileptogenic Region Localization. The analysis was based on time-frequency spectral analysis of scalp EEG recorded from 6 epilepsy patients. The results of time-frequency analysis and visual assessment were compared to verify reliability of the time-frequency analysis. A paired \(t\)-test of peak frequencies and powers between ictal HFOs and interictal HFOs demonstrated that ictal HFOs had significantly higher frequencies (\(p=0.0328\)) and more power (\(p=0.0423\)) than interictal HFOs. Pearson correlation analysis demonstrated high correlations (\(\gamma =0.7808\) for frequency and \(\gamma =0.7550\) for power) between ictal and interictal HFOs. In conclusion, scalp interictal HFOs could be considered as an effective biomarker in epileptogenic region localization. In further study, investigations based on larger dataset using more advanced methods are worth performing.
References
Andrade-Valenca LP, Dubeau F, Mari F, Zelmann R, Gotman J (2011) Interictal scalp fast oscillations as a marker of the seizure onset zone. Neurology 77:524–531
Cendes F, Engel J (2011) Extending applications for high-frequency oscillations. Neurology 77:518–519
Engel JJ, Bragin A, Staba R, Mody I (2009) High-frequency oscillations: what is normal and what is not? Epilepsia 50:598–604
Firpi H, Smart O, Worreli G, Marsh E, Dlugos D, Litt B (2007) High-frequency oscillations detected in epileptic networks using swarmed neural-network features. Ann Biomed Eng 35(9):1573–1584
Jacobs J, LeVan P, Chander R, Hall J, Dubeau F, Gotman J (2008) Interictal high-frequency oscillations (80–500 Hz) are an indicator of seizure onset areas independent of spikes in the human epileptic brain. Epilepsia 49:1893–1907
Kobayashi K, Jacobs J, Gotman J (2009) Detection of changes of high-frequency activity by statistical time-frequency analysis in epileptic spikes. Clin Neurophysiol 120:1070–1077
Kobayashi K, Watanabe Y, Inoue T, Oka M, Yoshinaga H, Ohtsuka Y (2010) Scalp-recorded high-frequency oscillations in childhood sleep-induced electrical status epilepticus. Epilepsia 51:2190–2194
Le-Van-Quyen M (2007) bragin, A.: Analysis of dynamic brain oscillations: methodological advances. Trends Neurosci 30:365–373
Valderrama M, Quyen MV (2011) High-frequency oscillations and interictal spikes in partial epilepsy: joining the benefits. Clin Neurophysiol 122(1):3–4
Zijlmans M, Jacobs J, Kahn YU, Zelmann R, Dubeau F (2011) Ictal and interictal high frequency oscillations in patients with focal epilepsy. Clin Neurophysiol 122:664–671
Zijlmans M, Jacobs J, Kahn Y, Zelmann R, Dubeau F, Gotman J (2011) Ictal and interictal high frequency oscillations in patients with focal epilepsy. Clin Neurophysiol 122:664–671
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2014 Springer-Verlag Berlin Heidelberg
About this paper
Cite this paper
Pan, Y., Guan, C., Eng, HL., Ge, S.S., Ng, Y.l., Chan, D.W.S. (2014). Quantitative Evaluation of Interictal High Frequency Oscillations in Scalp EEGs for Epileptogenic Region Localization. In: Sun, F., Li, T., Li, H. (eds) Knowledge Engineering and Management. Advances in Intelligent Systems and Computing, vol 214. Springer, Berlin, Heidelberg. https://doi.org/10.1007/978-3-642-37832-4_38
Download citation
DOI: https://doi.org/10.1007/978-3-642-37832-4_38
Published:
Publisher Name: Springer, Berlin, Heidelberg
Print ISBN: 978-3-642-37831-7
Online ISBN: 978-3-642-37832-4
eBook Packages: EngineeringEngineering (R0)