
Abstract
Sports provide physical, psychological, and social well-being to individuals. However, there may be a potentially damaging effect on articular cartilage with mid- and long-term exposure to sports. This chapter is aimed to critically review the existing literature regarding the association between sports participation and ankle osteoarthritis. This review demonstrates that in general, there is not enough evidence to conclude that sports increase the risk of ankle osteoarthritis. The existing literature related to this topic is scarce, and most of the studies have not controlled the risk analysis for the presence of other potentially associated risk factors for ankle osteoarthritis. Further research is needed on this topic with prospective comparative studies controlling for, at least, age, sex, body mass index, occupational workload, and previous ankle injuries.
Access provided by Autonomous University of Puebla. Download reference work entry PDF
Similar content being viewed by others

Introduction
Sports participation has clear benefits on social, psychological, and biological health and can be, therefore, generally recommended to patients. However, there have been some concerns on whether sport participation will damage the articular cartilage or not. Specifically, some studies have indicated an increased risk of hip and knee osteoarthritis from sports participation (Vingard et al. 1993; Deacon et al. 1997; Cooper et al. 1998; Vingard et al. 1998; Lane et al. 1999; Sandmark and Vingard 1999; Cheng et al. 2000; Lau et al. 2000; Kettunen et al. 2001), especially at the elite level (Lindberg et al. 1993; Vingard et al. 1995; Shepard et al. 2003; Schmitt et al. 2004). Although some researchers have suggested an increased risk of ankle osteoarthritis (Fig. 1) in sports as well (Brodelius 1961; Solonen 1966), the evidence for this association is not clear. In addition, there are many factors that may increase the risk of osteoarthritis in athletes that are not always controlled in the comparative analysis (Kohatsu and Schurman 1990; Imeokparia et al. 1994; Olsen et al. 1994; Thelin et al. 2006; Ratzlaff et al. 2011). Theoretically, to know the real effects of sports itself on the risk of ankle osteoarthritis, it is necessary to control for potentially associated risk factors for the development of osteoarthritis.


Ankle osteoarthritis
The purpose of this chapter is to provide a comprehensive and critical review of the existing literature regarding studies investigating the relationship between sports and the risk of ankle osteoarthritis.
Review of Evidence
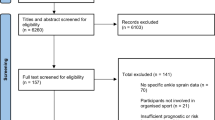
There are only few studies investigating the effects of sports participation on the development of ankle osteoarthritis. Only 12 studies were found, from which 2 case series were excluded (Andersson et al. 1989; Drawer and Fuller 2001). Thus, ten studies were finally included. Sports investigated in these studies include soccer, running, dance, and high jumping. All investigations were level III-evidence (cross-sectional or retrospective case-control) studies, except the one published by Panush et al. (1995).
Running
There are three studies investigating the effects of running on ankle osteoarthritis. Panush et al. compared the prevalence of hip, knee, and ankle osteoarthritis between 17 male runners (mean age 56 years) and 18 male non-runners (mean age 61 years) (Panush et al. 1986). Runners (53 % marathoners) exercised a mean of 28 miles per week for a mean of 12 years, corresponding to a mean lifetime mileage of 17,343 miles. The comparison of runners and non-runners was ankle pain 12 % and 5 %, respectively; osteophytes per subject 2.2 and 1.8, respectively; cartilage thickness 3 and 3.1 mm, respectively; and radiographic degenerative joint disease 0 % for both groups (all nonsignificant differences). This study was not influenced by differences in age, sex, body weight, and occupational workload, and history of joint injury was not controlled. The same group published some years later the 8-year follow-up of this sample (Panush et al. 1995). Twelve runners (42 % marathoners) and ten non-runners were available for follow-up (mean age 63 and 68 years, respectively). In this case, the quantification of running exposition was mean running time of 22 years, mean of 22 miles per week, and mean of lifetime mileage of 25,168. The authors found no significant differences in terms of ankle pain, range of motion, swelling, or radiographic osteoarthritis between runners and non-runners. The statistical analysis comparing runners and controls was not adjusted for many of the associated risk factors for osteoarthritis. In addition, the sample size was small and 20 % of runners and 10 % of controls were exposed to different other physical activities.
The effects of running on the risk of ankle osteoarthritis have been also evaluated by Konradsen et al. (1990). The authors compared clinical and radiographic hip, knee, and ankle osteoarthritis in 27 male orienteering runners (median age 58 years) and 27 matched controls (median age 57 years). Running exposition was mean of 40 years, median mileage of 21–42 km per week (depending on the age of the subjects), and percentage of mileage run as competition between 10 % and 16 % (depending on the age of the subjects). The researchers found no significant between-group differences in terms of ankle pain, alignment, range of motion, osteophytes, cartilage thickness, or radiographic degenerative joint disease. Interestingly, this study was conducted controlling for many of the important associated risk factors for osteoarthritis (age, sex, weight, and occupational workload). Although not formally controlled, previous ankle injury probably had no influence on the results. The limitations in this study may be the small sample size, the poorly detailed statistical analysis, and the fact that inactive runners were excluded from this study.
Soccer
Two studies have investigated the effects of soccer on ankle osteoarthritis. Brodelius was among the first to investigate the relationship between sports and ankle osteoarthritis (Brodelius 1961). The author compared 34 male soccer players (aged 21–46 years) and 16 female dancers (aged 18–39 years) with 195 control subjects with regard to radiographic ankle osteoarthritis. Exposition to sports was 5–20 years for soccer players and 3–30 years for dancers. Brodelius showed higher prevalence of ankle osteoarthritis in athletes compared with controls. In controls, osteoarthritis increased with age, but was not related to sex. Radiographic signs occurred in 33 of 34 soccer players and 14 of 16 dancers. In soccer players, 13 of 15 subjects with previous ankle injury had radiographic signs of ankle osteoarthritis. The study controlled previous injuries, age, and sex but not other important risk factors. In addition, the definition of ankle osteoarthritis was only based on radiographs. Given the design and details of this study, the most important conclusion was that overuse and injury were associated with ankle osteoarthritis, rather than sports itself increased the risk of osteoarthritis.
Ankle osteoarthritis in soccer players was also studied by Solonen (Solonen 1966). The author reported a clinical and radiological study comparing hip, knee, and ankle osteoarthritis in 60 male soccer players (mean age 26 years) and 40 control subjects (mean age 41 years). Male soccer players had 5–23 years of experience (mean 13 years). Controls were not exposed to soccer. Twenty-two percent of soccer players had abnormal ankle range of motion, but some of them had severe ankle injuries or ankle sprains. Radiographic evaluation was only possible in 36 soccer players and demonstrated 92 % of severe radiographic changes of ankle osteoarthritis, compared with 20 % in the control group. The study has several limitations: lack of inferential comparative statistics, important differences in mean age between groups, likely influence of previous ankle injuries on the risk of ankle osteoarthritis, and lack of control for other important associated risk factors (occupational workload or obesity). The lack of inferential between-group statistical comparison prevents any strong conclusion regarding the risk of ankle osteoarthritis from soccer participation.
American Football
Vincelette et al. presented a comparative study of foot and ankle radiographic osteoarthritis between 59 professional American football players and 50 age-matched control subjects (Vincelette et al. 1972). The sample characteristics were all males, mean age 23 years for players and 23 years for controls. Football exposure was a mean of 9.5 years in the players group. No controls had ever played football. The author found that mild signs of osteoarthritis, periarticular “new bone,” dorsal osteophytes of the talus, and interosseous ligament calcification in the players and control groups were 30 % and 6 %, 47 % and 20 %, 20 % and 10 %, and 32 % and 2 %, respectively. For severe changes, the corresponding values were 63 % and 0 %, 29 % and 0 %, 61 % and 2 %, and 32 % and 2 %, respectively. In this study, no statistical comparison was reported, although the differences appear to be clinically relevant. The study did not adjust for body mass index or previous injuries. Occupational workload was not controlled, but may not be an issue in this case given that players were young professionals.
Volleyball
Gross and Marti reported a comparative study on ankle osteoarthritis comparing 22 former elite volleyball players and 19 healthy age-matched untrained controls (Gross and Marti 1999). Players had a mean age of 34 years (36 years in the control group) and had played during an average of 5.5 h per week for 8.5 years. Most volleyball players had an injury (ankle sprain, lateral ligament ruptures, or mechanical instability) and eight underwent surgical repair. While subchondral sclerosis and osteophytes were significantly more prevalent in volleyball players than in controls, the difference in joint space narrowing was not significant. No severe grades of ankle osteoarthritis could be observed in the former elite volleyball players. The authors only found that anterior drawer sign and functional instability were significant and independent predictors of an increased radiological index for ankle osteoarthritis. In contrast, career length, intensity as volleyball player, clinical signs of ankle instability, and age were not independent predictors of ankle osteoarthritis. The authors concluded that volleyball could not be considered an independent risk factor for ankle osteoarthritis.
Dance
In addition to the study previously reviewed by Brodelius involving ballet dancers (Brodelius 1961), van Dijk and co-workers reported a case-control study aimed to investigate the risk of hip, ankle, subtalar, and first metatarsophalangeal joint osteoarthritis in a similar sample (van Dijk et al. 1995). The authors assessed 19 female ex-ballet dancers (mean age 59 years) with a mean duration of their career of 37 years (mean time of dance per week of 45 h) and 19 female controls. The authors found significantly higher prevalence of ankle osteoarthritis in ballet dancers compared with controls. This study was controlled by age, sex (only females included), height, and weight, but not for occupational workload and previous injury, among others. Of particular concern is that all ballet dancers had previous joint injuries, although no details on the type of injuries were reported. Forty-seven percent of control subjects had been exposed to recreational sports for an average of 2 h per week for 8 years.
High Jumping
Schmitt et al. studied the prevalence of clinical and radiographic ankle osteoarthritis in 40 former elite male high jumpers (mean age 42 years, mean years of retirement 16) at least 10 years after retirement from competition compared with 40 age-, sex-, and body mass index-matched controls. The characteristics of sport exposition were duration of career mean 10 years, training 18 h per week, strength training 5 h per week, jumps per week 716, and sports after retirement 4 h per week. Training history was obtained with the aid of questionnaires. The researchers found a significant negative correlation between the number of jumps during the active carrier and radiological scores, with no radiological differences between the takeoff and swinging leg. Athletes did not have more ankle osteoarthritis compared with the matched controls. Severe joint space narrowing was rare in former athletes. Joint injuries in the past were related to a poorer radiological score, i.e., increased signs of osteoarthritis. The authors were not able to demonstrate that high jumpers had an increased risk of ankle osteoarthritis. The study had some limitations: associated risk factors for osteoarthritis were not controlled, statistics for radiographic changes not detailed, and exposure to other sports after retirement.
Combination of Sports
There is one study that included information on ankle osteoarthritis in athletes of different sports. Kujala et al. published a national population-based study comparing the cumulative 21-year incidence of hospital admissions for hip, knee, and ankle osteoarthritis between 2,049 male athletes who had represented Finland in international events during 1920 and 1965 and 1,403 controls previously classified as healthy at the age of 20 years (Kujala et al. 1994). Athletes were divided into endurance (long-distance running, cross-country skiing), team (soccer, ice hockey, basketball, track and field), and power (boxing, wrestling, weight lifting, throwing) sports. The authors found that the percentage of ankle osteoarthritis in endurance, team, and power sports was 0 %, 0.6 %, and 0.4 %, respectively, and 0 % in the control subjects. The authors also reported the odds ratio for osteoarthritis in the athletes compared with controls, but this information was unfortunately not specified for ankle osteoarthritis. However, it is unlikely that there were significant differences in the risk of ankle osteoarthritis between athletes and controls (only nine athletes were admitted to the hospital for ankle osteoarthritis in the studied period). Therefore, it might be concluded that sports do not increase the risk of ankle osteoarthritis. Some additional limitations included the lack of control for history of joint injury, the absence of matched controls for some sports (ice hockey, basketball, weight lifters), and the lack of information for sport exposure. In addition, considering only hospital admissions for osteoarthritis may miss other patients with less severe cases of osteoarthritis not seeking treatment and not in need of surgical treatment.
Discussion
Osteoarthritis is a prevalent disorder in many countries, and this may be explained, at least in part, by a longer life expectancy. It is likely that the presence of other risk factors plays an important role in the etiology of osteoarthritis. Some researchers have suggested a damaging effect of sports on the articular cartilage of the ankle (Brodelius 1961; Solonen 1966). However, the analysis of a specific risk factor must be performed taking into account that other risk factors are influencing the risk of osteoarthritis for the studied risk factor. Thus, the primary goal of this chapter is to provide a comprehensive and critical review of the existing literature regarding studies investigating the relationship between sports and the risk of ankle osteoarthritis. The principal findings of this review are as follows: (1) the literature investigating the association is limited; (2) most of the existing studies have not controlled the risk analysis for the presence of other potentially associated risk factors for ankle osteoarthritis; and (3) in general, there is not enough evidence to conclude that sport increases the risk of ankle osteoarthritis.
The most important limitations were the lack of control for other potential risk factors for osteoarthritis; the retrospective or cross-sectional nature of most of the studies; the limited information on the length of follow-up, as well as relatively short follow-up when this information was provided; and a lack of specific quantification of the exposure to sports. Some of the existing studies are case series with lack of a control group (Andersson et al. 1989; Drawer and Fuller 2001), which means that the risk of osteoarthritis from sports participation cannot be assessed. Regarding the type of studies, none of them were prospective in nature. Studies with level III evidence (case-control or cross-sectional) do not provide a strong causal-effect relationship between sports and ankle osteoarthritis. Also, follow-up should be long enough to establish the real effects of sports on articular cartilage. In terms of the potential influence of other risk factors, it is important to understand that ankle osteoarthritis may be related to many factors, including, but not limited to, older age, female sex, obesity, osteoporosis, occupation, sports activities, previous joint injury, muscle weakness or dysfunction, proprioceptive deficit, lower limb malalignment, leg-length inequality, and genetic factors (Felson et al. 2000; Hunter et al. 2002; Aluoch and Wao 2009; Bosomworth 2009; Neogi and Zhang 2011). As the presence of any of these factors in an athlete may increase the risk of osteoarthritis rather than the exposure to sports itself, the risk analysis for each sport should be controlled for the presence of as many of these factors as possible. There are some potentially associated risk factors that may have major relevance, like age, sex, weight, occupational workload, and previous injuries (Kohatsu and Schurman 1990; Imeokparia et al. 1994; Felson et al. 2000; Hunter et al. 2002; Thelin et al. 2006; Aluoch and Wao 2009; Bosomworth 2009; Neogi and Zhang 2011).
The present review differentiates between studies controlling three or less of these important risk factors or those controlling four or five of them. Table 1 summarizes the evidence for each sport depending on the quantity of risk factors controlled. None of the reviewed studies have controlled or considered all of these factors simultaneously. As shown, only the study by Konradsen et al. controlled many of the important risk factors (Konradsen et al. 1990). Only previous injuries were not completely controlled in their study, as there were three patients with injuries (although one of them was excluded from the comparative analysis). From these studies, one may conclude that running does not increase the risk of ankle osteoarthritis. The evidence for the other sports (American football, volleyball, high jumping, and ballet) is too limited (only one study in each sport) to draw clear conclusions. Soccer could not be included in Table 1 because no statistical comparison was provided (Brodelius 1961; Solonen 1966), and accordingly so no clear conclusions can be drawn. In general, five of seven studies concluded that sports were not related to ankle osteoarthritis.
Conclusions
-
The literature investigating the association between sports and ankle osteoarthritis is limited.
-
Most of the existing studies have an insufficient control of potential associated risk factors for osteoarthritis (age, gender, body mass index, occupational workload, and previous ankle injuries).
-
In general, there is not enough evidence to conclude that sports increase the risk of ankle osteoarthritis.
-
The limited evidence available for sports participation and risk of ankle osteoarthritis refers to running, soccer, American football, volleyball, high jumping, and ballet.
-
Running, even in subjects with high cumulative lifetime mileage, is not associated with increased risk of ankle osteoarthritis.
-
The evidence for soccer, American football, volleyball, high jumping, and ballet is too limited to draw any clear conclusion.
-
The evidence suggesting that soccer increases the risk of ankle osteoarthritis is too limited to draw any conclusions.
-
Future research is clearly needed before any strong conclusions can be stated about ankle osteoarthritis and sports participation.
References
Aluoch MA, Wao HO (2009) Risk factors for occupational osteoarthritis: a literature review. AAOHN J 57:283–290
Andersson S, Nilsson B, Hessel T, Saraste M, Noren A, Stevens-Andersson A, Rydholm D (1989) Degenerative joint disease in ballet dancers. Clin Orthop Relat Res 238:233–236
Bosomworth NJ (2009) Exercise and knee osteoarthritis: benefit or hazard? Can Fam Physician 55:871–878
Brodelius A (1961) Osteoarthrosis of the talar joints in footballers and ballet dancers. Acta Orthop Scand 30:309–314
Cheng Y, Macera CA, Davis DR, Ainsworth BE, Troped PJ, Blair SN (2000) Physical activity and self-reported, physician-diagnosed osteoarthritis: is physical activity a risk factor? J Clin Epidemiol 53:315–322
Cooper C, Inskip H, Croft PR, Campbell L, Smith G, McLaren M, Coggon D (1998) Individual risk factors for hip osteoarthritis: obesity, hip injury, and physical activity. Am J Epidemiol 147:516–522
Deacon A, Bennell K, Kiss ZS, Crossley K, Brukner P (1997) Osteoarthritis of the knee in retired, elite Australian rules footballers. Med J Aust 166:187–190
Drawer S, Fuller CW (2001) Propensity for osteoarthritis and lower limb joint pain in retired professional soccer players. Br J Sports Med 35:402–408
Felson DT, Lawrence RC, Dieppe PA, Hirsch R, Helmick CG, Jordan JM, Kington RS, Lane NE, Nevitt MC, Zhang Y, Sowers M, McAlindon T, Spector TD, Poole AR, Yanovski SZ, Ateshian G, Sharma L, Buckwalter JA, Brandt KD, Fries JF (2000) Osteoarthritis: new insights. Part 1: the disease and its risk factors. Ann Intern Med 133:635–646
Gross P, Marti B (1999) Risk of degenerative ankle joint disease in volleyball players: study of former elite athletes. Int J Sports Med 20:58–63
Hunter DJ, March L, Sambrook PN (2002) Knee osteoarthritis: the influence of environmental factors. Clin Exp Rheumatol 20:93–100
Imeokparia RL, Barrett JP, Arrieta MI, Leaverton PE, Wilson AA, Hall BJ, Marlowe SM (1994) Physical activity as a risk factor for osteoarthritis of the knee. Ann Epidemiol 4:221–230
Kettunen JA, Kujala UM, Kaprio J, Koskenvuo M, Sarna S (2001) Lower-limb function among former elite male athletes. Am J Sports Med 29:2–8
Kohatsu ND, Schurman DJ (1990) Risk factors for the development of osteoarthrosis of the knee. Clin Orthop Relat Res 261:242–246
Konradsen L, Hansen EM, Sondergaard L (1990) Long distance running and osteoarthrosis. Am J Sports Med 18:379–381
Kujala UM, Kaprio J, Sarna S (1994) Osteoarthritis of weight bearing joints of lower limbs in former elite male athletes. BMJ 308:231–234
Lane NE, Hochberg MC, Pressman A, Scott JC, Nevitt MC (1999) Recreational physical activity and the risk of osteoarthritis of the hip in elderly women. J Rheumatol 26:849–854
Lau EC, Cooper C, Lam D, Chan VN, Tsang KK, Sham A (2000) Factors associated with osteoarthritis of the hip and knee in Hong Kong Chinese: obesity, joint injury, and occupational activities. Am J Epidemiol 152:855–862
Lindberg H, Roos H, Gardsell P (1993) Prevalence of coxarthrosis in former soccer players. 286 players compared with matched controls. Acta Orthop Scand 64:165–167
Neogi T, Zhang Y (2011) Osteoarthritis prevention. Curr Opin Rheumatol 23:185–191
Olsen OE, Vingard E, Koster M, Alfredsson L (1994) Etiologic fractions for physical work load, sports, and overweight in the occurrence of coxarthrosis. Scand J Work Environ Health 20:184–188
Panush RS, Schmidt C, Caldwell JR, Edwards NL, Longley S, Yonker R, Webster E, Nauman J, Stork J, Pettersson H (1986) Is running associated with degenerative joint disease? JAMA 255:1152–1154
Panush RS, Hanson CS, Caldwell JR, Longley S, Stork J, Thoburn R (1995) Is running associated with osteoarthritis? An eight-year follow-up study. J Clin Rheumatol 1:35–39
Ratzlaff CR, Steininger G, Doerfling P, Koehoorn M, Cibere J, Liang MH, Wilson DR, Esdaile JM, Kopec JA (2011) Influence of lifetime hip joint force on the risk of self-reported hip osteoarthritis: a community-based cohort study. Osteoarthr Cart 19:389–398
Sandmark H, Vingard E (1999) Sports and risk for severe osteoarthrosis of the knee. Scand J Med Sci Sports 9:279–284
Schmitt H, Brocai DRC, Lukoschek M (2004) High prevalence of hip arthrosis in former elite javelin throwers and high jumpers. 41 athletes examined more than 10 years after retirement from competitive sports. Acta Orthop Scand 75:34–39
Shepard GJ, Banks AJ, Ryan WG (2003) Ex-professional association footballers have an increased prevalence of osteoarthritis of the hip compared with age matched controls despite not having sustained notable hip injuries. Br J Sports Med 37:80–81
Solonen KA (1966) The joints of the lower extremities of football players. Ann Chir Gynaecol Fenn 55:176–180
Thelin N, Holmberg S, Thelin A (2006) Knee injuries account for the sports-related increased risk of knee osteoarthritis. Scand J Med Sci Sports 16:329–333
van Dijk CN, Lim LSL, Poortman A, Strubbe EH, Marti RK (1995) Degenerative joint disease in female ballet dancers. Am J Sports Med 23:295–300
Vincelette P, Laurin CA, Lévesque HP (1972) The footballer’s ankle and foot. Can Med Assoc J 107:873–877
Vingard E, Alfredsson L, Goldie I (1993) Sports and osteoarthritis of the hip. An epidemiologic study. Am J Sports Med 21:195–200
Vingard E, Sandmark H, Alfredsson L (1995) Musculoskeletal disorders in former athletes. A cohort study in 114 track and field champions. Acta Orthop Scand 66:289–291
Vingard E, Alfredsson L, Malchau H (1998) Osteoarthrosis of the hip in women and its relationship to physical load from sports activities. Am J Sports Med 26:78–82
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2015 Springer-Verlag Berlin Heidelberg
About this entry

Cite this entry
Alentorn-Geli, E., Samuelsson, K., Karlsson, J. (2015). Sports Participation and Risk of Ankle Osteoarthritis. In: Doral, M.N., Karlsson, J. (eds) Sports Injuries. Springer, Berlin, Heidelberg. https://doi.org/10.1007/978-3-642-36569-0_193
Download citation
DOI: https://doi.org/10.1007/978-3-642-36569-0_193
Published:
Publisher Name: Springer, Berlin, Heidelberg
Print ISBN: 978-3-642-36568-3
Online ISBN: 978-3-642-36569-0
eBook Packages: MedicineReference Module Medicine