
Abstract
The practice of ankle arthroscopy is constantly evolving. The very nature of the techniques generated and the published literature available mean that surgical procedures can often gain and lose popularity among surgeons in equal measures and directly influence their practices worldwide. This chapter aims to educate the reader on current techniques being generated around ankle arthroscopy but also to provide balanced opinions based on clinical expertise and the evidence-based medicine available. It may not be an exhaustive appraisal of every technique but focuses on major conditions and procedures performed. It is possible that in 5 years, techniques may change again for newer discoveries or revert back to more established methods, the classic example being the original Broström procedure. The generation of diverse biomaterials can lead to technique changes that are not applicable to every surgeon due to practicing laws in certain countries, but despite these restrictions, it is hoped that readers will find the content beneficial.
Access provided by Autonomous University of Puebla. Download reference work entry PDF
Similar content being viewed by others


Brief History of Ankle Arthroscopy
Arthroscopy is now well established as a technique utilized by foot and ankle surgeons worldwide. The roots of arthroscopy date back to the early twentieth century when in 1912 a Danish doctor, Dr. Severin Nordentoft, used a laparoscope traditionally utilized in internal medicine to inspect the internal aspect of a knee joint. It is widely believed he attributed the term arthroscopy to this technique. Derived from Greek phraseology “arthro” means joint and “scope” is a reference to the phrase to see, to observe, or to view. In 1918 a Japanese professor, Kenji Takagi, used cystoscopes to visualize the interior of a knee joint, and he has been credited as the pioneer of joint arthroscopy. He further developed the technique, appreciating the different diameter sizes of arthroscopes and also varying viewing angles, on which modern-day instruments are based. Around this time a young American resident named Michael Burman began using arthroscopies in anatomy laboratories in 1931 and after travels to Europe from New York reported on his experience with arthroscopy of multiple joints, mainly hips and knees because the ankle was often considered too small to access. Part of the reasoning for this was the congruent nature of the ankle joint. As an effective hinge-type synovial joint with the axis of movement around the intermalleolar axis allowing mainly plantar flexion and dorsiflexion, many anatomists agreed the joint was just too restricted in its dimensions to use the arthroscope effectively. But it was Takagi in 1939 who then described a systematic approach to examine an ankle with an arthroscope. What followed in the postwar era was the development of endoscopic instruments using fiber optics by Masaki Watanabe who popularized this technique using previously described portals on the anterior and posterior aspects of the ankle. Many surgeons worldwide have, since then, described and popularized a variety of surgical techniques, including modifications of patient positioning during surgery, different portal placements, and different procedures, all of which have been derived in some way from the pioneering work by Nordentoft, Takagi, and colleagues.
This chapter aims to educate the reader on new approaches and developments in ankle arthroscopy and surgical techniques in the ankle. The breadth of this subject is extremely vast, and the subjects discussed here could be referred to as controversial, topical, or evolving but are all the subject of wide variation in technique practices among surgeons across the globe.
Osteochondral Defects of the Ankle Joint: Introduction
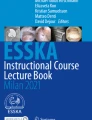
Ankle injuries account for probably more joint injuries among athletes than any other (Nelson et al. 2007), and the incidence of osteochondral lesions of the talus (OLT) in this population can be up to 30 % (Aktas et al. 2008). The classification of these lesions was popularized by Berndt and Harty in 1959 (Berndt and Harty 1959) (Fig. 1), but many more classification systems exist, including the more up-to-date MRI classification described by Hepple et al. (1999). The Berndt and Harty classification was expanded in 2001 by Scranton and McDermott (2001) who added a type V describing a subchondral bone cyst with intact overlying cartilage, thus postulating retrograde drilling may be a suitable intervention. Raikin proposed a further expansion to the classification system in 2004 describing “massive” defects of >3,000 mm3 suitable for allograft reconstruction (Raikin 2004). Distal tibial osteochondral lesions are comparably rare, reportedly occurring in <3 % of 880 ankle arthroscopies (Mologne and Ferkel 2007). This may be due to the different mechanical properties of the tibial cartilage being stiffer than that of the talus (Athanasiou et al. 1995) or the relative concavity of the tibial surface being less prone to injury than the convex talus.


The Berndt and Harty classification of talar osteochondral defects. (I) Subchondral compression (fracture). (II) Partial detachment of osteochondral fragment. (III) Completely detached fragment without displacement from fracture bed. (IV) Detached and displaced fragment
Treatment options for OLTs can be complex. Below is a guide to some current treatment options:
-
Nonoperative treatment
-
Immobilization in a cast or boot
-
Medication (NSAIDs)
-
Functional bracing
-
Intra-articular injections
-
Steroid/local anesthetic
-
Viscosupplementation injections (hyaluronic acid)
-
Platelet-rich plasma injections
-
Mesenchymal stem cell injections
-
-
Electrical/electromagnetic stimulation
-
Ultrasound stimulation
-
-
Operative treatment
-
Cartilage cap fixation
-
Retrograde drilling of cystic defects
-
Bone marrow stimulation/microfracture
-
Chondral/osteochondral transplantation/implantation
-
Mosaicplasty
-
Osteochondral autologous transfer system (OATS)
-
Autologous cancellous bone grafting (e.g., iliac crest)
-
Autologous chondrocyte implantation (ACI)
-
Collagen-induced autologous chondrocyte implantation (CACI)
-
Matrix-induced autologous chondrocyte implantation (MACI)
-
Membranes
-
Three-dimensional scaffolds
-
-
-
Osteochondral allograft transfer system (including particulated juvenile cartilage allograft transplantation)
-
Synthetic biodegradable scaffolds
-
-
Many of these surgical procedures, such as bone marrow stimulation and autologous or allograft tissue transfer systems, are well established in orthopedic practice. Marrow stimulation techniques are probably the gold standard to treat smaller primary OLTs <1.5 cm (Chuckpaiwong et al. 2008) with good results commonly seen in around 80–85 % of patients (Zengerink et al. 2010). OATS/mosaicplasty/autologous cancellous bone grafting techniques requiring cartilage/osseous transfer have the added potential complication of donor site morbidity ranging from 0 % to 50 % (Valderrabano et al. 2009; Zengerink et al. 2010); however, they still produce good outcomes in around 80–90 % of patients in published series (Hangody et al. 2001; Valderrabano et al. 2009; Imhoff et al. 2011; Woelfle et al. 2013). Bulk allograft tissue transfers have been well documented, especially in larger defects, as described by Raikin (2004). For both moderate and large defects, case series reports do tend to show an improvement in AOFAS scores and relatively low rates of graft problems, which is certainly encouraging for what is a difficult condition to manage that otherwise may require joint arthroplasty or arthrodesis (Hahn et al. 2010; El-Rashidy et al. 2011).
The Evolution of Autologous Chondrocyte Implantation (ACI) Procedures
The changes over the years in the development of cellular transplantation for cartilage defects in the ankle are quite complex. The following is a brief description of each step along the evolutionary pathway to the development of all-arthroscopic techniques for cartilage regeneration in the ankle.
First-Generation ACI
The first published use of ACI techniques was in the knee using a two-stage procedure to harvest the local cartilage and then delaying the reimplanting of the cultured chondrocytes under a periosteal patch (Brittberg et al. 1994). This technique was later adopted in the ankle joint to treat osteochondral lesions of the talus, incorporating host cancellous bone graft as a scaffold to fill bony defects if necessary and then covering the defect with periosteal patches (Giannini et al. 2001). Following this early work, ACI has been used with good success with positive outcomes generally possible in 70–92 % of cases (Koulalis et al. 2002; Whittaker et al. 2005; Baums et al. 2006; Giannini et al. 2009a; Nam et al. 2009; Zengerink et al. 2010). The technique, however, does require two separate operations, and, depending on the size and location of the talar lesion, autologous cancellous bone graft may be necessary and a malleolar osteotomy may be required (van Bergen et al. 2011).
The use of structural bone graft to support the chondrocyte suspension is variably reported in the literature. Peterson et al. recommended bone grafting for ACI in lesions deeper than 5–6 mm, while Choi et al. reported worse outcomes following bone marrow stimulation in lesions deeper than 7 mm and Angthong et al. in lesions deeper than 7.8 mm (Petersen et al. 2003; Choi et al. 2009; Angthong et al. 2013). This first-generation technique was substantiated as a rational technique on discovery that the regenerated cartilage cap over the original OCL demonstrated features of hyaline cartilage in part rather than the typical fibrocartilage seen following other techniques (Browne et al. 2005; Whittaker et al. 2005; Giannini et al. 2008).
Second-Generation ACI
First-generation ACI is a technically challenging procedure with difficulties encountered in retaining the chondrocytes under the periosteal patch and suturing/attaching the periosteal patch, leading to the development of hypertrophy within the surrounding cartilage border (Henderson et al. 2006), delamination, or calcification that may require debridement. Alleviating these difficulties and reducing the need for autologous tissue, collagen membranes were developed to replace the periosteal patch. An example of these collagen membranes is a bilayer construct of porcine types I and III collagen, with a porous surface allowing adhesion and cellular invasion into the collagen matrix and a compact cell-occlusive surface preventing extrusion of any contents into the joint (Brittberg 2010) (Fig. 2).


Porcine collagen matrix (types I/III collagen) (Chondro-Gide®, Geistlich Surgery, Wolhusen, Switzerland)
These collagen-induced autologous chondrocyte implantation (CACI) membranes proved popular in knee surgery and were shown to reduce the symptoms and problems associated with chondral hypertrophy (Bartlett et al. 2005, 2006; Gomoll et al. 2009). Isolated use of a collagen membrane in ankle surgery to contain chondrocytes without MACI technology (see below) has not been frequently reported. There are recent reports, however, of the use of this so-called second-generation technology collagen bilayer membrane to contain spongiosa bone grafts instead of chondrocyte suspensions. The distinct advantage of this technique is the need for only one operation and the harvesting of “mesenchymal stem cells” from the iliac crest as precursors to differentiation into stable chondral cells (Valderrabano et al. 2013). In this study, 26 patients received a modified autologous matrix-induced chondrogenesis (AMIC®), effectively a sealing of an autograft OCL with the collagen membrane. They demonstrated a significant improvement in AOFAS scores (60–89, p < 0.01) and increased participation in sports postoperatively.
Third-Generation ACI
The next step in the evolution of chondrocyte implantation was to incorporate the cultured cells directly onto the collagen membrane before reimplantation in a fashion similar to an ACI technique but with the use of fibrin glue to secure the membrane to the OLT. The need for autologous bone graft under the membrane is determined by the surgeon and is carried out as required prior to membrane attachment. This method of treatment is commonly referred to as matrix-induced autologous chondrocyte implantation (MACI).
The membrane provides a biological environment that allows chondrocyte adherence and integration into the collagen fibers. Cellular activity has been demonstrated showing synthesized matrix containing proteoglycans and type II collagen despite low oxygen tension in the chondrocytes. On the collagen membrane, the chondrocytes show the ability to redifferentiate and also migrate through the fibrin glue toward the normal host subchondral bone. This migration creates an environment for a heterogeneous mix of immature mesenchymal and chondral cells that can lead to increased proliferation of chondrocytic tissue. The numbers of chondrocytes forming and proliferating on the membrane are of sufficient density to allow for cellular apoptosis at quite high rates; however, the remaining cells are viable, expressing normal phenotypic behavior and potentially lead to development of normal hyaline cartilage (Brittberg 2010).
MACI procedures traditionally utilize the same methods as the first- and second-generation techniques (Ronga et al. 2005; Dixon et al. 2011). The difference is that once the cartilage biopsy is processed to isolate the chondrocytes from the extracellular matrix, these cells are then seeded directly onto an absorbable purified membrane ready for reimplantation on the OLT. These techniques still do have the disadvantage, however, of requiring two operations with potential donor site morbidity. Currently, cartilage cells are more often harvested from either the rim of the OLT or the anterior aspect of the talus (Anders et al. 2012; Johnson et al. 2013) or potentially from the detached piece of cartilage from the original OLT (Giannini et al. 2005b).
There are no publications comparing the outcomes of second- and third-generation techniques in treating OLTs. Bartlett et al. published a randomized controlled trial comparing CACI and MACI in the knee and reported no significant difference in function at 1 year between the two groups, although the trend was for a larger improvement in the MACI group, with good or excellent results in 72.3 % MACI versus 59.1 % CACI (Bartlett et al. 2005).
Case series of MACI in the talus tend to vary with regard to the severity of the lesions and whether or not there was a need for autologous structural bone graft under the membrane; however, in general, in line with other ACI techniques, there is a tendency to significantly improve functional scores such as the AOFAS postoperatively (Schneider and Karaikudi 2009; Anders et al. 2012). Worth noting though is that in some reports, the technique was used for small lesions that would probably be better treated with less demanding procedures such as microfracture with arguably similar outcomes (Giza et al. 2010).
Collagen/Hyaluronic Acid-Based Scaffolds
The next step in the use of the MACI membranes was the use of membrane as a three-dimensional scaffold (Giannini et al. 2008) to contain the cultured chondrocytes. Examples of such technology used include BioSeed®-C and chondrotissue® (BioTissue Technologies, Freiburg, Germany) (Fig. 3), NOVOCART® 3D (Tissue Engineering Technologies, Reutlingen, Germany), Hyalograft C (Anika Therapeutics, Bedford, MA, withdrawn from the market at time of writing), and the earlier discussed Chondro-Gide® (Geistlich Surgery, Wolhusen, Switzerland). Studies using these scaffolds are discussed later.


Chondrotissue®, BioTissue Technologies, Freiburg, Germany
These scaffolds tend to feature a porous structure that allows a uniform diffusion and arrangement of the cultured chondrocytes, supporting cell migration. In comparison to the two-dimensional membranes, these newer structures are thought to enhance cellular organization, proliferation, and thus maintained cellular viability. The enhanced volume of the three-dimensional structure also allows the scaffold to act as a void-filler (to a certain degree), potentially negating the need for a cancellous allograft/autograft. The need for a talar structural graft clearly depends on the depth of the OCL. Some of the manufacturers guide the surgeon in deciding whether or not a graft is required. With the use of NOVOCART® 3D, an autologous spongiosa graft is recommended if the defect exceeds 7 mm in depth; the manufacturers of BioSeed®-C suggest using two scaffolds on top of one another for deep defects or autologous graft if needed. The BioSeed®-C scaffolds are up to 2 mm thick. In short, there are no specific guidelines for all scaffolds, and the surgeon will decide if a graft is needed below the scaffold.
Gel-Type Autologous Chondrocyte Implantation
The potential advantage of this type of scaffold is the ease of application of a gel to exactly match the size of the defect in all dimensions. As discussed later, this type of technology has been adapted to generate single-stage all-arthroscopic surgery in the ankle. Lee et al. described a two-stage technique using the calcaneocuboid joint as the harvest site (they reported no morbidity with this technique) (Lee et al. 2013). The series, performed with a declared interest from the manufacturers, looked at 38 patients, 11 of whom had previous interventions for OCLs. The lesions had mean widths and lengths of 12 and 16 mm, respectively; 85 % required medial malleolar osteotomy for access. After OCL preparation, the chondrocytes were mixed with a thrombin/fibrin gel (Chondron®, Sewon Cellontech Co, South Korea) and injected into the defect and allowed to harden for 5 min. AOFAS scores improved from 71 ± 14 preoperatively to 91 ± 12 at 24 months. Ninety-five percent of patients had a second-look arthroscopy at 12 months, with 21/36 showing fissuring of cartilage and seven a flap of cartilage, but only two either loose or displaced lesions. There were two delayed unions and one nonunion of medial malleolar osteotomies. Interestingly, the authors reported that three of six subchondral cysts had filled in on follow-up MRI at 24 months. Despite the seemingly high rates of abnormal cartilage on follow-up arthroscopy, the authors still reported that 75 % of the patients had normal/near-normal cartilage.
Synthetic Bone Substitutes in the Treatment of Osteochondral Lesions of the Talus
The development of synthetic bone substitutes has many potential advantages over current techniques of tissue transfer systems. Allograft donor tissue has the potential for graft rejection, although this is unlikely (Phipatanakul et al. 2004; Meehan et al. 2005), but immunologic response to the tissue can increase the presence of catabolic enzymes such as metalloproteinases (MMPs) and reduce the proteoglycan content of the allograft, which could lead to structural change and arthritis (Giannini et al. 2010). There is also the potential for degradation and questionable viability of the transplanted cartilage tissue (Marco et al. 1992; Williams et al. 2004), especially if the graft is frozen and not fresh osteochondral tissue. Allograft can also be prohibitively expensive and limited in its availability considering that exact size-matching is required in most cases. Autograft tissue requires a donor site, and this introduces the potential for donor site morbidity.
The ideal solution is, therefore, to perform one operation, potentially arthroscopically, requiring no donor site harvesting with a material that will provide structural support and allow regeneration of normal hyaline cartilage. This solution would ideally have a three-dimensional profile rather than a flat membranous profile.
Calcium Sulfate/Polymer-Based Scaffold
The introduction of three-dimensional scaffolds designed to mimic normal anatomy allows treatment of osteochondral cystic lesions without bone grafting. Creating a stable interface between the cartilage and bone using an osteoconductive material allows gradual integration of host matrix. One product available is BioMatrix™ CRD (Arthrex Naples Florida, USA) (Fig. 4), but it is not substantiated by any in vivo clinical trials yet. This is a biphasic bovine type 1 collagen and β-tricalcium phosphate with polylactic acid. A product recently withdrawn from the market is a synthetic composite material of polylactide-co-glycolide, calcium sulfate, and polyglycolide fibers (TRUFIT Plug, Smith and Nephew, Andover, Massachusetts). Purported benefits were a functional scaffold for chondrogenic and osteogenic cells and residual resorption of the synthetic scaffold being replaced by a functional matrix (Gao et al. 2005; Pearce et al. 2012). Results with the TRUFIT have been mixed, with one small series involving patients with failed primary microfracture surgery or large primary cystic lesions showed a significant improvement in the functional rating scales with a reasonably high satisfaction overall but questionable reintegration of the graft on T2 sequencing MRI mapping (Pearce et al. 2012). An earlier study of failed microfracture surgery, however, demonstrated implant failure clinically and radiologically in active military personnel, with failed integration on MRI and continued pain in the ankle (Garcia et al. 2010). Although Carmont et al. recommended waiting 24 months for integration of the implant (Carmont et al. 2009), other series in knee surgery also showed problems with graft integration (Sgaglione and Florence 2009).


Three-dimensional synthetic scaffolds (Arthrex BioMatrix™ CRD)
Two-Stage All-Arthroscopic Surgery for Osteochondral Defects of the Talus
The use of the ACI scaffolds, although the harvesting of chondral tissue was still required, was thought to be a huge step forward in terms of the development of chondral tissue replacement, partly because they heralded the introduction of all-arthroscopic techniques in the ankle.
In 2008, using a HYAFF 11 (benzylic ester of hyaluronic acid)-based scaffold, Giannini et al. published their results of an all-arthroscopic technique for treating OCLs (Giannini et al. 2008). Forty-six patients with type II/IIa (Giannini et al. 2005a) lesions, some over 2 cm2, were treated with a two-stage arthroscopic procedure (the first to harvest chondral tissue from the detached OCL or taken from the tibia or periphery of the lesion and the second to attach the scaffold). The surgeries were a mix of primary and revision procedures, and five patients required a bone graft (not clear if done arthroscopically). The AOFAS scores significantly improved at 36 months (p < 0.005), and there was no difference in outcomes in those who required bone grafting. Twenty of twenty-nine athletes resumed to same level of sports. The authors also performed second-look arthroscopies in three patients and found evidence on histology of presence of all the components of hyaline cartilage, which was very encouraging.
Aurich et al. described a similar procedure in 2011 (Aurich et al. 2011). Using a chondrocyte-loaded three-dimensional matrix (ARTHROMATRIX, Orthogen Pty Ltd, Melbourne, Australia), they treated 14 patients with defects up to 6 mm deep and 3 cm2. Patients showed a significant improvement in AOFAS and pain scores at a mean of 24.5 months follow-up, but 9 of 18 sports persons returned to the same level of sports. On MRI assessment using the MOCART (magnetic resonance observation of cartilage repair tissue) scores, they found that the signal intensity was the same as adjacent cartilage in 2 patients, had slight alteration in 12, and had large alterations in 5. Other studies also have shown heterogeneous signal patterning (Nam et al. 2009).
Magnan et al. used a MACI HYAFF 11 (Verigen, Leverkusen, Germany) scaffold to treat 30 patients with primary lesions 1.5–4 cm2 (Magnan et al. 2012). Again, patients required a two-stage procedure, the first to harvest the chondral tissue. Twenty-five had an all-arthroscopic approach, three required malleolar osteotomies for large posteromedial lesions, and two had conversion to anterior arthrotomies because of failed arthroscopic procedures (learning curve). At a mean follow-up of 45 months, the AOFAS scores improved significantly from 36.9 to 83.9 postoperatively with good/excellent results in 28. In four recurrent lesions, biopsies showed fibrocartilage rather than hyaline cartilage in contrast to the findings by Giannini et al. (2013).
One-Stage Arthroscopic Surgery for Osteochondral Defects of the Talus
The techniques described in the previous sections involve more than one surgical procedure. There is also a significant cost factor to consider when harvesting chondrocytes to culture for implantation. Harvesting also can be associated with donor site morbidity. These factors have led to the evolution of single-stage arthroscopic solutions.
The use of concentrated bone marrow contents as a source of mesenchymal stem cells enables differentiation into cells of differing lineages such as chondrocytes and osteoblasts while catering for matrix growth with the necessary mechanical stability, because autologous bone marrow cells contain precursor cells for regeneration of hyaline cartilage but also growth factors necessary for neoangiogenesis (Funayama et al. 2008; Chang et al. 2013). Such techniques have been shown to provide good results compared to microfracture techniques when used in an equine model to regenerate cartilage in defects. There also usually is a higher type II collagen and essential glycosaminoglycan content with bone marrow aspirate driven cartilage (Fortier et al. 2010). Valderrabano et al. applied iliac crest spongiosa grafts, rich in marrow cells, to talar defects and covered the graft with a collagen membrane; however, this necessitated open surgical techniques (Valderrabano et al. 2013).
Combining bone marrow aspirate with a scaffold matrix is now the latest development being used as a single-stage arthroscopic procedure to treat osteochondral defects of the talus.
Giannini et al. first published their results in 2009 and later in 2013 (Giannini et al. 2009b, 2013). They used two different methods of application of the marrow concentrate. The first 23 patients had marrow aspirate mixed with collagen powder (Spongostan, Johnson and Johnson, UK) and platelet gel; the remaining 26 were treated with a hyaluronic acid membrane (Fidia Advanced BioPolymers, Italy), platelet gel, and the marrow concentrate. The sizes of the talar lesions were 2.24 ± 1.23 cm2 with a depth of 3.9 ± 0.9 mm. Nine of the 49 patients had prior treatment for the OCL. After 4 years there was a significant improvement in AOFAS scores (63.73 ± 14.13 to 82.19 ± 17.04), but there was a decrease in AOFAS scores between 24 and 48 months. Seventy-eight percent of athletes returned to the same level of sports. Detailed MRI at 24 months (in 20 patients) including T2 lesion mapping and MOCART scoring demonstrated 45 % had complete filling of the defect and 45 % had hypertrophic changes. The subchondral bone was also disrupted in 65 %. Interestingly, they failed to demonstrate any correlation between clinical scores at 48 months and negative changes on MRI.
Using a similar concept, Miller and Schon (2012) combined microfracture techniques with application of a collagen paste (Flowable Wound Matrix, Integra LifeSciences) mixed with a centrifuged iliac crest bone marrow aspirate. The mixture was inserted through a dry arthroscopy portal and held in place with fibrin glue. The report supplies only anecdotal evidence of encouraging results, but clearly this is another important step taken, similar to that of Lee et al. (2013) in the development of readily available, cost-friendly, easily implantable scaffolds for the treatment of OCLs.
The future of osteochondral defect repair will depend on the clinical results of techniques used. Herein lies the problem. There are no randomized, indeed, no comparative controlled trials using different implants. Trials are invariably retrospective surgeon series. The need for high-quality, randomized controlled trials is clearly evident, but the development of single-stage arthroscopic techniques is still a major advancement in treating talar OCLs.
Osteochondral Defects of the Talus: New Resurfacing Implant Techniques
The use of HemiCAP® resurfacing implants (Arthrosurface Inc., Franklin, MA, USA) (Fig. 5) has been popular in orthopedic surgical procedures such as first metatarsal resurfacing for hallux rigidus (Aslan et al. 2012), patellar resurfacing for isolated lesions (Davidson and Rivenburgh 2008), and proximal humeral resurfacing for glenohumeral pathology (Delaney et al. 2014). The management of large medial talar osteochondral defects is challenging, and this technology is now being investigated by foot and ankle surgeons as a potential solution to the problem.


The HemiCAP® talus implant (Arthrosurface, Franklin, USA)
The concern over the use of resurfacing implants is the alteration of the geometry and surface contour of the articular surface and an alteration in the distribution of forces over the joint. This could potentially lead to increasing pain and disability in the joint and early or catastrophic failure of the implant because of increased contact pressures (Loening et al. 2000; Custers et al. 2007). Alternatively subsidence of the implant can lead to destruction and collapse of the surrounding cartilage (Milentijevic and Torzilli 2005). This is especially true in the ankle joint because of its high congruence and significant forces being constantly transmitted with weight bearing, although the cartilage in the ankle does have different biomechanical and biological properties than in other joints (Treppo et al. 2000). The natural response of the ankle’s talar cartilage is to compress on weight bearing as measured by a contact strain of between 30 % and 40 % in cartilage 1.4–1.5 mm thick (Li et al. 2008; Wan et al. 2008; Van Ginckel et al. 2011). The position of the implant is thus critical to ensure good position with the surrounding cartilage surface.
To test the implant and its optimal position, Van Dijk et al. performed a cadaver study in 2010 in which they inserted 11 implants of varying offsets and sizes (van Bergen et al. 2010). The implants are suitable for osteochondral defects of around 15 mm in circumference (the implants had been manufactured previously based on geometric data collected at the authors’ institution from computed tomography scans of 52 patients with talar osteochondral defects). The main reason for choosing 15 mm as a limiting size is the general consensus in the literature suggesting that lesions larger than 15 mm are less likely to respond well to primary arthroscopic treatment such as microfracture (Choi et al. 2009; Zengerink et al. 2010). A medial malleolar osteotomy was performed to expose the talus (Seil et al. 2001). Using the appropriate instrumentation, the implant was inserted onto the talus ensuring the best position relative to the contour of the talus and depth relative to adjacent cartilage. Contact pressures were measured using a thin pressure-sensitive film inserted in the tibiotalar joint. After the talus was removed from the ankle, the level of the implant was checked relative to the cartilage with a digital caliper with a resolution of 0.01 mm. Out of 15 available offset sizes, six were used in the study. The lateral part of the implant was found to be recessed by a mean of 0.57 mm (standard deviation 0.16 mm). The medial part was recessed by a mean of 0.03 mm (standard deviation 0.40 mm). The central part was inspected visually and was recessed in 10 and protruding in one. The contribution of “prosthesis area” before implantation to the total joint pressure was 3.3 % and after implantation it was 0.09 % in the recessed specimens. In the protruding specimen it was 44 %.
This cadaver study showed that the procedure is reproducible; however, it definitely has some limitations. The authors recognized the limitations, including the elderly cohort of cadavers who do not routinely suffer from osteochondral defects, the static loading methods which do not represent the true mechanics of the cartilage under physiological dynamic loading, and the fact that the tibia was loaded in isolation and not with the fibula. The slightly recessed position (0.5 mm below the surface) of the implant was shown to be “optimal” with regard to the proposed changes of the surrounding surface with weight bearing and the compressibility of the cartilage.
Initial clinical reports emerged in 2011 by the same investigators of the cadaver study. A single case report of a 20-year-old female athlete with a 17 × 8 × 8 mm medial talar dome lesion demonstrated “considerable reduction in pain and resumption of playing korfball at a competitive level.” The AOFAS score improved from 74 preoperatively to 90 postoperatively.
The same authors then followed up on this case report and published a prospective study in 2012 (van Bergen et al. 2012) that included 15 patients with osteochondral defects on the medial talar dome averaging 15.7 mm ± 2.9 mm (anteroposterior direction) and 9.2 mm ± 3.1 mm (medial lateral direction), with symptoms lasting >1 year following previous surgery of varying types from bone grafting to debridement and bone marrow stimulation. Using the Berndt and Harty classification, there were 13 stage 5 lesions, 1 stage 3 lesion, and 1 unclassifiable (Berndt and Harty 2004). The operations were performed in a similar manner to that described above. Patients were kept in a plaster cast for 2 weeks postoperatively, after which time full range of motion was allowed with non-weight bearing in a range-of-motion boot for 4 weeks. After 6 weeks, physical therapy was increased and weight bearing gradually instituted as long as the osteotomy had healed. At time points up to 1 year postoperatively, the numeric rating scale (NRS) of pain, SF-36 (Short Form 36), AOFAS score, and FAOS (Foot and Ankle Outcome Score) were collected and plain radiographs taken. NRS pain reduced from 2.5 ± 2.3 preoperatively to 0.9 ± 1.2 after 1 year (p = 0.021). The median AOFAS score improved from 69 (42–75) preoperatively to 87 (58–100) after 1 year (p = 0.001). The FAOS categories of pain, function, sports activity, and quality of life all improved significantly after 1 year. The “symptoms” category did not, however, improve significantly (53.6 preoperatively, 56.3 after 1 year). The SF-36 physical component improved significantly but was less than the normal population at 1 year (p = 0.008). Preoperatively three out of ten athletes were able to participate in sports; at 1 year, eight out of ten were playing sports (five at pre-injury frequency). There were no lasting complications.
Although this study does show some promising results, it is important to realize that the follow-up is short term. The implant clearly has a theoretical value, and time will tell if this will translate into clinical results. The surgical procedure, although similar to other implantation techniques such as osteochondral autograft transfer, has a number of key elements, not least of which is very exact contouring of the implant to the existing articular surface. The implant is currently restricted in its use due to its size, which would require sacrifice of normal cartilage if used in smaller lesions.
Lateral Ligament Reconstruction: An All-Arthroscopic Technique
One of the most commonly encountered injuries in athletics is the lateral ankle ligament complex injury (Hershman et al. 2012; McCarthy et al. 2013). In most cases, nonoperative treatment is advised, followed by functional rehabilitation. A possible exception to this is a severe injury or grade III injury with objective signs of instability on clinical testing in a professional athlete. Following operative or nonoperative treatment of acute lateral instability, clinical signs of instability on examination are generally less apparent following surgical reconstruction. For this reason, later recurrence is probably less likely after surgery than after nonoperative treatment in the professional sportsperson. Surgeons are now more frequently performing acute repairs in these patients (van den Bekerom et al. 2013). In those treated nonoperatively, if chronic instability becomes apparent, then a commonly performed procedure is an anatomical lateral ligament complex reconstruction or Broström procedure, or a modification thereof (Broström 1966). Traditionally this is performed through an open lateral incision based around the anterior aspect of the lateral malleolus. It is, however, frequently combined with ankle arthroscopy (either anterior or posterior) through the standard portals if concomitant pathology is suspected in the ankle joint, such as an impingement lesion or talus osteochondral defect that requires operative treatment (Hintermann et al. 2002).
Other techniques to stabilize the lateral ligament complex have been described. Thermal shrinkage of the lateral ligament capsular tissue has been performed, but this technique has not been adopted particularly well among surgeons (Maiotti et al. 2005). The “all inside” arthroscopic lateral ligament reconstruction is an evolution of the standard open Broström technique. This allows the surgeon to perform the surgery through the standard arthroscopic portals or new accessory portals. A number of authors have reported their experience with this technique (Corte-Real and Moreira 2009; Kim et al. 2011; Nery et al. 2011; Cottom and Rigby 2013). Table 1 summarizes the current available literature on the subject.
This technique is based around standard anterolateral and anteromedial ankle arthroscopy portals. Any concomitant lesion in the ankle can be treated before the lateral ligament reconstruction. Concomitant lesions include anterior or anterolateral bony or soft tissue impingement, talar osteochondral defects, posterior impingement, peroneal tendon injuries, and medial deltoid ligament sprains. Each author has individual slight modifications to the technique, some using one anchor and some using two anchors. The two-anchor technique probably recreates a more natural footprint of the anterior talofibular ligament (ATFL), but this is not substantiated by any evidence. The differing techniques all share a common goal and that is to approximate the distal ATFL remnants with a secure suture onto the distal fibula while being careful to avoid the sural and superficial peroneal nerves and the peroneal tendons. Through the standard anterolateral portal, the ATFL insertion onto the anterior distal fibula is debrided with a suitable soft tissue shaver. Once the remnant is removed, the surgeon then prepares the fibula further with a burr to remove periosteum to expose a vascular bony surface. This gives the distal ATFL that is to be inserted onto the fibula a suitable biological environment for it to heal successfully. Using the bone suture anchor of the surgeon’s choice, this is now inserted securely into the distal fibula at the original ATFL attachment with one or two anchors. It is important to be careful when inserting the anchors not to inadvertently breach the cortex of the fibula. This anchor is generally inserted through the standard anterolateral portal (Corte-Real and Moreira 2009), but some authors suggest inserting the anchor through a more distal accessory anterolateral portal and at the same time capturing the more distal ATFL remnants (Nery et al. 2011). Passing the sutures through the distal ATFL remnant using a separate accessory portal incision or simply using a microsuture lasso, the suture can then secure the distal ATFL remnant onto the fibula while tightening the knot with the foot held in dorsiflexion and eversion.
The current literature on this technique is limited. The cohorts and outcome measures in the studies are quite heterogeneous and are, therefore, not truly comparable. All of the studies do report good outcomes with reasonable follow-up and rates of re-injury that are comparable to traditional open methods of repair. The procedure is still a relatively underused technique, possibly because the standard open lateral ligament reconstruction is very well regarded with predictable good results and low complication rates and little patient morbidity. The anatomical reconstruction of the calcaneofibular ligament (CFL) that is sometimes necessary in a Broström reconstruction may dissuade some surgeons from using this procedure. There also is an increased technical challenge to this operation. To determine whether this procedure is any more successful than an open lateral ligament complex reconstruction will require further research in the form of high-quality level 1 randomized controlled trials. The suspicion is, however, that this procedure will become more popular as surgeons continue to push the boundaries and orthopedic implant companies develop instrumentation to facilitate these techniques.
The Future of Ankle Arthroscopy: Flexible Arthroscopy?
The future of arthroscopy relies heavily on the future collective of surgeons adopting techniques, mastering them, and subsequently evolving the techniques with new approaches. This can be, in part, influenced by the surgeon developing new ideas and novel approaches, but undoubtedly in this day and age, the surgeon also is heavily reliant on the provision of modern instrumentation and research and development to make operations possible. The product manufacturers and companies are, therefore, also responsible for the evolution of modern arthroscopy, usually guided by surgical leaders in their fields.
A perennial problem for the surgeon is the difficulty in navigating the entire articular surface of the ankle joint. The solutions to this problem have been to introduce new anatomical portals, use smaller rigid arthroscopes, alter the viewing angle of the arthroscopy lens, and increase the distraction across the ankle. The problem with introducing new techniques is the inherent risk associated with them. The straight, rigid arthroscope, even the smaller 2.7-mm versions, is unable to view the whole joint surface adequately because of the convexity of the talar surface and even introducing the scope into the gutters can often be difficult. Trying to navigate the farthest recesses of the ankle with modern instruments also can lead to instrument breakage, especially if using the 2.7-mm arthroscope, or iatrogenic damage to the delicate articular cartilage. To improve access to difficult-to-reach places in the ankle, surgeons have developed new approach portals, but this has the potential to increase the morbidity from nerve and vessel injury or fistula formation. Increasing the traction can improve some of the working spaces, but can also make maneuvering the instruments a little harder due to the soft tissue tension.
The development of flexible arthroscopes has been attempted years ago with little success or subsequent development (Takahashi and Yamamoto 1997), and to date, few publications exist concerning this issue in ankle arthroscopy (DiGiovanni et al. 2009). Perhaps the reason for the lack of subsequent publications is that the current arthroscopic techniques are more than sufficient for their application. Users of flexible arthroscopes often encountered problems, such as poor visual fields and difficulty in maintaining orientation, but, despite this, recently, surgeons were still trying to ascertain if this technique has any credibility in its application to modern surgery. Insertion of the flexible arthroscope caused deformation necessitating a rigid plastic cannula; rigid arthroscopes provided clearer and larger visual field resolution, but they did not allow access through the anterior approach to certain areas such as the posterior talar dome beyond the mid-coronal plane. Of course, just because the surgeon can visualize these hard-to-reach areas does not mean that they can actively intervene with other surgical instruments because the instruments are rigid. The use or even need for flexible arthroscopy will continue to be debated. Skeptics will argue the surgeon can safely access everywhere needed with current methods either from the anterior or posterior approach while using rigid instrumentation, and they are correct in saying so. If the need for a purely diagnostic arthroscopy arises, then there is no doubt that flexible arthroscopy is appealing, but with the use of MRI scans, there is little need for this.
References
Aktas S, Kocaoglu B, Gereli A et al (2008) Incidence of chondral lesions of talar dome in ankle fracture types. Foot Ankle Int 29:287–292
Anders S, Goetz J, Schubert T et al (2012) Treatment of deep articular talus lesions by matrix associated autologous chondrocyte implantation results at five years. Int Orthop 36:2279–2285
Angthong C, Yoshimura I, Kanazawa K et al (2013) Critical three-dimensional factors affecting outcome in osteochondral lesion of the talus. Knee Surg Sports Traumatol Arthrosc 21(6):1–9
Aslan H, C İtak M, Baş EG et al (2012) Early results of HemiCAP® resurfacing implant. Acta Orthop Traumatol Turc 45:17–21
Athanasiou KA, Niederauer GG, Schenck RC (1995) Biomechanical topography of human ankle cartilage. Ann Biomed Eng 23:697–704
Aurich M, Bedi HS, Smith PJ et al (2011) Arthroscopic treatment of osteochondral lesions of the ankle with matrix-associated chondrocyte implantation: early clinical and magnetic resonance imaging results. Am J Sports Med 39:311–319
Bartlett W, Gooding CR, Carrington RWJ et al (2005) Autologous chondrocyte implantation at the knee using a bilayer collagen membrane with bone graft. A preliminary report. J Bone Joint Surg (Br) 87:330–332
Bartlett W, Krishnan SP, Skinner JA et al (2006) Collagen-covered versus matrix-induced autologous chondrocyte implantation for osteochondral defects of the knee: a comparison of tourniquet times. Eur J Orthop Surg Traumatol 16:315–317
Baums MH, Heidrich G, Schultz W et al (2006) Autologous chondrocyte transplantation for treating cartilage defects of the talus. J Bone Joint Surg 88:303–308
Berndt AL, Harty M (1959) Transchondral fractures (osteochondritis dissecans) of the talus. J Bone Joint Surg Am 41-A:988–1020
Berndt AL, Harty M (2004) Transchondral fractures (osteochondritis dissecans) of the talus. J Bone Joint Surg Am 86-A:1336
Brittberg M (2010) Cell carriers as the next generation of cell therapy for cartilage repair: a review of the matrix-induced autologous chondrocyte implantation procedure. Am J Sports Med 38:1259–1271
Brittberg M, Lindahl A, Nilsson A et al (1994) Treatment of deep cartilage defects in the knee with autologous chondrocyte transplantation. N Engl J Med 331:889–895
Broström L (1966) Sprained ankles. V. Treatment and prognosis in recent ligament ruptures. Acta Chir Scand 132:537–550
Browne JE, Anderson AF, Arciero R et al (2005) Clinical outcome of autologous chondrocyte implantation at 5 years in US subjects. Clin Orthop Relat Res 436:237–245
Carmont MR, Carey-Smith R, Saithna A, Dhillon M, Thompson P, Spalding T (2009) Delayed incorporation of a trufit plug: perseverance is recommended. Arthroscopy 25:810–4
Chang NJ, Lam CF, Lin CC et al (2013) Transplantation of autologous endothelial progenitor cells in porous PLGA scaffolds create a Microenvironment for the regeneration of hyaline cartilage in rabbits. Osteoarthritis Cartilage 21(10):1613–1622
Choi WJ, Park KK, Kim BS et al (2009) Osteochondral lesion of the talus: is there a critical defect size for poor outcome? Am J Sports Med 37:1974–1980
Chuckpaiwong B, Berkson EM, Theodore GH (2008) Microfracture for osteochondral lesions of the ankle: outcome analysis and outcome predictors of 105 cases. Arthroscopy 24:106–112
Corte-Real NM, Moreira RM (2009) Arthroscopic repair of chronic lateral ankle instability. Foot Ankle Int 30:213–217
Cottom JM, Rigby RB (2013) The “all inside” arthroscopic Broström procedure: a prospective study of 40 consecutive patients. J Foot Ankle Surg 52(5):568–574
Custers RJ, Dhert WJ, van Rijen MH et al (2007) Articular damage caused by metal plugs in a rabbit model for treatment of localized cartilage defects. Osteoarthritis Cartilage 15:937–945
Davidson PA, Rivenburgh D (2008) Focal anatomic patellofemoral inlay resurfacing: theoretic basis, surgical technique, and case reports. Orthop Clin North Am 39:337–346, vi
Delaney RA, Freehill MT, Higgins LD et al (2014) Durability of partial humeral head resurfacing. J Shoulder Elbow Surg 23(1):e14–22
DiGiovanni CW, Patel A, Tocci SL (2009) Is the future of foot and ankle arthroscopy flexible? Curr Orthop Pract 20:320–325
Dixon S, Harvey L, Baddour E et al (2011) Functional outcome of matrix-associated autologous chondrocyte implantation in the ankle. Foot Ankle Int 32:368–374
El-Rashidy H, Villacis D, Omar I et al (2011) Fresh osteochondral allograft for the treatment of cartilage defects of the talus: a retrospective review. J Bone Joint Surg Am 93:1634–1640
Fortier LA, Potter HG, Rickey EJ et al (2010) Concentrated bone marrow aspirate improves full-thickness cartilage repair compared with microfracture in the equine model. J Bone Joint Surg Am 92:1927–1937
Funayama A, Niki Y, Matsumoto H et al (2008) Repair of full-thickness articular cartilage defects using injectable type II collagen gel embedded with cultured chondrocytes in a rabbit model. J Orthop Sci 13:225–232
Gao C, Gao J, You X et al (2005) Fabrication of calcium sulfate/PLLA composite for bone repair. J Biomed Mater Res A 73:244–253
Garcia EJ, Bear RR, Schoenfeld AJ et al (2010) Treatment of osteochondral lesions of the talus with a biosynthetic scaffold: a report of four cases. J Bone Joint Surg Am 92:1774–1779
Giannini S, Buda R, Grigolo B et al (2001) Autologous chondrocyte transplantation in osteochondral lesions of the ankle joint. Foot Ankle Int 22:513–517
Giannini S, Buda R, Faldini C et al (2005a) Surgical treatment of osteochondral lesions of the talus in young active patients. J Bone Joint Surg Am 87:28–41
Giannini S, Buda R, Grigolo B et al (2005b) The detached osteochondral fragment as a source of cells for autologous chondrocyte implantation (ACI) in the ankle joint. Osteoarthritis Cartilage 13:601–607
Giannini S, Buda R, Vannini F et al (2008) Arthroscopic autologous chondrocyte implantation in osteochondral lesions of the talus surgical technique and results. Am J Sports Med 36:873–880
Giannini S, Battaglia M, Buda R et al (2009a) Surgical treatment of osteochondral lesions of the talus by open-field autologous chondrocyte implantation: a 10-year follow-up clinical and magnetic resonance imaging T2-mapping evaluation. Am J Sports Med 37(Suppl 1):112S–118S
Giannini S, Buda R, Cavallo M (2009b) One-step bone marrow-derived cell transplantation in talar osteochondral lesions. Clin Orthop Relat Res 467:3307–3320
Giannini S, Buda R, Grigolo B et al (2010) Bipolar fresh osteochondral allograft of the ankle. Foot Ankle Int 31:38–46
Giannini S, Buda R, Battaglia M et al (2013) One-step repair in talar osteochondral lesions: 4-year clinical results and t2-mapping capability in outcome prediction. Am J Sports Med 41:511–518
Giza E, Sullivan M, Ocel D et al (2010) Matrix-induced autologous chondrocyte implantation of talus articular defects. Foot Ankle Int 31:747–753
Gomoll AH, Probst C, Farr J et al (2009) Use of a type I/III bilayer collagen membrane decreases reoperation rates for symptomatic hypertrophy after autologous chondrocyte implantation. Am J Sports Med 37:20S–23S
Hahn DB, Aanstoos ME, Wilkins RM (2010) Osteochondral lesions of the talus treated with fresh talar allografts. Foot Ankle Int 31:277–282
Hangody L, Kish G, Módis L et al (2001) Mosaicplasty for the treatment of osteochondritis dissecans of the talus: two to seven year results in 36 patients. Foot Ankle Int 22:552–558
Henderson I, Gui J, Lavigne P (2006) Autologous chondrocyte implantation: natural history of postimplantation periosteal hypertrophy and effects of repair-site debridement on outcome. Arthroscopy 22:1318.e1–1324.e1
Hepple S, Winson IG, Glew D (1999) Osteochondral lesions of the talus: a revised classification. Foot Ankle Int 20:789–793
Hershman EB, Anderson R, Bergfeld JA et al (2012) An analysis of specific lower extremity injury rates on grass and Field Turf playing surfaces in National Football League Games: 2000–2009 seasons. Am J Sports Med 40:2200–2205
Hintermann B, Boss A, Schäfer D (2002) Arthroscopic findings in patients with chronic ankle instability. Am J Sports Med 30:402–409
Imhoff AB, Paul J, Ottinger B et al (2011) Osteochondral transplantation of the talus long-term clinical and magnetic resonance imaging evaluation. Am J Sports Med 39:1487–1493
Johnson B, Lever C, Roberts S et al (2013) Cell cultured chondrocyte implantation and scaffold techniques for osteochondral talar lesions. Foot Ankle Clin 18:135–150
Kim ES, Lee KT, Park JS et al (2011) Arthroscopic anterior talofibular ligament repair for chronic ankle instability with a suture anchor technique. Orthopedics 34(4)
Koulalis D, Schultz W, Heyden M (2002) Autologous chondrocyte transplantation for osteochondritis dissecans of the talus. Clin Orthop Relat Res 395:186–192
Lee KT, Kim JS, Young KW et al (2013) The use of fibrin matrix-mixed gel-type autologous chondrocyte implantation in the treatment for osteochondral lesions of the talus. Knee Surg Sports Traumatol Arthrosc 21:1251–1260
Li G, Wan L, Kozanek M (2008) Determination of real-time in-vivo cartilage contact deformation in the ankle joint. J Biomech 41:128–136
Loening AM, James IE, Levenston ME et al (2000) Injurious mechanical compression of bovine articular cartilage induces chondrocyte apoptosis. Arch Biochem Biophys 381:205–212
Magnan B, Samaila E, Bondi M et al (2012) Three-dimensional matrix-induced autologous chondrocytes implantation for osteochondral lesions of the talus: midterm results. Adv Orthop 2012:942174
Maiotti M, Massoni C, Tarantino U (2005) The use of arthroscopic thermal shrinkage to treat chronic lateral ankle instability in young athletes. Arthroscopy 21:751–757
Marco F, Leon C, Lopez-Oliva F et al (1992) Intact articular cartilage cryopreservation in vivo evaluation. Clin Orthop Relat Res 283:11–20
McCarthy MM, Voos JE, Nguyen JT et al (2013) Injury profile in elite female basketball athletes at the Women’s National Basketball Association combine. Am J Sports Med 41:645–651
Meehan R, McFarlin S, Bugbee W et al (2005) Fresh ankle osteochondral allograft transplantation for tibiotalar joint arthritis. Foot Ankle Int 26:793–802
Milentijevic D, Torzilli PA (2005) Influence of stress rate on water loss, matrix deformation and chondrocyte viability in impacted articular cartilage. J Biomech 38:493–502
Miller SD, Schon LC (2012) Arthroscopic filling of talar osteochondral defects with stem cell – rich collagen paste. Tech Foot Ankle Surg 11:135–139
Mologne TS, Ferkel RD (2007) Arthroscopic treatment of osteochondral lesions of the distal tibia. Foot Ankle Int 28:865–872
Nam EK, Ferkel RD, Applegate GR (2009) Autologous chondrocyte implantation of the ankle: a 2- to 5-year follow-up. Am J Sports Med 37:274–284
Nelson AJ, Collins CL, Yard EE et al (2007) Ankle injuries among United States high school sports athletes, 2005–2006. J Athl Train 42:381
Nery C, Raduan F, Del Buono A et al (2011) Arthroscopic-assisted Broström-Gould for chronic ankle instability: a long-term follow-up. Am J Sports Med 39:2381–2388
Pearce CJ, Gartner LE, Mitchell A et al (2012) Synthetic osteochondral grafting of ankle osteochondral lesions. Foot Ankle Surg 18:114–118
Petersen L, Brittberg M, Lindahl A (2003) Autologous chondrocyte transplantation of the ankle. Foot Ankle Clin 8:291–303
Phipatanakul WP, VandeVord PJ, Teitge RA et al (2004) Immune response in patients receiving fresh osteochondral allografts. Am J Orthop (Belle Mead NJ) 33:345–348
Raikin SM (2004) Stage VI: massive osteochondral defects of the talus. Foot Ankle Clin 9:737–744, vi
Ronga M, Grassi FA, Montoli C et al (2005) Treatment of deep cartilage defects of the ankle with matrix-induced autologous chondrocyte implantation (MACI). Foot Ankle Surg 11:29–33
Schneider TE, Karaikudi S (2009) Matrix-Induced Autologous Chondrocyte Implantation (MACI) grafting for osteochondral lesions of the talus. Foot Ankle Int 30:810–814
Scranton PE, McDermott JE (2001) Treatment of type V osteochondral lesions of the talus with ipsilateral knee osteochondral autografts. Foot Ankle Int 22:380–384
Seil R, Rupp S, Pape D et al (2001) Approach to open treatment of osteochondral lesions of the talus. Orthopade 30:47–52
Sgaglione NA, Florence AS (2009) Bone graft substitute plug failure with giant cell reaction in the treatment of osteochondral lesions of the distal femur: a report of 2 cases with operative revision. Arthroscopy 25:815–819
Takahashi T, Yamamoto H (1997) Development and clinical application of a flexible arthroscopy system. Arthroscopy 13:42–50
Treppo S, Koepp H, Quan EC et al (2000) Comparison of biomechanical and biochemical properties of cartilage from human knee and ankle pairs. J Orthop Res 18:739–748
Valderrabano V, Leumann A, Rasch H et al (2009) Knee-to-ankle mosaicplasty for the treatment of osteochondral lesions of the ankle joint. Am J Sports Med 37:105S–111S
Valderrabano V, Miska M, Leumann A et al (2013) Reconstruction of osteochondral lesions of the talus with autologous spongiosa grafts and autologous matrix-induced chondrogenesis. Am J Sports Med 41:519–527
van Bergen CJ, Zengerink M, Blankevoort L et al (2010) Novel metallic implantation technique for osteochondral defects of the medial talar dome: a cadaver study. Acta Orthop 81:495–502
van Bergen CJ, Tuijthof GJ, Sierevelt IN et al (2011) Direction of the oblique medial malleolar osteotomy for exposure of the talus. Arch Orthop Trauma Surg 131:893–901
van Bergen CJ, Reilingh ML, Dijk C (2012) Novel metal implantation technique for secondary osteochondral defects of the medial talar dome – one-year results of a prospective study. Fuß Sprunggelenk 10:130–137
van den Bekerom MP, Kerkhoffs GM, McCollum GA et al (2013) Management of acute lateral ankle ligament injury in the athlete. Knee Surg Sports Traumatol Arthrosc 21:1390–1395
Van Ginckel A, Roosen P, Almqvist KF et al (2011) Effects of in vivo exercise on ankle cartilage deformation and recovery in healthy volunteers: an experimental study. Osteoarthritis Cartilage 19:1123–1131
Wan L, de Asla RJ, Rubash HE et al (2008) In vivo cartilage contact deformation of human ankle joints under full body weight. J Orthop Res 26:1081–1089
Whittaker JP, Smith G, Makwana N et al (2005) Early results of autologous chondrocyte implantation in the talus. J Bone Joint Surg (Br) 87:179–183
Williams RJ, Dreese JC, Chen C-T (2004) Chondrocyte survival and material properties of hypothermically stored cartilage an evaluation of tissue used for osteochondral allograft transplantation. Am J Sports Med 32:132–139
Woelfle JV, Reichel H, Nelitz M (2013) Indications and limitations of osteochondral autologous transplantation in osteochondritis dissecans of the talus. Knee Surg Sports Traumatol Arthrosc 21:1925–1930
Zengerink M, Struijs PA, Tol JL et al (2010) Treatment of osteochondral lesions of the talus: a systematic review. Knee Surg Sports Traumatol Arthrosc 18:238–246
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2015 Springer-Verlag Berlin Heidelberg
About this entry

Cite this entry
Roche, A.J., Calder, J.D. (2015). Arthroscopy of the Ankle: New Approaches. In: Doral, M.N., Karlsson, J. (eds) Sports Injuries. Springer, Berlin, Heidelberg. https://doi.org/10.1007/978-3-642-36569-0_141
Download citation
DOI: https://doi.org/10.1007/978-3-642-36569-0_141
Published:
Publisher Name: Springer, Berlin, Heidelberg
Print ISBN: 978-3-642-36568-3
Online ISBN: 978-3-642-36569-0
eBook Packages: MedicineReference Module Medicine