
Abstract
Coronary artery calcium (CAC) is calcium compound deposited within atherosclerotic plaque along its aging. The amount of the calcium is known to be proportional to the whole plaque burden in the subject. Based on this acknowledgment, the quantitative amount of CAC has been applied in clinical field as an indicator for cardiovascular event risk. Among several methods to score the CAC, Agatston score has been widely used in research and practice as a representative scoring method. To stratify cardiovascular risk, CAC score was stratified by the score or percentile within a corresponding cohort by age and gender. In spite of controversy, the CAC scoring methods were validated to be feasible in clinical routine practice. The certain facts about the CAC are that the CAC score predicts CAD risk of intermediate- and high-risk populations; zero CAC score suggests very low risk of CAD unless other risk factors are associated; faster CAC score increase suggests higher risk of CAD; ethnic and sexual differences exist; CAC score is not for diagnosing CAD but for cardiovascular risk assessment.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others

Keywords
- Coronary Artery Disease
- Coronary Artery Calcium
- Coronary Artery Calcium Score
- Plaque Burden
- Significant Coronary Artery Disease
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
2 Scoring Methods
-
The first quantification method for CAC was suggested by Agatston using electron-beam CT (EBCT) [3].
-
Besides scoring methods, the reference standard is important for practical application.
2.1 Agatston Score [3]
-
Scanning protocol is suggested for standardization of image quality.
Parameters
Conditions
Prospective data acquisition
At 80 % of R-R interval
Tube voltage
130 kVp
Tube current
(630 mA)
Slice thickness
(3 mm)
Acquisition time
(100 ms)
Contrast enhancement
None
-
Coronary artery calcium should be identified by analyzers with classifying branches.
-
Calcium area segmentation is semiautomatic using threshold technique, higher than 130 Hounsfield units (HU) and larger than single pixel.
-
The density of calcium area is stratified as “density factor” based on peak HU in two-dimensional ROI.
Density factors
Hounsfield units
1
130–199
2
200–299
3
300–399
4
Over 400
-
Agatston score (AS) is a global sum of products by calcium areas, density factors, and slice thickness.
$$ AS={\displaystyle \sum}_{x=1}^n\left(\frac{A_x\cdot {D}_x\cdot SL}{3}\right) $$x, serial number of ROIs; A, area of ROIs; D, density factor; SL, slice thickness
2.2 Volume Score [4]
-
The volume score (VS) was invented to overcome drawbacks of AS such as nonlinear measurement of HU (density factors) and complexity of measurement.
-
Scanning protocol and threshold value for segmentation are same as AS.
-
The VS is acquired as a global sum of ROI volumes.
$$ VS={\displaystyle \sum}_{x=1}^n\left({A}_x\cdot SL\right) $$ -
The reproducibility of examination is higher by VS than by AS.
-
However, AS has greater reference standard criteria.
2.3 Mass Score [5]
-
Instead of adopting indirect parameters, the mass score (MS) was designed for more direct assessment of calcium mass.
-
Scanning field includes calcium hydroxyapatite [Ca10(PO4)6(OH)2, CaHA] phantoms as reference standard materials.
-
Initially, the HUs of CaHA phantoms are measured in corresponding images. Based on real calcium density in the phantoms, density-HU plotting with a linear fitting equation is possible.
$$ HU=a\cdot \left[ CaHA\right]+b $$[CaHA], calcium densities in CaHA phantoms
-
Since the calcium mass is a product of calcium density and its volume, the MS can be acquired from the fitting equation and the volume of ROIs.
$$ MS={\displaystyle \sum}_{x=1}^n\left[\left(\frac{H{U}_x-b}{a}\right)\cdot {A}_x\cdot SL\right] $$ -
The strength of MS is the consistency of measured values throughout different scanning environments.
-
The MS is the most accurate and reproducible technique for CAC quantification.
-
Drawbacks of the MS are the complexity of assessment and lack of reference standard criteria for clinical application.
2.4 Other Scores
2.4.1 CAC Progression Rate [6]
-
Based on the fact that CAC increasing speed is associated with the risk of CAD, CAC progression rate (R) is suggested.
-
R reflects a percentile interval change of VS.
$$ R=100\cdot {e}^{\left\{\frac{\varDelta \left[ \ln (VS)\right]}{T}\right\}-1} $$T, time interval between examinations
-
The R may be a useful marker for a subsequent monitoring of the coronary atherosclerotic burden in single subject.
-
Drawbacks are the complexity of assessment and lack of the reference standard criteria.
2.4.2 Calcium Coverage Score [7]
-
The calcium coverage score (CCS) is the percentage of coronary arteries affected by calcium.
-
In a multiethnic large-scale cohort study, the CCS predicted cardiovascular events better than AS and MS.
-
A drawback is insufficient clinical application results including reference standard criteria.
3 Clinical Significance of CAC
3.1 Cardiovascular Risk by Plaque Burden (Figs. 4.1, 4.2, 4.3, 4.4, and 4.5)

A 72-year-old female. (a) Non-enhanced axial CT for calcium scoring shows no calcium in the coronary arteries. Small nodular calcification is noted in the descending aortic wall. (b) Total Agatston score is zero (From Hoff et al. [9])

A 77-year-old male. (a) Small calcific nodules are noted in the mid left anterior descending artery. Other calcific nodules are noted in the descending aortic wall and hilar lymph nodes. (b) Total Agatston score is 34.86, which means mild plaque burden. The subject is less than the 25th percentile in the same age and gender group (From Hoff et al. [9])

A 69-year-old male. (a) Small nodular calcification is noted at the branching level of the left main coronary artery. (b) Total Agatston score is 53.07, which means mild plaque burden. Due to younger age than case 2, this subject is plotted between the 25th and 50th percentiles in the same age and gender group (From Hoff et al. [9])

A 71-year-old female. (a) Two calcific nodules are noted at the left anterior descending artery. (b) Total Agatston score is 71.90, which means mild plaque burden. Due to female gender, this subject is plotted between the 50th and 75th percentiles in the same age and gender group (From Hoff et al. [9])

A 61-year-old male with diabetes mellitus. (a) Diffuse calcification is noted from the orifice level of the left main coronary artery to the mid level of the left anterior descending artery. (b) Volume rendered 3-D image in 4-chamber orientation reveals heavy calcium in the left anterior descending and right coronary arteries. (c) Total Agatston score is 776.45, which means extensive plaque burden. This subject is stratified to higher than the 75th percentile in the same age and gender group. Stratification higher than the 75th percentile means high cardiovascular risk (From Hoff et al. [9])
-
An initial meta-analysis-based guideline for CAC Agatston score focused on plaque burden and its clinical interpretation (Table 4.1) [8].
Table 4.1 The interpretation guideline of Agatston score -
Nonlinear stratification of Agatston score matched with plaque burden and its clinical interpretation.
-
This guideline is simple to apply on routine practice.
-
However, diversity of CAC score by sex and age was not considered.
3.2 Cardiovascular Risk by Percentile Stratification (Figs. 4.1, 4.2, 4.3, 4.4, and 4.5)
-
Based on multicenter large cohort prospective research, Agatston score distributions by age strata and genders were suggested as an interpretation guideline (Table 4.2) [9].
Table 4.2 Distributions of Agatston score by age strata and genders -
Since the age factor is stratified as decades, interpolated data can demonstrate percentile zone graph for practical application.
-
This guideline reflects the diversity of CAC by genders and ages so that more practical application on clinical field is possible.
-
Since the result display is intuitive, this guideline is equipped in most CAC analyzing tools.
-
CAC score higher than the 75th percentile was reported to present higher cardiovascular risk than the score below the 25th percentile [10].
3.3 CAD Risk Per Patient
-
The CAC scoring pursues an evaluation of cardiovascular risk in a target subject based on data from communities.
-
Can we use CAC score to evaluate CAD per patient?
-
Based on histological comparison, intraplaque calcium amount was reported to be proportional to the total plaque volume [11]. This means the positive CAC score can estimate total plaque burden per plaque and per patient.
-
Through many reports supporting the relationship between CAC score and CAD severity per patient, some papers suggest cutoff values (AS 371 or 400) of CAC score for prediction of flow-limiting CAD per patient [12, 13].
-
The regional distribution and specific patterns of calcium may suggest plaque features in per patient level. Shell-like and diffuse calcifications have higher relationship with significant stenosis and noncalcified plaque than nodular calcification [14].
-
Yes, we can use CAC score to predict the severity of CAD in per patient level when the CAC score is high enough. In contrast, low to zero CAC score is limited to preclude the possibility of significant CAD generally.
3.4 Zero Calcium Score
-
According to interpretation guidelines of CAC, a zero score means very low cardiovascular risk with the lowest percentiles in both male and female (Tables 4.1 and 4.2).
-
However, no calcium is detected in uncalcified soft plaque, which is more important for acute coronary syndrome.
-
Theoretically, CAC cannot reflect the risk of acute coronary syndrome, which is more fatal than stable angina.
-
The clinical meaning of zero CAC score reaches a consensus, although some controversy continues until now [15].
-
The zero CAC score virtually exclude cardiovascular risk more likely in subjects older than 50 years of age and subjects without other significant risk factors [16, 17].
-
The zero CAC score implies very low cardiovascular risk in the intermediate term (around 3.5 years) [18].
-
Based on specific conditions, the zero CAC score can be used as an indicator to preclude significant CAD.
3.5 CAC-Concordant Clinical Parameters
-
Currently, the CAC score is regarded as a feasible independent marker for cardiovascular risk stratification.
-
The CAC score is used as a reference standard or a major input factor for cardiovascular risk estimation during the other clinical studies.
3.5.1 Coronary Age [19]
-
As a cardiovascular risk predictor, the “coronary age” was suggested by a large cohort study using MESA data.
-
Based on the 50th percentile CAC score by ethnicity and gender, the coronary age is calculated as a polynomial function of Agatston score (Table 4.3).
Table 4.3 Prediction of coronary age based on Agatston score by ethnicity and gender -
A true biological age of the subject’s coronary artery as well as the degree of the coronary arterial damage during the subject’s aging process.
-
The coronary age can be applied to enhance patient’s compliance to treatment of CAD and modification of one’s lifestyle.
3.5.2 DM Mortality
-
The National Cholesterol Education Program (NCEP) regards diabetes mellitus as a CAD equivalent condition due to its high incidence in diabetic group [20].
-
The cardiovascular risk of the diabetics, especially asymptomatic patients, can be monitored using CAC score.
-
In a large cohort study based on US National Death Registry, the all-cause mortality of the asymptomatic diabetics increased in proportion to Agatston score [21].
-
Relative risk ratios for all-cause mortality in asymptomatic diabetic patients are 3.76, 1.76, 1.44, and 1.06 by hypertension, current smoking, CAC score, and age, respectively (p < 0.05) [21].
-
Combining with other hazardous variables, the diabetics can be monitored in a more strict way.
3.5.3 Cardiac Risk of Hypertensive Disease
-
Left ventricular hypertrophy of the hypertensive suggests a high cardiovascular risk.
-
In a hypertensive cohort, CAC score showed a significant correlation with the severity of left ventricular hypertrophy as well as its clinical marker, QT dispersion on ECG [22].
-
Since CAC score is correlated with abnormal lipid profile and ascending aortic prominence, CAC score monitoring may be a comprehensive indicator of cardiovascular risk for hypertensive patients.
4 Appropriateness Criteria for CAC
4.1 AHA Criteria [23]
-
When is CAC score appropriate for detection of CAD and risk assessment?
Without
With
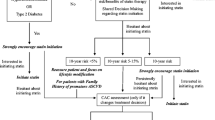
Asymptomatic patients
Low pretest-probability
Family history of premature CAD
Known CAD
Intermediate pretest-probability
-
When is CAC score inappropriate for detection of CAD and risk assessment?
Without
With
Asymptomatic patients
Known CAD
Low pretest-probability
4.2 European Criteria [24]
-
CAC score is a good predictor of cardiovascular events in intermediate-risk Caucasian population.
-
Rapid CAC progression is associated with higher risk of events.
-
A zero CAC score is associated with a very low prevalence of CAD.
4.3 ASCI Criteria [25]
-
How is CAC scored in the coronary artery disease (CAD) risk assessment for the general population?
Framingham risk score
Criteria
Asymptomatic subjects with
Low
Inappropriate
Moderate
Appropriate
High
Appropriate
5 Summary
-
CAC score predicts CAD risk of intermediate- and high-risk populations.
-
A zero score suggests very low risk of CAD unless other risk factors are associated.
-
Faster CAC score increase suggests higher risk of CAD.
-
Ethnic and sexual differences exist.
-
CAC score is not for diagnosing CAD but for cardiovascular risk assessment.
Abbreviations
- AS:
-
Agatston score
- CAC:
-
Coronary artery calcium
- CAD:
-
Coronary artery disease
- CaHA:
-
Calcium hydroxyapatite
- CCS:
-
Calcium coverage score
- EBCT:
-
Electron-beam CT
- HU:
-
Hounsfield units
- MS:
-
Mass score
- VS:
-
Volume score
References
Rumberger JA, Simons DB, Fitzpatrick LA, Sheedy PF, Schwartz RS. Coronary artery calcium area by electron-beam computed tomography and coronary atherosclerotic plaque area. A histopathologic correlative study. Circulation. 1995;92:2157–62.
Schmermund A, Bailey KR, Rumberger JA, Reed JE, Sheedy 2nd PF, Schwartz RS. An algorithm for noninvasive identification of angiographic three-vessel and/or left main coronary artery disease in symptomatic patients on the basis of cardiac risk and electron-beam computed tomographic calcium scores. J Am Coll Cardiol. 1999;33:444–52.
Agatston AS, Janowitz WR, Hildner FJ, Zusmer NR, Viamonte Jr M, Detrano R. Quantification of coronary artery calcium using ultrafast computed tomography. J Am Coll Cardiol. 1990;15:827–32.
Callister TQ, Cooil B, Raya SP, Lippolis NJ, Russo DJ, Raggi P. Coronary artery disease: improved reproducibility of calcium scoring with an electron-beam ct volumetric method. Radiology. 1998;208:807–14.
Hong C, Becker CR, Schoepf UJ, Ohnesorge B, Bruening R, Reiser MF. Coronary artery calcium: absolute quantification in nonenhanced and contrast-enhanced multi-detector row ct studies. Radiology. 2002;223:474–80.
Yoon HC, Emerick AM, Hill JA, Gjertson DW, Goldin JG. Calcium begets calcium: progression of coronary artery calcification in asymptomatic subjects. Radiology. 2002;224:236–41.
Brown ER, Kronmal RA, Bluemke DA, Guerci AD, Carr JJ, Goldin J, Detrano R. Coronary calcium coverage score: determination, correlates, and predictive accuracy in the multi-ethnic study of atherosclerosis. Radiology. 2008;247:669–75.
Rumberger JA, Brundage BH, Rader DJ, Kondos G. Electron beam computed tomographic coronary calcium scanning: a review and guidelines for use in asymptomatic persons. Mayo Clin Proc. 1999;74:243–52.
Hoff JA, Chomka EV, Krainik AJ, Daviglus M, Rich S, Kondos GT. Age and gender distributions of coronary artery calcium detected by electron beam tomography in 35,246 adults. Am J Cardiol. 2001;87:1335–9.
Georgiou D, Budoff MJ, Kaufer E, Kennedy JM, Lu B, Brundage BH. Screening patients with chest pain in the emergency department using electron beam tomography: a follow-up study. J Am Coll Cardiol. 2001;38:105–10.
Rumberger JA. Coronary artery calcification: “…Empty your cup.”. Am Heart J. 1999;137:774–6.
Rumberger JA, Sheedy PF, Breen JF, Schwartz RS. Electron beam computed tomographic coronary calcium score cutpoints and severity of associated angiographic lumen stenosis. J Am Coll Cardiol. 1997;29:1542–8.
Moser KW, O’Keefe Jr JH, Bateman TM, McGhie IA. Coronary calcium screening in asymptomatic patients as a guide to risk factor modification and stress myocardial perfusion imaging. J Nucl Cardiol. 2003;10:590–8.
Thilo C, Gebregziabher M, Mayer FB, Zwerner PL, Costello P, Schoepf UJ. Correlation of regional distribution and morphological pattern of calcification at ct coronary artery calcium scoring with non-calcified plaque formation and stenosis. Eur Radiol. 2010;20:855–61.
Lee J. Coronary artery calcium scoring and its impact on the clinical practice in the era of multidetector CT. Int J Cardiovasc Imaging. 2011;27 Suppl 1:9–25.
Knez A, Becker A, Leber A, White C, Becker CR, Reiser MF, Steinbeck G, Boekstegers P. Relation of coronary calcium scores by electron beam tomography to obstructive disease in 2,115 symptomatic patients. Am J Cardiol. 2004;93:1150–2.
Ergun E, Kosar P, Ozturk C, Basbay E, Koc F, Kosar U. Prevalence and extent of coronary artery disease determined by 64-slice CTA in patients with zero coronary calcium score. Int J Cardiovasc Imaging. 2011;27:451–8.
Church TS, Levine BD, McGuire DK, Lamonte MJ, Fitzgerald SJ, Cheng YJ, Kimball TE, Blair SN, Gibbons LW, Nichaman MZ. Coronary artery calcium score, risk factors, and incident coronary heart disease events. Atherosclerosis. 2007;190:224–31.
Sirineni GK, Raggi P, Shaw LJ, Stillman AE. Calculation of coronary age using calcium scores in multiple ethnicities. Int J Cardiovasc Imaging. 2008;24:107–11.
Grundy SM, Benjamin IJ, Burke GL, Chait A, Eckel RH, Howard BV, Mitch W, Smith Jr SC, Sowers JR. Diabetes and cardiovascular disease: a statement for healthcare professionals from the American Heart Association. Circulation. 1999;100:1134–46.
Raggi P, Shaw LJ, Berman DS, Callister TQ. Prognostic value of coronary artery calcium screening in subjects with and without diabetes. J Am Coll Cardiol. 2004;43:1663–9.
Pan NH, Yang HY, Hsieh MH, Chen YJ. Coronary calcium score from multislice computed tomography correlates with QT dispersion and left ventricular wall thickness. Heart Vessels. 2008;23:155–60.
Taylor AJ, Cerqueira M, Hodgson JM, Mark D, Min J, O’Gara P, Rubin GD, American College of Cardiology Foundation Appropriate Use Criteria Task Force; Society of Cardiovascular Computed Tomography; American College of Radiology; American Heart Association; American Society of Echocardiography; American Society of Nuclear Cardiology, North American Society for Cardiovascular Imaging; Society for Cardiovascular Angiography and Interventions; Society for Cardiovascular Magnetic Resonance. ACCF/SCCT/ACR/AHA/ASE/ASNC/NASCI/SCAI/SCMR 2010 appropriate use criteria for cardiac computed tomography. A report of the American College of Cardiology Foundation Appropriate Use Criteria Task Force, the Society of Cardiovascular Computed Tomography, the American College of Radiology, the American Heart Association, the American Society of Echocardiography, the American Society of Nuclear Cardiology, the North American Society for Cardiovascular Imaging, the Society for Cardiovascular Angiography and Interventions, and the Society for Cardiovascular Magnetic Resonance. Circulation. 2010;122:e525–55.
Oudkerk M, Stillman AE, Halliburton SS, Kalender WA, Mohlenkamp S, McCollough CH, Vliegenthart R, Shaw LJ, Stanford W, Taylor AJ, van Ooijen PM, Wexler L, Raggi P, European Society of Cardiac Radiology; North American Society for Cardiovascular Imaging. Coronary artery calcium screening: current status and recommendations from the European Society of Cardiac Radiology and North American Society for Cardiovascular Imaging. Eur Radiol. 2008;18:2785–807.
ASCI CCT and CMR Guideline Working Group, Tsai IC, Choi BW, Chan C, Jinzaki M, Kitagawa K, Yong HS, Yu W, Asian Society of Cardiovascular Imaging Cardiac Computer Tomography; Cardiac Magnetic Resonance Imaging Guideline Working Group. ASCI 2010 appropriateness criteria for cardiac computed tomography: a report of the Asian Society of Cardiovascular Imaging Cardiac Computed Tomography and Cardiac Magnetic Resonance Imaging Guideline Working Group. Int J Cardiovasc Imaging. 2010;26 Suppl 1:1–15.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2015 Springer-Verlag Berlin Heidelberg
About this chapter
Cite this chapter
Lee, J. (2015). Calcium Scoring. In: Lim, TH. (eds) Practical Textbook of Cardiac CT and MRI. Springer, Berlin, Heidelberg. https://doi.org/10.1007/978-3-642-36397-9_4
Download citation
DOI: https://doi.org/10.1007/978-3-642-36397-9_4
Published:
Publisher Name: Springer, Berlin, Heidelberg
Print ISBN: 978-3-642-36396-2
Online ISBN: 978-3-642-36397-9
eBook Packages: MedicineMedicine (R0)