
Abstract
Most clinicians and patients consider obesity just as a problem of energy balance: more energy input than expenditure. However, the epidemiological data and the clinical practice clearly show that obesity is more complex than described by this simple equation. In particular, the chapter underlined the possible role of negative body image in the etiology of this disturbance. Specifically, we suggested that unhealthful weight-control behaviors, that induce significant weight gain over time, may be driven by an allocentric negative body image that is no more updated by contrasting egocentric representations driven by perception (allocentric lock). In other words, subjects are locked to an allocentric negative representation of their body that their sensory inputs are no more able to update even after the dramatic body changes following a successful diet or bariatric surgery. In the chapter, we also discussed the possible role of virtual reality (VR) in addressing this problem within an integrated treatment approach. Specifically, we suggested that adding a 10-session experiential protocol based on the free NeuroVR (http://www.neurovr.org) virtual reality software to the classical treatment of obesity may improve its long-term outcome. The characteristics of the protocol and the outcome of two controlled clinical trials used to test it (VEPSY UPDATED - ISRCTN59019572, and AVATOB-NCT01394393) are detailed and discussed.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
15.1 Introduction
Weight-related disorders are becoming a critical problem in both Western and developing countries. During the past 20 years, there has been a dramatic increase in both obesity and eating disorders in most countries and rates remain high. Unfortunately, the treatment of weight-related disorders is not easy: the typical treatment includes a combination of diet, exercise, cognitive and/or behavior modification, and the final choice depends on the overall health condition, level of disorders, and willingness to address the problem.
The raising prevalence of weight-related disorders is pushing eating disorder and obesity researchers to start a collaboration between the fields to address them. In particular, their effort is focused on the identification of risk factors that are shared between these weight-related disorders (Haines and Neumark-Sztainer 2006): apparently, unhealthful weight-control behaviors—such as fasting (going without eating for 24 h for weight control), vomiting, or laxative abuse—are the common antecedents of both obesity and eating disorders (Haines and Neumark-Sztainer 2006; Neumark-Sztainer et al. 2006; Neumark-Sztainer 2009; Johnston 2004; Stice et al. 2005, 2008). For example, Neumark-Sztainer and colleagues (Neumark-Sztainer et al. 2006) discussed the results of the Project EAT II (Eating Among Teens), a longitudinal study involving 2,516 ethnically and socioeconomically diverse adolescents. They report that, 5 years later, the use of unhealthful weight-control behaviors increased six times the risk for binge eating with loss of control, three times the risk for being overweight, and two to five times the risk for extreme weight-control behaviors such as the use of diet pills and self-induced vomiting. A similar result was found by Stice and colleagues (2008): in a different longitudinal study fasting was the best predictor for the future onset, 5 years later, of binge eating and bulimia nervosa.
It is well-known from epidemiological studies that childhood obesity has different ethnic, socioeconomic (compared with affluent white children, the poor Hispanic, white, and black children have 2.7, 1.9, and 3.2 times higher odds of obesity), and behavioral risk factors (Singh et al. 2008). Between the behavioral variables higher television viewing, and higher physical inactivity levels were all independently associated with higher obesity prevalence.
However, in a 4-year longitudinal study on 496 adolescent girls, Stice and colleagues (2005) studied the psychological and behavioral risk factors able to predict the onset of obesity in adolescent girls. Their data show that participants who were on a weight-loss diet, or who used maladaptive compensatory behaviors for weight control at T1 of the study showed, 4 years later, an increased risk for obesity onset. A more recent 10-year longitudinal study confirmed this datum (Neumark-Sztainer et al. 2012). As stated by the authors:
Findings clearly indicate that dieting and unhealthy weight control behaviors, as reported by adolescents, predict significant weight gain over time (p. 80).
These data have an important clinical implication: the evidence that youths practicing unhealthful weight-control behaviors are at higher risk for obesity implies that prevention and treatment interventions should also focus on the causes of these behaviors. In other words, why do adolescents decide to start such radical weight-control behaviors? In a recent letter to the Yahoo Answer site an adolescent girl wrote:
I hate my body so much. My top half (arms, stomach) is fine. I have a very flat stomach, my arms are great (my back is even bony looking) I wear a XS, S in shirts. but my lower half (butt, thighs) are huge, seriously I mean how can I loose weight there? (online: http://answers.yahoo.com/question/index?qid=20120504232627AAPkxrl).
The words of the girl clearly explain her behavior: she wants going on diet because she does not like her body (Riva et al. 2000c). A study by Kostanski and Gullone (1999) with a sample of 431 Australian pre-adolescent children (7–10 years) confirms this interpretation: pre-adolescents as young as 7 years of age are unsatisfied with their body appearance and deliberately engage in restrictive eating behaviors. More, a recent study (Friend et al. 2012) showed that in adolescents frequent self-weighing is associated with lower body satisfaction and higher rates of unhealthy and extreme weight-control behaviors.
This is even true for morbid obesity, a chronic condition that is hard to treat with diet, exercise, and psychological treatment alone. For this reason, in contrast to the nonsurgical treatment of obesity, bariatric surgery is becoming the treatment of choice for morbid obesity (van Hout and van Heck 2009).
Nevertheless, all roses have thorns, and this is true for bariatric surgery, too. In fact, this approach does not lead to equal results in every patient (van Hout et al. 2003): the long-term efficacy is strongly influenced by compliance to adequate dietary rules in which psychosocial factors and behavioral changes can play a major role.
In particular, a critical problem is the expected outcome of the treatment. As underlined by Kaly and colleagues (2008) there is a significant difference between the weight loss clinicians consider successful following bariatric surgery and the weight loss potential patients expect to achieve. As a general guideline, bariatric surgery is considered successful when 50 % of excess weight is lost and the weight loss is sustained up to 5 years. However, most obese patients have different expectations: in the previous study, patients declared to be “happy” after a 77 ± 9 % excess body weight loss and considered “acceptable” a 67 ± 10 % excess body weight loss. A 49 ± 14 % excess body weight loss, the gold standard for clinicians, was considered “disappointing”.
The situation does not always change after the treatment: a problem affecting some patients is body image dissatisfaction (Pecori et al. 2007; Adami et al. 1999; Morrow et al. 2008): patients with 200 pounds overweight still have body disparagement after losing 100 pounds. For example, in a recent post in a blog, some months after bariatric surgery Stella writes:
I feel like I have somewhat of a “dysmorphic” view of my body I don’t really see myself as a size 4 or a size 2 (only if they run big since I gained a few lbs) I still see myself as fat and the damn skin on my arms does not help the matters. I have such a hard time finding shirts cause of it and I can almost never find a dress cause I don’t want my arm cheese to show. I want to be normal, is this normal??? (online: http://www.shrinkingstella.com/).
The words of the woman clearly explain her situation: the weight loss was unable to modify her negative experience of the body. This expectation was linked to the common belief that the best way to improve one’s body image is to lose weight. However, recent studies have questioned this belief: dietary intervention, even if accompanied by significant weight loss, may be ineffective in reducing total body dissatisfaction (Rosen et al. 1995; Rosen 1996a). And unfortunately body disparagement has a negative effect on long-term follow-up of obesity, even the one treated using bariatric surgery: uncontrolled eating and grazing after surgery are associated with poorer and elevated psychological distress (Colles et al. 2008).
Given the importance of body image satisfaction for the quality of life of obese persons, these findings argue for the potential benefits of treatment strategies for improving appearance satisfaction for obese individuals, to improve the success of their weight-management efforts (Thompson et al. 1999). Unfortunately, obesity researchers have not yet systematically added body image interventions in their programs. Almost 20 years ago in a review on the behavioral obesity treatment literature, Rosen (1996b) did not find any study including psychological techniques specifically designed to modify body image. But today, the situation is not radically different. In their new cognitive behavioral approach to the treatment of obesity (Cooper et al. 2010) Cooper and Fairburn address the experience of the body only as potential obstacle to the acceptance of weight maintenance (Cooper et al. 2003) and not as a one of the possible causes of the disorder. Unfortunately, the results of the proposed approach are similar to the old one (Cooper et al. 2010):
Both of the main treatments resulted in an average weight loss of about ten percent of initial weight… The participants were subsequently followed-up for three years post-treatment. The great majority regained almost all the weight that they had lost with the new treatment being no better than the behavioural treatment in preventing weight regain (p. 706).
We do not agree with this vision (Riva et al. 2006). Following the emerging “embodied cognition” approach (Bermúdez et al. 1995; Clark 1997; Clancey 1997; Gallagher 2003) we consider body image as an integral part of the subjects’ identity. As noted by Gallagher (1995) the body experience is not neutral but it places constraints on intentional consciousness:
changes or distortion introduced at the level of body schema result in changes or distortions in intentional consciousness (p. 239).
In particular in this chapter we will introduce and discuss the “allocentric lock theory” (Riva 2007, 2012; Riva et al. 2012b; Riva and Gaudio 2012). Specifically, we will suggest that an allocentric negative body image that is no more updated by contrasting egocentric representations driven by perception is the common antecedent of both obesity and eating disorders (Riva 2011). In other words, these patients are locked to an allocentric (observer view) negative representation of their body that their sensory inputs are no more able to update even after dramatic body changes, including the one following either a diet or bariatric surgery. Moreover, we will discuss the possible role of virtual reality (VR) in addressing it. Specifically, we suggest that adding a 10-session experiential protocol based on virtual reality to the treatment of obesity may improve its long-term outcome.
15.2 Unlocking the Allocentric Lock
15.2.1 The Allocentric Lock Theory
Psychology and neuroscience indicate that our spatial experience, including the experience of the body, involves the integration of different sensory inputs within two different reference frames: egocentric and allocentric (Klatzky 1998; Mou et al. 2004):
-
Egocentric frame: it is referred to the body of the observer and allows him/her to locate objects relative to the body center. When we adopt an egocentric stance we represent the object relative to ourselves.
-
Allocentric frame: it is referred to space external to the perceiver. When we adopt an allocentric stance the object is represented independently of our own current relation with it.
As suggested by Byrne and Becker (2007), the transformation from egocentric to allocentric representations of space is done by neurons in different medial temporal lobe structures. If, for some reasons, this transformation is impaired, the subjects cannot use anymore the sensory inputs to update the contents of the allocentric representation of their body. This is what may be behind the body dissatisfaction experienced by many obese patients even after a significant weight loss: an altered somato representation—that is not updated by contrasting egocentric parietal representations driven by perception—priming the processing of any further body-related experience (Riva 2011). In simpler words, the egocentric perception-driven experience of the real body does not modify the allocentric memory-driven experience of a negative body: these patients are locked to an allocentric negative representation of their body (Riva 2010). However, the impossibility of using sensory inputs for updating the allocentric representation of the body—patients hate their body even after the surgery or significant weight loss—locks the patients into an unsatisfying body that may explain their depression and low quality of life (Omalu et al. 2007; Masheb et al. 2007).
15.2.2 Unlocking the Virtual Body Using Virtual Reality
The evolution of technology is providing new tools and methods for health care (Riva et al. 2004b). Between them, an emerging trend is the use of virtual reality (VR) (Satava and Jones 2002; Riva and Gamberini 2000; Riva and Gaggioli 2008).
VR consists of a three-dimensional (3D) graphical environment where a user can interface with the environment through a variety of computer peripheral devices. Using visual, aural, or haptic devices, the user can experience the environment as if it were a part of the real world (Riva and Davide 2001).
In surgery, for instance, VR is used in simulation training (Fried et al. 2010). In fact, VR allows the surgeon to interact efficiently with 3D computerized databases of medical images in real-time using his natural senses and skills (Tanoue et al. 2010). In sum, for physicians, and surgeons, the ultimate goal of VR is the presentation of virtual objects to all of the human senses in a way identical to their natural counterpart (Székely and Satava 1999).
In clinical psychology, the ultimate goal is different. VR is used to offer a new human-computer interaction paradigm in which patients are no longer simply external observers of images on a computer screen but are active participants within a computer-generated 3D virtual world (Riva et al. 2002). Moreover, VR can be considered an “embodied technology” for its effects on body perceptions (Spagnolli and Gamberini 2005): it is possible the use of VR for inducing controlled changes to the experience of the body (Riva et al. 2000a; Riva 1997; Slater et al. 2010; Lenggenhager et al. 2007).
On the one side, different authors showed that is possible to use VR both to induce illusory perceptions—e.g. a fake limb (Slater et al. 2009)—by altering the normal association between touch and its visual correlate. It is even possible to generate a body transfer illusion (Slater et al. 2010): Slater and colleagues substituted the experience of male subjects’ own bodies with a life-sized virtual human female body.
On the other side, it is also possible to use VR to improve body image (Riva 1998a, b), even in patients with eating disorders (Riva et al. 1999, 2000b, 2003) or obesity (Riva et al. 2000a, 2006).
As noted by Gallagher (1995), “[different] studies indicate that changes in various aspects of body schemata have an effect on the way subjects perceive their own body” (p. 237). Following this vision it is possible the use of VR to induce a controlled sensory rearrangement that facilitates an update of the locked allocentric representation of the body.
A possible strategy toward this goal is the adaptation to virtual reality of the imagery rescripting method developed for the treatment of post-traumatic stress disorders (Smucker et al. 1995; Riva 2011). Specifically, Riva developed a specific body image rescripting protocol based on VR that is included as part of the experiential cognitive therapy (ECT) described below.
15.2.2.1 The Proposed Approach: The Experiential Cognitive Therapy
Developed by Giuseppe Riva and his group (Riva et al. 1998, 2000a), ECT is a relatively short term (15-session in 6 weeks), patient-oriented approach that focuses on individual discovery (Riva et al. 2004a, 2006). As in the case of cognitive behavioral therapy (CBT), ECT uses a combination of nutritional, cognitive, and behavioral procedures to help the patient identify and change the maintaining mechanisms in obesity and eating disorders. However, ECT differs from the typical CBT approach in the use of VR, in its focus on empowerment and in its focus on the negative emotions related to the body:
-
Its focus on the body experience. A major reason patients want to lose weight (Rosen 1996b). The experience of the body is not addressed only as potential obstacle to the acceptance of weight maintenance (Cooper et al. 2003). As we underlined before, in line with the emerging “embodied cognition” approach (Bermúdez et al. 1995; Clark 1997; Clancey 1997; Gallagher 2003), we consider body image as an integral part of the subjects’ identity.
-
Its focus on the empowerment process. We consider a critical goal for the long-term efficacy of bariatric surgery, the ability of the patient in defining a realistic target weight range, in monitoring eating behaviors and in managing the frustration related to weight fluctuations. However, we do not consider these abilities as behavioral skills only. Here we agree with the DiClemente position (1986) that describes them as part of a broader individual dimension, defined “control self-efficacy”: “an individual’s ability to control the addictive behavior in a variety of provocative situations” (p. 303). Bandura (1989, 1997) proposed the concept of self-efficacy as an explanation of behavior and behavior change. People tend to avoid activities they believe exceed their coping abilities and undertake those they consider themselves capable of handling. Following this approach, the main strategy to raise self-efficacy is “empowerment”, the process of helping people feel a sense of control over their lives. Within this process there are three critical dimensions to address: (Menon 1999)
-
Perceived control. Includes beliefs about authority, decision-making skills, availability of resources, autonomy in the scheduling and performance of work, etc.;
-
Perceived competence. Reflects role-mastery, which besides requiring the skillful accomplishment of one or more assigned tasks, also requires successful coping with non-routine role-related situations;
-
Goal internalization. This dimension captures the energizing property of a worthy cause or exciting vision.
-
-
The use of virtual reality(VR). VR helps the therapist in providing the two above features of our approach: body experience treatment and empowerment. The use of a VR treatment makes it possible to induce a controlled sensory rearrangement (see Table 15.1) that facilitates an update of the locked allocentric representation of the body (Riva 1998a, c). Further, VR has the right features to support empowerment, since it is a special, sheltered setting where patients can start to explore and act without feeling threatened (Botella et al. 1998).
Table 15.1 The VR body image rescripting protocol (Adapted from Riva 2011)
ECT has been tested in different case studies and two controlled trials with 211 obese patients (Riva et al. 2006) and 36 binge eating patients (Riva et al. 2003). The two controlled trials show that ECT provides better results in the follow-up than competing approaches, including both nutritional and cognitive behavioral therapy.
15.2.2.2 The Protocol
The protocol (Riva 2011) includes five weekly group sessions aimed at improving motivation to change and assertiveness, and 10 biweekly virtual reality sessions.
The first VR session is used to assess any stimuli that could elicit abnormal eating behavior. Specifically, the attention is focused on the patient’s concerns about food, eating, shape, and weight. This assessment is normally part of the Temptation Exposure with Response Prevention protocol (Schlundt and Johnson 1990). At the end of the first VR session the therapist uses the miracle question, a typical approach used by the solution-focused brief therapy (deShazer 1985; McFarland 1995). According to this approach, the therapist asks the patient to imagine what life would be like without her/his complaint. Answering this question in writing the patient constructs her/his own solution, which then guides the therapeutic process (deShazer 1988). According to de Shazer (1988) this approach is useful for helping patients establish goals that can be used to verify the results of the therapy. Using VR to experience the effects of the miracle, the patient is more likely not only to gain an awareness of her need to do something to create change but also to experience a greater sense of personal efficacy.
The next nine VR sessions are used to assess and modify:
-
The expectations and emotions related to food and weight. This is done both by integrating different cognitive-behavioral methods: Countering, Alternative Interpretation, Label Shifting, Deactivating the Illness Belief (see Table 15.1).
-
The strategies used to cope with difficult interpersonal and potential maintenance situations. This is done both by using the Temptation Exposure with Response Prevention (Schlundt and Johnson 1990; Riva 1998c)—and by working on these three empowering dimensions (Menon 1999): perceived control, perceived competence and goal internalization.
-
The body experience of the subject. To do this the virtual environment integrates the therapeutic methods used by Butter and Cash (1987) and Wooley and Wooley (1985), and the body image rescripting protocol based on the Allocentric Lock hypothesis (see Table 15.1) (Smucker et al. 1995).
15.2.2.3 The Virtual Reality Experience
The VR sessions are based on the free NeuroVR software (http://www.neurovr.org). NeuroVR is an enhanced version of the original Virtual Reality for Body Image Modification (VEBIM) immersive virtual environment, previously used in different preliminary studies on non-clinical subjects (Riva 1997, 1998a).
NeuroVR is composed of 14 virtual environments, used by the therapist within a 60-minute session with the patient. The environments present critical situations related to the maintaining/relapse mechanisms (e.g., Home, Supermarket, Pub, Restaurant, Swimming Pool, Beach, and Gymnasium) and two body image comparison areas.
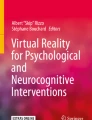
Using the NeuroVR Editor (see Fig. 15.1), the psychological stimuli/stressors appropriate for any given scenario can be chosen from a rich database of 2D and 3D objects, and easily placed into the pre-designed virtual scenario by using an icon-based interface (no programming skills are required).

The NeuroVR Editor
In addition to static objects, the NeuroVR Editor allows both to add audio object and to overlay on the 3D scene video composited with a transparent alpha channel.
The editing of the scene is performed in real time, and effects of changes can be checked from different views (frontal, lateral and top).
The edited scene is then visualized and experienced using the NeuroVR Player.
Through the VR experience, the patients practice both eating/emotional/relational management and general decision-making and problem-solving skills. By directly practicing these skills within the VR environment, the patient is helped in developing specific strategies for avoiding and/or coping with these.
Specifically, in the VR sessions the therapist uses the “20/20/20 rule”. During the first 20 min, the therapist focuses on getting a clear understanding of the patient’s current concerns, level of general functioning, and the experiences related to food. This part of the session tends to be characterized by patients doing most of the talking, although therapist guides with questions and reflection to get a sense of the patient’s current status. The second 20 min is devoted to the virtual reality experience. During this part of the session the patient enters the virtual environment and faces a specific critical situation. Here, the patient is helped in developing specific strategies for avoiding and/or coping with it. In the final 20 min, the therapist explores the patient’s understanding of what happened in VR and the specific reactions—emotional and behavioral—to the different situations experienced. If needed, some new strategies for coping with the VR situations are presented and discussed. The different techniques used in the VR sessions are detailed in Table 15.1.
15.3 Conclusions
Most clinicians and patients consider obesity just as a problem of energy input and expenditure: more energy input than expenditure. However, the clinical practice and epidemiological data clearly show that obesity is more complex than expected by this simple equation. In particular, this chapter underlined the possible role of negative body image in the etiology of this disturbance.
Specifically, we suggested that body disparagement may be produced by an allocentric negative body image that is no more updated by contrasting egocentric representations driven by perception. In other words, these subjects are locked to an allocentric (observer view) negative representation of their body that their sensory inputs are no more able to update even after dramatic body changes. The impossibility of using sensory inputs for updating the allocentric representation of the body—patients hate their body even after a significant weight loss—locks the patients into an unsatisfying body that may explain their depression, low quality of life and difficulty in maintaining an effective eating behavior (Omalu et al. 2007; Masheb et al. 2007).
How can we unlock this virtual body? This chapter suggested as possible answer an exciting new technology: virtual reality (VR). VR is well-known by surgeons: it is used in surgical training and allows the surgeon to interact efficiently with 3D computerized databases of medical images in real-time using his natural senses and skills. However, VR can be considered an “embodied technology” for its effects on body perceptions: VR can be used for inducing controlled changes to the experience of the body. In sum, it is possible the use of VR to induce a controlled sensory rearrangement that facilitates an update of the locked allocentric representation of the body.
Specifically, a specific body image rescripting protocol based on VR is part of the ECT described in this chapter. ECT is a relatively short term (five weekly group sessions aimed at improving motivation to change and assertiveness, and 10 biweekly virtual reality sessions in 6 weeks), patient-oriented approach that focuses on individual discovery. As cognitive behavioral therapy (CBT), ECT uses a combination of nutritional, cognitive, and behavioral procedures to help the patient identify and change the maintaining mechanisms in obesity and eating disorders. However, ECT differs from the typical CBT approach in the use of VR, in its focus on empowerment and in its focus on the negative emotions related to the body (Villani et al. 2012).
In the VR sessions the therapist uses the “20/20/20 rule”. During the first 20 min, the therapist focuses on getting a clear understanding of the patient’s current concerns, level of general functioning, and the experiences related to food. The second 20 min are devoted to the virtual reality experience. During this part of the session, the patient enters the virtual environment and faces a specific critical situation. In the final 20 min, the therapist explores the patient’s understanding of what happened in VR and the specific reactions—emotional and behavioral—to the different situations experienced.
ECT has been tested in different case studies and two controlled trials with 211 obese patients and 36 binge eating patients (VEPSY UPDATED-ISRCTN59019572). The two controlled trials show that ECT provides better results in the follow-up than competing approaches. This positive experience is being replicated in Mexico. The “Laboratorio de Enseñanza Virtual y Ciberpsicología” at the School of Psychology of the Universidad Nacional Autonoma de Mexico, in cooperation with the Obesity Unit of the Medica Sur Hospital in México City have recently started a controlled clinical trial, recently approved by the US ClinicalTrial.gov database (Virtual Environments For Supporting Obesity Treatment—AVATOB-NCT01394393). The trial, that will include 60 morbid obese patients both treated with bariatric surgery and without it, started its work in June 2011 and is expected to complete in 2013.
Even if the final results are not available yet, recently we reported (Riva et al. 2012a, b) the clinical case of Patricia, a 44-year-old woman, who entered in the bariatric protocol with a weight of 114 kg., 1.55 m. tall and a B.M.I. of 47. Even if at the start of the protocol her weight was 80.2 kg (a 30 % body weight loss and a 62 % excess body weight loss), the weight loss achieved after the surgery was unable to modify her negative experience of the body: she expressed the need to improve self-esteem, be more attractive, and also be more attractive to others. Moreover, the clinical data underlined a moderate level of depression matched by a high level of body dissatisfaction. The clinical data after the treatment showed a significant improvement in all the psychological variables matched both by an improvement in the subjective physical and emotional well-being, and by relevant behavioral changes in the personal and social daily life.
In conclusion, the available clinical data suggest the added value of ECT as part of an integrated obesity treatment based on the experiential approach allowed by virtual reality. Longer follow-up data and multi-centric trials are required to investigate the possible effects of the behavioral and body image changes on the long-term maintenance of the weight loss.
References
Adami GF, Meneghelli A, Bressani A, Scopinaro N (1999) Body image in obese patients before and after stable weight reduction following bariatric surgery. J Psychosom Res 46(3):275–281. doi:S0022399998000944
Bandura A (1989) Social cognitive theory. In: Vasta R (ed) Annals of child development, vol 6., Six theories of child developmentJAI Press, Greenwich, pp 1–60
Bandura A (1997) Self-efficacy: The exercise of control. W H Freeman and Co., New York
Bermúdez J, Marcel AJ, Eilan N (1995) The body and the self. MIT Press, Cambridge
Botella C, Perpiña C, Baños RM, Garcia-Palacios A (1998) Virtual reality: a new clinical setting lab. Studies in Health Technology and Informatics 58:73–81
Butters JW, Cash TF (1987) Cognitive-behavioral treatment of women’s body image satisfaction: a controlled outcome-study. J Consult Clin Psychol 55:889–897
Byrne P, Becker S, Burgess N (2007) Remembering the past and imagining the future: a neural model of spatial memory and imagery. Psychol Rev 114(2):340–375
Clancey WJ (1997) Situated cognition: on human knowledge and computer representation. Cambridge University Press, Cambridge
Clark A (1997) Being there: putting brain body and world together again. MIT Press, Cambridge
Colles SL, Dixon JB, O’Brien PE (2008) Grazing and loss of control related to eating: two high-risk factors following bariatric surgery. Obesity (Silver Spring) 16(3):615–622. doi:oby200710110.1038/oby.2007.101
Cooper Z, Doll HA, Hawker DM, Byrne S, Bonner G, Eeley E, O’Connor ME, Fairburn CG (2010) Testing a new cognitive behavioural treatment for obesity: a randomized controlled trial with three-year follow-up. Behav Res Ther 48(8):706–713. doi:10.1016/j.brat.2010.03.008
Cooper Z, Fairburn CG, Hawker DM (2003) Cognitive-behavioral treatment of obesity: a clinician’s guide. Guilford Publications, Inc., New York
deShazer S (1985) Keys to solutions in brief therapy. W.W. Norton, New York
deShazer S (1988) Clues: investigating solutions in brief therapy. Norton, New York
DiClemente CC (1986) Self-efficacy and the addictive behaviors. J Soc Clin Psychol 4:302–315
Fried MP, Sadoughi B, Gibber MJ, Jacobs JB, Lebowitz RA, Ross DA, Bent JP 3rd, Parikh SR, Sasaki CT, Schaefer SD (2010) From virtual reality to the operating room: the endoscopic sinus surgery simulator experiment. Otolaryngol Head Neck Surg 142(2):202–207. doi:S0194-5998(09)01772-010.1016/j.otohns.2009.11.023
Friend S, Bauer KW, Madden TC, Neumark-Sztainer D (2012) Self-weighing among adolescents: associations with body mass index, body satisfaction, weight control behaviors, and binge eating. J Acad Nutr Diet 112(1):99–103. doi:10.1016/j.jada.2011.08.036
Gallagher S (1995) Body schema and intentionality. In: Bermúdez JL, Marcel A, Eilan N (eds) The body and the self, vol 225–244. MIT Press, Cambridge, MA
Gallagher S (2003) Bodily self-awareness and object perception. Theoria et Historia Scientiarum: International Journal for Interdisciplinary Studies 7 (1):online: http://www2.canisius.edu/~gallaghr/theoria03.html
Haines J, Neumark-Sztainer D (2006) Prevention of obesity and eating disorders: a consideration of shared risk factors. Health Educ Res 21(6):770–782
Johnston JM (2004) Eating disorders and childhood obesity: who are the real gluttons? CMAJ 171(12):1459–1460. doi:171/12/145910.1503/cmaj.1041111
Kaly P, Orellana S, Torrella T, Takagishi C, Saff-Koche L, Murr MM (2008) Unrealistic weight loss expectations in candidates for bariatric surgery. Surg Obes Relat Dis 4(1):6–10. doi:S1550-7289(07)00715-010.1016/j.soard.2007.10.012
Klatzky RL (1998) Allocentric and egocentric spatial representations: definitions, distinctions and interconnections. In: Freska C, Habel C, Wender KF (eds) Spatial Cognition: an interdisciplinary approach to representation and processing of spatial knowledge. Springer-Verlag, Berlin, pp 1–17
Kostanski M, Gullone E (1999) Dieting and body image in the child’s world: conceptualization and behavior. J Genet Psychol 160(4):488–499
Lenggenhager B, Tadi T, Metzinger T, Blanke O (2007) Video ergo sum: manipulating bodily self-consciousness. Science 317(5841):1096–1099. doi:317/5841/109610.1126/science.1143439
Masheb RM, White MA, Toth CM, Burke-Martindale CH, Rothschild B, Grilo CM (2007) The prognostic significance of depressive symptoms for predicting quality of life 12 months after gastric bypass. Compr Psychiatry 48(3):231–236. doi:S0010-440X(07)00014-410.1016/j.comppsych.2007.01.005
McFarland B (1995) Brief therapy and eating disorders. Jossey-Bass Publishers, San Francisco
Menon ST (1999) Psychological empowerment: definition, measurement, and validation. Canadian Journal of Behavioural Science 31(3):161–164
Morrow J, Gluck M, Lorence M, Flancbaum L, Geliebter A (2008) Night eating status and influence on body weight, body image, hunger, and cortisol pre- and post- Roux-en-Y Gastric Bypass (RYGB) surgery. Eat Weight Disord 13(4):e96–e99 5219 [pii]
Mou W, McNamara TP, Valiquette CM, Rump B (2004) Allocentric and egocentric updating of spatial memories. J Exp Psychol Learn Mem Cogn 30(1):142–157
Neumark-Sztainer D (2009) Preventing obesity and eating disorders in adolescents: what can health care providers do? J Adolesc Health 44(3):206–213. doi:S1054-139X(08)00663-010.1016/j.jadohealth.2008.11.005
Neumark-Sztainer D, Wall M, Guo J, Story M, Haines J, Eisenberg M (2006) Obesity, disordered eating, and eating disorders in a longitudinal study of adolescents: how do dieters fare 5 years later? J Am Diet Assoc 106(4):559–568. doi:S0002-8223(06)00004-610.1016/j.jada.2006.01.003
Neumark-Sztainer D, Wall M, Story M, Standish AR (2012) Dieting and unhealthy weight control behaviors during adolescence: associations with 10-year changes in body mass index. J adolesc health: off publ Soc adolesc Med 50(1):80–86. doi:10.1016/j.jadohealth.2011.05.010
Omalu BI, Ives DG, Buhari AM, Lindner JL, Schauer PR, Wecht CH, Kuller LH (2007) Death rates and causes of death after bariatric surgery for Pennsylvania residents, 1995–2004. Arch Surg 142 (10):923–928; discussion 929. doi:142/10/923 [pii] 10.1001/archsurg.142.10.923
Pecori L, Serra Cervetti GG, Marinari GM, Migliori F, Adami GF (2007) Attitudes of morbidly obese patients to weight loss and body image following bariatric surgery and body contouring. Obes Surg 17(1):68–73
Riva G (1997) The virtual environment for body-image modification (VEBIM): Development and preliminary evaluation. Presence, Teleoperators, and Virtual Environments 6(1):106–117
Riva G (1998a) Modifications of body image induced by virtual reality. Percept Mot Skills 86:163–170
Riva G (1998b) Virtual environment for body-image modification: virtual reality system for the treatment of body image disturbances. Comput Hum Behav 14(3):477–490
Riva G (1998c) Virtual Reality vs. Virtual Body: The use of virtual environments in the treatment of body experience disturbances. Cyber Psychol Behavior 1(2):129–137
Riva G (2007) Virtual Body, real pain: The Allocentric Lock Hypothesis. In: Zampini M, Pavani F (eds) Body Representation Workshop, Rovereto, Italy, 8–10 October 2007. Università degli Studi di Trento, Rovereto, Italy, p online: http://www.cimec.unitn.it/events/brw/Poster/107_abs_GIUSEPPE_RIVA.pdf
Riva G (2010) Neuroscience and Eating Disorders: The role of the medial temporal lobe. Nature Precedings, online: http://precedings.nature.com/documents/4235/. Accessed July, 2012
Riva G (2011) The key to unlocking the virtual body: virtual reality in the treatment of obesity and eating disorders. J Diabetes Sci Technol 5(2):283–292
Riva G (2012) Neuroscience and eating disorders: The allocentric lock hypothesis. Medical Hypotheses 78:254–257. doi:S0306-9877(11)00566-410.1016/j.mehy.2011.10.039
Riva G, Gamberini L (2000) Virtual reality in telemedicine. Telemedicine Journal 6(3):325–338
Riva G, Davide F (eds) (2001) Communications through virtual technologies: identity, community and technology in the communication age. emerging communication: Studies on new technologies and practices in communication. Ios Press. Online: http://www.emergingcommunication.com/volume1.html, Amsterdam
Riva G, Gaggioli A (2008) Virtual clinical therapy. Lecture Notes in Computer Sciences 4650:90–107
Riva G, Gaudio S (2012) Allocentric lock in anorexia nervosa: new evidences from neuroimaging studies. Med Hypotheses 79(1):113–117
Riva G, Bacchetta M, Baruffi M, Rinaldi S, Molinari E (1998) Experiential cognitive therapy in anorexia nervosa. Eating and Weight Disorders 3:141–150
Riva G, Bacchetta M, Baruffi M, Rinaldi S, Molinari E (1999) Virtual reality based experiential cognitive treatment of anorexia nervosa. J Behav Therap Exp Psychiatr 30(3):221–230
Riva G, Bacchetta M, Baruffi M, Rinaldi S, Vincelli F, Molinari E (2000a) Virtual reality based experiential cognitive treatment of obesity and binge-eating disorders. Clin Psychol Psychotherap 7(3):209–219
Riva G, Bacchetta M, Baruffi M, Rinaldi S, Vincelli F, Molinari E (2000b) Virtual reality-based experiential cognitive treatment of obesity and binge-eating disorders. Clin Psychol Psychotherap 7(3):209–219
Riva G, Marchi S, Molinari E (2000c) Body image and eating restraint: a structural modeling analysis. Eat Weight Disord 5(1):38–42
Riva G, Bacchetta M, Cesa G, Conti S, Molinari E (2003) Six-month follow-up of in-patient experiential-cognitive therapy for binge eating disorders. CyberPsychol Behav 6(3):251–258
Riva G, Botella C, Légeron P, Optale G (eds) (2004a) Cybertherapy: Internet and Virtual Reality as Assessment and Rehabilitation Tools for Clinical Psychology and Neuroscience. IOS Press; Online: http://www.cybertherapy.info/pages/book3.htm, Amsterdam
Riva G, Vatalaro F, Davide F, Alcañiz M (eds) (2004b) Ambient intelligence: the evolution of technology, communication and cognition towards the future of human-computer interaction. IOS Press. On-line: http://www.emergingcommunication.com/volume6.html, Amsterdam
Riva G, Bacchetta M, Cesa G, Conti S, Castelnuovo G, Mantovani F, Molinari E (2006) Is severe obesity a form of addiction? Rationale, clinical approach, and controlled clinical trial. CyberPsychol Behav 9(4):457–479
Riva G, Cárdenas-López G, Duran X, Torres-Villalobos GM, Gaggioli A (2012a) Virtual reality in the treatment of body image disturbances after bariatric Surgery: a clinical case. Stud Health Technol Inform 181:54–59
Riva G, Castelnuovo G, Cesa G, Gaggioli A, Mantovani F, Molinari E (2012b) Virtual reality for enhancing the cognitive behavioral treatment of obesity: a controlled Study with one-year follow-up. In: Medicine 2.0′12 Boston
Riva G, Molinari E, Vincelli F (2002) Interaction and presence in the clinical relationship: virtual reality (VR) as communicative medium between patient and therapist. IEEE Trans Inf Technol Biomed 6(3):198–205
Rosen JC (1996a) Body image assessment and treatment in controlled studies of eating disorders. Int J Eat Disord 19:341–343
Rosen JC (1996b) Improving body image in obesity. In: Thompson JK (ed) Body image, eating disorders and obesity. American Psychological Association, Washington, pp 425–440
Rosen JC, Orosan P, Reiter J (1995) Cognitive behavior therapy for negative body image in obese women. Behav Ther 26:25–42
Satava RM, Jones SB (2002) Medical applications of virtual reality. In: Stanney KM (ed) Handbook of virtual environments: design, implementation, and applications. Lawrence Erlbaum Associates, Inc., Mahwah, pp 368–391
Schlundt DG, Johnson WG (1990) Eating disorders: assessment and treatment. Allyn and Bacon, Needham Heights
Singh GK, Kogan MD, Van Dyck PC, Siahpush M (2008) Racial/Ethnic, Socioeconomic, and Behavioral Determinants of Childhood and Adolescent Obesity in the United States: Analyzing Independent and Joint Associations. Ann Epidemiol 18(9):682–695
Slater M, Perez-Marcos D, Ehrsson HH, Sanchez-Vives MV (2009) Inducing illusory ownership of a virtual body. Front Neurosci 3(2):214–220. doi:10.3389/neuro.01.029.2009
Slater M, Spanlang B, Sanchez-Vives MV, Blanke O (2010) First person experience of body transfer in virtual reality. PLoS ONE 5(5):e10564. doi:10.1371/journal.pone.0010564
Smucker MR, Dancu C, Foa EB, Niederee JL (1995) Imagery rescripting: a new treatment for survivors of childhood sexual abuse suffering from posttraumatic stress. J Cogn Psychotherap 9:3–17
Spagnolli A, Gamberini L (2005) A place for presence. understanding the human involvement in mediated interactive environments. Psychology Journal 3 (1):6-15. On-line: http://www.psychnology.org/article801.htm
Stice E, Presnell K, Shaw H, Rohde P (2005) Psychological and behavioral risk factors for obesity onset in adolescent girls: a prospective study. J Consult Clin Psychol 73(2):195–202
Stice E, Davis K, Miller NP, Marti CN (2008) Fasting increases risk for onset of binge eating and bulimic pathology: a 5-year prospective study. J Abnorm Psychol 117(4):941–946. doi:2008-16252-01910.1037/a0013644
Székely G, Satava RM (1999) Virtual reality in medicine. Bmj 319(7220):1305
Tanoue K, Uemura M, Kenmotsu H, Ieiri S, Konishi K, Ohuchida K, Onimaru M, Nagao Y, Kumashiro R, Tomikawa M, Hashizume M (2010) Skills assessment using a virtual reality simulator, LapSim, after training to develop fundamental skills for endoscopic surgery. Minim Invasive Ther Allied Technol 19(1):24–29. doi:10.3109/13645700903492993
Thompson JK, Heinberg LJ, Altabe M, Tantleff-Dunn S (1999) Exacting beauty: Theory, assessment and treatment of body image disturbance. American Psychological Association, Washington DC
van Hout GC, van Heck GL (2009) Bariatric psychology, psychological aspects of weight loss surgery. Obes Facts 2(1):10–15. doi:00019356410.1159/000193564
van Hout GC, Leibbrandt AJ, Jakimowicz JJ, Smulders JF, Schoon EJ, Van Spreeuwel JP, van Heck GL (2003) Bariatric surgery and bariatric psychology: general overview and the Dutch approach. Obes Surg 13(6):926–931. doi:10.1381/096089203322618795
Villani D, Gatti E, Confalonieri E, Riva G (2012). Am I my avatar? A tool to investigate virtual body image representation in adolescence. CyberPsych Behav Soc Netw 15(8):435-440
Wooley SC, Wooley OW (1985) Intensive out-patient and residential tratment for bulimia. In: Garner DM, Garfinkel PE (eds) Handbook of psychotherapy for anorexia and bulimia. Guilford Press, New York, pp 120–132
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2013 Springer-Verlag Berlin Heidelberg
About this chapter
Cite this chapter
Riva, G., Cipresso, P., Mantovani, F., Dakanalis, A., Gaggioli, A. (2013). New Technologies for Improving the Psychological Treatment. In: Capodaglio, P., Faintuch, J., Liuzzi, A. (eds) Disabling Obesity. Springer, Berlin, Heidelberg. https://doi.org/10.1007/978-3-642-35972-9_15
Download citation
DOI: https://doi.org/10.1007/978-3-642-35972-9_15
Published:
Publisher Name: Springer, Berlin, Heidelberg
Print ISBN: 978-3-642-35971-2
Online ISBN: 978-3-642-35972-9
eBook Packages: Biomedical and Life SciencesBiomedical and Life Sciences (R0)