
Abstract
In nontraumatic osteonecrosis (ON) of the femoral head, several abnormalities in the coagulation-fibrinolysis system have been reported, including increase of plasminogen activator inhibitor-1 level [1], the presence of antiphospholipid antibodies [2], familial heterozygous protein S deficiency [3], and antithrombin III deficiency [4]. These abnormalities are thought to induce hypercoagulability in the blood vessels.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
- Japanese White Rabbit
- Methylprednisolone Acetate
- Gluteus Medius Muscle
- Warfarin Plus
- Platelet Aggregation Assay
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
1 Corticosteroid-Induced Animal Model for ON
In nontraumatic osteonecrosis (ON) of the femoral head, several abnormalities in the coagulation-fibrinolysis system have been reported, including increase of plasminogen activator inhibitor-1 level [1], the presence of antiphospholipid antibodies [2], familial heterozygous protein S deficiency [3], and antithrombin III deficiency [4]. These abnormalities are thought to induce hypercoagulability in the blood vessels.
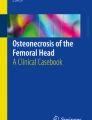
Based on several animal ON model experiments, the relationship between hypercoagulability and corticosteroid-induced ON was also indicated [5–7]. Corticosteroid-induced osteonecrosis was firstly developed in rabbits, in which high-dose methylprednisolone (MPSL) (20 mg/kg) can induce multifocal ON in conjunction with thrombocytopenia, hypofibrinogenemia, and hyperlipemia (Fig. 33.1). In this model, the blood platelet levels significantly decreased 1 week after the injection of MPSL (p < 0.05) and then gradually recovered and reached almost a normal level or even a little higher after 5 weeks. Histologically, an organizing thrombus was observed in the intraosseous arteriole, indicating the presence of some degree of coagulopathy .



(a) The macroscopical appearance of ON in the femur and humerus 4 weeks after corticosteroid injection. The yellowish-colored areas (arrows) mainly located in the metaphysis represent osteonecrosis area. (b) The sequential changes in the blood platelet levels. Although there was no significant difference between the rabbits with ON (ON+) and those without ON (ON−), the blood platelet levels significantly decreased 1 week after the injection of MPSL (p < 0.05) and then gradually recovered and reached almost a normal level after 5 weeks. ON osteonecrosis. (c) Morphological changes in the vessels of the femur 4 weeks after corticosteroid injection. An organizing thrombus is seen in the intraosseous arteriole, which is accompanied with fibrinous exudate in its wall, just adjacent to the ON in the metaphysis (hematoxylin and eosin, ×200) (Permission from Yamamoto et al. [5])
Based on this animal model for ON, several investigations for the prevention of ON has recently been reported [6–9].
2 Combined Effects of Warfarin and Lipid-Lowering Agent [6]
In 2004, combined effects of warfarin and lipid-lowering agent (probucol) on the prevention of corticosteroid-induced ON have been proposed for the prevention of corticosteroid-induced ON [6].
Male adult Japanese white rabbits were injected once intramuscularly with 20 mg/kg of methylprednisolone acetate (MPSL) into the right gluteus medius muscle. These rabbits were divided into four groups, (1) warfarin plus probucol (WP group, n = 25), (2) probucol alone (PA group, n = 30), (3) warfarin alone (WA group, n = 26), or (4) no treatment (non-prophylactic (NP) group, n = 20). Both the femora and humeri were histopathologically examined for the presence of ON 2 weeks after the MPSL injection and hematological examinations before and after steroid injection were performed.
The incidence of ON in the WP group (5 %) was significantly lower than that observed in the NP group (70 %) (p < 0.0001). While the incidences of ON in the PA and WA groups (37 and 33 %, respectively) were also significantly lower than that seen in the NP group (p < 0.05), they were significantly higher than that in the WP group (p < 0.01 and p < 0.05, respectively) (Fig. 33.2).

The incidence of osteonecrosis (ON) in the warfarin plus probucol treatment group (WP group, 5 %) was significantly lower than that seen in the non-prophylactic treatment group (NP group, 70 %) (p < 0.0001). While the incidence of ON in the probucol treatment group (PA group, 37 %) and the warfarin treatment group (WA group, 33 %) was significantly lower than that observed in the NP group (p < 0.05), these levels are significantly higher than those seen in the WP group (p < 0.01 and p < 0.05, respectively) (Reproduced from Motomura et al. [6])
The levels of PT-INR in both the WP and WA groups were significantly higher (p < 0.01, p < 0.05, respectively) than those observed in either the NP or PA group throughout the experimental period (Fig. 33.3a). The LDL levels in the WP group remained at significantly lower levels at all the time points tested than those seen in the NP and WA groups (p < 0.05, Fig. 33.3b). The PA group showed significantly lower LDL levels during the study than the NP or WA groups (p < 0.05, Fig. 33.3a). The plasma LDL/HDL cholesterol ratios were significantly lower in the WP group than those in the NP group at all of the time points tested (p < 0.05). The LDL/HDL cholesterol ratios observed in the PA group were also significantly lower than those in the NP group (p < 0.05) at every time point (Fig. 33.3c). There were no significant differences in plasma lipid levels (LDL, VLDL, triglyceride, and LDL/HDL cholesterol) between the WP and PA groups (Fig. 33.3a, b).

(a) The levels of PT-INR in the WP group were significantly higher than those seen in either the NP or PA groups during the experimental period (p < 0.01). The PT-INR levels in the WA group were also significantly higher than those in NP or PA groups at any of the time points tested (p < 0.05). (b) The LDL levels in the WP group remained significantly lower than those seen in the NP or WA groups at all of the time points tested (p < 0.05). The PA group also exhibited significantly lower LDL levels than the NP or WA groups throughout the study (p < 0.05). (c) Plasma LDL/HDL cholesterol ratios were significantly lower in the WP group than that seen in the NP group at all of the time points tested (p < 0.05). The LDL/HDL cholesterol ratios in the PA group were also significantly lower than those in the NP group at any time point examined (p < 0.05) (Reproduced from Motomura et al. [6])
3 Effects of Antiplatelet Drug [7]
In 2010, the effects of antiplatelet drug (clopidogrel) on the prevention of corticosteroid-induced ON have been proposed [7].
Sixty-five adult male Japanese white rabbits ranging in age from 28 to 32 weeks were used. The body weight was 3,490 ± 180 g (mean ± SD). These rabbits were randomly divided into two groups. One group received 5 mg/kg of body weight of clopidogrel (Sanofi-Aventis, Paris, France) mixed with normal saline (5 ml/kg/day) which was administered intragastrically through a rubber gastric tube into the stomach (AP group; n = 35). The other group received normal saline alone (5 ml/kg/day) intragastrically (NS group; n = 30). All rabbits were given the drug or normal saline once daily for 3 weeks. One week after the initiation of the study, all rabbits were injected intramuscularly 20 mg/kg of body weight of methylprednisolone acetate (MPSL; Pfizer, New York, USA) into the right gluteus medius muscle. Both the femora and humeri were examined histopathologically for the presence of ON 3 weeks later. Both the platelet aggregation assay and hematologic examinations were performed before and after the MPSL injection.
The incidence of ON in the AP group (48.5 %) was significantly lower than that observed in the NS group (73.3 %) (Fig. 33.4). The platelet aggregations in the AP group were significantly inhibited by the administration of clopidogrel. The levels of total cholesterol and triglycerides showed no significant differences between the AP and NS group.

The incidence of ON in each group. The incidence of ON in the AP group (48.5 %) was significantly lower than that observed in the NS group (73.3 %)
4 Perspective
Corticosteroids, a classic risk factor of ON, are known to induce hyperlipidemia as well as a hypercoagulable and hypofibrinolytic state of plasma. The pathogenesis of nontraumatic ON is generally considered to be multifactorial, and it seems that no one factor adequately accounts for the development of ON. Combination treatments, such as anti-coagulopathy drugs and lipid-lowering agents, seem to be the useful candidates for considering the prevention of corticosteroid-induced ON.
References
Glueck CJ, Freiberg R, Glueck HI, et al. Hypofibrinolysis: a common, major cause of osteonecrosis. Am J Hematol. 1994;45:156–66.
Korompilias AV, Gilkeson GS, Ortel TL, Seaber AV, Urbaniak JR. Anticardiolipin antibodies and osteonecrosis of the femoral head. Clin Orthop. 1997;345:174–80.
Pierre-Jacques H, Glueck CJ, Mont MA, Hungerford DS. Familial heterozygous protein-S deficiency in a patient who had multifocal osteonecrosis. A case report. J Bone Joint Surg. 1997;79A:1079–84.
Kubo Kubo T, Tsuji H, Yamamoto T, Nakahara H, Nakagawa M, Hirasawa Y. Antithrombin III deficiency in a patient who had multifocal osteonecrosis. Clin Orthop Relat Res. 2000;378:306–11.
Yamamoto AR, Yamamoto T, Irisa T, Sugioka Y, Sueishi K. Effects of pulse methylprednisolone on bone and marrow tissues. Corticosteroid-induced osteonecrosis in rabbits. Arthritis Rheum. 1997;40:2055–64.
Motomura Motomura G, Yamamoto T, Miyanishi K, Jingushi S, Iwamoto Y. Combined effects of an anticoagulant and a lipid-lowering agent on the prevention of steroid-induced osteonecrosis in rabbits. Arthritis Rheum. 2004;50:3387–91.
Yamaguchi Yamaguchi R, Yamamoto T, Motomura G, Ikemura S, Iwasaki K, Zhao G, Iwamoto Y. Effects of an anti-platelet drug on the prevention of steroid-induced osteonecrosis in rabbits. Rheumatology. 2012;51:789–93.
Nishida Nishida K, Yamamoto T, Motomura G, Jingushi S, Iwamoto Y. Pitavastatin may reduce risk of steroid-induced osteonecrosis in rabbits. Clin Orthop Relat Res. 2008;466:1054–8.
Ikemura Ikemura S, Yamamoto T, Motomura G, Yamaguchi R, Zhao G, Iwasaki K, Iwamoto Y. Preventive effects of the anti-vasospasm agent via the regulation of the Rho-kinase pathway on the development of steroid-induced osteonecrosis in rabbits. Bone. 2013;53:329–35.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2014 Springer-Verlag Berlin Heidelberg
About this chapter
Cite this chapter
Yamamoto, T., Motomura, G., Yamaguchi, R., Iwamoto, Y. (2014). The Role of Coagulopathy in the Pathogenesis and Prevention of Corticosteroid-Induced Osteonecrosis. In: Koo, KH., Mont, M., Jones, L. (eds) Osteonecrosis. Springer, Berlin, Heidelberg. https://doi.org/10.1007/978-3-642-35767-1_33
Download citation
DOI: https://doi.org/10.1007/978-3-642-35767-1_33
Published:
Publisher Name: Springer, Berlin, Heidelberg
Print ISBN: 978-3-642-35766-4
Online ISBN: 978-3-642-35767-1
eBook Packages: MedicineMedicine (R0)