
Abstract
Avascular necrosis (AVN) of the femoral head is a rare but devastating complication following fractures of the proximal femur or hip dislocation. Traumatic AVN derives from the interruption of the blood flow to the femoral head, which is mainly supplied by the medial circumflex femoral artery (MCFA) in the adult hip [1, 2]. The incidence of AVN depends on the fracture pattern and the integrity of the deep branch of the MCFA. In addition to traumatic interruption of the femoral head blood supply, the MCFA can be injured iatrogenically. Symptoms and radiographic changes in hips with AVN of the femoral head usually occur late and often months after the trauma. There is no curative treatment and therefore prevention is most important. While total hip arthroplasty shows very good clinical results in elderly patients, it is not the treatment of choice in children and adolescents with AVN. For this age group, hip preserving alternatives include core decompression, femoral osteotomies, and various bone grafting techniques.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
1 Introduction
Avascular necrosis (AVN) of the femoral head is a rare but devastating complication following fractures of the proximal femur or hip dislocation. Traumatic AVN derives from the interruption of the blood flow to the femoral head, which is mainly supplied by the medial circumflex femoral artery (MCFA) in the adult hip [1, 2]. The incidence of AVN depends on the fracture pattern and the integrity of the deep branch of the MCFA. While fractures with close proximity to the nutrient vessels (femoral head and neck fractures) have a considerable risk for AVN, AVN rarely occurs in fractures which do not interfere with the MCFA (intertrochanteric or femoral shaft fractures). In addition to traumatic interruption of the femoral head blood supply, the MCFA can be injured iatrogenically. Symptoms and radiographic changes in hips with AVN of the femoral head usually occur late and often months after the trauma. There is no curative treatment and therefore prevention is most important.
This article (1) describes the pathophysiology of AVN with a special focus on the vascular anatomy of the femoral head, (2) reports on the different modalities to assess the integrity of the nutrient vessels, (3) compares the different injury patterns and their associated risk of AVN, and (4) provides information to prevent iatrogenic damage to the blood supply of the femoral head.
2 Blood Supply to the Femoral Head
2.1 Vascular Anatomy of the Femoral Head
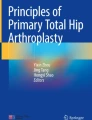
Precise knowledge of the vascular anatomy of the femoral head helps to understand the etiology of traumatic AVN. The deep branch of the MCFA provides the main blood supply to the femoral head [1, 2]. Most commonly, it arises from the deep femoral artery or, alternatively, from the common femoral artery (Fig. 14.1). There are five constant branches of the MCFA. Of these, the most relevant for the femoral head perfusion is the deep branch of the MCFA [1, 2]. It runs posteriorly towards the intertrochanteric crest between the pectineus muscle medially and the iliopsoas tendon laterally (Fig. 14.1). The deep branch of the MCFA then runs along the inferior border of the obturator externus muscle, which is the most important structure to protect the course of the MCFA (Fig. 14.1). As long as the obturator externus muscle is in continuity, the deep branch of the MCFA is not under relevant tension even with the femoral head dislocated [1]. After crossing the obturator externus tendon posteriorly, a constant trochanteric branch is given off which runs between the quadratus femoris muscle and the triceps coxae (gemelli and obturator internus muscles; Fig. 14.1). The deep branch of the MCFA continues cranially and ventrally to the triceps coxae muscles and penetrates the joint capsule at the level of the superior border of the gemellus superior muscle (Fig. 14.1). At the posterosuperior aspect of the femoral neck, it splits up into four to five retinacular vessels (Fig. 14.1). The retinacular vessels lie extraosseously but intracapsularly and enter the head 2–4 mm lateral to the bone-cartilage junction.

Vascular anatomy of the femoral head. (a) The deep branch of the medial circumflex femoral artery (MCFA) runs towards the intertrochanteric crest between the pectineus muscle medially and the iliopsoas tendon laterally. (b) The MCFA then runs along the inferior border of the obturator externus muscle. (c) After crossing the obturator externus tendon posteriorly, a trochanteric branch is given off which runs between the quadratus femoris muscle and the triceps coxae (gemelli and obturator internus muscles). The deep branch of the MCFA continues cranially and ventrally to the triceps coxae muscle and enters the joint capsule at the level of the superior border of the gemellus superior muscle. (d) At the posterosuperior aspect of the femoral neck, it splits up into four to five retinacular vessels which enter the head (Reprinted with permission Tannast et al. [3])
Multiple anastomoses with the MCFA exist [1]. The most important anastomosis regarding femoral head perfusion is a branch of the inferior gluteal artery, which runs along the piriformis muscle [1, 4]. It could be shown that this vessel has the capacity to compensate for an interruption of the blood supply of the afferent portion of the MCFA [5]. The lateral circumflex femoral artery or the ligamentum teres arteries contribute very little to head perfusion [2]. Usually, the intraosseous blood flow cannot compensate for an intracapsular injury to the deep branch of the MCFA. Therefore, in clinical practice, viability of the femoral head directly depends on the integrity of the MCFA.
2.2 Assessment of the Integrity of the Nutrient Vessels of the Femoral Head
Damage to the MCFA can theoretically occur by direct traumatic injury from the accident (i.e., rupture of the vessel), kinking due to fracture and/or joint dislocation, thrombosis, vasospasm, or iatrogenic injury (e.g., forced closed reduction, surgical approach, hardware insertion).
2.2.1 Preoperative Modalities for Detection of an Interrupted Blood Supply to the Femoral Head
A reliable, clinically routinely usable, preoperative technique to diagnose an injury of the MCFA with interruption of the blood supply to the femoral head does not exist. Direct visualization of the nutrient vessels to the femoral head is possible by angiography [5, 6]. It can show the interruption of the MCFA but is unable to show the ultimate perfusion of femoral head. Two historic studies [5, 6] tried to correlate the angiographic results in proximal femoral fractures with the occurrence of AVN at most recent follow-up. In hips with preserved blood supply to the femoral head in the angiography, AVN occurred very rarely. In contrast, if the preoperative blood supply to the femoral head was interrupted in the angiography, this did not necessarily end up in an AVN. In these cases, the blood supply can sometimes even be restored by simple closed internal rotation of the hip in femoral neck fractures or after open reduction and internal fixation [6, 7]. This supports the theory of a transient kinking and/or vasospasm of the nutrient vessels. Despite its utility, angiography has not become part of the routine clinical follow-up. Nowadays, CT angiography may be a promising noninvasive alternative to conventional angiography [8]. The MCFA and its anastomoses can be visualized in detail with this technique [8]. However, similar to classic angiography, the terminal intraosseous blood flow to the femoral head is not visible. The usability of this technique in clinical routine has not yet been proven.
There are two imaging modalities that can show the preoperative femoral head vascularity with proximal femoral fractures. The first modality is the dynamic magnetic resonance imaging (MRI), which monitors quantitatively the flow of an intravenously applied contrast agent in the femoral head [9]. The signal intensity of the fractured side before and after application of gadolinium is then compared to the unaffected side. Similarly, bone scintigraphy (as the second modality) uses an intravenously applied radiographic tracer [10, 11]. Unlike dynamic MRI, this method reveals more qualitative results. Despite relative promising results of these two techniques, neither has found its way into clinical routine use.
2.2.2 Intraoperative Assessment
One of the most reliable and technically simple methods to assess femoral head perfusion is intraoperative drilling of the femoral head [7]. After reduction of the fracture, two to four 2.0 mm drill holes are made at the base of the femoral head to assess femoral head bleeding. This requires an open approach to the hip and usually takes up to 2 min until reliable bleeding from the femoral head may be observed. If a closed reduction and percutaneous fixation is attempted, the retrograde blood flow through the cannulated screws can provide a relatively reliable assessment of the femoral head perfusion [12]. More sophisticated methods such as laser Doppler flowmetry [13] and intramedullary oxygen tension measurements [14] have been described but basically offer a lower sensitivity and specificity for prediction of AVN in comparison to direct drilling of the femoral head.
3 Injury Patterns of the Proximal Femur
The incidence of traumatic AVN of the femoral head depends on the fracture pattern and its proximity to the deep branch of the MCFA (Table 14.1). While the femoral head and neck fractures have the highest incidence of AVN (up to 40 % [18]), the incidence decreases for intertrochanteric fractures (1–5 % [17, 18, 23]), and AVN rarely occurs in femoral shaft fractures [24] (Table 14.1). Femoral head necrosis has also been reported following traumatic dislocations with an incidence ranging up to 26 % [25–27].
Fractures of the proximal femur are divided into head, neck, intertrochanteric, and femoral shaft fractures. For each fracture pattern, the etiology of AVN, the anatomical relation to the MCFA, and the incidence of AVN reported in literature are summarized.
3.1 Femoral Head Fractures
Among the different fracture types of the proximal femur, femoral head fractures have the highest incidence for AVN ranging up to 40 % (Table 14.1) [18]. Femoral head fractures typically are related to direct mechanical damage to the intraosseous blood flow from the retinacular vessels (Fig. 14.2). The vascularity of the femoral head fragment can only be reestablished by diffusion from the viable femoral head portion. Based on two systematic reviews [15, 16], an increased risk for AVN has not been found for a specific subtype of femoral head fracture or concomitant traumatic dislocation. However, in both reviews [15, 16], the risk of AVN was associated with the type of approach used for surgical treatment (Table 14.2). The highest incidence of 16 % was found for the posterior approach, followed by the trochanteric flip approach with 13 % and the anterior approach with 8 % [15, 16]. These results suggest that an iatrogenic lesion to the nutrient vessels of the femoral head may play an important role. The posterior approach to the hip can potentially be dangerous for the blood supply to the femoral head if the topographical course of the MCFA is not fully understood and respected (Fig. 14.1). If a trochanteric osteotomy is conducted, the osteotomy should exit just anterior to the most posterior insertion of the gluteus medius muscle in order to protect the deep branch of the MCFA [34].

(a) Femoral head fractures have the highest incidence of avascular necrosis (AVN) of the femoral head ranging up to 40 % [18] and typically are related to direct mechanical damage to the retinacular vessels. (b) In medial neck fractures, direct mechanical trauma to the nutrient vessel results in increased risk for AVN compared to (c) lateral neck fractures which less likely interfere with the MCFA. (d) AVN rarely occurs in hips with intertrochanteric fractures because these fractures usually do not interfere with the nutrient vessel
3.2 Femoral Neck Fractures
AVN in femoral neck fractures is typically the result of an injured retinaculum (Fig. 14.2). Several risk factors have been reported that can be attributed to the integrity of the retinacular vessels. This includes the location of neck fracture [17, 18], fracture dislocation [13, 17, 22], quality of reduction [19], delay of treatment [18, 29], and type of treatment [17, 18, 20, 21] (Table 14.2).
3.2.1 Location of Femoral Neck Fracture
Medial femoral neck fractures have an increased incidence of AVN (28 %) in comparison to lateral neck fractures (18 %, Table 14.1) [17, 18]. The increased incidence for medial neck fractures can be explained by the very close topographical relationship of the retinacular vessels and the fracture (Figs. 14.2 and 14.3). Lateral neck fractures show an increased distance between the fracture and the terminal branches of the MCFA; therefore, the fracture has less potential to damage the vessel (Fig. 14.2).

(a) A 49-year-old male patient with a medial femoral neck fracture. (b) He underwent closed reduction and screw fixation resulting in insufficient reduction and stabilization. (c) At a 1.2 year follow-up, avascular necrosis of the femoral head occurred necessitating total hip arthroplasty
3.2.2 Fracture Dislocation
Fracture dislocations of the femoral neck can be classified as varus/valgus, dorsal/ventral, and rotational (Fig. 14.4).

Neck fractures with (a) varus dislocation cause tension and possibly rupture of the retinacular vessels. (b) A mild valgus dislocation (<30°) relaxes the retinacular vessels and does not impair the blood supply [6]. (c) However, a severe valgus dislocation results in kinking of the retinacular vessels and impaired blood supply [19]. (d) A mild dorsal tilt usually does not impair perfusion of the femoral head. However, a severe dorsal tilt and, particularly, when in combination with a varus dislocation, leads to impairment of the head perfusion. (e) Rotational errors can compromise the head vascularity. Flexion of the head can stretch the retinacular vessels and result in rupture. Extension of the femoral head can result in impaired blood supply by kinking of the vessel
A varus dislocation without dorsal angulation inevitably causes tension on the retinacular vessels (Fig. 14.4). This can lead to an impairment of the femoral blood supply [6, 13]. Eventually, the vulnerable retinaculum ruptures with large dislocations. A valgus impaction without dorsal angulation theoretically relaxes the retinaculum (Fig. 14.4). Isolated valgus impactions up to 30° do not impair the blood supply to the femoral head [6]. However, large valgus impactions are associated with AVN [19] and attributed to kinking of the retinacular vessels.
A dorsal tilt of the femoral head can lead to a kinking of the posterosuperiorly located retinaculum (Fig. 14.4). A reperfusion of the femoral head can be achieved by simple (closed) internal rotation of the leg [6] or by anatomical open reduction and internal fixation [6, 13]. An additional varus dislocation can aggravate the kinking of the retinacular vessels [6].
Rotational errors at the level of the femoral neck can typically occur when performing closed reduction [35] or by excessive torque from an implant (e.g., a dynamic hip screw [36]). Rotational errors are hard to detect with fluoroscopy or conventional radiographs but can have serious consequences on the retinaculum. A flexion of the head fragment can stretch the retinaculum (Fig. 14.4). However, a large extension of the head fragment may compromise the head vascularity by kinking of the vessel (Fig. 14.4).
3.2.3 Quality of Reduction
Quality of reduction was found to be a significant predictor for AVN (Table 14.2) [19]. Severe residual varus and valgus deformities are associated with a higher incidence of AVN [19]. The same principles as mentioned above (see Sect. 14.3.2.2) apply for the integrity of the vascularity.
3.2.4 Delay of Treatment and Tamponade Effect
Delay of treatment of more than 12–24 h is associated with a higher risk of AVN (Table 14.2). This could be attributed to a tamponade effect of the retinacular vessels by hemarthrosis. Because the retinacular vessels are extraosseous and intracapsular, they may be compressed by increased hydrostatic pressure resulting from the fracture hematoma. This tamponade effect can occur in both displaced and non-displaced fractures [37–39]. This would explain the presence of AVN in undisplaced fractures [17]. The time limit of 12 h is somewhat arbitrarily chosen but could be reproduced in a canine animal model [40].
3.2.5 Type of Treatment
An increased incidence of AVN was found for neck fractures treated surgically compared to hips with nonsurgical treatment (Table 14.2). Additionally, the incidence of AVN was increased in hips with open reduction and internal fixation compared to hips with closed reduction only (Table 14.2). With an open treatment the MCFA can potentially be iatrogenically damaged. However, type of treatment might also be confounding with previously mentioned risk factors such as location of fracture or fracture dislocation.
3.3 Intertrochanteric and Greater Trochanteric Fractures
Intertrochanteric fractures are rarely associated with AVN, and the incidence ranges from 1 to 5 % (Table 14.1). Generally, these fractures do not interfere directly with the anatomical course of the deep branch of the MCFA in the adult hip (Fig. 14.2). Associated risk factors have therefore not clearly been described based on large patient cohorts. Assumed risk factors that can compromise the vascular supply are high-energy trauma, associated fractures of the base of the femoral neck, and iatrogenic vascular damage [41].
Three case reports exist for isolated fractures of the greater trochanter and femoral head necrosis [42–44]. Two patients were treated conservatively [43, 44], while one patient was treated with open reduction and screw fixation [42]. Interestingly, all cases occurred in children aged between 12 and 13 years. In adults, greater trochanteric fractures typically involve avulsion fractures of the tip. In the pediatric population, the fracture often involves the trochanteric growth plate. This results in a larger fragment of the greater trochanter which extends far medial in the femoral neck [45] and may compromise the blood supply of the MFCA (Fig. 14.5).

Radiograph of the proximal femur and angiography of the medial circumflex femoral artery (MCFA) of a 6-year-old male. Both the epiphyseal and trochanteric growth plates are clearly visible. All cases of a greater trochanteric fracture resulting in AVN of the femoral head occurred in children. These fractures often involve the trochanteric growth plate. This results in a larger fragment of the greater trochanter which extends far medial in the femoral neck and may compromise the blood supply of the MFCA [45] (Reprinted with permission Trueta [45])
3.4 Femoral Shaft Fractures
Although femoral shaft fractures generally do not interfere with the course of the MCFA, a few cases of AVN following antegrade intramedullary nailing of the femur have been reported [24]. In these cases an iatrogenic damage to the MCFA at the location of nail insertion at the proximal femur has been described [32]. For geometrical and biomechanical reasons, the piriformis fossa has been recommended as nail insertion point of straight femoral nails. However, the piriformis fossa has a high risk for iatrogenic damage to the MCFA due to its close proximity (Fig. 14.6). In a cadaver study, nail insertion in the piriformis fossa resulted in damage to the nutrient vessel in all cases with complete disruption of the MCFA in 57 % [32]. In addition, intramedullary femoral reaming may put the vascular supply of the femoral head at risk (Table 14.2). The tip of the greater trochanter was suggested as a more appropriate insertion point with the use of an anatomically shaped femoral nail [32]. The problem can be aggravated when oversized implants for adults are used in the pediatric population, which represent the majority of these cases with femoral shaft fractures and AVN of the femoral head [24] (Table 14.2).

(a) Fourteen-year-old male patient who sustained a femoral shaft fracture which was treated with antegrade intramedullary nailing. A very medial nail insertion point was chosen in close proximity to the medial circumflex femoral artery (MCFA). Eight months postoperative, avascular necrosis of the femoral head occurred. (Reprinted with permission Orler et al. [24]) (b) The risk of avascular necrosis of the femoral head following antegrade intramedullary nailing of the femur depends on the location of nail insertion [32]. In a cadaver study the use of the piriformis fossa as location of insertion with its close proximity to the MCFA showed damage to the nutrient vessel in all cases with complete disruption of the MCFA in 57% [32] (Reprinted with permission Dora et al. [32])
3.5 Traumatic Hip Dislocation
Traumatic hip dislocation is not necessarily associated with AVN. It could be shown that the obturator muscle is the most important structure to protect the MCFA in the dislocated position (Fig. 14.7) [1]. This fact is based on cadaver experiments for surgical hip dislocations [1]. As long as the obturator externus muscle is in continuity, the deep branch of the MCFA is not in danger or under relevant tension even with the femoral head dislocated [34, 47, 48]. Since the obturator externus muscle typically remains intact in traumatic hip dislocations [46], additional factors have to contribute to the reported incidence of AVN up to 26 % (Table 14.1) following traumatic hip dislocations. These additional risk factors for AVN include direction of dislocation [25], concomitant fracture [25, 26], delay of reduction [25, 27], and surgical approach [33] (Table 14.2).

Posterior traumatic hip dislocations have an increased incidence for AVN compared to anterior dislocations (29 vs. 9 %; Table 14.1) [25]. A concomitant femoral fracture may mechanically harm the nutrient vessels to the femoral head. The incidence of AVN for dislocations without fractures is zero to 22 % (Fig. 14.8) [46]. In contrast, the incidence for dislocations with a concomitant femoral head or acetabulum fracture was 66 % [25]. Early reduction may reduce the incidence of AVN [25, 27]. Based on laser Doppler studies, the femoral head blood supply can be reduced in the dislocated position, but will normalize after reduction in all hips [47]. With a delay of 6 or 12 h for reduction, the incidence increases from 5 to 59 % [27] or from 18 to 57 % [25], respectively. When performing a standard Kocher-Langenbeck approach (with or without detachment of the short external rotators), the MCFA can potentially be iatrogenically harmed. This could explain the three times higher incidence of AVN in traumatic hip dislocations with a posterior approach for internal fixation in comparison to the anterior approach [33].


(a) A 59-year-old male patient with traumatic posterior hip dislocation with a fracture of the femoral head and posterior acetabular wall. (b) Open reduction with internal fixation of the femoral head and posterior wall was performed using a trochanteric flip approach. (c) Half a year postoperative, avascular necrosis of the femoral head occurred necessitating total hip arthroplasty
4 Summary
Traumatic AVN of the femoral head derives from the interruption of the blood supply to the femoral head. The MCFA plays the key role for maintenance of the femoral head viability. The incidence of AVN varies greatly among the different fracture types of the proximal femur. It is directly correlated to the proximity of the fracture site with the topographical course of the MCFA. Preoperative noninvasive assessment of intact vascularity of the femoral head is theoretically possible with various imaging modalities. However, none of these methods has found its way into clinical routine use. The most sensitive and specific method to determine an intact vascularity is bleeding of the femoral head after intraoperative drilling. Lack of bleeding may be due to an interruption of the afferent blood supply to the femoral head, from either a definitive (e.g., rupture) or transient (e.g., vasospasm, kinking) stop of the MCFA.
References
Gautier E, Ganz K, Krugel N, Gill T, Ganz R. Anatomy of the medial femoral circumflex artery and its surgical implications. J Bone Joint Surg Br. 2000;82(5):679–83.
Sevitt S, Thompson RG. The distribution and anastomoses of arteries supplying the head and neck of the femur. J Bone Joint Surg Br. 1965;47:560–73.
Tannast M, Mack PW, Klaeser B, Siebenrock KA. Hip dislocation and femoral neck fracture: decision-making for head preservation. Injury. 2009;40(10):1118–24.
Kalhor M, Horowitz K, Gharehdaghi J, Beck M, Ganz R. Anatomic variations in femoral head circulation. Hip Int. 2012;22(3):307–12.
Brünner S, Christiansen J, Kristensen JK. Arteriographic prediction of femoral head viability in medial femoral neck fractures. Acta Chir Scand. 1967;133(6):449.
Müssbichler H. Arteriographic studies in fractures of the femoral neck and trochanteric region type and incidence of findings in pre-and postoperative examina tions, relation to fracture dislocation and prognostic value. Angiology. 1970;21(6):385–402.
Gill TJ, Sledge JB, Ekkernkamp A, Ganz R. Intraoperative assessment of femoral head vascularity after femoral neck fracture. J Orthop Trauma. 1998;12(7):474–8.
Zlotorowicz M, Czubak J, Kozinski P, Boguslawska-Walecka R. Imaging the vascularisation of the femoral head by CT angiography. J Bone Joint Surg Br. 2012;94(9):1176–9.
Hirata T, Konishiike T, Kawai A, Sato T, Inoue H. Dynamic magnetic resonance imaging of femoral head perfusion in femoral neck fracture. Clin Orthop Relat Res. 2001;393:294–301.
Bauer G, Weber DA, Ceder L, Darte L, Egund N, Hansson LI, Strömqvist B. Dynamics of technetium-99m methylenediphosphonate imaging of the femoral head after hip fracture. Clin Orthop Relat Res. 1980;152:85–92.
D’Ambrosia RD, Riggins RS, Stadalnik RC, Denardo GL. Vascularity of the femoral head: 99mTc diphosphonate scintigraphy validated with tetracycline labeling. Clin Orthop Relat Res. 1976;121:143–8.
Cho M-R, Lee S-W, Shin D-K, Kim S-K, Kim S-Y, Ko S-B, Kwun K-W. A predictive method for subsequent avascular necrosis of the femoral head (AVNFH) by observation of bleeding from the cannulated screw used for fixation of intracapsular femoral neck fractures. J Orthop Trauma. 2007;21(3):158–64.
Sugamoto K, Ochi T, Takahashi Y, Tamura T, Matsuoka T. Hemodynamic measurement in the femoral head using laser Doppler. Clin Orthop Relat Res. 1998;353:138–47.
Watanabe Y, Terashima Y, Takenaka N, Kobayashi M, Matsushita T. Prediction of avascular necrosis of the femoral head by measuring intramedullary oxygen tension after femoral neck fracture. J Orthop Trauma. 2007;21(7):456–61.
Giannoudis PV, Kontakis G, Christoforakis Z, Akula M, Tosounidis T, Koutras C. Management, complications and clinical results of femoral head fractures. Injury. 2009;40(12):1245–51.
Guo JJ, Tang N, Yang HL, Qin L, Leung KS. Impact of surgical approach on postoperative heterotopic ossification and avascular necrosis in femoral head fractures: a systematic review. Int Orthop. 2010;34(3):319–22.
Moon ES, Mehlman CT. Risk factors for avascular necrosis after femoral neck fractures in children: 25 Cincinnati cases and meta-analysis of 360 cases. J Orthop Trauma. 2006;20(5):323–9.
Yeranosian M, Horneff JG, Baldwin K, Hosalkar HS. Factors affecting the outcome of fractures of the femoral neck in children and adolescents a systematic review. J Bone Joint Surg Am. 2013;95(1):135–42.
Garden RS. Malreduction and avascular necrosis in subcapital fractures of the femur. J Bone Joint Surg Br. 1971;53(2):183–97.
Holmberg S, Kalén R, Thorngren KG. Treatment and outcome of femoral neck fractures an analysis of 2418 patients admitted from their own homes. Clin Orthop Relat Res. 1987;218:42–52.
Johnson JT, Crothers O. Nailing versus prosthesis for femoral-neck fractures. A critical review of long-term results in two hundred and thirty-nine consecutive private patients. J Bone Joint Surg Am. 1975;57(5):686–92.
Strömqvist B, Hansson LI, Nilsson LT, Thorngren K-G. Hook-pin fixation in femoral neck fractures a two-year follow-up study of 300 cases. Clin Orthop Relat Res. 1987;218:58–62.
Aguado-Maestro I, Escudero-Marcos R, Garcia-Garcia JM, Alonso-Garcia N, Perez-Bermejo DD, Aguado-Hernandez HJ, Nistal-Rodriguez J, Garcia-Alonso M. Results and complications of pertrochanteric hip fractures using an intramedullary nail with a helical blade (proximal femoral nail antirotation) in 200 patients. Rev Esp Cir Ortop Traumatol. 2013;57(3):201–7.
Orler R, Hersche O, Helfet DL, Mayo KA, Ward T, Ganz R. Avascular necrosis of the femoral head as a serious complication following femoral nailing in children and adolescents. Unfallchirurg. 1998;101(6):495–9.
Brav EA. Traumatic dislocation of the hip: army experience and results over a 12 year period. J Bone Joint Surg Am. 1962;44:1115–34.
Epstein HC. Posterior fracture-dislocations of the hip; long-term follow-up. J Bone Joint Surg Am. 1974;56(6):1103–27.
Hougaard K, Thomsen PB. Traumatic posterior dislocation of the hip—prognostic factors influencing the incidence of avascular necrosis of the femoral head. Arch Orthop Trauma Surg. 1986;106(1):32–5.
Delbet MP. Fractures du col de femur. Bull Mem Soc Chir. 1907;35:387–9.
Jain R, Koo M, Kreder HJ, Schemitsch EH, Davey JR, Mahomed NN. Comparison of early and delayed fixation of subcapital hip fractures in patients sixty years of age or less. J Bone Joint Surg Am. 2002;84(9):1605–12.
Pillai A, Little K, Chappell A. Osteonecrosis of the femoral head following medullary nailing of the femur in an adult. Acta orthopaedica belgica. 2007;73(2):258.
Wu C-C, Yu C-T, Hsieh C-P, Chen S-J, Chang L. Femoral head avascular necrosis after interlocking nail of a femoral shaft fracture in a male adult: a case report. Arch Orthop Trauma Surg. 2008;128(4):399–402.
Dora C, Leunig M, Beck M, Rothenfluh D, Ganz R. Entry point soft tissue damage in antegrade femoral nailing: a cadaver study. J Orthop Trauma. 2001;15(7):488–93.
Stannard JP, Harris HW, Volgas DA, Alonso JE. Functional outcome of patients with femoral head fractures associated with hip dislocations. Clin Orthop Relat Res. 2000;377:44–56.
Ganz R, Gill TJ, Gautier E, Ganz K, Krugel N, Berlemann U. Surgical dislocation of the adult hip a technique with full access to the femoral head and acetabulum without the risk of avascular necrosis. J Bone Joint Surg Br. 2001;83(8):1119–24.
Shan-hong Q. Accuracy of closed reduction for displaced subcapital femoral neck fractures assisted by C-arm X-ray machine. CRTER. 2012;16(9):1643–6.
Mohan R, Karthikeyan R, Sonanis SV. Dynamic hip screw: does side make a difference? Effects of clockwise torque on right and left DHS. Injury. 2000;31(9):697–9.
Beck M, Siebenrock KA, Affolter B, Nötzli H, Parvizi J, Ganz R. Increased intraarticular pressure reduces blood flow to the femoral head. Clin Orthop Relat Res. 2004;424:149–52.
Bonnaire F, Schaefer DJ, Kuner EH. Hemarthrosis and hip joint pressure in femoral neck fractures. Clin Orthop Relat Res. 1998;353:148–55.
Crawfurd EJ, Emery RJ, Hansell DM, Phelan M, Andrews BG. Capsular distension and intracapsular pressure in subcapital fractures of the femur. J Bone Joint Surg Br. 1988;70(2):195–8.
Woodhouse CF. Dynamic influences of vascular occlusion affecting the development of avascular necrosis of the femoral head. Clin Orthop Relat Res. 1964;32:119–29.
Shih L-Y, Chen T-H, Lo W-H. Avascular necrosis of the femoral head-an unusual complication of an intertrochanteric fracture. J Orthop Trauma. 1992;6(3):382–5.
Kaweblum M, Lehman WB, Grant AD, Strongwater A. Avascular necrosis of the femoral head as sequela of fracture of the greater trochanter: a case report and review of the literature. Clin Orthop Relat Res. 1993;294:193–5.
Linhart W, Stampfel O, Ritter G. Post-traumatic femur head necrosis following trochanter fracture. Z Orthop Ihre Grenzgeb. 1984;122(6):766.
Stougard J. Post-traumatic avascular necrosis of the femoral head in children. Report of two cases. J Bone Joint Surg Br. 1969;51(2):354–5.
Trueta J. The normal vascular anatomy of the human femoral head during growth. J Bone Joint Surg Br. 1957;39(2):358–94.
Tannast M, Pleus F, Bonel H, Galloway H, Siebenrock KA, Anderson SE. Magnetic resonance imaging in traumatic posterior hip dislocation. J Orthop Trauma. 2010;24(12):723–31.
Notzli HP, Siebenrock KA, Hempfing A, Ramseier LE, Ganz R. Perfusion of the femoral head during surgical dislocation of the hip. Monitoring by laser Doppler flowmetry. J Bone Joint Surg Br. 2002;84(2):300–4.
Tannast M, Siebenrock KA. Open therapy of femoroacetabular impingement. Oper Orthop Traumatol. 2010;22(1):3–16.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2014 Springer-Verlag Berlin Heidelberg
About this chapter
Cite this chapter
Steppacher, S.D., Haefeli, P.C., Anwander, H., Siebenrock, K.A., Tannast, M. (2014). Traumatic Avascular Necrosis of the Femoral Head. In: Koo, KH., Mont, M., Jones, L. (eds) Osteonecrosis. Springer, Berlin, Heidelberg. https://doi.org/10.1007/978-3-642-35767-1_14
Download citation
DOI: https://doi.org/10.1007/978-3-642-35767-1_14
Published:
Publisher Name: Springer, Berlin, Heidelberg
Print ISBN: 978-3-642-35766-4
Online ISBN: 978-3-642-35767-1
eBook Packages: MedicineMedicine (R0)