
Abstract
Primary thymic epithelial neoplasms represent the most common type of tumors of the anterior mediastinum. These tumors have been a source of major controversy over the years due to their difficulties for histopathologic typing and often unpredictable biologic behavior. Unlike malignant epithelial neoplasms arising at other organs, these tumors were felt for many years to be unsuitable for histologic grading. In fact, the latest WHO schema for the classification of thymic epithelial neoplasms does not mention grading for these tumors at all. More recent observations, however, have demonstrated that thymic epithelial neoplasms form part of a continuous spectrum of lesions that may closely resemble their parent organ at the one end or be very poorly differentiated at the other extreme [1]. Based on these observations, a novel conceptual approach was recently introduced for the classification of thymic epithelial neoplasms that is based on the histologic degree of differentiation of the lesions [2]. The histologic grading of these tumors is based on the premise that these lesions can range from well-differentiated to moderately differentiated to poorly differentiated neoplasms. This is supported by the observation of tumor progression in thymoma whereby recurrences show transformation of a low-grade histologic type to that of a higher-grade histology [3]. The degree of differentiation in any given tumor will depend on the presence or absence of the organotypical features of differentiation of the thymus and on the degree of cytological atypia displayed by the tumor cells (see Table 4.1).
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others



Keywords
- Adenoid Cystic Carcinoma
- Perivascular Space
- Thymic Carcinoma
- Mucoepidermoid Carcinoma
- Cytological Atypia
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
4.1 Introduction
Primary thymic epithelial neoplasms represent the most common type of tumors of the anterior mediastinum. These tumors have been a source of major controversy over the years due to their difficulties for histopathologic typing and often unpredictable biologic behavior. Unlike malignant epithelial neoplasms arising at other organs, these tumors were felt for many years to be unsuitable for histologic grading. In fact, the latest WHO schema for the classification of thymic epithelial neoplasms does not mention grading for these tumors at all. More recent observations, however, have demonstrated that thymic epithelial neoplasms form part of a continuous spectrum of lesions that may closely resemble their parent organ at the one end or be very poorly differentiated at the other extreme [1]. Based on these observations, a novel conceptual approach was recently introduced for the classification of thymic epithelial neoplasms that is based on the histologic degree of differentiation of the lesions [2]. The histologic grading of these tumors is based on the premise that these lesions can range from well-differentiated to moderately differentiated to poorly differentiated neoplasms. This is supported by the observation of tumor progression in thymoma whereby recurrences show transformation of a low-grade histologic type to that of a higher-grade histology [3]. The degree of differentiation in any given tumor will depend on the presence or absence of the organotypical features of differentiation of the thymus and on the degree of cytological atypia displayed by the tumor cells (see Table 4.1).
Tumors displaying most or all of the organotypical features of thymic differentiation and absence of cytological atypia are categorized as low-grade or well-differentiated thymic epithelial neoplasms (also designated, by convention, thymoma), tumors retaining only some of the organotypical features of the thymus but displaying mild to moderate cytologic atypia correspond to moderately differentiated thymic epithelial neoplasms (atypical thymomas), and tumors showing total loss of the organotypical features of the thymus and displaying overt cytologic evidence of malignancy correspond to high-grade or poorly differentiated thymic epithelial neoplasms (also designated, by convention, thymic carcinomas) [2, 4]. It is to be noted that the grading of these tumors is based on a combination of architectural and cytological parameters as observed on routine microscopy on hematoxylin-eosin-stained slides and does not require the use of special stains or other ancillary techniques.
4.2 Well-Differentiated Thymic Epithelial Neoplasms (Thymoma)
The diagnosis of well-differentiated thymoma is based on the identification of the organotypical features of differentiation of the thymus and the absence of significant cytological atypia in the tumor cells. The organotypical features of the thymus can vary depending on whether the tumor cells are attempting to recapitulate the normal, mature thymus of infants and adolescents or whether they resemble the normal involuted thymus of the adult (see Table 4.1). In general, the better-differentiated tumors are characterized by a thick capsule, fibrous bands with prominent lobulation, and an overwhelming population of immature T-lymphocytes admixed with the neoplastic epithelial cells, thus closely resembling the thymic cortex in children and adolescents. Dilated perivascular spaces and so-called areas of “medullary” differentiation are other frequent features seen in these lesions. The neoplastic epithelial cells are characterized by large vesicular nuclei with prominent eosinophilic nucleoli and are surrounded by an indistinct rim of abundant lightly eosinophilic or amphophilic cytoplasm (Fig. 4.1). Mitoses are not a feature of the neoplastic cells, although in some cases they may be relatively frequent in the surrounding immature T-lymphocytic population. Well-differentiated thymomas that resemble the normal involuted thymus of the adult are composed predominantly of a monotonous population of oval to spindle cells admixed with variable numbers of T-lymphocytes. The neoplastic spindle cells are characterized by bland-appearing oval nuclei with dispersed chromatin and inconspicuous nucleoli surrounded by a scant rim of lightly eosinophilic cytoplasm (Fig. 4.2). The cells are devoid of nuclear pleomorphism or mitotic activity.

Well-differentiated thymoma. This lymphocyte-predominant type contains two neoplastic epithelial cells (center) surrounded by lymphocytes. The epithelial cells are characterized by large, vesicular nuclei with prominent eosinophilic nucleoli surrounded by an indistinct rim of amphophilic cytoplasm

Well-differentiated thymoma of spindle cell type. The tumor is composed of cells with oval to spindle nuclei. The nuclei have dispersed chromatin and absent or inconspicuous nucleoli. There is no mitotic activity
4.3 Moderately Differentiated Thymic Epithelial Neoplasms (Atypical Thymoma)
These tumors are characterized by partial loss of the organotypical features of differentiation of the normal thymus, with mild to moderate increase in cytologic atypia of the neoplastic epithelial cells. Atypical thymoma may be composed of round/polygonal or oval/spindle cells. The majority of these tumors, however, are composed of large, round to polygonal epithelial cells admixed with scattered T-lymphocytes. Architecturally, the tumors may show some of the organotypical features commonly found in thymoma, such as a thick capsule, lobulation, and perivascular spaces (Fig. 4.3). The tumor cells, however, are much larger than in conventional thymomas, and the cells are characteristically surrounded by abundant eosinophilic cytoplasm showing well-defined cell borders. The nuclei are also larger than in thymomas and show an increase in chromatin deposition with often prominent eosinophilic nucleoli (Fig. 4.4). Occasional mitotic figures can be observed in the epithelial cells; mitoses may be typical or more rarely atypical but are usually not numerous (usually <2 per 10 high-power fields). A distinctive feature of these tumors is the presence of well-defined cell membranes in the epithelial tumor cells which contrasts with the indistinct cytoplasmic cell borders seen in thymoma. The polygonal shape of the cells and the sharply outlined, thick cell membranes often impart an epidermoid appearance to these tumors. In fact, microscopic foci displaying abrupt squamous differentiation are a frequent finding in these lesions. The tumors are distinguished by a highly cohesive growth pattern forming solid sheets of tumor cells, in contrast to the discohesive growth pattern of well-differentiated thymomas that are characterized by isolated tumor cells separated by abundant lymphocytes. Perivascular spaces are often numerous and show a tendency to display prominent peripheral palisading of tumor cells around the lumen of the vessels. Atypical thymomas composed of oval or spindle cells are also characterized by increase of their nuclear size, with a heavy chromatin pattern, frequent eosinophilic nucleoli, and occasional mitotic figures.

Moderately differentiated thymic epithelial neoplasm (atypical thymoma). Tumor cells form solid sheets around the dilated thin-walled blood vessels. Epithelial cells predominate, but there are also scattered lymphocytes

Moderately differentiated thymic epithelial neoplasm (atypical thymoma). Higher magnification of the tumor showing large round to polygonal cells with sharply defined cell membranes and enlarged, hyperchromatic nuclei with occasionally prominent eosinophilic nucleoli
4.4 Poorly Differentiated Thymic Epithelial Neoplasms (Thymic Carcinoma)
These tumors are defined as having lost the characteristic organotypical features of the thymus and by displaying overt cytologic evidence of malignancy. Thymic carcinomas can display a wide variety of microscopic appearances and may closely resemble carcinomas of other organs [4, 5]. As such, they represent essentially a diagnosis of exclusion requiring strict clinical and radiographic demonstration of the absence of a primary tumor elsewhere. A large number of histologic varieties of thymic carcinoma have been described. In the study by Suster and Rosai [4], the tumors could be divided based on their morphologic features into those of low-grade and high-grade histology. It remains debatable whether some of the tumors in the low-grade category may not be best reclassified as moderately differentiated thymic epithelial neoplasms (atypical thymoma), a category that was not yet acknowledged at the time of publication of that study [4]. In any event, the several categories of thymic carcinoma have been described as follows:
-
Squamous cell carcinoma. These tumors may be well differentiated or poorly differentiated and resemble squamous cell carcinoma in other sites. They, however, usually retain a lobular growth pattern typical of other thymomas.
-
Mucoepidermoid carcinoma (Fig. 4.5). These tumors resemble the homonymous tumors of the salivary glands and may present likewise as either well-differentiated, moderately differentiated, or poorly differentiated carcinomas.
Fig. 4.5 
Poorly differentiated thymic epithelial neoplasm. This tumor has the microscopic features of a mucoepidermoid carcinoma. It is composed of islands of polygonal, epidermoid tumor cells containing cystic luminal spaces filled with mucin. There is no resemblance to the normal thymus
-
Lymphoepithelioma-like carcinoma (Fig. 4.6). These tumors resemble the homonymous tumors of the nasopharynx.
-
Clear cell carcinoma (Fig. 4.7). These tumors are composed of clear cells containing abundant glycogen in their clear cytoplasm.
Fig. 4.7 
Clear cell carcinoma of the thymus. The tumor is composed of clear cells but also shows keratinization. The tumor did not display any of the organotypical features of differentiation of the normal thymus
-
Basaloid carcinoma. These tumors resemble basal cell carcinomas of the skin and are composed of uniform round to oval cells with hyperchromatic nuclei and prominent peripheral palisading.
Fig. 4.6 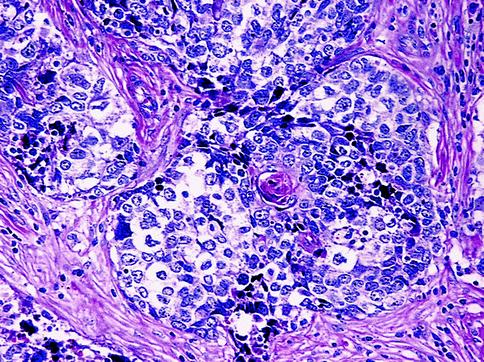
Lymphoepithelioma-like carcinoma. The tumor shows islands of primitive-appearing cells with central comedo-like areas of necrosis
-
Mucinous adenocarcinoma. These tumors resemble mucin-secreting tumors in other parts of the body [6].
-
Adenoid cystic carcinoma. These tumors resemble homonymous tumors of salivary glands [7].
-
Small cell neuroendocrine carcinoma. These tumors are indistinguishable from homonymous pulmonary carcinomas.
-
Sarcomatoid carcinoma. This tumor type, is composed predominantly of spindle cells, suggesting the diagnosis of a mesenchymal malignancy. Foci of epithelial differentiation may be scant but are useful for the final diagnosis.
-
Anaplastic carcinoma. This tumor type, is usually composed of pleomorphic cells, showing almost no signs of differentiation.



The cytologic and architectural features of these tumors are essentially similar to those of their counterparts in other organs [5]. In general, thymic carcinoma is characterized by marked cytologic atypia, increased mitotic activity, and frequent areas of necrosis and vascular invasion.
4.4.1 Comments
-
1.
Great controversy has existed in the literature regarding the best approach to the classification of thymic epithelial neoplasms. The controversy has centered in recent years mainly on the issue of whether morphology alone is sufficient to predict the clinical behavior of these tumors. The consensus of opinion seems to be that morphology alone, particularly for the better-differentiated (low-grade) variants of thymic epithelial neoplasms, is an unreliable predictor of clinical behavior and that staging (i.e., the status of capsular integrity) is the most important parameter for the prediction of biologic behavior in these tumors.
-
2.
The identification of moderately differentiated tumors (atypical thymoma) may be of significance due to their higher incidence of capsular invasion, tendency for earlier recurrence, and potential for transformation into a higher-grade malignancy [1, 4].
-
3.
Several series of thymomas showing uncommon microscopic features have been published during the last few years. For example, there are papers describing thymomas with prominent papillary and pseudopapillary features and so-called adenomatoid spindle cell thymomas, just to mention a few [8, 9]. It is important to recognize these variants and not to confuse them with thymic carcinomas. Also it is worth remembering, as pointed out in the study of invasive spindle cell thymomas (WHO type A), “that histologic features do not correlate with invasion or encapsulation because all thymomas, regardless of their histologic type are capable of invasion” [10].
Books and Monographs
Rosai J (1999) Histological typing of tumors of the thymus. World Health Organization international histological classification of tumours, 2nd edn. Springer, Berlin
Weidner N, Cote RJ, Suster S, Weiss LM (eds) (2009) Modern surgical pathology, 2nd edn. Saunders Elsevier, Philadelphia
Articles
Suster S, Moran CA (1996) Primary thymic epithelial neoplasms with combined features of thymoma and thymic carcinoma. A clinicopathologic study of 22 cases. Am J Surg Pathol 20:1469–1480
Suster S, Moran CA (1999) Thymoma, atypical thymoma and thymic carcinoma. A novel conceptual approach to the classification of neoplasms of thymic epithelium. Am J Clin Pathol 111:826–833
Suster S, Moran CA (1999) Primary thymic epithelial neoplasms. Spectrum of differentiation and histologic features. Semin Diagn Pathol 16:2–17
Suster S, Rosai J (1991) Thymic carcinoma. A clinicopathologic study of 60 cases. Cancer 67:1025–1032
Suster S, Moran CA (1998) Thymic carcinoma: spectrum of differentiation and histologic types. Pathology 30:111–122
Ra SH, Fishbei MC, Baruch-Oren T et al (2007) Mucinous adenocarcinomas of the thymus: report of 2 cases and review of the literature. Am J Surg Pathol 31:1330–1338
Di Tommaso L, Kuhn E, Kurrer M et al (2007) Thymic tumor with adenoid cystic carcinomalike features: a clinicopathologic study of 4 cases. Am J Surg Pathol 31:1161–1167
Kalhor N, Suster S, Moran CA (2011) Spindle cell thymomas (WHO type A) with prominent papillary and pseudopapillary features: a clinicopathologic and immunohistochemical study of 10 cases. Am J Surg Pathol 35:372–377
Weissferdt A, Kalhor N, Suster S, Moran CA (2010) Adenomatoid spindle cell thymomas: a clinicopathological and immunohistochemical study of 20 cases. Am J Surg Pathol 34:1544–1549
Moran CA, Kalhor N, Suster S (2010) Invasive spindle cell thymomas (WHO type A): a clinicopathologic correlation of 41 cases. Am J Clin Pathol 134:793–798
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2013 Springer-Verlag Berlin Heidelberg
About this chapter
Cite this chapter
Suster, S., Moran, C. (2013). Tumors of the Thymus. In: Damjanov, I., Fan, F. (eds) Cancer Grading Manual. Springer, Berlin, Heidelberg. https://doi.org/10.1007/978-3-642-34516-6_4
Download citation
DOI: https://doi.org/10.1007/978-3-642-34516-6_4
Published:
Publisher Name: Springer, Berlin, Heidelberg
Print ISBN: 978-3-642-34515-9
Online ISBN: 978-3-642-34516-6
eBook Packages: MedicineMedicine (R0)