
Abstract
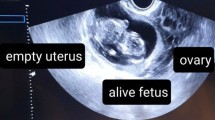
Often findings of antenatal ultrasound or neonatal examinations done as part of an evaluation of congenital anomalies necessitate surgery.
-
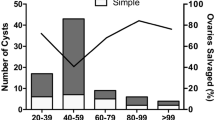
The majority of findings are simple follicular cysts associated with high maternal steroid production.
-
When reasonably small (<7 cm) torsion is unlikely, regression occurs rapidly, serial ultrasound examination to monitor disappearance is sufficient.
-
Intrauterine fetal cyst aspiration has been tried and yielded good results.
-
If larger than 5 cm, the cyst should be removed to relieve pressure and its consequent pain, to prevent torsion and to rule out large cystic teratoma.
-
An attempt should be made to preserve normal and functioning ovarian tissue, even if necrotic.
-
A laparoscopic approach is the ideal approach for diagnosis and treatment.
-
Percutaneous aspiration should not be tried.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others

Keywords
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
Often findings of antenatal ultrasound or neonatal examinations done as part of an evaluation of congenital anomalies necessitate surgery.
-
The majority of findings are simple follicular cysts associated with high maternal steroid production.
-
When reasonably small (<7 cm) torsion is unlikely, regression occurs rapidly, serial ultrasound examination to monitor disappearance is sufficient.
-
Intrauterine fetal cyst aspiration has been tried and yielded good results.
-
If larger than 5 cm, the cyst should be removed to relieve pressure and its consequent pain, to prevent torsion and to rule out large cystic teratoma.
-
An attempt should be made to preserve normal and functioning ovarian tissue, even if necrotic.
-
A laparoscopic approach is the ideal approach for diagnosis and treatment.
-
Percutaneous aspiration should not be tried.
Resection of Benign Cyst
Surgery through Pfannenstiel incision:
-
A thin-walled ovarian cyst is shown in Fig. 1.


Fig. 1
-
Careful assessment is necessary before the initial incision is made. The incision in the ovarian cortex facilitates symmetric reconstruction. An elliptical incision is made through the thin cortex of the benign cyst (Fig. 2).


Fig. 2
-
A plane is developed by the use of blunt dissection. The end of the knife is then inserted and a plane developed over the cyst wall. Fine-needle electrocautery or microsurgical can be used to separate the cyst wall from the ovarian cortex (Fig. 3).


Fig. 3
-
The inner ovarian stroma may be approximated with a purse-string suture of 5/0 non-reactive material. Closure of the ovary is done with a baseball or simple stitch. NB: The redundent cortex can be removed and the dead space obliterated with an internal closure, with care taken that suture material does not penetrate the ovarian cortex (Fig. 4).


Fig. 4
Tips
-
Low-power magnification (surgical loupes) often assists the surgeon in identifying the correct plane in the cyst wall and ovarian parenchyma.
-
If the cortex is quite friable, it is necessary to place interrupted 6/0–7/0 non-reactive sutures to achieve adequate approximation.
Common Pitfalls
-
Rupture of fragile cyst wall and spillage of the pelvic cavity
-
Excessive redundant thin cortex: can present a special problem in ovarian reconstruction
-
Rough manipulation of the Fallopian tubes
Ovarian Transposition Before Radiotherapy
Surgery through the Pfannenstiel incision:
-
This procedure is done, e.g. when there is ovarian transposition in a patient being treated for malignancy before receiving radiotherapy.
-
The ovaries are suspended out of the field of radiation.
-
Bisharah and Tulandi have recommended transection of the ovarian ligament and transposition of the ovaries without affecting the Fallopian tubes.
-
This is associated with positioning of the ovaries laterally and anteriorly at the level of the anterosuperior iliac spines (Fig. 5).


Fig. 5
Tips
-
Gonads are sensitive to radiation. It is estimated that the sensitivity of the oocytes to radiation is the lethal dose required to eliminate 50 % of the oocytes (LD50) of 2 Gy
Common Pitfalls
-
The consequences of not transecting the ovarian ligament will affect the Fallopian tubes.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2013 Springer-Verlag Berlin Heidelberg
About this chapter
Cite this chapter
Said, H., Carachi, R. (2013). F11 Ovarian Surgery. In: Carachi, R., Agarwala, S., Bradnock, T.J., Lim Tan, H., Cascio, S. (eds) Basic Techniques in Pediatric Surgery. Springer, Berlin, Heidelberg. https://doi.org/10.1007/978-3-642-20641-2_124
Download citation
DOI: https://doi.org/10.1007/978-3-642-20641-2_124
Publisher Name: Springer, Berlin, Heidelberg
Print ISBN: 978-3-642-20640-5
Online ISBN: 978-3-642-20641-2
eBook Packages: MedicineMedicine (R0)