
Abstract
This chapter focuses on techniques used in studying the upper gastrointestinal tract, including a double contrast upper gastrointestinal series, a single contrast gastrointestinal series, and various postoperative studies. The radiologist does not follow a rigid sequence in performing a study. The technique and contrast agents are tailored to the clinical and surgical history and the specific clinical questions to be answered. In performance of the study, the radiologist alters techniques and patient position based on the fluoroscopic findings and the patient’s ability to perform the examination. If the radiologist understands the elements of image interpretation and the radiographic findings of various diseases, he or she will understand what images are necessary to obtain while performing a study.
Access provided by Autonomous University of Puebla. Download reference work entry PDF
Similar content being viewed by others


Keywords
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
Introduction
This chapter focuses on techniques used in studying the upper gastrointestinal tract, including a double contrast upper gastrointestinal series, a single contrast gastrointestinal series, and various postoperative studies. The radiologist does not follow a rigid sequence in performing a study. The technique and contrast agents are tailored to the clinical and surgical history and the specific clinical questions to be answered. In performance of the study, the radiologist alters techniques and patient position based on the fluoroscopic findings and the patient’s ability to perform the examination. If the radiologist understands the elements of image interpretation and the radiographic findings of various diseases, he or she will understand what images are necessary to obtain while performing a study.
In single contrast, the radiologist fills the gastrointestinal lumen with barium or water-soluble contrast, creating a “cast” of the lumen (Fig. 15.1). The edge of the lumen is seen in profile, as a continuous column of barium (Rubesin 1995).The gastric and small intestinal folds are seen as tubular or sinuous radiolucencies if the contrast column is not too dense. The en face structural detail is obscured if the contrast is too dense. Visualization of intestinal folds is achieved by using a contrast material of the correct density or by compressing the abdomen to flatten the organ (Fig. 15.2), making the anteroposterior thickness of the barium column less, and effectively decreasing its radiographic density. The folds of the stomach and duodenum are also seen if the lumen is nearly collapsed, termed mucosal relief. The intestinal folds are composed of mucosa and submucosa, and therefore interpretation of disease arising in the mucosa or submucosa is made by evaluating fold size, contour, shape, and surface texture. In some instances, barium fills the grooves between tufts of gastric or duodenal mucosa, enabling true en face visualization of the mucosal surface.


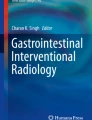
The single contrast image. The value of distension. In single contrast, the radiologist evaluates the luminal contour and the mucosal/submucosal folds seen as tubular radiolucencies in the barium column. (a) Spot radiograph from single contrast upper gastrointestinal series shows incomplete distension of the duodenum. Focally thickened folds (arrows) are possibly seen on the lateral wall of the second part of the duodenum. (b) The second part of the duodenum is now fully distended by the barium column; a focally lobulated 1.5 cm polypoid mass (arrows) is seen on the lateral wall. This proved to be a villous adenoma


The single contrast image. The value of compression. Spot radiograph obtained during compression demonstrates the folds of the gastric antrum as thin, sinuous radiolucent filling defects (arrows). The folds of the proximal duodenal bulb are demonstrated (arrowheads)
In double contrast (also termed air contrast), the radiologist coats the mucous layer of the viscus with sticky high density barium, enabling true visualization of the mucosa (Fig. 15.3). The radiologist also can evaluate the luminal contour and the fold pattern similar to a single contrast study (Fig. 15.4). In some studies, a shallow barium pool can demonstrate a depression or elevated lesion (Fig. 15.5). In many places, however, the high density barium, however, gives an extremely dense barium pool that the radiologist cannot see through (Fig. 15.6). Therefore, the mucosa is only seen in air contrast or at the edge of the barium pool.


The double contrast image: en face mucosal detail. In air contrast, high density barium enters the interstices between elevations, revealing the mucosal pattern. Spot radiograph from double contrast upper gastrointestinal series shows disruption of the normal areae gastricae pattern by numerous 1–2 mm round uniformly sized nodules. This was marked lymphoid hyperplasia due to H pylori gastritis


The double contrast image: the luminal contour versus detail demonstrated in air contrast by barium coating. Spot radiographs of the upper gastric body and the gastric fundus obtained with the patient in (a) an erect frontal view and (b) a right side down view (“right lateral”). The contour of the fundus is slightly lobulated (arrowheads). Large, smooth sinuous folds are manifested en face a smooth, lobulated lines coated by barium (arrows). This patient had portal hypertension and gastric varices


The double contrast image: the shallow barium pool. Spot radiograph obtained with patient in right side down position demonstrates a 3 cm ovoid, smooth-edged mass (arrowheads) just posterior to the gastric cardia (thin arrow). The areae gastricae are preserved and have not yet been stretched by this submucosal mass. This proved to be a gastrointestinal stromal tumor


The double contrast image: the dense barium pool partly obscures mucosal detail. (a) Spot radiograph of the distal esophagus obtained during rapid drinking of barium with the patient in an upright LPO position demonstrates an irregular, ulcerated contour (arrowheads) in the gastric cardia and a questionably thick fold in the distal esophagus (thin arrows). (b) Spot radiograph obtained seconds later demonstrates a 1.5 cm ovoid polypoid filling defect (arrowhead) in the contrast column in the distal esophagus. (c) Spot radiograph obtained with the patient in a right side down position while refluxing barium into the distal esophagus demonstrates a 4 cm lobulated mass (arrowheads) obliterating the normal landmarks of the gastric cardia. A barium filled ulcer (U) is seen centrally. Nodular mucosa (long arrow) is seen superior to the ulcer. A polypoid mass (short arrow) extends into the distal esophagus. This was an adenocarcinoma of the gastric cardia extending into the distal esophagus. The nodular mucosa is shown only in the shallow barium pool. The nodular surface of the ulcer is shown in the barium pool
In sum, in single contrast, the radiologist evaluates the luminal contour for abnormalities that protrude into or out of the lumen, the size of the viscus, the mucosal/submucosal folds, and the motility of the organ (Levine et al. 1988). In double contrast, the radiologist evaluates the luminal contour, the en face mucosal detail, and the shallow portions of the barium pool (Rubesin et al. 2008).
Patient Preparation
The presence of fluid or undigested food in the stomach or duodenum compromises the properties of the contrast agents and makes interpretation of obstruction or motor disorder difficult. Therefore, the patient is instructed not to eat or drink after midnight, the day before the examination. In reality, a patient with normal motility will empty liquid from the stomach rapidly, so we allow all patients to take their morning medications with a small enough amount of water to safely ingest pills. If the esophagus is the only organ in question, the patient can probably drink a fluid that does not coat the mucosa (water, solution with sugar only) the morning of the examination. Insulin dependent diabetics should not take insulin the day of the examination. Any activity that stimulates salivary secretion (smoking, gum chewing, and throat lozenges) should be avoided. Medications that coat the mucosa (antacids, etc) should not be taken.
Contrast Agents
High density barium is a 250% w/v barium. In general, it contains two groups of particle sizes, a larger particle that adheres to the mucus, enabling visualization of the surface, and a smaller particle. The barium particles are not in solution, but float in a water suspension. To achieve the appropriate barium viscosity, there is a narrow range of water that can be added to dry barium (Rubesin and Herlinger 1986). As water is added to the dry barium, the water adheres to the barium particles forming a thick, paste, like substance. Once all the water binding sites are filled, a small amount of additional water rapidly transforms the mixture into a flowing suspension. Too much added water will alter the coating properties of the suspension (Cumberland 1977). The barium mixture must sit for at least 5 min to allow proper hydration of the barium particles. The mixture is then aggressively shaken and stirred again. Minor adjustments of the amount of water added according to the manufacturer’s recommendation may be necessary if the pH or mineral content of the radiologist’s water are unusual.
Low density barium should be about 40–50% w/v for the upper gastrointestinal tract (Gelfand 1978). This type of barium does not coat the mucosa well, but is thinner and easier to drink than high density barium.
Water-soluble contrast agents are variably hyperosmolar; Gastrografin is about 6–8 times normal osmolality, oral omnipaque about two times hyperosmolality. The iodine in these agents has a horrific taste, therefore strong flavoring agents must be used to mask the flavor of the iodine. Water-soluble contrast agents are vastly inferior to barium in the demonstration of anatomy. However, if a perforation is present, these agents are resorbed from the mediastinum or peritoneum. In contrast, barium in the mediastinum or peritoneum incites a granulomatous reaction. With an upper gastrointestinal tract leak, this granulomatous reaction has little clinical consequences. However, with a colonic leak, barium mixed with feces in the peritoneal space can incite a potentially fatal peritonitis.
There is a controversial risk of pulmonary edema if water-soluble agents enter the lungs. This radiologist does not believe that the small amount of aspirated water-soluble contrast agent can incite pulmonary edema on an osmolar basis. If a pulmonary edema occurs, it is either a chemical or allergic reaction to material in the water-soluble contrast agent or a reaction to aspiration of oral contents. Barium in the lungs may not be as innocuous as thought. Large barium particles that clump in alveoli may block alveoli, resulting in atelectasis or possible superinfection.
Given the true lack of science concerning contrast agents in the lungs or entering the peritoneal space from an upper gastrointestinal leak and the relative ineffectiveness of water-soluble contrast agents in imaging the upper gastrointestinal tract, we use the following guidelines. If there is a strong suspicion for aspiration or tracheoesophageal fistula, barium is used. If there is a strong suspicion of a leak, water-soluble contrast is used. If no leak is demonstrated, we usually repeat the images with high density barium.
The Digital Fluoroscope
We use a standard digital fluoroscope. Standing at the patient’s side enables direct communication with the patient, exact positioning of the patient, and direct palpation of the abdomen. The radiologist uses the “last image hold” feature to briefly analyze the radiographic findings while the radiation beam is off. When the radiographic image is satisfactory, a spot radiograph is obtained.
We constantly change the magnification setting from lower to higher magnification and back. Low magnification gives the “big picture.” Low magnification is of lower radiation dose, is satisfactory to evaluate esophageal motility and is able to demonstrate the overall location and configuration of a viscus or the location of a large tumor. Higher magnification has a greater radiation dose, but has the greater resolution needed to analyze anatomic details. The mucosal details or staple lines seen at higher resolution are frequently not visible on lower magnification radiographs.
The advantages of a remote control fluoroscope are a larger tube to image capture device distance and the ability to angle the tube. A patient in a wheelchair can be “rolled” into the remote control fluoroscope without placing him or her in a “swallowing chair.” The disadvantages of the remote control fluoroscope are the lack of direct contact with the patient, resulting in inferior patient position and inferior palpation, and the lack of an option for decubitus images. We have long discarded our remote control unit and replaced it with a standard fluoroscope.
Double Contrast Upper Gastrointestinal Series
A double contrast upper gastrointestinal series is the standard examination of the esophagus, stomach, and duodenum (Laufer 1975; Shirakabe et al. 1982; Levine et al. 1988; Rubesin 2008). This study is used to assess for inflammatory or neoplastic disease of the upper gastrointestinal tract. It requires that the patient can communicate with the radiologist, follow instructions, and turn on the fluoroscopic tabletop. A single contrast upper gastrointestinal series is performed when the patient cannot follow commands or turn on the fluoroscopic tabletop. A single contrast study is also used when there is only interest in demonstration of large findings such as perforation, obstruction, herniation, volvulus, or postoperative anatomy.
The order of spot radiographs is not as important as the presence of mucosal coating. If the mucosa is not coated by high density barium, little or no information is available. Therefore, the radiologist washes the mucosa with high density barium, lets the barium clear by gravity, either in the erect position, or by turning the patient, then takes a radiograph when there is either no barium pool or an extremely shallow barium pool on the dependent surface.
Glucagon is given routinely at the beginning of the study (Miller et al. 1974; Maglinte et al. 1982). Glucagon causes gastric and duodenal hypotonia, resulting in better distension of the stomach and duodenum. Glucagon does not alter esophageal peristalsis, but does diminish lower esophageal sphincter pressure. The only contraindication for the use of intravenous glucagon is a history of insulinoma or pheochromocytoma. We do not give glucagon to insulin dependent diabetics, because it is important to evaluate gastric peristalsis and gastric emptying in patients with diabetes. Routinely, 0.1 mg glucagon is injected intravenously immediately prior to the study. 1 mg glucagon is given intravenously if there is strong suspicion of a gastric carcinoma, if the study is being performed for follow-up of a gastric ulcer, or if the patient has a remote history of a Billroth I or Billroth II procedure.
Buscopan is not available in the United States. Even if it was, we often do not know our patient’s ophthalmologic, cardiac, or prostate histories well enough to safely administer Buscopan. Buscopan abolishes esophageal peristalsis and we prefer to evaluate this on every study. Buscopan probably enables better distension of the esophagus, antrum, and duodenum, however, in comparison to glucagon.
Images in Air Contrast
Effervescent is administered after the glucagon is injected. If there is a clinical history suggesting gastric or esophageal obstruction or severe esophagitis, effervescent agent is not initially given. Once no florid esophagitis or obstruction is demonstrated, then it is safe and comfortable for the patient to swallow effervescent agent.
The patient then rapidly drinks barium, gulping air, and regurgitating air from the stomach to distend the esophagus. The esophagus is studied with the patient in an erect left posterior oblique position (Fig. 15.7), as the esophagus has an ovoid shape, and this is the position that demonstrates the most esophageal surface en face (Fig. 15.8). If there is a history of solid food dysphagia, the barium cup is split, enabling the esophagus to be imaged in both left and right posterior obliquities (Fig. 15.9). Images of the cervical esophagus are obtained often without much air contrast. In some patients, a barium column remains in the distal esophagus. The radiologist must wait for the barium column to empty into the stomach and to obtain images just as the barium clears the distal esophagus but the air remains. In some patients only collapsed, mucosal relief views of the distal esophageal folds are possible.


Normal esophagus in air contrast. Spot radiographs of the (a) mid and (b) distal esophagus obtained while the patient rapidly drinks high density barium. The esophageal contour and esophageal folds shown in the shallow barium coating are smooth. The esophageal mucosa seen en face is smooth


Five millimeter squamous papilloma of mid esophagus demonstrated in air contrast. (a) Spot radiograph obtained with the patient in the left posterior oblique position. Barium coats the edge and interstices of a 5 mm finely lobulated polyp (arrow). (b) Spot radiograph obtained with the patient in a right posterior oblique position demonstrates the polyp as a barium coated elevation (arrow)


The value of imaging the esophagus in left and right obliquity in patients with solid food dysphagia. (a) Spot radiograph obtained with the patient in the erect, left posterior oblique position demonstrates a curvilinear barium coated line (arrow) and a vague ovoid area of increased density superior to the line. (b) Spot radiograph obtained with the patient in an erect, right posterior oblique position demonstrates a hemispheric- shaped barium coated line (arrows) surrounded a smooth hemisphere of increased density. The submucosal mass, questionable in a. is definitely seen in b. At surgery, an esophageal duplication cyst was removed
After esophageal images are obtained, the radiologist lets the barium bolus completely clear the esophagus if the clinical question is gastroesophageal reflux. The table is lowered. The patient is then rolled 360° to the right. Gastric coating is adequate if a dense, uniform line along the lesser curvature is seen or if the areae gastricae are demonstrated (Rubesin and Herlinger 1986). If not, the patient is rolled 1–2 more times.
The order of filming is not as important as the assessment that the coating is adequate. The radiographic positions are listed in Table 15.1 and are demonstrated in Figs. 15.10–15.18. The radiologist coats the surface to be imaged, by turning the patient, flowing the barium pool across the surface, then turning the patient again to spill the barium pool from the surface (Kikuchi et al. 1986). The last image hold function of the fluoroscope is used to assess coating and proper projection. If these factors are good, a spot radiograph is obtained. The radiologist turns the patient from side to side to coat the mucosa then obtain images. In general, turning the patient toward to left coats the greater curvature and turning the patient to the right coats the lesser curvature (Shirakabe et al. 1982). The mid anterior wall of the stomach is not coated unless the patient is turned into a prone position.


Air contrast view of stomach with patient in supine position. The “supine view” demonstrates the mucosa of the distal gastric body and proximal gastric antrum en face. The luminal contour is seen as a continuous white line


Air contrast view of stomach with patient in right side down position. The “right lateral view” demonstrates the gastric cardia, fundus and retrogastric region. Smooth folds radiate to the closed gastric cardia (arrow). The folds of the upper lesser curvature (arrowhead) are seen in the shallow barium pool


Air contrast view of stomach with patient in left posterior oblique position. The “LPO view” shows the en face mucosal detail of the distal gastric antrum


Air contrast view of stomach with patient in right posterior oblique position. The “RPO view” (also known as a Schatzki view) demonstrates the lesser curvature en face. This view may be taken with the patient in a recumbent, semi-erect, or erect patient position. In this patient, there are huge, lobulated folds on the lesser curvature due the multiple myeloma infiltrating the stomach. (Compare these folds with the normal sized lesser curvature folds in Fig. 15.11)


Air contrast view of stomach with patient in erect, frontal position. The “erect, frontal view” demonstrates the gastric fundus and upper gastric body mucosa en face


Air contrast view of stomach with patient in erect, left posterior oblique position. The “erect, steep LPO view” demonstrates the mucosal surface of the greater curvature en face


Air contrast view of stomach with patient in left side down (left lateral) position. The left lateral view demonstrates the anterior wall of the gastric antrum (arrow)


Air contrast view of duodenum with patient in left posterior oblique position. The “LPO view” often best demonstrates the en face surface of the posterior wall of the duodenal bulb and second portion of the duodenum in air contrast


View of distal duodenum with patient in supine position. An upper GI series evaluates the entire duodenum to the duodenal jejunal junction (long arrow). The third (arrowhead) and fourth (short arrow) portions of the duodenum are shown en face with the patient in a supine or prone position
Images of the gastric antrum should be obtained early in the examination, before much barium has spilled into the duodenum. If barium does spill into the duodenum, images of the distal gastric body and antrum may be “pieced together” by carefully positioning the patient. Erect images are of value for the gastric fundus, cardia, and high lesser curvature (Fig. 15.19). Erect views are also of value for the duodenal bulb, as the weight of the barium in the gastric antrum pulls the duodenum into a shallow obliquity and displays the bulb without overlap from the gastric antrum. An abnormality may be seen in one projection but not seen in another (Fig. 15.20). An abnormality may sometimes be seen better in air contrast or sometimes better in the barium pool (Fig. 15.21).


Comparison of the left and near right lateral views of the stomach in air contrast. (a) Spot radiograph of stomach obtained with patient in right side down view (a “right lateral”). Two questionable 3 mm polyps are seen (short arrow). (b) Spot radiograph obtained with the patient in a near-erect and near left lateral position (an “erect steep LPO”) demonstrates at least 6 small polyps, some manifested as ring shadows coated in barium (long arrow) and others manifested as ovoid, finely lobulated radiolucencies in the barium pool (short arrows). These were hyperplastic polyps. These images demonstrate how the right lateral view coats the lesser curvature in the barium pool and the near left lateral position coats the greater curvature. The two lateral views are not the same image


The value of different projections. (a) Coned-down view from spot radiograph of the lesser curvature with the patient in the supine position. There is a subtle barium collection (arrow) seen only in retrospect. (b) Spot radiograph obtained with the patient in a left posterior oblique position. A near rectangular shaped, smooth, barium coated line (arrow) protrudes outward from the incisura angularis. (c) Spot radiograph obtained during compression during the single contrast phase of the examination with the patient in a left posterior oblique position. A smooth-edged rectangular barium collection (long arrow) protrudes at the incisura angularis. A smooth, thin curved radiolucent collar of tissue (short arrows) is seen in the barium column. These findings demonstrate a benign gastric ulcer: the niche protrudes from the luminal contour. There is no associated gastric mass. There is a Hampton’s line (short arrows in c) representing a rim of mucosa at the ulcer’s edge slightly undermined by the ulcer extending laterally into the lamina propria and submucosal fat


The barium pool. (a) Spot radiograph of gastric antrum obtained with the patient in a left posterior oblique position. There is a 3 cm ovoid filling defect in the shallow barium pool (arrowhead). Its superior margin is slightly lobulated. Centrally an irregular V-shaped ulcer is filled with barium (arrow). (b) Spot radiograph obtained with the patient in a prone position shows thick lobulated folds along the distal lesser curvature. The mass is seen as a subtle filling defect (arrowhead), not seen as well as in a. These images demonstrate how a posterior wall mass is better seen in the shallow barium pool in the supine position in comparison to the prone position. Note that the compression balloon in b. was not centered over the lesion and that the barium pool was too dense
Images in Single Contrast
Once the air contrast portion of the examination is obtained, a limited single contrast examination is performed using thin barium. The single contrast portion of the examination focuses on esophageal motility, gross esophageal pathology, the anterior wall of the distal gastric body, antrum and duodenal bulb, and the duodenal sweep.
Esophageal motility is evaluated with the patient in a prone, right anterior oblique position to negate the effect of gravity (Ott et al. 1989). The refractory period for esophageal peristalsis is 20 s, so the patient must wait 20 s between single swallows. If there are no symptoms referable to the esophagus, two swallows suffice for the evaluation of motility. If the patient complains of dysphagia or chest pain or there is a clinical question of abnormal esophageal motility, five swallows are obtained. The patient swallows once, then opens their mouth to prevent double swallowing that may interrupt the peristaltic wave. Under low magnification (Fig. 15.22), the top of the fluoroscope is kept at the pharyngoesophageal segment for as long as possible to exclude double swallowing. Once the peristaltic wave is near the bottom of the image, the fluoroscope is moved to include the gastric cardia (Fig. 15.23).


Low magnification fluoroscopy of esophageal motility. Spot radiograph demonstrating the initial position for fluoroscopy of esophageal motility. The patient is in a right anterior oblique position. The fluoroscope is centered so the pharyngoesophageal segment (arrow) is seen near the upper portion of the image. In this short patient, the entire esophagus is visible. It is not known if evaluating motility without the effect of gravity, as in this position, or with single swallows in the upright position is the proper approach


Low magnification fluoroscopy of esophageal motility. The radiologist holds the fluoroscope in its original position until the peristaltic wave approaches the carina. This enables the radiologist to see if the patient is double swallowing, possibly disrupting the primary peristaltic wave. Once the peristaltic wave is near the carina, the fluoroscope is rapidly moved so the inferior portion of the image is at the gastric cardia. In this patient, no peristalsis was seen. The esophagus is dilated. The lower esophageal sphincter did not open at an appropriate time and had a “beak-like appearance” (arrow). This patient had two “negative” endoscopies. The upper GI series was the first study to make a diagnosis of achalasia
Esophageal morphology is evaluated as the patient rapidly drinks thin barium. Higher magnification images are obtained of the cervical (Fig. 15.24), mid and distal esophagus (Fig. 15.25) for webs, rings, and strictures (Chen et al. 1985). The radiologist identifies the level of the diaphragm by asking the patient to inhale and exhale, watching the extrinsic impression of the diaphragm on the distal esophagus or herniated stomach. A hiatal hernia or Schatzki ring may be “brought out” by increasing abdominal pressure with breathing or bearing down techniques. Alternatively, abdominal pressure may be elevated by placing the patient on a bolster or compression paddle.


Single contrast evaluation of cervical esophageal morphology. Spot radiograph obtained while the patient rapidly drinks thin barium in the right anterior oblique position. There is moderate incomplete opening of the cricopharyngeus (arrow), occluding about 70% of the AP luminal diameter. A spurt of barium (arrowhead) goes through the narrowed pharyngoesophageal segment


Single contrast evaluation of distal esophageal morphology. Spot radiograph obtained while patient rapidly drinks thin barium in the right anterior oblique position. A broad-based 2 cm ovoid ulcer (arrowhead) is seen in the distal esophagus. A track of barium (arrows) extends into the mediastinum. This patient had Crohn’s distal of the distal esophagus with a fissure into the mediastinum
The gastric and duodenal images obtained with the combination of thick and thin barium are inferior to single contrast images obtained only with thin barium during a single contrast upper gastrointestinal series. It is often difficult to “see through” the combination of thick and thin barium (Fig. 15.26). The radiologist relies on compression performed with the patient in a prone (Fig. 15.27) or upright position. The radiologist focuses on the portions of stomach below the rib cage and the duodenum, as these are the areas that are compressible. The posterior wall of the duodenal bulb is often best seen en face with the patient in the left posterior oblique position (Fig. 15.28). The anterior wall of the duodenal bulb is best visualized, in general, with the patient in the right anterior oblique or erect right posterior oblique position (Fig. 15.29). As one-half of duodenal ulcers are on the anterior wall of the bulb, the right anterior oblique position is important for the demonstration of an anterior wall ulcer as a focal barium collection.


The combination of high density and thin barium may obscure en face mucosal detail. Spot radiograph obtained with the patient in a right anterior oblique position. The contour of the distal gastric antrum, pylorus (arrow), and duodenal bulb are demonstrated, but the dense barium obscures the en face detail


Compression image for the anterior wall of the duodenal bulb. Spot radiograph obtained with the patient in a right anterior oblique position. Although the duodenal bulb is filled with barium, the folds of the pylorus and lateral portion of the bulb (arrow) are visible


Compression image for the posterior wall of the duodenal bulb. Spot radiograph with the patient in a left posterior oblique position demonstrates a 7 mm round barium collection (arrow) on the posterior wall of the duodenal bulb. The upper bulb contour is deformed. The mucosa of the duodenal bulb is nodular. This patient with metastatic breast cancer was on chemotherapy and had nausea. The upper GI demonstrated an unsuspected benign ulcer on the posterior wall of the duodenal bulb


Compression images for demonstration of the anterior wall of the duodenal bulb. (a) Spot radiograph of the stomach in the supine position shows lack of filling of the duodenal bulb. (b) Spot radiograph of the duodenal bulb in the right anterior oblique position shows a 7 mm round contrast collection (arrow), seen as a “double density” in the duodenal bulb. (c) Spot radiograph of the stomach and duodenal bulb in the right posterior oblique position shows the anterior wall of the duodenal bulb in profile. A 7 mm benign ulcer (arrow) is seen on the anterior wall. (Note that images a–c are from a study using water-soluble contrast)
Testing for Gastroesophageal Reflux
Any barium residue in the esophagus is cleared from the esophagus by having the patient drink water. The radiologist rolls the patient from side to side, bathing the gastric cardia in a large pool of barium. In general, gastroesophageal reflux is most frequently seen when the patient turns from a supine to slight right anterior oblique position. A water siphon test can be performed, by having the patient drink water while the gastric cardia is bathed in barium. This mimics the one-half of episodes of gastroesophageal reflux that related to lowering of lower esophageal sphincter pressure during swallowing.
Single Contrast Upper Gastrointestinal Series
A single contrast examination is performed on patients who are unable to undergo a double contrast study or when a limited examination will provide sufficient information for patient care. Barium is used when the clinical question is obstruction or anatomy. Water-soluble contrast agents are used when a perforation is suspected (see Fig. 15.29).
Esophageal peristalsis is studied as described above, using low magnification to study single swallows of thin barium. Thin barium is then rapidly ingested to fully distend the esophagus. Esophageal fold thickness may be evaluated with collapsed mucosal relief images.
Before the stomach is filled with a large volume of contrast, compression views of the anterior wall of gastric antrum and duodenal bulb may be obtained in the prone and right anterior oblique positions, respectively (see Fig. 15.29). These early images usually show the folds of the antrum, pylorus and duodenal bulb better than when the stomach is overfilled with barium.
Further filling of barium is used to assess the overall contour of the stomach (Fig. 15.30) in the positions listed in Table 15.2. The radiologist can only safely compress portions of the stomach below the rib cage. Therefore, the upper gastric body and gastric fundus are often flooded with barium.


The single contrast image. Spot radiograph from single contrast upper GI series with the patient in a right posterior oblique position. When the viscus is filled with a large volume of barium, the contour is well demonstrated, but folds may be obscured. For example, the contour of the distal lesser curvature is well shown (arrowhead), but the antral folds are not demonstrated. When the viscus is incompletely filled with contrast, the folds of the posterior wall are shown, but the contour is poor visualized. For example, the folds of the posterior wall of the mid and distal gastric body are demonstrated (short arrows), but the contour of the distal gastric body is poorly seen (long arrow)
If the patient can stand, upright compression views in positions similar to a double contrast UGI are performed.
If there is question of thickened gastric folds or gastric narrowing, effervescent agent can be given to distend the stomach. The radiologist should not believe that these are true air contrast images, as no mucosal coating is present.
Suspected Esophageal or Gastric Outlet Obstruction
Neither glucagon nor effervescent agent should be used when the clinical history suggests obstruction (vomiting, severe abdominal pain, plain radiograph, scout image or CT demonstrating a dilated esophagus, or stomach with debris or air-fluid levels). Instead, about one fourth of a cup of high density barium is ingested. Views of the esophagus are obtained in the upright LPO position. If no esophageal obstruction is seen, the patient remains upright, watching the barium flow through the fluid/debris filled stomach. The patient is then lowered in a right lateral position, keeping barium in the distal gastric antrum, limiting barium mixing with the debris filled lumen. Images of the obstructing tumor, ulcer, or scarring are obtained. If barium passes easily into the duodenum and there is no obstruction, either a double contrast or single contrast upper gastrointestinal series may be performed, given the questions to be answered and the patient’s condition.
The Postoperative Stomach
The Immediate Postoperative Stomach
In the immediate postoperative period, a contrast study is performed to exclude a complication such as a leak or abnormal emptying due to obstruction or severe adynamic ileus.
Low magnification scout images of the “big picture” are obtained in supine and as erect-as-possible positions. Higher magnification images are necessary to demonstrate staple lines. Oblique scout images are obtained in the position that a leak may be best demonstrated.
The patient swallows one swallow of water-soluble contrast, in an erect position as possible. The radiologist checks for laryngeal penetration. If the patient aspirates contrast into the trachea, the radiologist should consider giving high density barium or passing a nasogastric tube into the distal esophagus/stomach superior to a staple line to allow injection of water-soluble contrast. Once the patient is shown to be swallow-safe, three or four swallows of water-soluble contrast are swallowed. Radiographs of the site of expected perforation are obtained early, before the area is flooded with contrast (Fig. 15.31). After these early images, the patient ingests more water-soluble contrast to fill the stomach and duodenum, if no leak is seen.


Leak after gastric bypass. (a) Spot radiograph of the esophagogastric junction after the patient swallows one swallow of water-soluble contrast. The patient had fever and mild abdominal pain 1 day after gastric bypass. Contrast barely fills the gastric pouch. A spurt of contrast (arrow) is seen going through a 4 mm hole in the left lateral wall of the gastric pouch. (b) Spot radiograph obtained 5 s after a. The gastric pouch (arrowhead) is partially filled with contrast. Contrast enters a collection lateral to the pouch and enters two of three Jackson-Pratt drainage tubes (long arrows for the lateral tube, short arrows for the more superior tube)
The patient positions where leaks are typically demonstrated are the following:
-
Frontal views or RPO views of the distal esophagus, esophagogastric junction, and gastric cardia
-
Frontal and LPO views of the esophagojejunal anastomosis after total gastrectomy
-
Left or right lateral views of an antecolic gastrojejunostomy for obstruction
-
LPO or RAO, if possible, views of a pyloroplasty
-
Upright or prone views, if possible, of a gastrojejunostomy after Billroth II procedure
The Remote Postoperative Stomach
The most common complication in the remote postoperative period is abnormal viscus emptying due to gastric atony or anastomotic obstruction related to ulcer or stricture formation. Bleeding may result from bile reflux gastritis, recurrent H. pylori gastritis, or recurrence of carcinoma or lymphoma. If the stomach was operated upon more than a decade before, a carcinoma may have developed.
The radiologist should have been alerted to the type of surgery previously performed. Some forms of gastric surgery (e.g., vagotomy and pyloroplasty, esophagogastrectomy) incorporate a pyloroplasty or pyloromyotomy to improve gastric emptying. In other patients, an anastomosis replaces the pylorus. In patients with a gastroduodenostomy (Billroth I), gastrojejunostomy (Billroth II), or pyloroplasty/myotomy, 1 mg glucagon is administered to prevent rapid gastric emptying of barium unless the clinical history suggests obstruction.
The majority of postoperative stomachs are behind the left rib cage and are inaccessible to palpation. Therefore, effervescent agent and double contrast technique are used in the remote postoperative period in patients with a Billroth I or Billroth II procedure (Fig. 15.32). No effervescent agent is administered, however, to any patient with an absent or restricted stomach. Therefore, no effervescent agent is given to patients who have had a fundoplication, gastric bypass, lap band, gastric sleeve, vertical band gastroplasty, or esophagojejunostomy.


Gastrojejunal anastomosis after Billroth II procedure. Spot radiograph from double contrast upper GI series demonstrates an end to side anastomosis between the gastric body (B) and the jejunum (J) manifested as a thick radiolucent bar (arrows)
For a Billroth I or II, one-half cup of barium is administered after the effervescent agent. If the barium runs immediately into the small intestine, another ½ cup is given with the patient in a supine position. The patient is turned to coat the stomach and images are obtained in all obliquities (Fig. 15.33). The gastrojejunal anastomosis is often best visualized in a slight RPO or lateral view. Once air contrast images are obtained, a limited single contrast study using thin barium is used to evaluate the esophagus, gastric emptying, and the duodenum or jejunum. Erect compression of the gastrojejunal anastomosis may be achieved if the stomach falls below the rib cage.


Adenocarcinoma of stomach 25-years after Billroth I procedure. Spot radiograph of stomach from double contrast upper gastrointestinal series demonstrates a 5 cm area of thick, lobulated folds (arrowheads) with a nodular surface (short arrows) in the distal gastric body. The contour of the lesser curvature is abnormal (long arrows) indicating the infiltrative nature of the tumor
In patients with gastric restriction (fundoplication, operations for morbid obesity), only one or two swallows of high density barium are initially ingested, checking for obstruction at the appropriate site. If no obstruction is seen, further amounts of high density barium are given, appropriate for the expected size of the stomach. Areas of expected luminal narrowing (fundoplication, gastroenteric anastomoses) can be indirectly measured by taking a radio-opaque object of known size (e.g., a barium tablet) and taking a radiograph of this object at the same height from the tabletop as the area of luminal narrowing. Once obstruction is excluded, the small intestine distal to the stomach is evaluated with thin barium.
Operations for Morbid Obesity
This chapter does not go into detail concerning the postoperative stomach and operations for morbid obesity. The following are guides imaging techniques in the immediate postoperative period.
In the immediate postoperative period, studies may be performed to show the anatomy that was created, to check for viscus emptying and to exclude a leak. Check for leaks at these sites
-
1.
Gastric bypass: distal esophagus, gastric pouch along staple lines, gastrojejunal anastomosis, jejunal stump, and jejunojejunostomy. Also check for obstruction at the gastrojejunostomy or ischemia or obstruction of the alimentary limb due to herniation through a retrocolic gastrojejunostomy.
-
2.
Laparoscopic band: distal esophagus, gastric fundus
-
3.
Vertical banded gastroplasty: distal esophagus, gastric pouch along staple line, excluded portion of fundus along staple line, gastric pouch outlet
-
4.
Gastric sleeve: gastric staple line/outlet
Obstruction due to postoperative edema, inflammation, or ischemia may occur at the gastric pouch outlet (VBG or sleeve). Obstruction at the lap band in the immediate postoperative period may be due to edema, too small a band or bunching of the stomach at the band. Obstruction at the lap band in the remote postoperative period may be due to too tight a band, slip of stomach through the band, or ingestion of too large a bolus to pass through the band (Fig. 15.34).


Meat impaction above laparoscopic band. The patient complained of 4 days of dysphagia. A spot radiograph was obtained in the right anterior oblique position in an attempt to eliminate the small amount of barium administered that obscured the esophagus in the upright position. The laparoscopic band (short arrowheads) and the esophagogastric junction (short arrow) are identified. A 5 × 1.5 cm radiolucent filling defect (long arrows) with a nodular surface is seen in the distal esophagus. A second 2.5 cm filling defect (long arrowhead) is seen spanning the esophagogastric junction. Large pieces of pork were removed at endoscopy
Although images of the distal esophagus are usually sufficient with the patient in the erect position, the patient should be placed in a recumbent position to fill the upper portion of a gastric pouch. The lateral view is often helpful to image a gastrojejunostomy. A steep RPO view is helpful to demonstrate a staple line along the high lesser curvature. If no leak or obstruction is seen with water-soluble contrast, we usually give a small amount of high density barium and repeat the study. In patients with gastric bypass, thin barium is then given to image the jejunojejunostomy.
Tube Studies
The radiologist can evaluate the stomach and duodenum through an indwelling nasogastric or feeding tube. In a relatively immobile patient, a single contrast examination is performed. If the clinical questions is a gastric or duodenal leak, water-soluble contrast is injected. Otherwise, single contrast barium is injected into the tube slowly in an attempt to avoid gastroesophageal reflux.
The entire stomach should be bathed in contrast; therefore, at least 100 or more ml of contrast are utilized. The patient is turned into a right lateral position to examine the anterior wall of the gastric antrum and to empty contrast into the duodenum. The anterior wall of the high greater curvature is bathed in contrast in the left lateral position. An immobile patient may have to be physically turned by the examiners to achieve the lateral position.
If there is question of gastrostomy tube placement, water-soluble contrast is injected through the gastrostomy tube. If any resistance is encountered during injection the radiologist stops and turns the patient into a lateral position to check for a kink or suture blocking the tube or for malposition of the tube outside of the gastric lumen (Fig. 15.35). If the tube is placed in the distal stomach, a right lateral view best visualizes the relationship of tube to the anterior gastric wall. If the tube is placed in the upper gastric body, a left lateral view is important.


The value of the lateral view during a “tube check.” A patient with a gastrostomy tube complains of upper abdominal pain during tube feeds. (a) Spot radiograph obtained after a small amount of contrast is injected through the gastrostomy tube. (b) If no resistance to the flow of contrast is felt during tube injection, more contrast can be injected. Although no leak is seen, not enough contrast bathes the mid greater curvature. (c) The patient is turned into a right side down position. The tip of the gastrostomy tube (arrow) is outside the greater curvature of the stomach. Contrast fills an irregular track (arrowhead) that enters the anterior wall of the stomach. No free leak into the peritoneal cavity is seen
If there is no clinical concern about tube position, and if the patient is mobile and there is a question of subtle gastric disease, a double contrast examination of the stomach and duodenum can be achieved by injecting high density barium and then room air through the tube (Fig. 15.36).


Double contrast examination of stomach through a gastrostomy tube. Spot radiograph centered on the high lesser curvature demonstrates the balloon of a gastrostomy tube (arrow). A benign gastric ulcer is manifested as a 1 cm barium collection (arrowhead) on the posterior wall just opposite the gastrostomy tube
References
Chen YM, Ott DJ, Gelfand DW, et al. Multiphasic examination of the esophagogastric region for strictures, rings, and hiatal hernia: evaluation of the individual techniques. Gastrointest Radiol. 1985;10:311–6.
Cumberland DC. Optimum viscosity of barium suspension for use in the double contrast barium meal. Gastrointest Radiol. 1977;2:169–74.
Gelfand DW. High density, low viscosity barium for fine mucosal detail on double-contrast upper gastrointestinal examinations. Am J Roentgenol. 1978;130:831–3.
Kikuchi Y, Levine MS, Laufer I, et al. Value of flow technique for double-contrast examination of the stomach. Am J Roentgenol. 1986;147:1183–4.
Kressel HY, Laufer I. Principles of double contrast diagnosis. In: Laufer I, editor. Double contrast gastrointestinal radiology with endoscopic correlation. Philadelphia: WB Saunders; 1979. p. 19–58.
Laufer I. A simple method for routine double contrast study of the upper gastrointestinal tract. Radiology. 1975;117:513–8.
Laufer I, Kressel HY. Principles of double contrast diagnosis. In: Levine MS, Rubesin SE, Laufer I, editors. Double contrast gastrointestinal radiology. Thirdth ed. Philadelphia: WB Saunders; 2000. p. 8–46.
Levine MS, Rubesin SE, Herlinger H, et al. Double-contrast upper gastrointestinal examination: technique and interpretation. Radiology. 1988;165:593–602.
Maglinte DDT, Caudill LD, Krol KL, et al. The minimum effective dose of glucagon in upper gastrointestinal radiography. Gastrointest Radiol. 1982;7:119–22.
Miller RE, Chernish SM, Skukas J, et al. Hypotonic roentgenography with glucagon. Am J Roentgenol. 1974;121:264–74.
Ott DJ, Chen YM, Hewson EG, et al. Esophageal motility: assessment with synchronous videotape fluoroscopy and manometry. Radiology. 1989;173:419–22.
Rubesin SE. Gallery of double-contrast terminology. Gastroenterol Clin North Am. 1995;24:259–88.
Rubesin SE, Herlinger H. The effect of barium suspension viscosity on the delineation of areae gastricae. Am J Roentgenol. 1986;146:35–8.
Rubesin SE, Levine MS, Laufer I. Review for residents – double-contrast upper gastrointestinal radiography: a pattern approach for diseases of the stomach. Radiology. 2008;246:33–48.
Shirakabe H, Kobayashi S, Maruyama M. Principles and application of double contrast radiography. In: Shirakabe H, Nishizawa M, Maruyama M, Kobayashi S, editors. Atlas of x-ray diagnosis of early gastric cancer. 2nd ed. Tokyo: Igaku-Shoin; 1982. p. 19–43.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2013 Springer-Verlag Berlin Heidelberg
About this entry
Cite this entry
Rubesin, S.E., Levine, M.S. (2013). Upper Gastrointestinal Tract: Imaging Techniques. In: Hamm, B., Ros, P.R. (eds) Abdominal Imaging. Springer, Berlin, Heidelberg. https://doi.org/10.1007/978-3-642-13327-5_13
Download citation
DOI: https://doi.org/10.1007/978-3-642-13327-5_13
Publisher Name: Springer, Berlin, Heidelberg
Print ISBN: 978-3-642-13326-8
Online ISBN: 978-3-642-13327-5
eBook Packages: MedicineReference Module Medicine