
Abstract
Peripheral blood mononuclear cells were obtained from healthy Japanese individuals ranging in age from 20 to 90 years old and analyzed by using three color flow cytometer with regards to the number and percentage of various lymphocytes. In addition, we assessed the proliferative capacity of T cells in the presence of an anti-CD3 monoclonal antibody and the amount of cytokines produced in the supernatant.
The results showed that an age-related decline was observed in the numbers of CD3+ T cells, CD8+ T cells, naive T cells, CD8+CD28+ T cells, and B cells and in the proliferative capacity of T cells. The rate of decline in these immunological parameters except for the number of CD8+ T cells was steeper in males than in females (p <0.05). An age-related increase was observed in the number of CD4+ T cells, memory T cells, and NK cells and in the CD4/CD8 ratio. The rate of increase of these immunological parameters was steeper in females than in males (p <0.05). The T cell proliferation index (TCPI), which was calculated based on T cell proliferative activity and the number of T cells, showed an age-related decline. The rate of decline in the TCPI was again steeper in males than in females (p <0.05). The score of immunological vigor calculated using 5 T cells parameters also declined with age, and the rate of decline was steeper in males than in females (p <0.05). The present study has confirmed the age-related changes in immunological parameters reported in literature. In addition, we found that a statistically significant gender difference was observed between males and females in some immunological parameters such as the number of T cells and TCPI. The slower rate of decline in the immunological parameters studied in females than in males may be consistent with the fact that women survive for longer period of time than men.
Access provided by Autonomous University of Puebla. Download reference work entry PDF
Similar content being viewed by others


Keywords
- Age-related change
- Peripheral blood lymphocytes
- T cell proliferation index
- CD8+CD28+ T cells
- Scoring of immunological vigor
Introduction
Immunological functions are known to decline with age in many animal models and humans (Linton and Dorshkind 2004; Utsuyama et al. 1992; Hirokawa et al. 2006). Understanding the level of immunological functions at an individual level is clinically important, since the immunological decline is accompanied by various diseases such as infections, cancer, and vascular diseases.
Accumulating evidences mainly obtained from animal models have shown that age-related immunological decline mainly occurs in T cell-dependent immune functions and is mainly caused by thymic involution that begins in the early phase of life (Hirokawa et al. 2006).
In humans, data regarding immunological functions are mainly obtained from blood serum and blood cells. Serum contains immunoglobulins, complements, and cytokines. The levels of IgG and IgA in serum show a trend of increase with age (Suzuki et al. 1984). The level of complements does not change remarkably with age. The level of cytokines in healthy people is generally low. In contrast, the level of white blood cells (WBC) changes remarkably during disease and also with aging. WBC comprises granulocytes, lymphocytes, and monocytes. There are various subpopulations of lymphocytes with different functions. Data regarding the age-related changes in lymphocytes and their functions are not sufficiently available as yet.
The purpose of this study is to provide immunological data on peripheral blood lymphocytes obtained from 162 male and 194 female healthy volunteers, ranging in age from 20 to 90 years. Our study discusses the age-related changes in subpopulations of peripheral blood lymphocytes from both immunological and gerontological viewpoints.
Number of Whole WBCs, Red Blood Cells, Neutrophils, and Lymphocytes in the Blood
The number of red blood cells (RBC) showed a significant age-related decrease (p <0.001) in males but no significant change in females (p = 0.9535) (Fig. 1a, b) (Table 1). The difference between males and females with regard to the age-related decline in the number of RBC was statistically significant (p <0.001). Although an age-related decline was observed in males, but not in females, the absolute level of RBC was higher in males than in females regardless of age.

Age-related changes in the number of red blood cells (RBC) in males (a) and females (b), white blood cells (WBCs) in males (c) and females (d), neutrophils in males (e) and females (f), and lymphocytes in males (g) and females (h). Scale of abscissas is age of subjects, years
The number of WBCs including granulocytes, lymphocytes, and monocytes showed a declining trend with age in both males (p = 0.0824) and females (p = 0.2588); no statistically significant difference was observed between males and females in this regard (Fig. 1c, d) (Table 1).
The number of neutrophils showed a decreasing trend with age in both males (p = 0.2178) and females (p = 0.1063); no significant difference was observed between males and females (Fig. 1e, f) (Table 3).
The number of lymphocytes showed a decreasing trend with age in males (p = 0.0593) and an increasing trend with age in females (p = 0.1249); statistically significant difference was observed in the age-related change between males and females (p = 0.015) (Fig. 1g, h) (Table 1).
Flow Cytometric Analysis
In 1992, we reported age-related change in subpopulations of lymphocytes in healthy subjects ranging in age from 6 to 102 years (Utsuyama et al. 1992). Recent studies confirmed most of the results presented in our previous report; i.e., an age-related decrease in CD3+ T cells, more pronounced decrease in CD8+ T cells than in CD4+ T cells, an age-related increase in CD4/CD8 ratio, a decrease in the number of naïve T cells with a concomitant increase in memory T cells, a decrease in B cells, and an increase in NK cells.
CD3+ T Cells
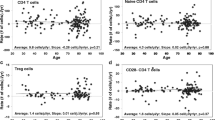
The number of CD3+ T cells showed a statistically significant decrease with age in males (p = 0.0176) and a decreasing trend with age in females (p = 0.1249). The difference in the age-related change in the number of CD3+ T cells between males and females was statistically significant (p = 0.049) (Fig. 2a, b) (Table 1).

Age-related changes in the number of T cells in males (a) and females (b), CD4+ T cells in males (c) and females (d), CD8+ T cells in males (e) and females (f), and the CD4/CD8 ratio in males (g) and females (h). Scale of abscissas is age of subjects, years
CD4+ T Cells
The number of CD4+ T cells showed an increasing trend with age in females (p = 0.1075) but no change in males (p = 0.9897). This difference between males and female was statistically significant (p = 0.005) (Fig. 2c, d) (Table 1).
CD8+ T Cells
The number of CD8+ T cells showed an age-related decrease in both males (p <0.0002) and females (p <0.0001), but no difference was observed between males and females with regard to this decrease (Fig. 2e, f) (Table 1).
The Ratio of CD4+ T Cells to CD8+ T Cells (CD4/CD8 Ratio)
The CD4/CD8 ratio increased with age in both males (p <0.0001) and females (p <0.0001), and this increase was significantly greater in females than in males (p <0.003) (Fig. 2g, h) (Table 1).
Olsson et al. (2000) reported that a decrease in the CD4/CD8 ratio was an important indicator of the immune risk phenotype (IRP). In the present survey, a contrasting feature was observed between CD4+ T cells and CD8+ T cells. The number of CD4+ T cells was in relatively steady level or showed an increasing trend with age, while the number of CD8+ T cells significantly decreased with age; therefore, the CD4/CD8 ratio showed a distinct age-related increase. Higher percentage and number of CD8+ T cells and a decreased CD4/CD8 ratio was observed in the Saudi male population compared with Caucasian controls (Shahabuddin 1995). Hence, racial difference should be considered in this case.
CD8+CD28+ T Cells
The number of CD8+CD28+ T cells showed an age-related decrease in both males (p <0.0001) and females (p <0.0001) (Fig. 3a, b), and the rate of this decline was more pronounced in males (−6.089) than in females (−4.136) (p = 0.038) (Table 1).

Age-related changes in the number of CD8+CD28+ T cells in males (a) and females (b), naive T cells in males (c) and females (d), memory T cells in males (e) and females (f), and native to memory T cells (N/M) ratio in males (g) and females (h). Scale of abscissas is age of subjects, years
A low number of CD8+CD28− T cells and high CD4/CD8 ratio are associated with populations that survive until the age of 100 years (Strindhall et al. 2007). Susceptibility to influenza infection in older adults is associated with an increased population of CD8+CD28− T cells (Xie and McElhaney 2007). In this respect, we confirmed that the number of CD8+CD28+ T cells decreased with age, and this decrease was associated with a decrease in the T cell proliferative activity, i.e., the rate of decline was significantly slower in female than in males, as mentioned later.
Using negative correlation between the number of CD8+CD28+ T cells and age, it is possible to assess the age by plugging the number of CD8+CD28+ T cells into the equation. We named the obtained value “T-lymphocyte age.” This is described in detail in the other chapter in this book, Hirokawa et al., “Assessment of age-related decline of immunological function and possible methods for immunological restoration in the elderly.”
CD4+CD45RA+ Naïve T Cells
The number of CD4+CD45RA+ naïve T cells showed a decreasing trend with age in both males (p = 0.2615) and females (p = 0.4470) (Fig. 3c, d) (Table 1). This decreasing trend was greater in males than in females, and the difference between males and females was statistically significant (p = 0.004).
CD4+CD45RO+ Memory T Cells
The number of CD4+CD45RO+ memory T cells showed an increasing trend with age in males (p = 0.1531) and an age-related increase in females (p = 0.0001) (p <0.0001) (Fig. 3e, f). In this case, there is no significant gender difference (Table 1).
Ratio of Naïve to Memory T Cells
The naïve to memory T cells (N/M) ratio showed an age-related decrease in both males (p <0.0001) and females (p = 0.0003), and this decrease was statistically significant (Fig. 3g, h). However, no significant gender difference was observed (Table 1).
CD4+CD25+ T Cells
It is still not clear whether the age-related increase in the prevalence of CD4+CD25(high) regulatory T cells (TREGs) is responsible for immune dysfunction in the elderly (Dejaco et al. 2006). In this respect, we found that the number of TREGs showed an increasing trend with age.
This subpopulation of T cells is well known to include regulatory T cells. The number of CD4+CD25+ T cells showed an increasing trend with age in both males (p = 0.7502) and females (p = 0.1818) (Fig. 4a, b), but this increase was statistically not significant. Further, no gender difference was observed (Table 1).

Age-related changes in the number of CD4+CD25+ T cells in males (a) and females (b), B cells (WBC) in males (c) and females (d), NK cells in males (e) and females (f). Scale of abscissas (a–f) is age of subjects, years. The correlation between the number of CD8+CD28+ T cells and the T cell proliferative activity in males (g) and females (h)
CD20+ B Cells
The absolute number of total B-lymphocytes increases about threefold from the base line in the first year of life and progressively decreases until adult age (Veneri et al. 2007). We further confirmed that the number of CD20+ B cells showed a decrease with age in males (p <0.05) and showed a decreasing trend with age in females (p = 0.15) (Fig. 4c, d); decline was significantly steeper in males than in females (p <0.001) (Table 1).
CD56+CD16+ NK Cells
The number of CD56+CD16+ NK cells showed an age-related increase in females (p = 0.0002) and an increasing trend with age in males (p = 0.19) (Fig. 4e, f). This increasing trend was greater in females than in male and the gender difference was statistically significant (p <0.001) (Table 1). Lee et al. (1996) reported higher percentage of NK cells in the Asian population than in Caucasian subjects.
T Cell Proliferative Activity
Proliferative Response of T Cells by Anti-CD3 Monoclonal Antibody
The proliferative response of T cells was measured by MTS method, and the value obtained was used for the expression of T cell proliferative activity. It showed an age-related decrease in both males (p <0.0001) and females (p <0.002) (Fig. 5a, b) (Table 1), but no gender difference was observed.

Age-related change in the T cells proliferative activity in males (a) and females (b), T cell proliferation index (TCPI) in males (c) and females (d), score of immunological vigor (SIV)-7 in males (e) and females (f), and SIV-5 (T cell immune score) in males (g) and females (h)
T Cell Proliferation Index (TCPI)
We developed a new parameter, T cell proliferation index (TCPI), which is calculated by using the proliferative activity and the number of T cells. Calculation of TCPI was shown in Materials and Methods in the last section. The TCPI showed an age-related decrease in both males (p <0.0002) and females (p <0.008) (Fig. 5c, d). The decrease was more pronounced in males than in females (p = 0.01) (Table 1).
Correlation Between CD8+CD28+ T Cells and T Cell Proliferative Activity
Both the number of CD8+CD28+ T cells and T cell proliferative activity showed an age-related decrease in both males and females, showing positive correlation between the number of CD8+CD28+ T cells and T cell proliferative activity (Fig. 4g, h). This correlation between them was statistically significant (p <0.01).
Scoring of Immunological Vigor (SIV)
SIV-7
Calculation of SIV was shown in Materials and Methods in the last section.
SIV-7 was calculated based on seven parameters: T cells number, TCPI, CD4/CD8 ratio, naïve T cell number, naive/memory T cells ratio, B cell number, and NK cell number. SIV-7 showed an age-related decrease in both males (p = 0.0005) and females (p <=0.0002) (Fig. 5e, f). No gender difference was observed (Table 1).
SIV-5
SIV-5 was calculated by using five parameters: T cells number, TCPI, CD4/CD8 ratio, naïve T cell number, and naive/memory T cells ratio; SIV-5 is sometimes termed as T cell immune score.
The T cell immune score showed an age-related decrease in both males (p = 0.0008) and females (p <0.0001) (Fig. 5g, h). No gender difference was observed (Table 1).
Cytokine Production
In the present study, lymphocytes were cultured in vitro in the presence of immobilized anti-CD3 mAb and the cytokines produced in the supernatant were assessed as described previously. The subjects for cytokine production comprised 64 males and 49 females; this sample size was not adequate for statistical analysis. This preliminary examination has revealed that an age-related decrease in the levels of IFNγ, IL-1β, IL-2, IL-4, IL-6, IL-10, TNFα, and TNFβ in both male and female subjects. In contrast, an age-related increase was observed in IL-5 and IL-8 (Table 2). Gender difference was observed in IL-6, IL-10, and TNFβ, showing more decreasing trend in males than in females.
Anti-CD3 stimulation of T-lymphocytes significantly increased IL-8 production, and this increase was more evident in the nonagenarian subjects (Mariani et al. 2001). Centenarians showed high level of IL-8, indicating that an increased level of IL-8 is related to longevity (Wieczorowska-Tobis et al. 2006). These reports were consistent with the result of the present study indicating an age-related increase in IL-8.
Individuals who are genetically predisposed to produce high level of IL-6 have a reduced capacity to reach the extreme limits of the human lifespan. On the other hand, a high IL-10 producing genotype is observed among centenarians (Caruso et al. 2004). These results were partly consistent with those of the present study, which showed that both IL-6 and IL-10 decreased with age. In future studies, an adequate sample size should be selected for analysis of cytokine production.
Difference in Gender
It is interesting to note that the rate of decline in the studied parameters differed with gender (Hirokawa et al. 2013). Table 1 lists the regression curves calculated for the data described above, and the significance of gender difference was examined by standardized major axis test (SMA) analysis.
The rate of decrease in the number of T cells, naïve T cells, and CD8+CD28+ cells, T cell proliferation index (TCPI), and SIV-5 parameters was slower in females than in males. Further, this difference was statistically significant (p <0.05–0.003). In more detail, the rate of decline in the number of T cells calculated by the regression curve was −6.150 in males and −2.390 in females. The rate of decline in TCPI was −0.016 in males and −0.008 in females. This gender difference in the T cells and TCPI vales was statistically significant (Table 1). The rate of increase in the number of CD4+ T cells was greater in females than in males and a statistically significant difference was observed between them (p <0.005). In other words, females showed slower rate of decline or greater rate of increase in these parameters, indicating that the immunological functions are relatively well preserved in elderly females than in elderly males. In other words, this finding may be consistent with the fact that women survive for longer periods than men (Hirokawa et al. 2013). Table 3 shows the values of these immunological parameters in elderly males and females over 60 years of age. All parameters show higher values in elderly females than in males; however, the difference is statistically not significant because of the small sample size.
Conclusions and Future Directions
The present study has confirmed the age-related changes in immunological parameters reported in literature. Above all, we introduced two new immunological parameters. One is T cell proliferation index (TCPI) using T cell proliferative activity and T cell number. The other is scoring of immunological vigor (SIV) using 5 or 7 immune parameters. These are useful to see the immune status of people at whole body level. In addition, we found that a statistically significant difference was observed between males and females in the rate of age-related decline of some immunological parameters such as the number of T cells and TCPI. The slower rate of decline in the immunological parameters studied in females than in males may be consistent with the fact that women survive for longer period of time than men. Studies in future are analyses of various immunological parameters in elderly patients suffering from various diseases such as infections, cancers, and vascular diseases.
Materials and Methods
Blood specimens: 2 ml of blood was taken in a tube containing ethylenediaminetetraacetic acid (EDTA-2 K) for hematological analysis performed using a PENTRA80 analyzer (Horiba, Kyoto, Japan); 8 ml of blood was taken in a cell preparation tube (vacutainer, 362,761, Becton Dickinson (BD), NJ) for collecting mononuclear cells and was used for immunological analyses.
Subjects: Healthy volunteers were selected based on clinical records and laboratory examinations. None of the blood donors were suffering from neoplastic or autoimmune disease; further, none were receiving any medications that could influence immune functions. Routine laboratory examinations of the serum were performed to examine the liver and kidney functions. A total of 162 males and 194 females were examined in the present study. Table 4 shows the number of male and female subjects and their ages.
Flow cytometry: Mononuclear cells that were obtained from the peripheral blood, as described above, were stained with a combination of 2 or 3 monoclonal antibodies (mAbs) conjugated with 2 or 3 chromophores. A fluorescence-activated cell sorting flow cytometer (FACScan BD) was employed in the present study.
Monoclonal antibodies: The antibodies used were fluorescein isothiocyanate (FITC) conjugated anti-CD4, FITC-conjugated anti-CD20, and FITC-conjugated anti-CD16; phycoerythrin (RD1)-conjugated anti-CD3, RD1-conjugated anti-CD8, and RD1-conjugated anti-CD25; phycoerythrin-Texas Red (ECD) conjugated anti-CD45RA and ECD-conjugated anti-CD3; and phycoerythrin-cyanin 5.1 (PC5) conjugated anti-CD28: phycoerythrin (PE)-conjugated anti-CD56. Those mAbs were purchased from Beckman Coulter. The following combinations of mAbs were used: CD3-RD1/CD20-FITC, CD4-FITC/CD8-RD1/CD45RA-ECD, CD4-FITC/CD8- RD1/CD28-PC5, CD56-PE/CD16-FITC, and CD3-ECD/CD4-FITC/CD25-RD1.
T cell proliferative activity: The proliferative response of T cells to anti-CD3 mAb (ORTHOCLONE OKT3, ORTHO BIOTEC, NJ) was assessed according to MTS method (Cell Titer 96 Aqueous One Solution Cell Proliferation Assay (Promega Co., WI)). Assays were performed in microplates (3860-096, Asahi Glass Co. Japan). The cells (1 × 105) in 0.2 ml of RPMI 1640 medium supplemented with 5% fetal bovine serum (FBS) were stimulated with immobilized anti-CD3 mAb (Orthoclone OKT3 Ortho. Biotec, NJ).
The plates were then placed in a 5% CO2 incubator for 72 h. After incubation for 68 h, 40 μl of MTS solution (Cell Titer 96 Aqueous One Solution Cell Proliferation Assay (Promega Co., WI)) was added into each well and absorbance at 490 nm was recorded with a spectrophotometric plate reader; this value was used for determining the relative magnitude of T cell proliferation (T cell proliferative activity).
T cells proliferation index (TCPI) and immunological age (IA): TCPI was calculated by the following equation.
In this equation, T cell proliferative activity was obtained as optical density (OD-480) ranging between 0.95 and 2.0 by the above-mentioned MTS method. The TCPI and age showed a statistically significant correlation: TCPI = −0.0174 × (Age) + 2.5348 (Fig. 5c, d). Using this equation, it is possible to calculate age by assigning a value to TCPI. The age calculated by this equation was referred to as immunological age (IA).
Scoring and grading of immunological functions: The values of immune parameters were standardized by assigning scores of 3 (high level), 2 (moderate level) and 1 (low level) according to the data base obtained from 300 healthy people. After standardization, the scores of different types of immune parameters were summed, and the numerical value obtained for each individual was termed the score of immunological vigor (SIV). These scores were then classified into 5 grades, as shown in Table 5.
SIV-7 comprises seven parameters that are number of T cells, TCPI, CD4/CD8 ratio, number of naïve T cells, naïve/memory ratio, number of B cells, and number of NK cells. SIV-5 comprise five T cell-related parameters that are number of T cells, TCPI, CD4/CD8 ratio, number of naïve T cells, and naïve/memory T cells ratio.
Assessment of cytokine production: Assays were performed in microplates (3860-024, Asahi Glass Co. Japan). Cells (1 × 106) in 1.5 ml of RPMI 1640 supplemented with 10% FBS were stimulated with immobilized anti-CD3 mAb (Orthoclone OKT3, Ortho Biotec, NJ). Culture supernatant was collected at 48 h and stored at −80 °C until use. A flow cytomix kit (BMS810FF, Bender MedSystems, Austria) was employed for the evaluation of cytokines (Interleukin (IL)-1β, IL2, IL-4, IL5, IL-6, IL-8, IL-10, IL-12/p70, interferon (IFN) γ, tumor necrosis factor (TNF) α, and TNFβ, and the assessment was performed using a FACScan analyzer.
Statistical Analysis: All statistical analyses were performed using StatView software. Statistical significance was defined as p <0.05. Gender difference was examined by SMA analysis.
References
Caruso C, Lio D, Cavallone L, Franceschi C (2004) Aging, longevity, inflammation and cancer. Ann N Y Acad Sci 1028:1–13
Dejaco C, Duftner C, Schirmer M (2006) Are regulatory T cells linked with aging? Exp Gerontol 41:339–345
Hirokawa K, Utsuyama M, Makinodan T (2006) Immunity and ageing. In: Pathy MSJ, Sinclair AJ, Morley JE (eds) Principles and practice of geriatric medicine, 4th edn. Wiley, Hoboken, pp 19–36
Hirokawa K, Utsuyama M, Hayashi Y, Kitagawa M, Makinodan T, Fulop T (2013) Slower immune system aging in women versus men in the Japanese population. Immun Aging 10:19–28
Lee B, Yap HK, Chew FT et al (1996) Age- and sex-related changes in lymphocyte subpopulations of healthy Asian subjects: from birth to adulthood. Cytometry 26:8–15
Linton PJ, Dorshkind K (2004) Age-related changes in lymphocytes development and function. Nat Immunol 5:133–139
Mariani E et al (2001) Different IL-8 production by T and NK lymphocytes in elderly subjects. Mech Ageing Dev 122:1383–1395
Olsson J et al (2000) Age-related change in peripheral blood T-lymphocyte subpopulations and cytomegalovirus infection in the very old: the Swedish longitudinal OCTO immune study. Mech Ageing Dev 121:187–201
Shahabuddin S (1995) Quantitative differences in CD8+ lymphocytes, CD4/CD8 ratio, NK cells, and HLA-DR(+)-activated T cells of racially different male populations. Clin Immunol Immunopathol 75:168–170
Strindhall J et al (2007) No immune risk profiles among individuals who reach 100 years of age: findings form Swedish NONA immune longitudinal study. Exp Gerontol 42:753–761
Suzuki K, Hirokawa K, Hatakeyama S (1984) Age-related change of distribution of immunoglobulin containing cells in human bone marrow. Changes in patients with benign monoclonal gammopathy and multiple myeloma. Virchows Arch A Pathol Anat Histopathol 404:243–251
Utsuyama M et al (1992) Differential age-change of CD4+CD45RA+ and CD4+CD29+ T cells subsets in human peripheral blood. Mech Ageing Dev 63:57–66
Veneri D et al (2007) Changes of human B and B-1a peripheral blood lymphocytes with age. Hematology 12:337–341
Wieczorowska-Tobis K et al (2006) Can an increased level of circulating IL-8 be a predictor of human longevity? Med Sci Monit 12:CR118–CR121
Xie D, McElhaney JE (2007) Lower GrB+CD62Lhigh CD8TCM effector lymphocyte response to influenza virus in older adults is associated with increased CD28nullCD8+ T lymphocytes. Mech Ageing Dev 128:392–400
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Section Editor information
Rights and permissions
Copyright information
© 2019 Springer Nature Switzerland AG
About this entry

Cite this entry
Utsuyama, M., Yoshida-Kikuchi, Y., Kitagawa, M., Hirokawa, K. (2019). Age-Related Changes in Subpopulations of Peripheral Blood Lymphocytes in Healthy Japanese Population. In: Fulop, T., Franceschi, C., Hirokawa, K., Pawelec, G. (eds) Handbook of Immunosenescence. Springer, Cham. https://doi.org/10.1007/978-3-319-99375-1_11
Download citation
DOI: https://doi.org/10.1007/978-3-319-99375-1_11
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-99373-7
Online ISBN: 978-3-319-99375-1
eBook Packages: Biomedical and Life SciencesReference Module Biomedical and Life Sciences