
Abstract
The temperament of behavioral inhibition (BI) is classically defined based on behavioral observations of a child’s fear and avoidance of novelty. Such behavioral observations have proven powerful in identifying individual differences in temperament, and such differences have been shown to be predictive of later developmental outcomes, particularly levels of shyness or anxiety. However, behavioral observations alone leave open several questions, including: (1) How does the brain of a child high in behavioral inhibition differ from a child low in behavioral inhibition? (2) Which domains of cognition are directly related to variation in behavioral inhibition? (3) For domains of cognition not directly related to behavioral inhibition, how do individual differences interact with behavioral inhibition to predict later risk for anxiety? Examining these questions, research has demonstrated that individual differences in the child’s ability to monitor and control their behaviors when trying to complete a goal, a set of processes known as “cognitive control,” may change the likelihood of a child high in behavioral inhibition developing later anxiety. However, relations between behavioral inhibition and cognitive control have been inconsistent across studies. Here, we leverage a cognitive neuroscience framework to review studies that have investigated the interrelations between behavioral inhibition, cognitive control, and anxiety. Critically, we separate cognitive control into the subdomains of “monitoring” and “control instantiation” as well as further parse control instantiation based on domain and time course. In making these distinctions, we show that there is consistent evidence that the behavioral inhibition phenotype is directly related to increased monitoring, but not levels of control instantiation. However, behavioral inhibition is related to the time course of control, and both monitoring and control interact with behavioral inhibition to predict increased risk for the development of anxiety. We suggest that continued progress in understanding the interrelations between behavioral inhibition and cognitive control will require a similar framework that separates cognitive control into subdomains.
Access provided by CONRICYT-eBooks. Download chapter PDF
Similar content being viewed by others

Keywords
- Behavioral inhibition
- Anxiety
- Response monitoring
- Cognitive control
- Inhibitory control
- Error related negativity
Behavioral inhibition (BI) is an early childhood temperament, grounded in biology (Fox, Henderson, Marshall, Nichols, & Ghera, 2005), characterized by negative reactivity and avoidance within new situations or in the presence of strangers (Fox et al., 2005; Kagan, Reznick, & Snidman, 1988). Behavioral inhibition is a known risk factor for the later development of anxiety (Chronis-Tuscano et al., 2009; Frenkel et al., 2015), particularly social anxiety (Clauss & Blackford, 2012). However, not all children with a history of behavioral inhibition develop anxiety, and there is substantial interest in identifying what individual and environmental factors influence the relations between behavioral inhibition and anxiety.
Individual differences in behavioral inhibition ultimately reflect individual differences at a neurocognitive level . Therefore, adopting a cognitive neuroscience approach in the study of behavioral inhibition can provide unique information about this temperament. Indeed, advances in neuroimaging techniques, and their application to the study of development, have led to considerable advances in our understanding of the behavioral inhibition phenotype and its relation to later anxiety. The present chapter integrates these recent findings and sketches the emerging neurocognitive picture of behavioral inhibition and how this temperament relates to the development of anxiety (see also Blackford et al. in chapter “The Neurobiology of Behavioral Inhibition as a Developmental Mechanism”).
Children with behavioral inhibition have been shown to cognitively process the world differently than children without behavioral inhibition. Children high in behavioral inhibition pay attention to different things in their environment (Pérez-Edgar et al., 2010), process threatening or novel stimuli differently (Schwartz, Wright, Shin, Kagan, & Rauch, 2003), and monitor and control their behavior differently (McDermott et al., 2009), compared to children low in behavioral inhibition. In this chapter, we focus on this last set of differences, outlining how children high in behavioral inhibition differ from children low in behavioral inhibition in terms of their ability to monitor and control behavior, a set of processes generally referred to as “cognitive control. ” We take a cognitive neuroscience perspective and focus on two main questions: (1) What aspects of cognitive control are related to variations in the behavioral inhibition phenotype? (2) What aspects of cognitive control interact with the behavioral inhibition temperament to predict later anxiety?
To foreshadow our answers to these questions, the literature seems to support the notion that behavioral inhibition is directly associated with hypersensitive monitoring of behavior. That is, children with high levels of behavioral inhibition spend more energy paying attention to their behaviors and environment. Moreover, this increased monitoring of behavior appears to increase risk for children high in behavioral inhibition to later develop anxiety. Similarly, control processes also appear to exacerbate the risk for later anxiety in children high in behavioral inhibition. However, unlike monitoring, increased control processes do not appear integral to the behavioral inhibition phenotype. We end this chapter with a discussion of outstanding research questions and the need for additional research to further clarify relations between behavioral inhibition, cognitive control, and anxiety.
The Behavioral Inhibition Phenotype
Before discussing the neuroscience of behavioral inhibition , and its relations with anxiety, it is important to provide a more detailed sketch of the behavioral inhibition phenotype and related concepts. Kagan, Reznick, Clarke, Snidman, and Garcia-Coll (1984) first described behavioral inhibition, referring to children exhibiting high levels of this temperament as displaying “inhibition to the unfamiliar” (see the chapter “The History and Theory of Behavioral Inhibition” by Kagan). These children display an aversion and negative reactivity toward strangers, novel toys, or new situations (Fox, Henderson, Rubin, Calkins, & Schmidt, 2001; Kagan & Snidman, 1991). In general, it is believed that these children exhibit increased reactivity of fear circuitry, a theory supported by more recent neuroimaging findings (Schwartz et al., 2003).
It should be noted that Kagan and Snidman (2004) prefer to denote early infant reactivity as the actual temperament, with observed behaviors in toddlerhood as one of the outcomes of the temperament. In contrast, we define the behavioral inhibition temperament as a set of inhibited behaviors observed during toddlerhood. Our basis for denoting the behavioral inhibition temperament as a phenotype observed in toddlerhood grows out of a series of studies finding that fear-related behavior (e.g., avoidance and freezing) in toddlerhood was related to and predicted biological differences (e.g., heart rate, cortisol, EEG) measured during toddlerhood and later (Fox et al., 2005). It is also worth noting that a related behavioral profile, social reticence, emerges in the early school years (Coplan, Rubin, Fox, Calkins, & Stewart, 1994). Social reticence is characterized by the avoidance of peer interactions while maintaining vigilance and attention toward these peers (see the chapter “Peer Relations and the Behaviorally Inhibited Child” by Rubin et al.). While behavioral inhibition in toddlerhood is predictive of later social reticence (Degnan et al., 2014), and behavioral inhibition is predicted by prior infant reactivity (Fox, Snidman, Haas, Degnan, & Kagan, 2015), we believe these phenomena reflect three related, but distinct, constructs. Thus, we reserve the term “behavioral inhibition” for the behavioral phenotype observed during toddlerhood and focus on this phenotype throughout the chapter.
Here, it is also worth noting related work by Rothbart (1981) and Rothbart and Bates (2006), which defines temperament within a dimensional structure. Briefly, this model of temperament classifies infants and young children in terms of “reactivity,” reflecting both positive and negative reactivity, and “regulation,” reflecting the ability of infants and children to self-sooth and control their own behavior (Rothbart, 1981; Rothbart & Bates, 2006). We note here that our conceptualization of behavioral inhibition and relations with cognitive control exhibit strong similarities to the prior conceptualization put forth by Rothbart (1981) and Rothbart and Bates (2006). Whereas prior work by Kagan et al. (1984) largely treated behavioral inhibition as a categorical variable (i.e., presence vs. absence of behavioral inhibition), we tend to explore behavioral inhibition as a continuous variable and treat the behavioral inhibition temperament as such within this chapter. Moreover, a key contribution of the Rothbart model was the conceptualization of self-regulation as an aspect of temperament (Rothbart, 1981; Rothbart & Bates, 2006). We continue this theoretical tradition here by investigating the relations between behavioral inhibition and cognitive control, with cognitive control reflecting strong similarities to the “regulation” dimension of Rothbart’s model (Rothbart, 1981; Rothbart & Bates, 2006).
Cognitive Control: Monitoring and Control Instantiation
Cognitive control refers to the set of neurocognitive processes allowing individuals to monitor and flexibly adapt their behavior in an effort to achieve a goal (Botvinick, Braver, Barch, Carter, & Cohen, 2001; Holroyd & Coles, 2002). A goal can be anything from a child riding their new bicycle along the sidewalk to performing well on a computer-based laboratory task. Although the distinction is sometimes made in the literature, researchers do not frequently enough define and study the various constructs that make up “cognitive control.” In this chapter, we argue that distinguishing among different components of cognitive control helps explain seemingly paradoxical findings between behavioral inhibition and cognitive control and highlights avenues for future research. While multiple taxonomies are possible (e.g., Nigg, 2017; Shenhav, Botvinick, & Cohen, 2013) and often useful, here we rely primarily on a simple distinction between the constructs of “monitoring” and “control instantiation.” We further parse control instantiation where appropriate but maintain a monolithic treatment of monitoring throughout the chapter.Footnote 1
We use the term “monitoring ” to refer to the neurocognitive processes associated with detecting when something goes wrong or noticing when changes occur that will impair the ability to achieve a goal. In the example of safely riding a bicycle down the street, monitoring would refer to noticing deviations from this goal, like accidentally swerving into the street or seeing objects on the sidewalk obstructing the path. In contrast, we reserve the term “control instantiation” for changes made to behavior (along with associated neural correlates) to increase the likelihood of achieving a goal. In the bicycle example, control instantiation would refer to the child changing their course direction or paying more attention after they detect themselves swerving into the street. Thus, monitoring and control instantiation are two complementary, but distinct, constructs of the broader concept of cognitive control.
In this chapter, we first review approaches to studying monitoring, relations with the behavioral inhibition phenotype, and ultimately, how interactions between monitoring and behavioral inhibition predict risk for later anxiety. Next, we turn to a description of control instantiation and the interrelations with behavioral inhibition and anxiety. Finally, we integrate findings across the monitoring and control domains and outline the emerging picture of relations between behavioral inhibition, cognitive control, and anxiety. We end this chapter with a discussion of outstanding questions and future research directions that should be pursued.
Monitoring
Within the laboratory, behavioral tasks and physiological recordings are often used to study monitoring. While monitoring is difficult to study directly at the behavioral level, one approach taken is to observe how behavior changes after participants make an error on a computer-based task (Danielmeier & Ullsperger, 2011). It is assumed that when the brain’s performance monitoring system detects a mistake, individuals slow down or improve their accuracy on the following trial. This way, researchers can indirectly assess whether the participant detected the mistake (i.e., whether the participant was monitoring their behavior or not). A problem with this approach, however, is that such behavioral measures are heavily confounded by control instantiation. Presumably, if an individual detects a mistake, then they will instantiate control in some way (e.g., increasing attention) to prevent future mistakes. Thus, the most direct approach to studying monitoring processes in children is to use neuroimaging techniques.
In adults, a substantial literature has identified a network of neural regions, centered around the cingulate cortex, which forms the performance monitoring system (Ullsperger, Danielmeier, & Jocham, 2014). Activation of this system can be reliably indexed using either functional magnetic resonance imaging (fMRI) or electroencephalography (EEG). For example, when participants make an error on a computer-based task , fMRI reveals increased activation within the medial frontal cortex (MFC), including the cingulate cortex (Ridderinkhof, Ullsperger, Crone, & Nieuwenhuis, 2004). Similarly, EEG recordings demonstrate a characteristic pattern of event-related potential (ERP) activity following errors: a negative voltage deflection over frontocentral scalp locations, termed the error-related negativity (ERN ; Gehring, Liu, Orr, & Carp, 2012), followed by a slower, positive voltage deflection over centroparietal scalp locations, termed the error positivity (Pe; Overbeek, Nieuwenhuis, & Ridderinkhof, 2005; Steinhauser & Yeung, 2010).
Source localization estimates of the ERN and Pe have localized these ERPs to a network of neural regions centered on the cingulate cortex (i.e., the performance monitoring system; Buzzell et al., 2017; Debener et al., 2005; Herrmann, Römmler, Ehlis, Heidrich, & Fallgatter, 2004). Additionally, time-frequency analyses focusing on theta-band EEG oscillations can be employed as a reliable index of performance monitoring system activation in response to errors (Cavanagh, Zambrano-Vazquez, & Allen, 2012). However, errors need not occur for the performance monitoring system to become activated, with increased activity having been observed for conflict (Buzzell, Roberts, Baldwin, & McDonald, 2013), uncertainty (Buzzell et al., 2016), external feedback about a task (Holroyd & Coles, 2002), or changes in task difficulty (Petersen & Posner, 2012). In sum, the performance monitoring system monitors for any situation that might signal the need for a participant to stop performing a task in an automatic fashion and, instead, instantiate control.
Monitoring and Behavioral Inhibition
Leveraging neuroimaging techniques , the literature consistently demonstrates that the behavioral inhibition phenotype is integrally linked to increased monitoring. The first evidence for a link between behavioral inhibition and neural measures of monitoring came from the study by McDermott et al. (2009). This study examined ERN magnitude in adolescence within a longitudinal cohort of children assessed for levels of behavioral inhibition in childhood, as a neural index of monitoring. Children with a history of behavioral inhibition had a significantly larger ERN, suggesting increased monitoring in these children (McDermott et al., 2009). Subsequent work in a separate cohort of children replicated this effect even earlier, at age 7 (Lahat et al., 2014).
In this second cohort, the ERN was assessed again in adolescence, both while the children believed they were being observed by others and also while alone (Buzzell et al., 2017). This social manipulation was done to capture the effects of social context on monitoring. The social context is thought to be particularly relevant for behavioral inhibition, as early behavioral inhibition is most evident in novel social situations and predicts both social reticence (Degnan et al., 2014) and social anxiety later in development (Chronis-Tuscano et al., 2009; Clauss & Blackford, 2012). Critically, increases in the ERN while under social observation were greatest for children with a history of behavioral inhibition (Buzzell, Troller-Renfree, et al., 2017). This more recent study demonstrates that beyond general increases in monitoring for children high in behavioral inhibition, monitoring in social contexts is particularly elevated (see the chapter “The Neural Mechanisms of Behavioral Inhibition” by Jarcho and Guyer and the chapter “The Social World of Behaviorally Inhibited Children: A Transactional Account” by Henderson et al.).
Beyond increased error monitoring, research also consistently reveals that children with a history of being high in behavioral inhibition exhibit increased activation of the performance monitoring system in response to a variety of events. For example, compared to children lower in behavioral inhibition, children higher in behavioral inhibition display heightened fMRI activity within the cingulate cortex—a key region of the performance monitoring system—for trials with high levels of stimulus conflict (i.e., for incongruent trials on an emotional Stroop task; Jarcho et al., 2013).
Moreover, similar findings were found when the N2 ERP component was employed as an index of monitoring (Lahat et al., 2014). Using a flanker task, 7-year-old children with a history of high behavioral inhibition exhibited a larger N2 to incongruent (high conflict) flanker stimuli (Lahat, Walker, et al., 2014). When these same children performed a go/no-go task, children with higher behavioral inhibition again demonstrated a larger N2, this time in response to infrequent “no-go” stimuli that require control (Lamm et al., 2014). This latter study also applied a source localization approach to estimate the neural source of the increased N2 component. Analyses revealed that children with higher behavioral inhibition had increased activity, in part, within the cingulate cortex (Lamm et al., 2014). To summarize, substantial evidence using fMRI, ERP, or EEG source localization approaches are consistent with the notion that the behavioral inhibition phenotype is associated with increased monitoring.
Monitoring, Behavioral Inhibition, and Anxiety
Parallel to the finding that behavioral inhibition is directly associated with increased monitoring, substantial research in adults and adolescents demonstrate that anxiety is also associated with increased monitoring, particularly in response to errors. Indeed, two reviews and a meta-analysis have linked increases in the ERN and frontal-midline theta oscillations of the EEG—both indices of error monitoring—to anxiety (Cavanagh & Shackman, 2015; Meyer, 2017; Moser, Moran, Schroder, Donnellan, & Yeung, 2013). However, it is also important to note that relations between the ERN and anxiety in children are mixed, at least when assessed at subclinical levels (for a review, see Meyer, 2017).
Recently, it has been suggested that relations between the ERN and subclinical anxiety changes direction as a function of age, with such a shift tracking normative development of fear and anxiety (Meyer, 2017). In very young children, anxiety associated with self-monitoring and the ERN may be limited, and instead anxious cognition may be associated with more external sources of fear (e.g., a strange developmental psychologist looking on as EEG is recorded). However, as children become older, sources of anxiety may shift toward an internal focus on one’s mistakes, and a concomitant increase in the ERN (Meyer, 2017). However, Meyer (2017) also notes that for children with clinical levels of anxiety, the typical relation between the ERN and anxiety is still observed, where a larger ERN is related to increased anxiety.
Alternatively, the theoretical framework put forth by Moser et al. (2013) suggests that the ERN is not a risk marker for later anxiety, but rather a symptom of anxiety. These authors suggest that the increased ERN observed in adolescents or adults with anxiety is the result of anxious cognition causing distraction and a shift toward a more in-the-moment style of cognitive control termed “reactive control.” One index for the shift toward a reactive strategy is increased effort (i.e., a larger ERN) at the monitoring stage of task processing (Moser et al., 2013). However, no evidence to date has ruled conclusively in favor of either the theoretical framework put forth by Moser et al. (2013) or the hypothesis suggested by Meyer (2017). To summarize, what remains clear in the literature is that consistent and robust relations between anxiety and a larger ERN are present in both adults and adolescents, whereas findings in young children have been mixed and theoretical explanations remain debated.
It is important to note that while relations between the ERN and anxiety in children have been mixed, the relations between behavioral inhibition and the ERN have been remarkably consistent. Studies reliably find that behavioral inhibition is predictive of an enhanced ERN in childhood (Lahat, Lamm, et al., 2014), late childhood to early adolescence (Buzzell, Troller-Renfree, et al., 2017), or mid-to-late adolescence (McDermott et al., 2009). Perhaps more striking, longitudinal relations between early behavioral inhibition and later anxiety are also consistently moderated by the level of monitoring that these children display, with increased monitoring—as measured by the ERN—amplifying the strength of longitudinal relations between behavioral inhibition and anxiety (Lahat, Lamm, et al., 2014; McDermott et al., 2009).
It should also be noted that a third study by Buzzell, Beatty, Paquette, Roberts, and McDonald (2017) reports on a mediation model in which ERN examined at age 12, specifically within social contexts, mediates relations between early behavioral inhibition and later social anxiety, but only when behavioral measures (post-error response time) are also included in the model. This more nuanced mediation model suggests one possible mechanism that takes into account social influences on brain and behavior and directly links behavioral inhibition to the development of social anxiety. Later in the chapter, we detail this mechanism outlined by Buzzell, Richards, et al. (2017).
However, it is important to note here that additional, unpublished analyses of the data reported by Buzzell, Troller-Renfree, et al. (2017) demonstrate that when the social context of the ERN is ignored, the ERN at age 12 also moderates the relation between behavioral inhibition and anxiety. That is, consistent with prior work (Lahat, Lamm, et al., 2014; McDermott et al., 2009), behavioral inhibition predicted later social anxiety only for children with a large ERN in this dataset as well. In this new analysis, social context was ignored, and the ERN was calculated as a difference wave (delta-ERN) based on all trials in the experiment. Thus, in all three of these studies (Buzzell, Troller-Renfree, et al., 2017; Lahat, Lamm, et al., 2014; McDermott et al., 2009), which span two longitudinal cohorts and three separate assessment ages, behavioral inhibition was predictive of later anxiety only for children with a relatively larger ERN.
Given that direct relations between the behavioral inhibition phenotype and an enhanced ERN also exists, these moderation analyses suggest that the monitoring component of behavioral inhibition plays a critical role in the development of later anxiety. Of course, we do not suggest that increased monitoring for children high in behavioral inhibition is the sole mechanism through which anxiety develops; indeed we contend that there are many developmental pathways through which anxious cognition may emerge. For instance, behavioral inhibition is also known to be associated with heightened reactivity of fear circuitry within the brain (Schwartz et al., 2003), a mechanism that undoubtedly plays a crucial role in the development of later anxiety. Nonetheless, increased monitoring, which appears to be an inherent feature of the behavioral inhibition phenotype, seems to play a critical role in the development of later anxiety.
Why would increased monitoring, which is commonly thought to be a useful and adaptive cognitive process, predispose an individual to develop clinical levels of anxiety? To answer this question, it is important to reflect on the phenotype of anxiety, and more specifically, social anxiety. Symptoms of social anxiety include rumination, worry, and self-focus, specifically within social contexts or while under social evaluation (Clark & Wells, 1995; Rapee & Heimberg, 1997). While worry or self-focus may be adaptive when maintained at normative levels, excessive worry or self-focus can drain attentional resources and lead to distraction (Eysenck, Derakshan, Santos, & Calvo, 2007; Moser et al., 2013; Rapee & Heimberg, 1997). Similarly, recent research has shown that monitoring can also sometimes lead to distraction (Buzzell, Beatty, et al., 2017; der Borght, Schevernels, Burle, & Notebaert, 2016), as opposed to control (Botvinick et al., 2001).
That is, it may be that monitoring is only adaptive when it leads to control instantiation. If you recognize that you are doing something wrong, but don’t do anything about it, that is not an adaptive process. If monitoring does not translate into control instantiation, or if excessive monitoring actually leads to impaired performance (Buzzell, Beatty, et al., 2017; Buzzell, Troller-Renfree, et al., 2017), then such a process becomes maladaptive and even pathological. Indeed, Moran, Bernat, Aviyente, Schroder, and Moser (2015) have shown that while anxious adults exhibit increased monitoring, as measured by a larger ERN, they also demonstrate a reduced ability to instantiate control following error detection, as measured by reduced interchannel phase synchrony (a measure of functional connectivity between medial and later prefrontal cortices). Thus, at least one reason why increases in monitoring might be associated with increased risk for anxiety is the propensity for excessive monitoring to cause distraction.
Given that behavioral inhibition is most strongly predictive of developing social anxiety as opposed to other subtypes of anxiety (e.g., generalized, specific phobia), the question remains as to why a relatively general neural response to error monitoring relates to behavioral inhibition and the development of a highly specified, and social-specific, disorder. One hypothesis is that within the majority of lab-based EEG studies, participants might believe that the experimenters are evaluating their performance to some degree. This is likely true even when the experimenters remain outside the room while the participant performs the task. Therefore, many of the studies investigating the ERN may, at least indirectly, reflect the measurement of error monitoring while under social observation.
Critically, the phenotypes of social anxiety (Clark & Wells, 1995; Rapee & Heimberg, 1997) and behavioral inhibition (Fox et al., 2005; Kagan et al., 1984) are most prevalent under social evaluation, or social settings in general. Therefore, it may be the presence of increased monitoring while under social observation that is most closely related to behavioral inhibition and social anxiety. In line with this hypothesis, three studies in adults have shown that not only does explicit manipulation of social evaluation increase the ERN magnitude (Hajcak, Moser, Yeung, & Simons, 2005) but that such increases are greatest for those with social (Barker, Troller-Renfree, Pine, & Fox, 2015) or performance (Masaki, Maruo, Meyer, & Hajcak, 2017) anxiety.
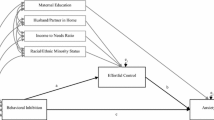
Similarly, a longitudinal study of children that were previously assessed for behavioral inhibition found that such social-specific increases in the ERN were directly predicted by behavioral inhibition levels measured approximately 10 years prior (Buzzell, Troller-Renfree, et al., 2017). More importantly, longitudinal relations between behavioral inhibition and social anxiety were explained by social-specific ERN increases, along with a maladaptive response to errors: post-error response time slowing (Buzzell, Troller-Renfree, et al., 2017). This most recent finding provides strong evidence for the hypothesis that excessive monitoring, particularly within social contexts, is one aspect of the behavioral inhibition phenotype that plays a critical role in the development of social anxiety later in life. Moreover, these data provide evidence that it is the maladaptiveness of such excessive error monitoring that leads to pathological levels of social anxiety: error monitoring only explained relations between behavioral inhibition and social anxiety insofar as greater slowing after errors in the social condition—with no improvement in accuracy—was observed (Buzzell, Troller-Renfree, et al., 2017). These findings open up an intriguing new line of research, though additional studies are needed.
Control Instantiation
Although the notion of monitoring is relatively monolithic, control instantiation can be meaningfully parsed into subdimensions. First, the type of control instantiation is important to specify. For example, two common types of control instantiation include, but are not limited to, inhibiting responses (inhibitory control) and switching between different tasks (task switching). Briefly, inhibitory control refers to the suppression of a stimulus representation, motor command, or other neural process, typically through suppression of motor-related neural activity (Aron, 2007). Task switching refers to the ability to flexibly switch between two (or more) sets of maintained information, task rules, or other neural ensembles, each of which is associated with alternative task goals (Braver, Reynolds, & Donaldson, 2003).
Additionally, control instantiation can be divided into whether it is deployed before or after a cognitively demanding event (e.g., conflict). Proactive control refers to the instantiation of control in an anticipatory manner, before the cognitive demand (Braver, 2012). In contrast, reactive control refers to the instantiation of control in a “just-in-time” manner, as it is needed, after the conflict occurs (Braver, 2012). In the example of a child riding their bike, if the child were to pay extra attention to the sidewalk and their steering, in an effort to prevent veering into the street, this would be an example of proactive control. In contrast, if the child were simply to wait until they accidently veered into the street, reacting to this event with corrective behavior, this would be an example of reactive control. It is worth noting that both proactive and reactive control can be adaptive, depending on the context, and healthy human behavior is associated with the use of both proactive and reactive control.
Similar to the construct of monitoring, control instantiation can be assessed using behavioral metrics , although not perfectly. Simply put, if a task is designed such that it requires control instantiation to be performed well, then a child’s control instantiation abilities can be indirectly inferred from how accurately (and quickly) they perform the task. For example, in order to measure inhibitory control, a “go/no-go” task can be employed, which requires participants to frequently respond to “go” stimuli while infrequently inhibiting responses to “no-go” stimuli (Bokura, Yamaguchi, & Kobayashi, 2001). Using such a task, accuracy on no-go trials can be measured as an index of control instantiation, more specifically inhibitory control. Alternatively, in order to test whether children instantiate control following a mistake, accuracy rates on trials that follow errors can be assessed (Danielmeier & Ullsperger, 2011).
However, the same problem that plagues behavioral measures of monitoring applies to the assessment of control instantiation. That is, behavioral measures of control instantiation are heavily confounded with monitoring, as control instantiation is rarely implemented without monitoring processes first detecting the need for control instantiation. Moreover, a given task that is designed to putatively measure a specific type of control is often confounded by other types of control that are also required to perform the task. For example, in a go/no-go task, not only is inhibitory control needed, but also attentional control directed toward the go and no-go stimuli is required (Schröger, 1993). Fortunately, control instantiation can be readily assessed using neural measures, allowing for selective measurement of brain regions known to be associated with a given control process.
The neural correlates of control instantiation are dependent on the type of control that is being instantiated. For example, if a task requires increased attentional allocation, then this will be observed in fMRI recordings as increased activity within a frontoparietal network, thought to be the source of attentional control (Corbetta & Shulman, 2002), along with amplification of the attended stimuli within the relevant sensory cortex. In contrast, if a task requires the inhibition of motor responses, activity within prefrontal and motor cortices will be observed (Aron, 2007). Evidence for control instantiation can also be observed using EEG, by assessing whether sensory processing is enhanced as the result of attention control (Roberts, Fedota, Buzzell, Parasuraman, & McDonald, 2014), or oscillations within the motor cortex are altered as the result of inhibitory control (Bengson, Mangun, & Mazaheri, 2012). In relation to determining proactive vs. reactive control instantiation, the location of neural activity does not typically differ, but the time course of activation does (Braver, 2012). That is, proactive control is associated with increased and sustained activation prior to the need for control, whereas reactive control is associated with increased neural activity closer in time, or following, when the control is needed.
Control Instantiation and Behavioral Inhibition
Evidence for relations between control instantiation and behavioral inhibition have been sparse and mixed. A relatively early study found that increases in control instantiation, particularly inhibitory control, was directly related to the behavioral inhibition phenotype (Thorell, Bohlin, & Rydell, 2004). In particular, Thorell et al. (2004) found that laboratory-based assessments of behavioral inhibition at age 5 were positively correlated with performance on go/no-go task, designed to assess inhibitory control. More recently, Lamm et al. (2014) also demonstrated that behavioral inhibition might be directly related to inhibitory control, finding that behavioral inhibition in toddlerhood was predictive of increased accuracy on a go/no-go task at age 7.
Despite these results, a number of studies have failed to identify a direct relation between the behavioral inhibition phenotype and inhibitory control (Jarcho et al., 2013, 2014; Lahat, Lamm, et al., 2014; Lahat, Walker, et al., 2014; Troller-Renfree et al., 2018; White, McDermott, Degnan, Henderson, & Fox, 2011). Additionally, the only study investigating relations between behavioral inhibition and attentional shifting found no relation between these constructs (White et al., 2011). Based on the results of these studies, it does not appear that there is strong evidence for a direct link between the behavioral inhibition phenotype and overall levels of control instantiation. However, in the section entitled “Control instantiation, behavioral inhibition, and anxiety,” we discuss substantial work suggesting that while the overall level of control instantiation may not relate directly to the behavioral inhibition phenotype, such control processes do seem to influence the strength of the relations between behavioral inhibition and later anxiety.
A recent study suggests that prior questions surrounding the direct relations between behavioral inhibition and control instantiation may have been ill posed. Instead of asking whether increased control is associated with behavioral inhibition, it might be better to ask whether the time course of control instantiation is what directly relates to behavioral inhibition. That is, perhaps a distinguishing feature of the behavioral inhibition phenotype is whether control is instantiated in a proactive vs. reactive manner, regardless of the overall intensity of control. Adopting this perspective, a recent study by Troller-Renfree, Buzzell, Pine, Henderson, and Fox (in press) employed the AX-CPT (Braver, 2012) to investigate whether the behavioral inhibition phenotype is directly related to a relatively stronger reactive control strategy, as opposed to a proactive control strategy.
The AX-CPT requires individuals to attend to one stimulus, the “cue,” and then respond to a second stimulus, “the probe,” based on the identity of both the cue and probe. Briefly, there are certain cue stimuli that are highly predictive of the probe, such that if proactive control is being used, performance should be most accurate on these trials. In contrast, there are also infrequent cue-probe pairings in which a different probe follows this cue. Here, performance will be impaired by the over-reliance on a proactive control strategy. Thus, by analyzing behavioral data from this task, it is possible to determine the degree to which a child relies relatively more on a proactive vs. reactive control strategy.
Using the AX-CPT, Troller-Renfree, Buzzell, Pine, et al. (in press) found that children with a history of increased behavioral inhibition have a tendency to not proactively deploy control in an effort to prevent mistakes. Rather, they seem to rely on employing control in a reactive and “just-in-time” manner.
While this recent finding is only the first step in probing whether the time course of control instantiation directly relates to the behavioral inhibition phenotype, these data suggest an intriguing possibility: prior work identifying a relation between behavioral inhibition and inhibitory control intensity (Lamm et al., 2014; Thorell et al., 2004) may have actually been driven by a stronger reactive control strategy in children with behavioral inhibition. The reason for this thinking is that tasks designed to test inhibitory control are often set up in such a way that inhibitory control cannot be deployed in a proactive manner; instead, these tasks seem to measure reactive inhibitory control. For example, in either a go/no-go or Stroop task, the most efficient method of performing these tasks well is to wait until the need for control is detected via monitoring processes and to then apply inhibitory control only at that point (i.e., to use a reactive control strategy). Thus, the occasional observations of a direct relation between behavioral inhibition and inhibitory control, at least at the behavioral level, may actually reflect the tendency for children with behavioral inhibition to adopt a reactive control strategy.
Control Instantiation, Behavioral Inhibition, and Anxiety
As previously mentioned, a review of the literature provides minimal evidence that increased control instantiation is an inherent component of the behavioral inhibition phenotype. Nonetheless, although control instantiation ability may reflect a developmentally distinct neurocognitive process that is orthogonal to the behavioral inhibition phenotype, control instantiation could still interact with behavioral inhibition to predict risk for anxiety . Additionally, at least one study to date has demonstrated that it is not the intensity of control instantiation but individual differences in the time course of control instantiation (i.e., proactive vs. reactive control) that is directly related to the behavioral inhibition phenotype (Troller-Renfree, Buzzell, Pine, et al., in press). Here, we review studies investigating whether the level of control instantiation, or the time course of control instantiation, interact with the behavioral inhibition phenotype to predict the development of later anxiety.
In both adults and children without a history of behavioral inhibition, increased levels of inhibitory control are typically associated with reduced anxiety symptoms (Eysenck et al., 2007; Kertz, Belden, Tillman, & Luby, 2015; Lengua, 2003). The fact that anxiety in either adults or children is associated with reduced levels of inhibitory control is a relatively intuitive connection: inhibitory control broadly reflects the ability to inhibit or control behavior, which might include the control or suppression of anxiety-provoking thoughts. Based on this logic, one might hypothesize that for children with a history of behavioral inhibition, lower levels of inhibitory control would exacerbate risk for developing later anxiety.
However, three studies, from two independent research groups, have actually demonstrated the opposite pattern: children with a history of behavioral inhibition and increased levels of inhibitory control are at greater risk of developing anxiety (Thorell et al., 2004; Troller-Renfree, Buzzell, Bowers, et al., 2018; White et al., 2011). In the first study, Thorell et al. (2004) found that 5-year-old children with high levels of behavioral inhibition and inhibitory control (assessed using a go/no-go task) were more likely to be rated as high in social anxiety by their teachers 3 years later. In a separate study by White et al. (2011), behavioral inhibition in early childhood (ages 2 and 3) was predictive of anxiety symptoms later in childhood (ages 4 and 5), but only for children with high levels of inhibitory control (as assessed using two Stroop tasks designed for children). Finally, in perhaps the most extensive investigation of relations between behavioral inhibition, inhibitory control, and later anxiety, Troller-Renfree, Buzzell, Bowers, et al. (2018) also found that higher levels of inhibitory control exacerbated later risk for anxiety, but only for children high in behavioral inhibition.
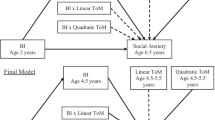
In this study, Troller-Renfree, Buzzell, Bowers, et al. (2018) analyzed the same cohort of children as White et al. (2011) but over a wider span of time (ages 2–12) and employed a go/no-go task to measure inhibitory control. Specifically, these authors had children perform a go/no-go task in the laboratory at ages 5, 7, and 9 and then modeled developmental slopes of inhibitory control ability across these time points, yielding initial estimates of the children’s inhibitory control ability at age 5, as well as estimates of how their inhibitory control ability changed over this 4-year period (e.g., an increasing, decreasing, or level slope). Troller-Renfree, Buzzell, Bowers, et al. (2018) found that behavioral inhibition predicted later social anxiety symptoms, but only for children with a steeper slope of inhibitory control development in the intervening years. This study not only provides additional evidence that high levels of inhibitory control ability increase risk for later anxiety in children with behavioral inhibition but also illustrates the importance of considering developmental trajectories in inhibitory control ability.
Given prior findings that increased levels of inhibitory control are protective against anxiety when behavioral inhibition is not measured or considered (Eysenck et al., 2007; Kertz et al., 2015; Lengua, 2003), why would the analyses involving behavioral inhibition show a categorically different set of relations? Some insight into this question comes from additional analyses in the study by White et al. (2011). In this study, children not only performed the Stroop task as a way to assess inhibitory control but also performed a Dimensional Change Card Sort Task, designed to assess task-switching ability (White et al., 2011). Recall that task switching reflects the ability to flexibly shift between various thoughts or behaviors based on task goals. Critically, White et al. (2011) found that for children high in behavioral inhibition, improved task-switching ability was indeed associated with a reduced risk for later anxiety.
Collectively, the study by White et al. (2011) suggests that not all forms of control instantiation are associated with increased risk for later anxiety for children with a history of behavioral inhibition. In fact, the only type of control instantiation that has been shown to increase risk for developing anxiety in children high in behavioral inhibition is inhibitory control. One possibility is that increased levels of inhibitory control leads to an “over controlled” and less flexible style of responding and interacting with others (Henderson, Pine, & Fox, 2015).
The studies to date support the notion that inhibitory control is a risk factor for later anxiety development in children with behavioral inhibition. However, it is important to note that extant research investigating these relations have relied solely on behavioral measures of inhibitory control. As mentioned above, inferences that can be drawn from behavioral measures of inhibitory control are limited—these measures are almost always confounded by monitoring. Because of this, an improved ability to monitor one’s behavior would lead to improved task performance even if the intensity of inhibitory control ability were held constant.
In order to rule out this alternative explanation, neural measures of both inhibitory control ability and monitoring would need to be assessed concurrently in the same children and controlled for. Thus, while the current literature suggests inhibitory control increases risk for later anxiety, neural evidence supporting this claim is needed. Using the AX-CPT, Troller-Renfree, Buzzell, Pine, et al. (in press) demonstrated that not only is behavioral inhibition (at ages 2 and 3) predictive of a more reactive control strategy at age 12 but that this control strategy moderates longitudinal relations between behavioral inhibition and social anxiety. Specifically, children with a history of behavioral inhibition only developed social anxiety symptoms if they also exhibited a more reactive control strategy (Troller-Renfree, Buzzell, Pine, et al., in press). Such findings are consistent with the fact that behavioral measures of increased inhibitory control also increase the likelihood that children with behavioral inhibition will develop anxiety, given that studies used to investigate inhibitory control often encourage a reactive control strategy. However, additional investigations of how behavioral inhibition and anxiety relate to both the intensity and time course of control instantiation, at both the behavioral and neural level, are needed.
The Emerging Picture
In surveying the existing literature on relations between behavioral inhibition and cognitive control, a coherent picture begins to emerge. An inherent aspect of the behavioral inhibition phenotype appears to be excessive monitoring, especially while under social evaluation, along with the adoption of a more reactive control strategy. In contrast, the majority of the evidence suggests that behavioral inhibition is not directly related to levels of control instantiation (inhibitory control or task switching).
That is, when placed within situations that require control, children with behavioral inhibition do not plan ahead, nor flexibly adapt their behavior. Instead, these children appear to excessively monitor their own behavior and such monitoring does not appear to be adaptive for children with behavioral inhibition as they are more likely to develop anxiety. These findings are largely in agreement, as behavioral tasks that assess inhibitory control often encourage a reactive control strategy, and increased monitoring is necessary to adopt such a reactive control strategy. It is worth noting that this generalization of behavioral inhibition and later risk for anxiety is not without limitations. An improved understanding of how cognitive control relates to behavioral inhibition and risk for anxiety will require additional longitudinal research that incorporates assessment of cognitive control using multiple tasks and neuroimaging techniques. Below, we outline unresolved issues and suggestions for future research within this domain.
Unresolved Questions and Future Directions
Need for More Longitudinal Research
It is worth noting that the majority of studies investigating relations between behavioral inhibition and cognitive control come from two longitudinal cohorts, studied by the same research group. An astounding degree of internal consistency has been observed in the results of several distinct experimental tasks assessing cognitive control within these two cohorts. However, strong scientific theory not only requires replication but also replication by independent researchers. While research by some independent research groups have corroborated the findings outlined here (Thorell et al., 2004), other work appears to conflict with these findings (Torpey et al., 2013). Thus, additional research into the relations between behavioral inhibition and cognitive control, preferably within a longitudinal context, is critically needed.
Does Inhibitory Control Relate to Behavioral Inhibition and Later Anxiety?
Throughout this chapter, we have asked which aspects of cognitive control are inherent to the behavioral inhibition phenotype, as well as which processes interact with behavioral inhibition to predict later risk for anxiety. Some evidence that inhibitory control is inherent to the behavioral inhibition phenotype has been published (Lamm et al., 2014; Thorell et al., 2004), though the majority of work suggests that inhibitory control is a developmentally distinct process (Jarcho et al., 2013, 2014; Lahat, Lamm, et al., 2014; Lahat, Walker, et al., 2014; Troller-Renfree, Buzzell, Bowers, et al., 2018; White et al., 2011). Inhibitory control does appear to consistently increase risk for later anxiety in children with a history of behavioral inhibition. However, such findings have relied exclusively on behavioral measures.
Given that tasks measuring inhibitory control are often confounded with monitoring and a reactive control strategy, other explanations are possible. A simple solution to this issue is to employ neural measures of inhibitory control to isolate this process from monitoring. For example, synchronized EEG oscillations between electrodes located over the frontal and motor cortices, or fMRI-based measures (e.g., increased correlation in the blood flow within frontal and motor regions), could both be taken as direct evidence of inhibitory control. Moreover, concurrent measurement of proactive vs. reactive control strategy could be assessed and controlled for. Such an approach would allow for a direct test of (1) whether inhibitory control is an inherent aspect of the behavioral inhibition phenotype and (2) whether increased inhibitory control exacerbates risk for later anxiety.
Why Does Increased Monitoring Increase Anxiety Risk ?
Monitoring is typically viewed as an adaptive process, allowing for the detection of situations that require control, allowing us to reach our goals. Within this context, why is excessive monitoring a risk factor for anxiety? Recent cognitive neuroscience research demonstrates that monitoring can sometimes cause distraction (Buzzell, Beatty, et al., 2017; der Borght et al., 2016; Purcell & Kiani, 2016) and that such a mechanism may help to explain why excessive monitoring is associated with anxiety (Buzzell, Troller-Renfree, et al., 2017). However, the boundary conditions of this effect are unknown.
Is the relation between monitoring and controlling an inverted “U” with a moderate amount of monitoring beneficial and an excessive amount maladaptive? Or, alternatively, is it that individuals with anxiety simply lack an additional mechanism that translates monitoring into control instantiation? If anxious individuals simply lack this secondary process, excessive monitoring could be a way to boost a “leaky signal” that connects monitoring and control instantiation in anxious individuals. Relatedly, what are the contexts within which excessive monitoring may or may not be maladaptive for anxious individuals? It appears that excessive monitoring is maladaptive within social situations, at least for children with a history of high behavioral inhibition (Buzzell, Troller-Renfree, et al., 2017). However, future work will be needed to directly test the alternative theories of maladaptive error monitoring in these children. Does the arousal from social situations simply push their monitoring toward the extreme end of an inverted “U,” overloading the cognitive system and causing distraction? Or does social situation impair the effectiveness of a separate mechanism linking monitoring and control?
Does the Time Course of Cognitive Control Matter?
To date, there has only been one study that investigates the time course of control instantiation in children with a history of behavioral inhibition (Troller-Renfree, Buzzell, Pine, et al., in press). It is critical that this finding be replicated but also that similar relations are evaluated at younger ages and in conjunction with neuroimaging approaches. Moreover, it would be helpful to test whether the control strategy adopted by children with behavioral inhibition changes based on the type of control being assessed, such as attentional control compared to inhibitory control. Finally, assessing the time course of control, and perhaps even monitoring, at much longer timescales (i.e., hours and days) could also be informative. For example, does anticipatory anxiety reflect excessive monitoring or control instantiation prior to an anxiety-provoking event? To summarize, the recent study by Troller-Renfree, Buzzell, Pine, et al. (in press) presents an exciting new line of research to pursue in terms of understanding of behavioral inhibition and relations to later anxiety; however, much more work is needed within this domain.
Need for Multidimensional Assessments of Cognitive Control
Throughout this chapter, we have reviewed a series of studies that each focus on one, or at most two, aspects of cognitive control. However, performing even simple laboratory tasks requires a coordinated effort across the brain, involving multiple neural systems and subsystems. Thus, to what extent are the findings of a study reporting on a given construct (e.g., inhibitory control), confounded by another construct (e.g., monitoring or control strategy)?
To answer such a question, multidimensional approaches that concurrently measure and analyze two or more constructs of cognitive control, on the same participants, are needed. At the most basic level, such an approach would allow for isolating a given construct of interest by statistically controlling for variability in other measured constructs. However, perhaps of greater interest would be to take a latent profile approach, identifying what profiles of cognitive control are associated with behavioral inhibition, anxiety, or their interaction. While such methods will require considerably larger samples sizes, we believe such approaches will provide invaluable insight into the nature of behavioral inhibition and the etiology of anxiety. Ultimately, such insight could inform novel approaches to treating anxiety, or early intervention strategies for children identified with high levels of behavioral inhibition and control profiles that place them at heightened risk for developing anxiety problems.
Conclusions
In conclusion, studying cognitive control in relation to behavioral inhibition provides unique insights into both the phenotype of behavioral inhibition, as well as the later development of anxiety. However, critical insights are provided when cognitive control is separated into the subdomains of monitoring and control instantiation. In doing so, the literature appears to support the view that monitoring is not only directly related to behavioral inhibition but also interacts with behavioral inhibition to predict later development of anxiety. In contrast, control instantiation does not appear to directly relate to behavioral inhibition, though this construct does seem to interact with behavioral inhibition to predict the later development of anxiety. Nonetheless, the complete set of interrelations between behavioral inhibition, cognitive control, and anxiety are not fully understood. Future longitudinal research, employing both behavioral and cognitive neuroscience methods, will be needed to arrive at a more complete understanding of how behavioral inhibition relates to cognitive control and predicts risk for later anxiety.
Notes
- 1.
In this chapter, for simplicity, we treat monitoring as a singular construct. Indeed, while extensive research has investigated the multifaceted nature of control instantiation, little research has investigated parsing of monitoring along additional dimensions. Nonetheless, parsing monitoring into relevant sub-constructs may be meaningful and useful. One possibility is that the neurocognitive process of monitoring differs based on the type of task that is being monitored, or the type of goal that one is trying to achieve. Another possibility is that monitoring may meaningfully be defined in terms of its time course, that is, whether monitoring occurs before or after an event of interest, and the duration for which monitoring is sustained.
References
Aron, A. R. (2007). The neural basis of inhibition in cognitive control. The Neuroscientist, 13(3), 214–228. https://doi.org/10.1177/1073858407299288
Barker, T. V., Troller-Renfree, S., Pine, D. S., & Fox, N. A. (2015). Individual differences in social anxiety affect the salience of errors in social contexts. Cognitive, Affective, & Behavioral Neuroscience, 15(4), 723–735. https://doi.org/10.3758/s13415-015-0360-9
Bengson, J. J., Mangun, G. R., & Mazaheri, A. (2012). The neural markers of an imminent failure of response inhibition. NeuroImage, 59(2), 1534–1539.
Bokura, H., Yamaguchi, S., & Kobayashi, S. (2001). Electrophysiological correlates for response inhibition in a go/NoGo task. Clinical Neurophysiology, 112(12), 2224–2232.
Botvinick, M. M., Braver, T. S., Barch, D. M., Carter, C. S., & Cohen, J. D. (2001). Conflict monitoring and cognitive control. Psychological Review, 108(3), 624.
Braver, T. S. (2012). The variable nature of cognitive control: A dual mechanisms framework. Trends in Cognitive Sciences, 16(2), 106–113.
Braver, T. S., Reynolds, J. R., & Donaldson, D. I. (2003). Neural mechanisms of transient and sustained cognitive control during task switching. Neuron, 39(4), 713–726. https://doi.org/10.1016/S0896-6273(03)00466-5
Buzzell, G. A., Beatty, P. J., Paquette, N. A., Roberts, D. M., & McDonald, C. G. (2017). Error-induced blindness: Error detection leads to impaired sensory processing and lower accuracy at short response-stimulus intervals. Journal of Neuroscience, 37, 2895–2903.
Buzzell, G. A., Richards, J. E., White, L. K., Barker, T. V., Pine, D. S., & Fox, N. A. (2017). Development of the error-monitoring system from ages 9–35: Unique insight provided by MRI-constrained source localization of EEG. NeuroImage, 157, 13–26. https://doi.org/10.1016/j.neuroimage.2017.05.045
Buzzell, G. A., Roberts, D. M., Baldwin, C. L., & McDonald, C. G. (2013). An electrophysiological correlate of conflict processing in an auditory spatial Stroop task: The effect of individual differences in navigational style. International Journal of Psychophysiology, 90(2), 265–271. https://doi.org/10.1016/j.ijpsycho.2013.08.008
Buzzell, G. A., Roberts, D. M., Fedota, J. R., Thompson, J. C., Parasuraman, R., & McDonald, C. G. (2016). Uncertainty-dependent activity within the ventral striatum predicts task-related changes in response strategy. Cognitive, Affective, & Behavioral Neuroscience, 16(2), 219–233.
Buzzell, G. A., Troller-Renfree, S. V., Barker, T. V., Bowman, L. C., Chronis-Tuscano, A., Henderson, H. A., … Fox, N. A. (2017). A neurobehavioral mechanism linking behaviorally inhibited temperament and later adolescent social anxiety. Journal of the American Academy of Child & Adolescent Psychiatry, 56(12), 1097–1105. https://doi.org/10.1016/j.jaac.2017.10.007
Cavanagh, J. F., & Shackman, A. J. (2015). Frontal midline theta reflects anxiety and cognitive control: Meta-analytic evidence. Journal of Physiology - Paris, 109(1), 3–15.
Cavanagh, J. F., Zambrano-Vazquez, L., & Allen, J. J. (2012). Theta lingua franca: A common mid-frontal substrate for action monitoring processes. Psychophysiology, 49(2), 220–238.
Chronis-Tuscano, A., Degnan, K. A., Pine, D. S., Perez-Edgar, K., Henderson, H. A., Diaz, Y., … Fox, N. A. (2009). Stable early maternal report of behavioral inhibition predicts lifetime social anxiety disorder in adolescence. Journal of the American Academy of Child and Adolescent Psychiatry, 48(9), 928–935. https://doi.org/10.1097/CHI.0b013e3181ae09df
Clark, D. M., & Wells, A. (1995). A cognitive model of social phobia. Social Phobia: Diagnosis, Assessment, and Treatment, 41(68), 00022–00023.
Clauss, J. A., & Blackford, J. U. (2012). Behavioral inhibition and risk for developing social anxiety disorder: A meta-analytic study. Journal of the American Academy of Child and Adolescent Psychiatry, 51(10), 1066.e1–1075.e1. https://doi.org/10.1016/j.jaac.2012.08.002
Coplan, R. J., Rubin, K. H., Fox, N. A., Calkins, S. D., & Stewart, S. L. (1994). Being alone, playing alone, and acting alone: Distinguishing among reticence and passive and active solitude in young children. Child Development, 65(1), 129–137.
Corbetta, M., & Shulman, G. L. (2002). Control of goal-directed and stimulus-driven attention in the brain. Nature Reviews. Neuroscience, 3(3), 201.
Danielmeier, C., & Ullsperger, M. (2011). Post-error adjustments. Frontiers in Psychology, 2, 233.
Debener, S., Ullsperger, M., Siegel, M., Fiehler, K., Von Cramon, D. Y., & Engel, A. K. (2005). Trial-by-trial coupling of concurrent electroencephalogram and functional magnetic resonance imaging identifies the dynamics of performance monitoring. Journal of Neuroscience, 25(50), 11730–11737.
Degnan, K. A., Almas, A. N., Henderson, H. A., Hane, A. A., Walker, O. L., & Fox, N. A. (2014). Longitudinal trajectories of social reticence with unfamiliar peers across early childhood. Developmental Psychology, 50(10), 2311–2323. https://doi.org/10.1037/a0037751
der Borght, L. V., Schevernels, H., Burle, B., & Notebaert, W. (2016). Errors disrupt subsequent early attentional processes. PLoS One, 11(4), e0151843. https://doi.org/10.1371/journal.pone.0151843
Eysenck, M. W., Derakshan, N., Santos, R., & Calvo, M. G. (2007). Anxiety and cognitive performance: Attentional control theory. Emotion, 7(2), 336.
Fox, N. A., Henderson, H. A., Marshall, P. J., Nichols, K. E., & Ghera, M. M. (2005). Behavioral inhibition: Linking biology and behavior within a developmental framework. Annual Review of Psychology, 56, 235–262.
Fox, N. A., Henderson, H. A., Rubin, K. H., Calkins, S. D., & Schmidt, L. A. (2001). Continuity and discontinuity of behavioral inhibition and exuberance: Psychophysiological and behavioral influences across the first four years of life. Child Development, 72(1), 1–21.
Fox, N. A., Snidman, N., Haas, S. A., Degnan, K. A., & Kagan, J. (2015). The relations between reactivity at 4 months and behavioral inhibition in the second year: Replication across three independent samples. Infancy, 20(1), 98–114. https://doi.org/10.1111/infa.12063
Frenkel, T. I., Fox, N. A., Pine, D. S., Walker, O. L., Degnan, K. A., & Chronis-Tuscano, A. (2015). Early childhood behavioral inhibition, adult psychopathology and the buffering effects of adolescent social networks: A twenty-year prospective study. Journal of Child Psychology and Psychiatry, and Allied Disciplines, 56(10), 1065–1073. https://doi.org/10.1111/jcpp.12390
Gehring, W. J., Liu, Y., Orr, J. M., & Carp, J. (2012). The error-related negativity (ERN/ne). In S. J. Luck & E. S. Kappenman (Eds.), Oxford library of psychology. The Oxford handbook of event-related potential components (pp. 231–291). New York, NY: Oxford University Press.
Hajcak, G., Moser, J. S., Yeung, N., & Simons, R. F. (2005). On the ERN and the significance of errors. Psychophysiology, 42(2), 151–160.
Henderson, H. A., Pine, D. S., & Fox, N. A. (2015). Behavioral inhibition and developmental risk: A dual-processing perspective. Neuropsychopharmacology: Official Publication of the American College of Neuropsychopharmacology, 40(1), 207–224. https://doi.org/10.1038/npp.2014.189
Herrmann, M. J., Römmler, J., Ehlis, A.-C., Heidrich, A., & Fallgatter, A. J. (2004). Source localization (LORETA) of the error-related-negativity (ERN/ne) and positivity (Pe). Cognitive Brain Research, 20(2), 294–299.
Holroyd, C. B., & Coles, M. G. H. (2002). The neural basis of human error processing: Reinforcement learning, dopamine, and the error-related negativity. Psychological Review, 109(4), 679–709. https://doi.org/10.1037/0033-295X.109.4.679
Jarcho, J. M., Fox, N. A., Pine, D. S., Etkin, A., Leibenluft, E., Shechner, T., & Ernst, M. (2013). The neural correlates of emotion-based cognitive control in adults with early childhood behavioral inhibition. Biological Psychology, 92(2), 306–314. https://doi.org/10.1016/j.biopsycho.2012.09.008
Jarcho, J. M., Fox, N. A., Pine, D. S., Leibenluft, E., Shechner, T., Degnan, K. A., … Ernst, M. (2014). Enduring influence of early temperament on neural mechanisms mediating attention–emotion conflict in adults. Depression and Anxiety, 31(1), 53–62. https://doi.org/10.1002/da.22140
Kagan, J., Reznick, J. S., Clarke, C., Snidman, N., & Garcia-Coll, C. (1984). Behavioral inhibition to the unfamiliar. Child Development, 55(6), 2212–2225. https://doi.org/10.2307/1129793
Kagan, J., Reznick, S., & Snidman, N. (1988). Biological bases of childhood shyness. Science, 240(4849), 167.
Kagan, J., & Snidman, N. (1991). Infant predictors of inhibited and uninhibited profiles. Psychological Science, 2(1), 40–44.
Kagan, J., & Snidman, N. (2004). The long shadow of temperament. Cambridge, MA: Harvard University Press.
Kertz, S. J., Belden, A. C., Tillman, R., & Luby, J. (2015). Cognitive control deficits in shifting and inhibition in preschool age children are associated with increased depression and anxiety over 7.5 years of development. Journal of Abnormal Child Psychology. https://doi.org/10.1007/s10802-015-0101-0
Lahat, A., Lamm, C., Chronis-Tuscano, A., Pine, D. S., Henderson, H. A., & Fox, N. A. (2014). Early behavioral inhibition and increased error monitoring predict later social phobia symptoms in childhood. Journal of the American Academy of Child and Adolescent Psychiatry, 53(4), 447–455. https://doi.org/10.1016/j.jaac.2013.12.019
Lahat, A., Walker, O. L., Lamm, C., Degnan, K. A., Henderson, H. A., & Fox, N. A. (2014). Cognitive conflict links behavioral inhibition and social problem solving during social exclusion in childhood. Infant and Child Development, 23(3), 273–282. https://doi.org/10.1002/icd.1845
Lamm, C., Walker, O. L., Degnan, K. A., Henderson, H. A., Pine, D. S., McDermott, J. M., & Fox, N. A. (2014). Cognitive control moderates early childhood temperament in predicting social behavior in seven year old children: An ERP study. Developmental Science, 17(5), 667–681. https://doi.org/10.1111/desc.12158
Lengua, L. J. (2003). Associations among emotionality, self-regulation, adjustment problems, and positive adjustment in middle childhood. Journal of Applied Developmental Psychology, 24(5), 595–618. https://doi.org/10.1016/j.appdev.2003.08.002
Masaki, H., Maruo, Y., Meyer, A., & Hajcak, G. (2017). Neural correlates of choking under pressure: Athletes high in sports anxiety monitor errors more when performance is being evaluated. Developmental Neuropsychology, 42(2), 104–112. https://doi.org/10.1080/87565641.2016.1274314
McDermott, J. M., Perez-Edgar, K., Henderson, H. A., Chronis-Tuscano, A., Pine, D. S., & Fox, N. A. (2009). A history of childhood behavioral inhibition and enhanced response monitoring in adolescence are linked to clinical anxiety. Biological Psychiatry, 65(5), 445–448.
Meyer, A. (2017). A biomarker of anxiety in children and adolescents: A review focusing on the error-related negativity (ERN) and anxiety across development. Developmental Cognitive Neuroscience, 27(Supplement C), 58–68. https://doi.org/10.1016/j.dcn.2017.08.001
Moran, T. P., Bernat, E. M., Aviyente, S., Schroder, H. S., & Moser, J. S. (2015). Sending mixed signals: Worry is associated with enhanced initial error processing but reduced call for subsequent cognitive control. Social Cognitive and Affective Neuroscience, 10(11), 1548–1556.
Moser, J. S., Moran, T. P., Schroder, H. S., Donnellan, M. B., & Yeung, N. (2013). On the relationship between anxiety and error monitoring: A meta-analysis and conceptual framework. Retrieved from https://books.google.com/books?hl=en&lr=&id=TIWMCgAAQBAJ&oi=fnd&pg=PA40&dq=moran+moser+anxiety+review+2013&ots=lI_94R2AFf&sig=AlE6Zh6X1CxwxYPqHjuAKi5W0A4
Nigg, J. T. (2017). Annual research review: On the relations among self-regulation, self-control, executive functioning, effortful control, cognitive control, impulsivity, risk-taking, and inhibition for developmental psychopathology. Journal of Child Psychology and Psychiatry, 58(4), 361–383.
Overbeek, T. J., Nieuwenhuis, S., & Ridderinkhof, K. R. (2005). Dissociable components of error processing: On the functional significance of the Pe Vis-à-Vis the ERN/ne. Journal of Psychophysiology, 19(4), 319–329.
Pérez-Edgar, K., Bar-Haim, Y., McDermott, J. M., Chronis-Tuscano, A., Pine, D. S., & Fox, N. A. (2010). Attention biases to threat and behavioral inhibition in early childhood shape adolescent social withdrawal. Emotion, 10(3), 349–357. https://doi.org/10.1037/a0018486
Petersen, S. E., & Posner, M. I. (2012). The attention system of the human brain: 20 years after. Annual Review of Neuroscience, 35(1), 73–89. https://doi.org/10.1146/annurev-neuro-062111-150525
Purcell, B. A., & Kiani, R. (2016). Neural mechanisms of post-error adjustments of decision policy in parietal cortex. Neuron, 89(3), 658–671. https://doi.org/10.1016/j.neuron.2015.12.027
Rapee, R. M., & Heimberg, R. G. (1997). A cognitive-behavioral model of anxiety in social phobia. Behaviour Research and Therapy, 35(8), 741–756. https://doi.org/10.1016/S0005-7967(97)00022-3
Ridderinkhof, K. R., Ullsperger, M., Crone, E. A., & Nieuwenhuis, S. (2004). The role of the medial frontal cortex in cognitive control. Science, 306(5695), 443–447. https://doi.org/10.1126/science.1100301
Roberts, D. M., Fedota, J. R., Buzzell, G. A., Parasuraman, R., & McDonald, C. G. (2014). Prestimulus oscillations in the alpha band of the EEG are modulated by the difficulty of feature discrimination and predict activation of a sensory discrimination process. Journal of Cognitive Neuroscience, 26(8), 1615–1628. https://doi.org/10.1162/jocn_a_00569
Rothbart, M. K. (1981). Measurement of temperament in infancy. Child Development, 52, 569–578.
Rothbart, M. K., & Bates, J. E. (2006). Temperament. In N. Eisenberg (Ed.), Handbook of child psychology. New York, NY: Wiley Retrieved from http://onlinelibrary.wiley.com/doi/10.1002/9780470147658.chpsy0303/full
Schröger, E. (1993). Event-related potentials to auditory stimuli following transient shifts of spatial attention in a go/Nogo task. Biological Psychology, 36(3), 183–207. https://doi.org/10.1016/0301-0511(93)90017-3
Schwartz, C. E., Wright, C. I., Shin, L. M., Kagan, J., & Rauch, S. L. (2003). Inhibited and uninhibited infants “grown up”: Adult amygdalar response to novelty. Science, 300(5627), 1952–1953. https://doi.org/10.1126/science.1083703
Shenhav, A., Botvinick, M. M., & Cohen, J. D. (2013). The expected value of control: An integrative theory of anterior cingulate cortex function. Neuron, 79(2), 217–240. https://doi.org/10.1016/j.neuron.2013.07.007
Steinhauser, M., & Yeung, N. (2010). Decision processes in human performance monitoring. Journal of Neuroscience, 30(46), 15643–15653.
Thorell, L. B., Bohlin, G., & Rydell, A.-M. (2004). Two types of inhibitory control: Predictive relations to social functioning. International Journal of Behavioral Development, 28(3), 193–203. https://doi.org/10.1080/01650250344000389
Torpey, D. C., Hajcak, G., Kim, J., Kujawa, A. J., Dyson, M. W., Olino, T. M., & Klein, D. N. (2013). Error-related brain activity in young children: Associations with parental anxiety and child temperamental negative emotionality. Journal of Child Psychology and Psychiatry, 54(8), 854–862.
Troller-Renfree, S., Buzzell, G. A., Bowers, M., Salo, V., Forman-Alberti, A., Smith, E., … Fox, N. A. (2018). Development of inhibitory control during childhood and its relations to early temperament and later social anxiety. https://doi.org/10.31234/osf.io/tj4hn
Troller-Renfree, S. V., Buzzell, G. A., Pine, D. S., Henderson, H., & Fox, N. A. (in press). Developmental consequences of not planning ahead: reduced proactive control moderates longitudinal relations between behavioral inhibition and anxiety. Journal of the American Academy of Child & Adolescent Psychiatry.
Ullsperger, M., Danielmeier, C., & Jocham, G. (2014). Neurophysiology of performance monitoring and adaptive behavior. Physiological Reviews, 94(1), 35–79. https://doi.org/10.1152/physrev.00041.2012
White, L. K., McDermott, J. M., Degnan, K. A., Henderson, H. A., & Fox, N. A. (2011). Behavioral inhibition and anxiety: The moderating roles of inhibitory control and attention shifting. Journal of Abnormal Child Psychology, 39(5), 735–747.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2018 Springer Nature Switzerland AG
About this chapter

Cite this chapter
Buzzell, G.A., Troller-Renfree, S.V., Morales, S., Fox, N.A. (2018). Relations between Behavioral Inhibition, Cognitive Control, and Anxiety: Novel Insights Provided by Parsing Subdomains of Cognitive Control. In: Pérez-Edgar, K., Fox, N. (eds) Behavioral Inhibition. Springer, Cham. https://doi.org/10.1007/978-3-319-98077-5_10
Download citation
DOI: https://doi.org/10.1007/978-3-319-98077-5_10
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-98076-8
Online ISBN: 978-3-319-98077-5
eBook Packages: Behavioral Science and PsychologyBehavioral Science and Psychology (R0)