
Abstract
Gas exchange is the primary function of the lung. The basic process is the transfer of oxygen (O2) from the inspired air to the bloodstream and the transport of carbon dioxide (CO2) produced by metabolism out of the body via the expired gas. The three main structural considerations at play to facilitate this function are (1) the system of airways and the mechanical actions of the chest wall and respiratory muscles to move gas in and out of the lung; (2) the provision of a blood-gas interface which is very thin and has a very large surface area to promote the passive flow of O2 and CO2, driven only by partial pressure differences between alveolar gas and pulmonary capillary blood; and (3) the provision of a pulmonary vasculature sufficient both to perfuse the very large surface area of the blood-gas interface and to accommodate the full cardiac output with relatively low resistance.
Gas exchange also occurs in the tissues throughout the body by passive transfer. Oxygen is transported to tissues by passive transfer from arterial blood, and CO2 is transported from tissues to venous blood by passive transfer to venous blood. The main transport mechanism for O2 in the blood is by binding of O2 with hemoglobin (Hb) in the red blood cells. There is minimal O2 dissolved in plasma. The three mechanisms for transport of CO2 in the blood are (1) dissolving in plasma, (2) forming dissociated bicarbonate ions (HCO3−), and (3) binding with Hb.
Several factors affect gas exchange including the rates of lung ventilation and perfusion, the matching of ventilation to perfusion within the lung, Hb levels, alveolar O2 partial pressure, metabolic demand, exercise, and pathological changes.
The most common tests for assessing gas exchange are the single-breath uptake of carbon monoxide (CO) by the lung (called DLCO or diffusing capacity in North America and called TLCO or transfer factor in Europe), the analysis of arterial blood gases (ABG), and the measurement of oxygen saturation of Hb using pulse oximetry (SpO2). These measurements are very useful in the diagnosis and management of various lung diseases.
This chapter will describe the pathways for gas exchange, factors affecting gas exchange, measurements of gas exchange, and the interpretation of such measurements.
Access provided by CONRICYT-eBooks. Download chapter PDF
Similar content being viewed by others


Keywords
5.1 Gas Phase Transport
The gas exchange pathway for a molecule of O2 is as follows (Fig. 5.1):
-
1.
Transport from the mouth through the airways of the lung to the alveoli by convective and diffusive gas flow and mixing
-
2.
Diffusion across the surfactant layer and the type 1 pneumocytes which form the alveolar wall
-
3.
Diffusion through the interstitium between the alveolar wall and the capillary wall
-
4.
Diffusion across the pulmonary capillary endothelium
-
5.
Diffusion through the plasma to the red blood cell
-
6.
Diffusion across the red blood cell membrane
-
7.
Diffusion through the red blood cell cytoplasm to the Hb molecule
-
8.
Binding with a Hb molecule
-
9.
Transport via the circulatory system to the rest of the body

Gas transport from alveolar gas to Hb molecule
This section describes the portion of the gas exchange process which occurs in the gas phase from the mouth to the blood-gas barrier.
The gas exchange pathway for O2 begins with the inspiration of air at the mouth. In order for the O2 to reach the alveolar space, it must traverse 18–24 generations of bifurcation in the bronchial tree. With each successive airway generation, the total surface area of the airways increases, and hence the velocity of the inhaled gas is reduced, so that the total amount of airflow remains constant. This affects the manner in which O2 is transported.
There are two main transport mechanisms in the gas phase – convection and diffusion. Convection refers to the bulk flow of gas driven by gas pressure. Diffusion refers to the movement of individual molecules driven by a partial pressure gradient for that molecule. In the large airways, gas transport is primarily by convection. As the gas moves deeper into the bronchial tree, diffusive transport becomes more and more important. At the level of the peripheral airways, gas transport is primarily by diffusion. Gas mixing at the interface between the inspired gas and the residual gas remaining in the lung at end exhalation occurs by both convection and diffusion as it moves through the airways. It should also be noted that the pores of Kohn and the canals of Lambert (connections between neighboring conducting airways and alveoli) are thought to provide pathways for collateral ventilation which improve gas mixing and transport between adjacent alveoli and adjacent acini.
The distribution of the inspired gas in the lung is not homogeneous. Consider a maximal single-breath maneuver from residual volume (RV) to total lung capacity (TLC) in a subject seated upright. At RV, the alveoli at the base of the lung will have a smaller volume than alveoli at the apex due to the effect of gravity on the lung as it is suspended within the thoracic cavity. The weight of the lung tends to pull the apical regions open and squeeze the basal regions closed. This effect increases as the lung becomes less elastic with age or disease processes. At the end of inhalation, all alveoli tend to be filled to the same volume so that proportionally more inspired gas goes to the basal regions, and they will have a higher O2 concentration.
In young, healthy subjects, the distribution of ventilation tends to approach uniformity. As the normal lung ages, the distribution of ventilation becomes less uniform, due mainly to the loss of elastic recoil. In people with lung diseases that cause airflow obstruction and/or loss of elastic recoil, the heterogeneity of ventilation can increase markedly. In such cases, the transport of inspired gas to the blood-gas barrier can become a consequential impediment to gas exchange.
The blood-gas barrier is the endpoint of gas phase transport. The blood-gas barrier is formed by the alveolar wall composed of type 1 pneumocytes covered by a film of surfactant, the interstitium (which may be a potential space or may contain interstitial fluid), and the endothelium of the capillaries (Fig. 5.1). There are 200–800 million alveoli in adult humans, depending on the size of their lungs. The blood-gas barrier has been estimated to have an area in the order of 100 m2 at TLC in a typical adult and a thickness that varies from 200 to 2000 nm. Fick’s law states that the mass transfer of a gas across a membrane driven by the partial pressure difference (P2 − P1) is directly proportional to its surface area (A) and inversely proportional to its thickness (T). Hence, the large area and small thickness of the blood-gas barrier are critically important for gas exchange. The other term in Fick’s law is the diffusivity (D) of the gas molecule, which is equal to its solubility divided by the square root of its molecular weight.
The alveolar blood-gas barrier is not analogous to a balloon which expands and contracts with inhalation and exhalation, surrounded by a sheet of blood. In such a model, the area for gas exchange would decrease during exhalation proportional to volume to the two-thirds power and the thickness of the membrane through which gas must diffuse would increase. In reality, there are several mechanisms to maintain the effective surface area for gas exchange at lower lung volumes. As the alveolus contracts and expands, there is folding and unfolding of the alveolar wall between the pulmonary capillaries. There is also a bulging of the pulmonary capillaries into the alveoli. Furthermore, there are openings in the alveolar walls (the pores of Kohn), which open as the alveolus expands with inhalation and close during exhalation. These mechanisms help to maintain the surface area available for diffusion across the blood-gas barrier at lower lung volumes, but there remains a decrease in the effective surface area as lung volume decreases. However, the decrease in diffusion at lower lung volumes is less than would be predicted by the balloon model.
Once a gas molecule has crossed the blood-gas barrier, it enters the pulmonary capillaries. The pulmonary capillary blood volume varies with height and sex. It is ~90 mL for an average adult male and ~65 mL for an average adult female.
5.2 Blood Phase Transport
5.2.1 The Pulmonary Circulation
Virtually the entire cardiac output is delivered by the right ventricle into the pulmonary vascular bed, which consists of a branching pulmonary arterial system, a pulmonary capillary bed, and a pulmonary venous system draining into the left atrium. Within the pulmonary arterial system, mean pressure is roughly 14 mmHg and mean pulmonary vascular resistance is 1.43 mmHg/L/min. During exercise, the mean pressure increases to 20 mmHg and the resistance falls to 0.62 mmHg/L/min.
The distribution of blood flow through this system is affected by gravitational forces (dependent regions receive more regional blood flow). This has been described by the West three-zone model: zone 1 at the top of the lung where alveolar pressures exceed vascular pressures, zone 2 in the middle of the lung where pulmonary arterial pressure (but not venous pressure) exceeds alveolar pressure, and zone 3 where vascular pressures exceed alveolar pressures. Smooth muscle tone, largely driven by oxygen tension (hypoxia promotes vascular constriction), also affects distribution of blood flow.
The state of inflation also affects vascular resistances and blood flow distribution. Specifically, as inflation increases, peri-alveolar vessels are compressed and extra-alveolar vessels are stretched open. This results in less blood flow/alveolus in nondependent regions and more blood flow/alveolus to dependent regions as the lung inflates. The net effect of these changes is that pulmonary vascular resistance is at its minimum near functional residual capacity, rising as the lung approaches either residual volume or total lung capacity.
As noted above, the pulmonary capillary bed contains approximately 65–90 mL of blood, and the alveolar-capillary surface area approaches 100 m2. Oxygen diffusion is driven by an alveolar-capillary O2 gradient of 60 mmHg (alveolar PAO2 of 100 mmHg minus mixed venous \( \mathrm{P}\overline{\mathrm{v}}{\mathrm{O}}_2 \) of 40 mmHg) and is virtually complete within 0.25 s, only a fraction of the estimated red blood cell transit time at rest of 0.75–2.5 s. CO2 diffusion is completed even faster, approximately 20× that of oxygen.
Generally, pulmonary capillary blood leaving each alveolus has about the same PO2 and PCO2 as the alveolar gas. However, the ultimate arterial PaO2 (and to a lesser extent PaCO2) depends upon the relationship of ventilation to perfusion (V̇A/Q̇) in each alveolar-capillary gas exchange unit and the distribution of these relationships. Indeed, in disease states with wide distributions of regional V̇A/Q̇, profound arterial hypoxemia can develop despite overall normal ventilation and perfusion (see V̇A/Q̇ discussion below). Note that even in normal lungs, the ultimate PaO2 in arterial blood is slightly lower than mean alveolar PAO2 because local matching of ventilation and perfusion in normal lungs is imperfect. In addition, a small amount of unoxygenated blood is added to pulmonary capillary blood through anatomic shunts connecting the venous bronchial circulation to the pulmonary venous blood.
5.2.2 Hemoglobin
Oxygen is carried in the blood in two forms: (1) combined with hemoglobin and (2) dissolved O2 in the plasma. Human hemoglobin (Hb) is a tetramer (four polypeptides) consisting of two α-polypeptides and two β-polypeptides, each containing a heme moiety. The tetramer consists of 547 amino acids and has a molecular weight of 64,800 daltons. The heme and globin interact with each other in a way that determines the O2-binding characteristics of hemoglobin.
Hb allows blood to carry much more oxygen than would be possible from simply dissolving oxygen in plasma. For example, 15 gm Hb in 100 mL of blood with a PO2 of 100 mmHg carries 20 mL of oxygen in contrast to 0.3 mL of oxygen dissolved in 100 mL of plasma with a PO2 of 100 mmHg. Oxygen does not oxidize hemoglobin; rather, it oxygenates hemoglobin, a reversible process. Combined with oxygen, hemoglobin is called oxyhemoglobin, whereas unoxygenated hemoglobin is called deoxyhemoglobin or reduced hemoglobin.
As oxygen molecules successively bind with heme groups, the hemoglobin molecule physically changes its shape, causing it to reflect and absorb light differently when it is oxygenated than when it is deoxygenated. This phenomenon is responsible for the bright red color of oxygenated hemoglobin and the deep purple color of deoxyhemoglobin. This difference in light absorption and reflection makes it possible to measure the amount of oxygenated hemoglobin present (see Sect. 5.7).
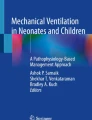
O2 affinity to hemoglobin increases during progressive oxygenation, a phenomenon called cooperativity. The cooperativity is responsible for the sigmoid shape of the oxyhemoglobin equilibrium curve (OEC), which affects how O2 is loaded and unloaded under physiologic conditions (Fig. 5.2). Its position often is expressed by the P50, or the PO2 that corresponds with 50% hemoglobin saturation. The normal P50 for human hemoglobin is approximately 27 mmHg. When the O2 affinity increases, the OEC shifts to the left (reduced P50). When the O2 affinity decreases, the OEC shifts to the right (increased P50).

Oxyhemoglobin equilibrium curve (OEC), which reflects Hb saturation as a function of PaO2. The green curve represents the normal position, where hemoglobin is 50% saturated at a PO2 of 27 mmHg. Factors that shift the curve to the left (blue curve) and to the right (red curve) are shown and discussed in the text
Several factors affect hemoglobin’s affinity for O2, resulting in either a left (increased affinity) or right (decreased affinity) shift in the OEC position, changing the hemoglobin O2 saturation for a given PaO2. Increased 2,3-diglycerophosphate (2,3-DPG) in the erythrocyte, acidemia, increased PaCO2, and hyperthermia decrease hemoglobin affinity for O2 (right shift of the curve). In contrast, decreased 2,3-DPG, alkalemia, decreased PaCO2, and hypothermia increase hemoglobin affinity for O2 (left shift of the curve).
When hemoglobin is bound to carbon monoxide (CO), its affinity for O2 is greatly increased; the binding of CO to one heme site increases O2 affinity of the other binding sites, causing a leftward shift of the OEC. This effect on hemoglobin O2 affinity explains why the formation of 50% carboxyhemoglobin causes more severe tissue hypoxia than when various forms of anemia cause the reduction of hemoglobin concentration to half the normal concentration.
The hemoglobin molecule simultaneously carries O2 and CO2, but not at the same binding sites. Oxygen combines with the molecule’s heme groups, whereas CO2 combines with the amino groups of the α- and β-polypeptide chains. The presence of O2 on the heme portions of hemoglobin hinders the combination of amino groups with CO2 (i.e., it hinders formation of carbaminohemoglobin); thus, the affinity of hemoglobin for CO2 is greater when it is not combined with oxygen (Haldane effect). Conversely, carbaminohemoglobin has a decreased affinity for O2 (Bohr effect). Thus, oxygenated blood carries less CO2 for a given PaCO2 than deoxygenated blood. It should be appreciated that the Haldane and Bohr effects are mutually enhancing. As O2 diffuses into the tissue cells, it dissociates from the hemoglobin molecule, enhancing its ability to carry CO2 (Haldane effect). At the same time, CO2 diffusion into the blood at the tissue level decreases hemoglobin’s affinity for O2 (Bohr effect), enhancing the release of O2 to the tissues.
5.3 Ventilation/Perfusion Matching
As noted above, alveolar gas and capillary blood rapidly equilibrate across the alveolar-capillary interface such that the blood exiting the pulmonary capillary will equal the alveolar gas PAO2 and PACO2. However, the ultimate arterial PaO2 and PaCO2 will depend on the distribution of ventilation/perfusion (V̇A/Q̇) relationships throughout the lungs and the FIO2 (Fig. 5.3). In units where ventilation with respect to perfusion is low, alveolar and capillary blood PO2 and PCO2 approach the mixed venous \( \mathrm{P}\overline{\mathrm{v}}{\mathrm{O}}_2 \) and \( \mathrm{P}\overline{\mathrm{v}}{\mathrm{CO}}_2 \). In contrast, in units where ventilation with respect to perfusion is high, the alveolar and capillary blood PO2 and PCO2 approach the inspired PIO2 and PICO2. At the extremes, shunts (V̇A/Q̇ = 0) and dead space (V̇A/Q̇ = infinity) do not participate in gas exchange but only serve to put mixed venous blood into arterial blood and inspired gas into expired gas, respectively.

Effect of ventilation/perfusion ratio on gas exchange. Notice how a V̇A/Q̇ ratio less than 1 results in a sharp fall in PAO2 but only a slight rise in PACO2, whereas a V̇A/Q̇ ratio greater than 1 results in a rise in PAO2 and a fall in PACO2. Pv–O2 and Pv–CO2 represent mixed venous gas values, and PIO2 and PICO2 represent inspired gas values. (Reproduced with permission of the © ERS 2018: European Respiratory Journal. Oct 2014; 44(4):1023–1041. https://doi.org/10.1183/09031936.00037014)
Note from Fig. 5.3 that at sea level with a PIO2 of 150 mmHg, a PICO2 of 0 mmHg, a \( \mathrm{P}\overline{\mathrm{v}}{\mathrm{O}}_2 \) of 40 mmHg, and a \( \mathrm{P}\overline{\mathrm{v}}{\mathrm{CO}}_2 \) of 45 mmHg, a V̇A/Q̇ of 1 results in a PaO2 of 80–100 mmHg, which fully saturates Hb. This is what occurs in the vast majority of normal alveolar-capillary units and results in a PaCO2 of 40 mmHg. In disease states producing large numbers of both low and high V̇A/Q̇ units (<1 and >1, respectively), high V̇A/Q̇ units can compensate for low V̇A/Q̇ units in removing CO2 and keep the PaCO2 near 40 mmHg. However, once pulmonary capillary hemoglobin is fully saturated with oxygen, the higher PaO2 in high V̇A/Q̇ units results in only a small increase in dissolved oxygen. A high V̇A/Q̇ unit can therefore not compensate for a low V̇A/Q̇ unit for oxygenation. The presence of large numbers of low V̇A/Q̇ units in disease thus has far more effects on oxygenation than carbon dioxide removal and, along with shunts (V̇A/Q̇ = 0), is the major cause of abnormal alveolar-arterial oxygen differences (\( {\mathrm{P}}_{\left(\mathrm{A}-\mathrm{a}\right){\mathrm{O}}_2} \)).
It has long been recognized that the normal lung has a distribution of V̇A/Q̇ units around one. This distribution is relatively tight in normal subjects, and the differences that do exist are explained by the greater effects of gravity on the vertical distribution of perfusion than on ventilation and the non-gravity dependent heterogeneity in ventilation and perfusion due to the structural asymmetry in the airways and blood vessels. As a consequence only a small alveolar-arterial difference (\( {\mathrm{P}}_{\left(\mathrm{A}-\mathrm{a}\right)\mathrm{O}2} \)) exists in normal subjects.
Vascular smooth muscle modulation is an important mechanism to assist in matching perfusion to ventilation. This is largely controlled by oxygen and is a locally mediated response of the pulmonary vasculature to the decrease in PAO2, which occurs when ventilation to the alveolar unit is reduced. This local hypoxic vasoconstriction serves to reroute blood flow to better-ventilated units.
Various models have been proposed to explain the effects of V̇A/Q̇ distributions in the lung. One of the most sophisticated is the multiple inert gas elimination technique (MIGET). Please see the Appendix for further details.
5.4 Diffusing Capacity (Transfer Factor) of the Lung for Carbon Monoxide
While it would be preferable to have a test that directly measures the conductance of O2 from inspired gas to binding with Hb, the nature of normal respiration precludes such a measurement using noninvasive techniques. Passive diffusion is driven by the difference in O2 partial pressure (PO2) across the blood-gas barrier. Consequently, in order to quantify the rate of O2 diffusion, measurements of the alveolar and pulmonary capillary PO2 would be required. While estimates of mean PAO2 might be made, the pulmonary capillary PO2 will vary between the \( \mathrm{P}\overline{\mathrm{v}}{\mathrm{O}}_2 \) and PaO2 during the course of blood flow through the pulmonary capillary bed.
In 1915, Marie Krogh published a method to estimate the conductance of gases across the blood-gas barrier using a very low concentration of CO as a proxy for O2. The transport of a CO molecule is very similar to that of an O2 molecule. The molecular weight and the solubility of CO are both a little lower than that of O2, with the net result that Fick’s law predicts CO transport across a membrane will be about 83% of O2 transport at the same driving pressure. Krogh’s method is based on the assumption that any CO molecule that diffuses across the blood-gas barrier is immediately tightly bound by Hb and consequently the pulmonary capillary PCO can be assumed to be zero. Hence, the driving pressure for CO is simply PACO which can be estimated knowing the CO concentration and volume of the inspired gas and the alveolar volume. The conductance of CO can then be calculated by measuring the uptake of CO over a given interval of breath-holding at TLC and dividing by the driving pressure and breath-hold time. Because the concentration of CO decreases as CO diffuses across the blood-gas barrier, the decay in PACO will be exponential, which precludes the use of a simple arithmetic calculation of diffusive flow. In the Krogh equation, an exponential diffusion constant was introduced which has since been modified and named the diffusing capacity of the lung for carbon monoxide (DLCO).
The Krogh equation is applied as follows:
where VA is the alveolar volume; FACOt0 and FACOt1 are the fractional alveolar gas concentrations of CO at time t0 and time t1, respectively; t0 is the time at the beginning of the measurement interval and t1 is the time at the end of the interval; PB is the ambient barometric pressure; and 47 mmHg is the partial pressure of water vapor at body temperature.
Diffusing capacity is an unfortunate term since, as we will see, the process includes more than diffusion and it is not a true capacity in the usual pulmonary function use of the term. Outside of North America, the measurement is more appropriately called transfer factor (TLCO).
An important step in translating Krogh’s experimental technique to a pulmonary function test was the single-breath maneuver developed by Forster and Ogilvie who introduced the use of helium as a tracer gas to permit the measurement of both VA and FACOt0. The single-breath maneuver consisted of exhalation to residual volume (RV), rapid inhalation of test gas to TLC, breath-holding at TLC for 10 s, and rapid exhalation back to RV. A sample of alveolar gas was collected during exhalation after discarding a given volume of gas for dead space washout. The Krogh equation is only applicable at a constant lung volume so rapid inhalation and exhalation were used to approximate a pure breath-hold maneuver. The test gas consisted of 0.3% CO, 10% He, 21% O2, and balance N2.
Helium was initially chosen as a tracer gas because it is biologically inert and has a very low solubility so that it can be safely assumed that all of the helium remains in the lung with no diffusion. As such, the alveolar He concentration at the end of the inhalation of test gas will remain constant for the duration of breath-holding and exhalation. This concentration is used to estimate the alveolar CO concentration at the beginning of breath-holding by assuming that during a rapid inhalation, the tracer gas (Tr) and CO will be diluted by the same fraction:
where FICO and FITr are the fractional concentrations of CO and Tr in the inhaled test gas, respectively. Because the alveolar concentration of Tr remains constant, FATrt0 is the same as the concentration of Tr in the exhaled gas sample, FsTr. Thus
Using this relationship, the Krogh equation becomes
where tBH is the breath-hold time and FsCO is the CO concentration in the exhaled gas sample.
Conventional DLCO systems use a simplified mass balance equation to calculate alveolar volume, which assumes that the lung ventilation is homogeneous and there is continuous, complete gas mixing in the alveolar space with no mixing of the dead space. In such a model, the volume of Tr inhaled into the alveolar space is FITr ∙ (VI − Vd) where VI is the inhaled volume of test gas and Vd is the dead space. The concentration of Tr in the alveolar space at end inhalation (which will be the same as FsTr) will then be the volume of Tr inhaled divided by the alveolar volume:
However, lung ventilation becomes progressively more heterogeneous in normal adults as age increases and to a greater degree in patients with obstructive lung diseases. In the 2017 ERS/ATS DLCO standards, a more accurate calculation of alveolar volume is recommended for DLCO systems with rapidly responding gas analyzers which measure all of the tracer gas inhaled and all of the tracer gas exhaled to determine how much tracer gas is left in the lung at end exhalation and use the measured tracer gas concentration at end exhalation to determine the end-expiratory alveolar volume.
Many current systems use 0.3% methane (CH4) as a tracer gas. Although it is not as insoluble or inert as helium, it has been shown to be acceptable for use as a tracer gas for measurement of DLCO. One of the reasons for using CH4 is that it can be measured using the same nondispersive, infrared gas analyzer technology that is used for measuring CO concentration.
In traditional units, DLCO is measured in mL/min/mmHg. As in other lung volume measurements, alveolar volume is reported under body temperature, saturated with water vapor (BTPS) conditions. While reporting in BTPS units is necessary for measures of lung volumes and flows, because they reflect the actual heated and humidified volumes that occur in the lung, this is not the case for gas exchange variables. In considering gas exchange, it is the number of moles of gas that are available for metabolism that is important rather than the amount of space that the gas takes up in the lung. For this reason, the DLCO calculated using VA in BTPS must be converted to standard temperature, pressure, and dry gas conditions (STPD). When using traditional units, the conversion factor from BTPS to STPD is 273/310 ∙ (PB − 47)/PB ∙ PB/760 or (PB − 47)/863. Outside of North America, DLCO (or TLCO) is reported in SI units which are mmol/min/kPa. To convert DLCO in SI units to traditional units, multiply by 2.987.
5.5 Interpretation of DLCO
Before interpreting a DLCO result, a number of non-disease factors that affect CO uptake need to be considered. Besides varying with age, sex, height, and possibly ethnicity, DLCO also changes with Hb, COHb, lung volume, PIO2, barometric pressure, and ventilation distribution. Because predicted DLCO values are derived from measurements in normal subjects who are disease-free, have normal Hb, have minimal COHb, are breathing room air, and have normal lung volumes and uniform ventilation distribution, allowances for all of these must be incorporated into an interpretation of a result.
5.5.1 Factors Affecting the Measurement of DLCO
-
(a)
Pulmonary capillary blood volume and Hb level: As noted above, gas exchange involves more than the diffusion of gas across the blood-gas barrier. Once a CO molecule has entered the plasma, it must diffuse into a red blood cell and bind with Hb. Roughton and Forster showed that the conductance of CO uptake is equal to the transmembrane conductance (Dm) plus the intra-blood conductance, with both steps of roughly equal importance. The latter term is the product of the reaction rate of CO with oxyhemoglobin (θ) and the volume of blood in the alveolar capillaries (Vc). Knowing that conductances in series add like resistances in parallel, the relationship is:
This relationship shows that DLCO will increase as pulmonary capillary blood volume increases. Furthermore, the reaction rate of CO with Hb is dependent on the Hb concentration in the blood such that θ will increase as Hb concentration increases.
where Hbref is the reference Hb concentration for the subject. While the common values for Hbref are 13.4 g/L for females and males <15 years old and 14.6 g/L for males >15 years old, studies have found that Hb concentrations in the normal population vary considerably with age and ethnicity as well as gender. A change of 10% in Hb concentration will result in a 4.4% change in DLCO. Anemia reduces DLCO, while polycythemia increases DLCO. Data from NHANES III provide a source of reference values for Hb levels in different age groups and ethnicities.
Pulmonary blood capillary volume will increase with increased cardiac output (e.g., exercise), a Müller maneuver, and the supine position among other mechanisms. A Valsalva maneuver can decrease pulmonary capillary blood volume. Note that the blood volume must be considered independently of blood flow. Static blood in the lung will also increase DLCO.
-
(b)
Carboxyhemoglobin : The partial pressure of CO in the pulmonary capillaries is not zero. Although CO is bound very tightly to Hb to form carboxyhemoglobin (COHb), because the pulmonary capillary PO2 is much higher than PCO (due to the very low concentration of CO present), some of the CO will be displaced from the COHb by the O2 and thus present a partial pressure of CO in the capillaries that will act as a back pressure, countering the PACO driving pressure. Furthermore, there is a very small amount of CO produced endogenously in the body. Other environmental sources of CO will contribute to higher levels of COHb. Smokers typically have 5–15% COHb depending on the amount of smoking. (Note that subjects are advised not smoke on the day of the DLCO test.) Outdoor and indoor air pollution, occupational exposures, and faulty heating or cooking appliances can all lead to increased COHb levels. Since CO is used in the test gas, repeated measurements of DLCO will also raise COHb levels. The inhalation of 0.3% CO in the single-breath maneuver typically causes COHb to increase by 0.6–0.7% for each maneuver.
The presence of COHb compromises the assumption that the CO driving pressure across the blood-gas barrier is simply the PACO and causes DLCO to be underestimated by about 1% for each 1% increase in COHb concentration. DLCO systems with rapid gas analyzers meeting the 2017 ERS/ATS standards can measure the CO concentration in the alveolar gas exhaled just prior to the inhalation of test gas in order to estimate the back pressure of CO in the pulmonary capillaries, which can then be used in the calculation of DLCO to offset the CO back pressure.
COHb has an additional effect on DLCO. The COHb in the pulmonary capillaries prior to testing is not available for binding leaving a reduced amount of Hb for further CO uptake. This so-called anemia effect will reduce DLCO measurements, but DLCO can be compensated for this effect using the CO back pressure measurement and equations provided in the 2017 ERS/ATS DLCO technical standards.
-
(c)
Alveolar O2 partial pressure : The reaction rate of CO with Hb is dependent on the PAO2. The affinity of Hb for CO is about 230 times the affinity of Hb for O2, and the competition for Hb-binding sites swings even more in favor of CO as the PAO2 decreases with a consequential increase in DLCO. In normal subjects tested at a barometric pressure of 760 mmHg (sea level), PAO2 is typically 100 mmHg. When barometric pressure is reduced, either by the presence of an atmospheric low pressure cell or an increase in altitude, PAO2 decreases and DLCO will increase by about 0.53% for each 100 m of increase in altitude. Note that the 2017 reference values for DLCO provided by the Global Lung Function Initiative are corrected to 760 mmHg and the 2017 ERS/ATS standards recommend correcting DLCO measurements to 760 mmHg. If other reference values are used and the measured DLCO is corrected to 760 mmHg, then the reference values should also be corrected to 760 mmHg using the altitude of the center in which the reference values were obtained as a proxy for PB, using the formula provided in the 2017 ERS/ATS standards.
The subject should not breathe supplemental oxygen for at least 10 min prior to a DLCO maneuver. However, if PAO2 has to be increased during the DLCO test for patients requiring supplemental O2, the resulting DLCO measurement will be reduced, and an adjustment for the change in PAO2 will be required as described in the 2017 ERS/ATS DLCO technical standards.
-
(d)
Lung volumes : As the lung inflates, Dm increases (due to unfolding membranes and increasing surface area), while Vc effects are variable (due to differential stretching and flattening of alveolar and extra-alveolar capillaries). The net effect of these changes is that DLCO tends to increase as the lung inflates. However, the relationship between DLCO and lung volume is complex and certainly not 1:1 with DLCO changes substantially less than lung volume changes. Thus, in a normal subject with a reduced inspired volume, the ratio DLCO/VA will rise.
The ERS/ATS recommends using the inspired volume (VI) as an index of test quality (Grade A requires VI to be >90% of the vital capacity (VC) and Grade F would be a VI/VC < 85%). This is based on two rationales: (a) a small VA resulting from a suboptimal inspiration from RV will variably reduce DLCO as described above; (b) a reduced VI will reduce the alveolar PAO2 from what would be expected, and this can increase DLCO as described above.
-
(e)
Ventilation distribution : CO uptake will primarily reflect gas exchange in lung units which contribute most to inhalation and exhalation. This is particularly important in diseases such as emphysema, where the inhaled CO will preferentially go to the better-ventilated regions of the lung and the subsequently measured CO uptake will be determined mainly by uptake properties of those regions. Under these conditions, the tracer gas dilution used to calculate VA will also reflect mainly regional dilution and underestimate the lung volume as a whole (a low VA/TLC ratio (eg <0.75–0.85)) especially when a small alveolar gas sample is used. There are no good ways to adjust for this other than to comment that DLCO in the setting of a low VA/TLC ratio is reflecting mainly the CO uptake properties of the better-ventilated regions of the lung.
5.5.2 Interpreting the Results
Once the DLCO measurement has been determined to be accurate and the appropriate adjustments have been made, the results need to be assessed in relation to a reference value. Many reference sets have been reported over the years with age, gender, and height being the most common prediction parameters. Race/ethnicity is also likely important, but data on these are limited. Unfortunately, there is considerable disparity among these data sets, and recommendations have been made to use the reference equation that best fits a normal population in your laboratory. More recently, the Global Lung Function Initiative (GLI) has taken a large number of these data sets, and using complex statistical procedures has produced a single set of reference equations. This is likely to become a worldwide standard. An abnormal DLCO is a value below the lower limit of normal (LLN) of the reference equation. Severity of the abnormality can be addressed by either reporting a percent predicted value or a Z score based on the number of standard deviations that the observed DLCO is below the predicted value.
Interpretation of the DLCO should be guided by the concept that CO uptake is driven largely by alveolar-capillary interface surface properties (Dm, which is affected by area and, to a lesser extent, thickness) and alveolar-capillary blood volume (Vc). Diseases that reduce either Dm or Vc (or both) can thus be expected to reduce DLCO. In practice this means a variety of disease states including interstitial diseases, pulmonary vascular diseases, alveolar inflammatory diseases, chronic capillary hypertension from left heart failure, and emphysema all are associated with a low DLCO (Table 5.1). Progressive loss of DLCO in these diseases implies worsening of either Dm or Vc (or both). In normal subjects, maneuvers that decrease Vc (Valsalva maneuver, high vertical G-forces) will also decrease DLCO.
DLCO can be expressed as DLCO with respect to alveolar volume (essentially the rate of CO concentration change during the breath-hold, often expressed as KCO). This is commonly reported as DLCO/VA, but it is important to remember that this expression does not represent DLCO “corrected” for VA. Since predicted values for KCO were obtained in normal subjects with normal VA, using this predicted KCO to infer normality when the VA is low is misleading.
KCO, however, can help further characterize the processes underlying a low DLCO. A high KCO (actual/reference ratio>1) implies a preserved Dm and Vc in the face of a loss of lung volume. As noted above, this is what occurs with a suboptimal inspired volume. In practice, this may also reflect an inability to fully inspire due to chest wall abnormalities or neuromuscular issues. A large lobectomy or pneumonectomy may also produce a low DLCO with a high KCO because the remaining capillary bed volume is increased by increased perfusion. A low DLCO with a KCO near the reference value (actual/reference ratio near 1), as noted above, does NOT imply normal Dm and Vc properties in the lung. Instead it means that loss of Dm and/or Vc roughly parallels the loss of VA, a situation reflecting many parenchymal lung diseases. Finally a low DLCO with a low KCO (actual/reference ratio <1) usually suggests a loss of Vc out of proportion to any loss in VA as would occur in predominant pulmonary vascular disease (Table 5.1).
DLCO can also be elevated, usually by mechanisms that increase Vc. For example, increasing the perfusion pressure of the pulmonary circulation can increase DLCO substantially because higher perfusion pressure recruits and distends pulmonary capillaries (increasing Vc). Exercise, the supine position, and Müller maneuvers (inspiratory efforts against a closed glottis) can all recruit and dilate alveolar capillaries, thereby increasing Vc and DLCO. Finally, acute alveolar hemorrhage with its large volume of hemoglobin in the lungs has also been noted to increase DLCO. To differentiate a high DLCO from alveolar hemorrhage from a high DLCO due to increased Vc, one needs to inspect serial measurements of DLCO made during the DLCO maneuver. In alveolar hemorrhage, subsequent measurements of DLCO will decrease, while in increased Vc, subsequent measurements of DLCO will remain elevated.
5.6 Blood Gas Assessment
An important measure of pulmonary gas exchange is the amount of O2 and CO2 in the blood. An arterial blood sample, typically drawn from the radial artery, is analyzed to determine the partial pressures of O2 (PaO2) and CO2 (PaCO2) and the pH in blood leaving the lungs. Blood gases can also be analyzed in mixed venous blood. Details regarding the techniques for this measurement are available in the American Thoracic Society Pulmonary Function Laboratory Management and Procedure Manual.
5.6.1 Arterial and Venous PO2
Arterial and venous PO2 are the partial pressures of oxygen in arterial and mixed venous blood, respectively. In normal subjects at sea level, arterial PaO2 is 80–100 mmHg, enough to easily fully saturate normal Hb (Fig. 5.2). Arterial hypoxemia is generally defined by values less than this, and severe arterial hypoxemia is generally defined as less than 55 mmHg, levels resulting in pulmonary vasoconstriction and the potential to compromise tissue oxygen delivery (see below).
Arterial hypoxemia can be a consequence of a low inspired oxygen concentration, alveolar hypoventilation, or V̇A/Q̇ mismatching (including shunts). Diffusion impairments due to thickened membranes are generally not responsible for reduced arterial PaO2 at rest. During exercise, however, blood flow velocity in patients with thickened alveolar-capillary membranes may increase enough to prevent equilibration between alveolar gas and capillary blood during the short transit through the lung, causing arterial hypoxemia. Thus, exercise can unmask diffusion defects that are not apparent at rest. A falling PaO2 with exercise indicates that a diffusion defect may be an important contributing factor for hypoxemia.
The difference between alveolar and arterial PO2 \( \left({\mathrm{P}}_{\left(\mathrm{A}-\mathrm{a}\right){\mathrm{O}}_2}\right) \) can be used to separate these mechanisms (a widened gradient suggests V̇A/Q̇ mismatch and/or shunt). P(A − a)O2 is calculated as the difference between the PaO2 and the PaO2. PaO2 is computed from the alveolar gas equation:
where RQ is the respiratory quotient (V̇CO2/V̇O2). The \( {\mathrm{P}}_{\left(\mathrm{A}-\mathrm{a}\right){\mathrm{O}}_2} \) is more sensitive and specific than the arterial PaO2 alone as an indicator of V̇A/Q̇ abnormalities. The \( {\mathrm{P}}_{\left(\mathrm{A}-\mathrm{a}\right){\mathrm{O}}_2} \) in healthy adults breathing room air increases with age. As a general rule, the \( {\mathrm{P}}_{\left(\mathrm{A}-\mathrm{a}\right){\mathrm{O}}_2} \) for an individual should be no more than half the chronologic age and no more than 25 mmHg while breathing room air. Thus, the upper normal limit of \( {\mathrm{P}}_{\left(\mathrm{A}-\mathrm{a}\right){\mathrm{O}}_2} \) for a 30-year-old person is 15 mmHg, whereas the upper normal limit of \( {\mathrm{P}}_{\left(\mathrm{A}-\mathrm{a}\right){\mathrm{O}}_2} \) for a 60-year-old individual is 25 mmHg. The \( {\mathrm{P}}_{\left(\mathrm{A}-\mathrm{a}\right){\mathrm{O}}_2} \) in normal adults is the result of the combination of mild V̇A/Q̇ mismatch and a small anatomic right-to-left shunt. Each of these mechanisms is responsible for about half the total \( {\mathrm{P}}_{\left(\mathrm{A}-\mathrm{a}\right){\mathrm{O}}_2} \).
The \( {\mathrm{P}}_{\left(\mathrm{A}-\mathrm{a}\right){\mathrm{O}}_2} \) increases with increasing alveolar PAO2. In lungs with severe nonuniform V̇A/Q̇ distribution, the \( {\mathrm{P}}_{\left(\mathrm{A}-\mathrm{a}\right){\mathrm{O}}_2} \) reaches a maximum at FIO2 of 0.6–0.7 and then decreases at higher FIO2 values. The decline in \( {\mathrm{P}}_{\left(\mathrm{A}-\mathrm{a}\right){\mathrm{O}}_2} \) at higher FIO2 is caused by more uniform rises in PaO2, which overcome the nonuniform distribution of V̇A/Q̇ ratios. This nonlinear relationship between the \( {\mathrm{P}}_{\left(\mathrm{A}-\mathrm{a}\right){\mathrm{O}}_2} \) and FIO2 makes reference \( {\mathrm{P}}_{\left(\mathrm{A}-\mathrm{a}\right){\mathrm{O}}_2} \) values obtained with supplemental O2 difficult to use in critically ill patients, whose FIO2 values vary frequently.
The PaO2/FIO2 ratio is a simple, bedside index of O2 exchange when V̇A/Q̇ mismatch is the primary cause of hypoxemia. However, this ratio loses reliability when hypoventilation contributes to hypoxemia. The PaO2/PAO2 ratio is another easily calculated index of oxygenation. It has advantages and disadvantages similar to that of the PaO2/FIO2 ratio. In addition, the PaO2/PAO2 ratio can be misleading if \( \mathrm{P}\overline{\mathrm{v}}{\mathrm{O}}_2 \) fluctuates. For example, when cardiac output decreases, the \( \mathrm{P}\overline{\mathrm{v}}{\mathrm{O}}_2 \) falls because the tissues extract more O2 from the arterial blood. Thus, more profoundly hypoxemic mixed venous blood decreases PaO2, resulting in lower PaO2/PAO2, but the decrease is not because of worsening gas exchange in the lungs; rather, it is because of low cardiac output. The PaO2/PAO2 ratio is also affected by PACO2 (e.g., hypoventilation).
The presence of right-to-left shunt can be differentiated from low V̇A/Q̇ causes of hypoxemia by breathing 100% O2. While the individual breathes pure O2, the alveolar PAO2 in different lung units differs according to differences in alveolar PACO2. Lung units with low V̇A/Q̇ ratios increase their PAO2 values maximally with elevation of the inspired PO2, but shunt does not. The amount of the shunt can be calculated with the following equation:
where Q̇s/Q̇t is the shunt (Q̇s) as a fraction of cardiac output (Q̇t), Cc′O2 is end-capillary O2 concentration, CaO2 is arterial O2 concentration, and \( \mathrm{C}\overline{\mathrm{v}}{\mathrm{O}}_2 \) is mixed venous O2 concentration. Healthy individuals have a small shunt that amounts to 2–5% of the cardiac output. This shunt or venous admixture occurs because some venous blood normally drains into the pulmonary veins, left atrium, or left ventricle from bronchial and myocardial (Thebesian) circulation.
Breathing 100% O2 increases the arterial PaO2 to greater than 600 mmHg in normal adults. If PaO2 only rises to 250 mmHg during 100% O2 breathing, the shunt is about one-fourth the cardiac output (25%). This procedure does not determine the anatomic location of a shunt, which may be intracardiac or intrapulmonary, but the calculation can help the clinician focus the differential diagnosis for causes of hypoxemia that develop predominantly by shunt mechanisms. Furthermore, because PaO2 shows little response to variations in FIO2 at shunt fractions that exceed 25%, the clinician may be encouraged to reduce toxic and marginally effective concentrations of O2. However, the shunt calculation frequently overestimates the true shunt because alveoli with very low V̇A/Q̇ ratios (<0.1) may collapse completely during O2 breathing.
Oxygen delivery to the tissue (DO2) is determined by arterial oxygen content (CaO2) × cardiac output (Q̇) and is normally 1000 mL/min (200 mL O2/L × 5 L/min). Tissues extract oxygen at different rates, but overall, under normal conditions, total body extraction is 25% of the oxygen delivered resulting in mixed venous oxygen content of 150 mL/L (75% Hb O2 saturation, venous \( \mathrm{P}\overline{\mathrm{v}}{\mathrm{O}}_2 \) near 40 mmHg). When oxygen delivery is compromised (hypoxemia or depressed cardiac output) or oxygen demands are high (e.g., exercise), total body tissue oxygen extraction can increase and mixed venous content will fall. In disease states where oxygen extraction is compromised, mixed venous oxygen and mixed venous \( \mathrm{P}\overline{\mathrm{v}}{\mathrm{O}}_2 \) will be high.
5.6.2 Arterial and Venous PCO2 and HCO3–
Arterial PaCO2 is the partial pressure of CO2 in arterial blood and is determined by the relationship between CO2 production in the tissues (V̇CO2) and alveolar ventilation in the lungs (V̇A):
where V̇CO2 is carbon dioxide production in mL/min, V̇A is alveolar ventilation in mL/min, and K is a constant accounting for CO2 content and its relationship to PaCO2 (described below) and is approximately 800 mmHg. Normal values for arterial PaCO2 are 35–45 mmHg, a value reflecting the alveolar ventilation required to bring the alveolar PAO2 to 100 mmHg breathing room air at sea level (PIO2 = 150 mmHg). Because of the relationship of PaCO2 with pH and HCO3− described below, a normal arterial PaCO2 results in a pH of 7.38–7.42. Hypercapnia usually results from reductions in V̇A necessary for a given V̇CO2 and creates an acidosis; hypocapnia usually results from excess V̇A for a given V̇CO2 and results in an alkalosis.
The transport pathway of CO2 begins with the diffusion of CO2 from tissues into the capillary blood and ends at the alveolar-capillary interface where CO2 rapidly diffuses along a concentration gradient into alveolar gas. Under normal conditions, the mixed venous \( \mathrm{P}\overline{\mathrm{v}}{\mathrm{CO}}_2 \) is 45 mmHg and the resulting gradient in the alveolus with a PaCO2 of 40 mmHg is 5 mmHg.
About 90% of the CO2 that enters the blood diffuses into the RBCs, where it undergoes one of three chemical reactions: (1) it remains as dissolved CO2, (2) it combines with the NH2 groups of hemoglobin to form carbaminohemoglobin, or (3) it combines with water to form H2CO3, which dissociates into H+ and HCO3−. The remaining 10% of the CO2 in the plasma exists as dissolved CO2 and carbamino compounds after reacting with NH2 groups of plasma proteins.
The amount of CO2 that dissolves in plasma at 37 °C is about 0.03 mmol/L for every mmHg of PCO2; thus, for a normal PaCO2 of 40 mmHg, the normal amount of dissolved CO2 in arterial blood is 40 × 0.03, or 1.2 mmol/L. Although the amount of dissolved CO2 is relatively small, it is in equilibrium with the plasma PaCO2, which in turn determines the direction and rate of CO2 diffusion at body tissue and alveolar levels.
In plasma, CO2 undergoes the following reaction:
The rate of this reaction is relatively slow in plasma, and the amount of carbonic acid (H2CO3) in the plasma is extremely small; even so, plasma H2CO3 is a major determinant of the blood’s H+ concentration (i.e., the pH). The reaction rate of CO2 with H2O in the erythrocyte is about 13,000 times faster than in the plasma due to the influence of carbonic anhydrase, an intracellular catalytic enzyme. As a result H+ is rapidly generated, but it is immediately buffered by hemoglobin and thus removed from solution. Consequently, the reaction keeps moving to the right, continually drawing more CO2 into the erythrocyte, generating HCO3− in the process. As HCO3− accumulates in the erythrocyte, its intracellular concentration rises; HCO3− then diffuses down its concentration gradient into the plasma. This mechanism is responsible for nearly all of the HCO3− in the plasma.
When negatively charged HCO3− ions diffuse out of the erythrocyte, an electropositive environment develops inside the erythrocyte. In response, Cl−, the most abundant anion in the plasma, diffuses into the erythrocyte (the so-called chloride shift, a process governed by the anion exchange protein 1 (AE or band 3) on the RBC membrane), which maintains intracellular electrical neutrality. Some movement of water inward occurs simultaneously with the chloride shift to maintain osmotic equilibrium, resulting in a slight swelling of erythrocytes in venous blood relative to those in arterial blood.
The CO2 hemoglobin equilibrium curve is essentially linear over the physiologic range of PaCO2, in contrast to the S-shaped oxyhemoglobin equilibrium curve. This means a change in alveolar ventilation is much more effective in changing arterial CO2 content than O2 content; for example, a doubling of the alveolar ventilation in the healthy lung cuts the blood CO2 content in half but changes arterial O2 content very little because hemoglobin is already nearly 100% saturated with normal ventilation. The steepness of the CO2 hemoglobin equilibrium curve also permits continued excretion of CO2 even in the presence of significant mismatching of pulmonary ventilation and blood flow.
5.7 Noninvasive Measurement of the Hemoglobin Oxygen Saturation
Pulse oximetry provides a quick, noninvasive measure of the hemoglobin O2 saturation (SpO2) which can be a useful indicator of problems with gas exchange. It is sometimes called the fifth vital sign. The measurement is based on the change in color of Hb that occurs when reduced Hb is oxygenated. Oxyhemoglobin is red, while reduced Hb (deoxyhemoglobin) is bluish-purple. The different colors affect the absorption of different wavelengths of light. Oxyhemoglobin absorbs more infrared light and transmits more red light. Conversely, reduced hemoglobin absorbs more red light and transmits more infrared light. A pulse oximeter has bright sources of red and infrared light that are shone through a thin area of skin with good perfusion such as the fingertip, toe, or earlobe. A detector on the opposite side monitors the change in light transmission that occurs with pulsatile blood flow. The ratio of red to infrared transmission during the arterial surge of blood is used to calculate the percentage of arterial Hb that is O2Hb.
A limitation of standard pulse oximetry is that COHb, being a cherry red color, is not distinguished from O2Hb and so that the reported SpO2 includes both O2Hb and COHb. This limitation can be overcome by using CO-oximetry which uses additional light sources with different wavelengths to detect COHb.
A normal, healthy person at altitudes less than 1 km should have SpO2 > 95%. A resting SpO2 ≤ 88% is often an indication of the need for continuous supplemental O2 therapy with the goal of increasing SpO2 above 92%. Similarly, if SpO2 falls below 88% during exercise or for a significant portion of a night’s sleep, supplemental O2 therapy may be indicated during exercise or sleep.
The correlation between PaO2 and SpO2 is nonlinear and is affected by temperature, pH, and PACO2. However, SpO2 measurements can complement the information obtained from arterial blood gas measurements. While PaO2 is the preferred measure of gas exchange from the lung to the bloodstream, arguments have been made that SpO2 is a better measure of oxygenation of the tissues. Arterial blood gas measurements provide data from a single time point, while SpO2 can be continuously monitored, including in ambulatory patients.
5.8 Example Cases
-
1.
A 63-year-old man has known COPD. There is very severe airway obstruction and substantial air trapping on spirometry and volume testing (Fig. 5.4). His arterial blood gases reveal a PaO2 of 61 mmHg, a PaCO2 of 49 mmHg, and a pH of 7.37. His hypercapnia is typical for severe COPD with a high work of breathing and his hypoxemia reflects both hypoventilation and ventilation/perfusion mismatching. The DLCO is dramatically reduced likely reflecting emphysematous destruction of alveoli. However, VI during the DLCO maneuver was only 65% of the FVC and 70% of the slow VC measured during volume testing – typical of bad airway obstruction where the longer expiratory time of the FVC maneuver (>12 s) and the longer time allowed for the “slow” VC produce larger vital capacities than the VI inhaled during the rapid inspiratory time of the DLCO maneuver. The impact of this low VI on such a markedly reduced DLCO, however, is likely small. More importantly, the slope of the exhaled CH4 over time curve is markedly downward consistent with poor gas mixing (consistent with the significant air trapping). This is also reflected in the VA/TLC ratio of only 29%. Both of these markers of poor gas mixing essentially mean that the observed DLCO is likely reflecting gas exchange properties in only a small portion of better-ventilated lung regions. The high KCO is interesting and may suggest that this better ventilated region has good gas transfer properties but a low DLCO from either a reduced inspired volume and/or regional volume compression from adjacent hyperinflated lung units.

Pulmonary function test results for case 1 fix VA = 2.19 (not = 12.0)
-
2.
A 65 year-old man with known interstitial lung disease reports worsening dyspnea over last 3 months. Arterial blood gases reveal a PaO2 of 53 mmHg (breathing room air), a PaCO2 of 36 mmHg, and a pH of 7.46. His hypoxemia reflects ventilation/perfusion mismatching due to his interstitial lung disease and should be treated with supplemental O2. His PaCO2 and pH reflect mild hyperventilation in response to his hypoxemia. His PFTs show marked loss of lung volumes over last 5 months (Fig. 5.5). His hemoglobin adjusted DLCO is very low. Testing looks good with a VI/VC of 93%, a flat CH4 over time tracing, and a VA/TLC ratio of 0.96. The dramatic drop in both volumes and DLCO since previous testing likely reflects progression of his ILD. Note that his DLCO has dropped to 28% of the previous value whereas his VA has dropped to only 44% of the previous value. This suggests that KCO has also dropped reflecting both lung parenchyma and capillary involvement.

Pulmonary function test results for case 2
Selected References
Bachofen H, Schurch S, Urbinelli M, Weibel ER. Relations among alveolar surface tension, surface area, volume, and recoil pressure. J Appl Physiol. 1987;62:1878–87.
Butler JP, Tsuda A. Transport of gases between the environment and alveoli – theoretical foundations. Compr Physiol. 2011;1(3):1301–16.
Chan ED, Chan MM, Chan MM. Pulse oximetry: understanding its basic principles facilitates appreciation of its limitations. Respir Med. 2013;107:789–99.
Cotes JE, Chinn DL, Miller MR. Lung function. 6th ed. Oxford: Blackwell Scientific Publications; 2006.
Culver BH, Graham BL, Coates AL, et al. Recommendations for a standardized pulmonary function report. An official American Thoracic Society technical statement. Am J Respir Crit Care Med. 2017;196:1463–72.
Engel LA. Gas mixing within the acinus of the lung. J Appl Physiol. 1983;54:609–18.
Forster RE. Chapter 5. Diffusion of gases across the alveolar membrane. In: Farhi LE, Tenney SM, editors. Handbook of physiology. Section 5.3. The respiratory system. Vol IV. Gas exchange. Bethesda, MD: American Physiological Society; 1987. p. 71–88.
Graham BL, Brusasco V, Burgos F, et al. 2017 ERS/ATS standards for single-breath carbon monoxide uptake in the lung. Eur Respir J. 2017;49:1600016.
Graham BL, Mink JT, Cotton DJ. Effects of increasing carboxyhemoglobin on the single breath carbon monoxide diffusing capacity. Am J Respir Crit Care Med. 2002;165:1504–10.
Graham BL, Mink JT, Cotton DJ. Implementing the three equation method of measuring single breath carbon monoxide diffusing capacity. Can Respir J. 1996;3:247–57.
Hollowell J, Van Assendelft O, Gunter E, et al. Hematological and iron-related analytes—reference data for persons aged 1 year and over: United States, 1988–94. National Center for Health Statistics. Vital Health Stat. 2005;11:1–156.
Huang YC, O’Brien SR, MacIntyre NR. Intrabreath diffusing capacity of the lung in healthy individuals at rest and during exercise. Chest. 2002;122(1):177–85.
Huang YC, MacIntyre NR. Real-time gas analysis improves the measurement of single-breath diffusing capacity. Am Rev Respir Dis. 1992;146(4):946–50.
Hughes JM, Bates DV. Historical review: the carbon monoxide diffusing capacity (DLCO) and its membrane (DM) and red cell (Theta.Vc) components. Respir Physiol Neurobiol. 2003;138(2–3):115–42.
Jones RS, Meade F. A theoretical and experimental analysis of anomalies in the estimation of pulmonary diffusing capacity by the single breath method. Q J Exp Physiol. 1961;46:131–43.
Kaminsky DA, Whitman T, Callas PW. DLCO versus DLCO/VA as predictors of pulmonary gas exchange. Respir Med. 2007;101(5):989–94.
Kohn HN. Zur Histologie der indurierenden fibrinösen Pneumonie. Münch Med Wschr. 1893;40:42–5.
Krogh M. The diffusion of gases through the lungs of man. J Physiol. 1915;49:271–300.
Lambert MW. Accessory bronchiole-alveolar communications. J Pathol Bacteriol. 1955;70:311–4.
MacIntyre N, Crapo R, Viegi G, et al. Standardisation of the single-breath determination of carbon monoxide uptake in the lung. Eur Respir J. 2005;26:720–35.
McCormack MC. Facing the noise: addressing the endemic variability in D(LCO) testing. Respir Care. 2012;57(1):17–23.
Ogilvie CM, Forster RE, Blakemore WS, Morton JW. A standardized breath holding technique for the clinical measurement of the diffusing capacity of the lung for carbon monoxide. J Clin Invest. 1957;36:1–17.
Paiva M, Engel LA. Gas mixing in the lung periphery. In: Chang HK, Paiva M, editors. Respiratory physiology. An analytic approach. Lung biology in health and disease, vol. 40. New York: Marcel Dekker, Inc; 1989. p. 245–76.
Piiper J, Scheid P. Chapter 4. Diffusion and convection in intrapulmonary gas mixing. In: Farhi LE, Tenney SM, editors. Handbook of physiology. Section 5.3. The respiratory system. Vol IV. Gas exchange. Bethesda, MD: American Physiological Society; 1984. p. 51–69.
Roughton FJW, Forster RE. Relative importance of diffusion and chemical reaction rates in determining rate of exchange of gases in the human lung, with special reference to true diffusing capacity of pulmonary membrane and volume of blood in the lung capillaries. J Appl Physiol. 1957;11:290–302.
Sikand RS, Magnussen H, Scheid P, Piiper J. Convective and diffusive gas mixing in human lungs: experiments and model analysis. J Appl Physiol. 1976;40:362–71.
Smith TC, Rankin J. Pulmonary diffusing capacity and the capillary bed during Valsalva and Muller maneuvers. J Appl Physiol. 1969;27:826–33.
Stanojevic S, Graham BL, Cooper BG, et al. Official ERS technical standards: Global Lung Function Initiative reference values for the carbon monoxide transfer factor for Caucasians. Eur Respir J. 2017;50:1700010.
Wanger J. ATS Pulmonary Function Laboratory Management and Procedure Manual. 3rd ed: American Thoracic Society, New York, NY, USA; 2016. https://www.thoracic.org/professionals/education/pulmonary-function-testing/
West JB, Dollery CT, Naimark A. Distribution of blood flow in isolated lung; relation to vascular and alveolar pressures. J Appl Physiol. 1964;19:713–24.
West JB, Wagner PD. Pulmonary gas exchange. Am J Respir Crit Care Med. 1998;157:S82–7.
West JB. Respiratory physiology: the essentials. 9th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2012.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Appendix
Appendix
The MIGET is based on the physical principles governing inert gas elimination by the lungs. When an inert gas in solution is infused into systemic veins, the proportion of gas eliminated by ventilation from a lung unit depends only on the solubility of the gas and the V̇A/Q̇ ratio of that unit. The relationship is given by the following equation:
where Pc′ and \( \mathrm{P}\overline{\mathrm{v}} \) are the partial pressures of the gas in end-capillary blood and mixed venous blood, respectively, and λ is the blood-gas partition coefficient. The ratio of Pc′ over \( \mathrm{P}\overline{\mathrm{v}} \) is known as the retention.
To obtain the V̇A/Q̇ distribution of the lung, a saline solution containing low concentrations of six inert gases of different solubility (sulfur hexafluoride [SF6], ethane, cyclopropane, isoflurane, diethyl ether, and acetone) is infused slowly into a peripheral vein until a steady state is reached. The inert gas concentrations in the arterial, mixed venous, and expired gas samples are collected and analyzed. Retention and excretion values for the inert gases are graphed against their solubility in blood. With a 50-compartment model, the retention-solubility plots can be transformed to obtain the distribution of V̇A/Q̇ ratios in the lung. A lung containing shunt units (V̇A/Q̇ = 0) shows increased retention of the least-soluble gas, SF6. Conversely, a lung having large amounts of ventilation-to-lung units with very high V̇A/Q̇ ratios and dead space (V̇A/Q̇ = infinity) shows increased retention of the high-solubility gases (such as ether and acetone).
In healthy subjects, the distributions for both ventilation and blood flow (dispersion) are narrow and span only one log of V̇A/Q̇ ratios. Essentially, no ventilation or blood flow occurs outside the range of approximately 0.3–3.0 on the V̇A/Q̇ ratio scale, and no significant intrapulmonary shunt is detected. With aging, the dispersion of ventilation and perfusion increases. In older subjects, as much as 10% of the total blood flow may go to lung units with V̇A/Q̇ values of less than 0.1, but still no shunt is detected. The increased low V̇A/Q̇ regions adequately explain the decreased Pao2 and increased \( {\mathrm{P}}_{\left(\mathrm{A}-\mathrm{a}\right){\mathrm{O}}_2} \) difference with aging. The cause of such age-related V̇A/Q̇ mismatch often is attributed to degenerative processes in the small airways with aging.
Various abnormal patterns of V̇A/Q̇ distributions measured by the MIGET method adequately explain gas exchange abnormalities in diseased lungs. For example, Fig. 5.6 shows the distribution of V̇A/Q̇ ratios from an individual with chronic obstructive lung disease. The V̇A/Q̇ distribution is bimodal, and large amounts of ventilation go to lung units with extremely high V̇A/Q̇ ratios. This V̇A/Q̇ pattern can be seen in individuals with predominant emphysema (Fig. 5.6, top). Presumably the high V̇A/Q̇ regions represent lung units in which many capillaries have been destroyed by the emphysematous process. In some patients, there are regions of low V̇A/Q̇ (Fig. 5.6, middle), as is commonly seen in patients with predominant chronic bronchitis. Finally, some patients have combinations of both high and low V̇A/Q̇ units (Fig. 5.6, bottom). Note that the main modes of V̇A and Q̇ in the middle and the bottom graphs center on units with V̇A/Q̇ ratio greater than 1 (high V̇A/Q̇ units).

Distribution of V̇A/Q̇ ratios in different patients with COPD, illustrating predominant emphysema, with high V̇A/Q̇ units (top), predominant chronic bronchitis, with low V̇A/Q̇ units (middle), and a mixture of both high and low V̇A/Q̇ units (bottom). (Reproduced with permission from Springer)
Rights and permissions
Copyright information
© 2018 Springer International Publishing AG, part of Springer Nature
About this chapter

Cite this chapter
Graham, B.L., MacIntyre, N., Huang, Y.C. (2018). Gas Exchange. In: Kaminsky, D., Irvin, C. (eds) Pulmonary Function Testing. Respiratory Medicine. Humana Press, Cham. https://doi.org/10.1007/978-3-319-94159-2_5
Download citation
DOI: https://doi.org/10.1007/978-3-319-94159-2_5
Published:
Publisher Name: Humana Press, Cham
Print ISBN: 978-3-319-94158-5
Online ISBN: 978-3-319-94159-2
eBook Packages: MedicineMedicine (R0)