
Abstract
Lung function is inextricably linked to pulmonary anatomy and structure. Human lungs have distinctively adapted to permit life in the earth’s unique atmosphere. While gas exchange happens at the alveoli, gas must first traverse the entire bronchial tree before crossing the pulmonary capillary bed to mix with the pulmonary circulation, and to transport gases via the cardiovascular system. Therefore, the lungs are co-dependent with the heart supplying adequate pulmonary blood flow to properly function. Before being able to interpret lung function, one must have an understanding of the critical aspects of pulmonary structure and function.
The functionality of the pulmonary system is based upon the structural components of which it is built. Each anatomical component of the pulmonary system supports its primary function, gas exchange. The human lungs are responsible for extraction of oxygen, elimination of waste products of metabolism, maintenance of pH balance, and host defense against the outside environment.
Access provided by CONRICYT-eBooks. Download chapter PDF
Similar content being viewed by others


Keywords
1.1 Pulmonary Structure
The primary function of the lungs is gas exchange. Knowledge of the anatomy and airflow pathways is important to understand how gas moves to the blood from the atmosphere. Human airway anatomy starts at the oro- and nasopharynx and terminates at the alveoli. The airways along this path can be divided into two zones: (1) conducting zone, consisting of large and medium airways that are responsible for mass transport of air from the atmosphere to the alveoli without gas exchange occurring, and (2) respiratory zone, consisting of small airways with alveolar sacs in their walls (airways <2 mm) and alveoli that participate in gas exchange with the blood.
1.1.1 Conducting Zone
Air moves through the mouth and nares to the oro- and nasopharynx. The oro- and nasopharynx combine to form the hypopharynx which houses the epiglottis, larynx, and upper esophageal sphincter. The larynx is a complex structure that contains the vocal cords and forms a passage for movement of air from the hypopharynx to the trachea. The trachea is a flexible single tubular airway passage which is kept patent by a series of c-shaped collagenous rings. Between the rings are smooth muscle and fibroelastic tissue. The posterior wall of the trachea contains no cartilaginous support and is comprised of a longitudinally oriented membrane that contains smooth muscle (Fig. 1.1). The trachea is 10–12 cm in length and is divided into an upper extrathoracic portion and a lower intrathoracic portion, separated at the level of superior aspect of the manubrium. At the angle of Louis (manubriosternal junction), the trachea divides into the left and right main stem (primary) bronchi at the main carina. The main stem bronchi then rapidly branch into shorter, smaller (secondary) lobar bronchi, then (tertiary) segmental bronchi, and then subsegemental bronchi until terminating into bronchioles. Like the trachea, bronchi are flexible and contain less collagenous support than the trachea, and the folded mucosa is encircled by a layer of smooth muscle (Fig. 1.2). Tertiary bronchi give rise to the terminal component of the conducting system, bronchioles, which are generally less than 1 mm in diameter. Bronchioles do not contain collagenous support but contain folded mucosa with a ring of smooth muscle (Fig. 1.3). The most distal bronchioles are named terminal bronchioles and also contain a thin layer of smooth muscle (Fig. 1.4). Since no gas exchange occurs in the conducting zone, this entire region is considered anatomical dead space (see Chap. 5), the total volume of which is ~150 mL.

Trachea histology. PM posterior membrane, TM trachealis muscle, G glands, E epithelium

Bronchus histology. Cross section of bronchus depicting microstructure of the airway wall. SM smooth muscle, C cartilage, G gland, BV blood vessel (bronchial circulation), E epithelium

Bronchiole histology. SM smooth muscle, G gland, E epithelium

Terminal bronchiole and respiratory bronchiole histology. Terminal bronchiole on end branching to form respiratory bronchiole lined with alveolar sacs. T terminal bronchiole, R respiratory bronchiole, AS alveolar sacs
1.1.2 Respiratory Zone
The respiratory zone begins as terminal bronchioles and subsequently divides into respiratory bronchioles forming anatomical units called acini. While respiratory bronchioles are still conducting airways, they contain alveolar sacs that can participate in gas exchange. The respiratory bronchioles divide into alveolar ducts that are completely lined with alveolar sacs. The alveolar ducts terminate with thin walled alveolar sacs and are the primary location for gas exchange. Due to this rapid branching, the cross-sectional area for gas exchange exponentially increases with each division. It is estimated that the total cross-sectional area of the lungs is approximately 50–75 m2 (Fig. 1.5). The volume of the respiratory zone is the majority of a subject’s total lung capacity. Figure 1.6 depicts the rapidly branching nature of the airway tree.

Bronchial tree, size, and number of airways

Silicone cast of the airway tree
1.1.3 Pulmonary Vasculature
With the primary function of the lungs being gas exchange, the lungs are dependent on adequate perfusion. The right heart pumps deoxygenated blood from the systemic circulation through the pulmonary circulation via the pulmonary artery. The main pulmonary artery bifurcates to a left and right side each supplying the ipsilateral lung. The pulmonary arteries then sequentially divide, following alongside the airway tree. Like the respiratory tree, the pulmonary arteries rapidly divide until forming a series of capillaries, about the diameter of a single red blood cell, that form networks around the alveoli, providing interfaces for gas exchange. Oxygenated blood is returned to the left heart via pulmonary veins and then out to the systemic circulation. As the entire cardiac output is circulated through the lungs, one of the unique features of the pulmonary circulation is its low resistance to flow, being about one tenth the resistance of the systemic circulation. This gives the lungs the ability to handle a large cardiac output at relatively low pulmonary pressures.
Because of the anatomic arrangement of the pulmonary vasculature along the airways, and the influence of gravity on blood flow and pulmonary compliance, the lung is uniquely situated to bring more blood flow to dependent regions that are better ventilated and less blood flow to nondependent regions that are less well ventilated. This matching of ventilation and perfusion is a key physiologic aspect of how the lung optimizes the efficiency of gas exchange.
The lungs have a dual blood supply, primarily from the pulmonary circulation but supported by bronchial arteries. The bronchial arteries arise from the aorta and intercostal arteries providing oxygenated blood to the airways and lung supporting tissues and ending at the level of the terminal bronchioles. As the bronchial arteries arise from peripheral arterial circulation, they deliver oxygenated blood to the lung tissues. They also supply blood to the lower third of the esophagus, the vagus nerve, the visceral pleura, the pericardium, the hilar lymph nodes and the vasa vasorum of the thoracic aorta and pulmonary arteries and veins. Venous drainage from the lower trachea and lobar bronchi is via the bronchial veins to the right atrium. However, venous drainage from the more distal lung is via anastomoses between the bronchial veins and pulmonary veins to the left atrium is to the right atrium via the azygous system from the airways down to the lower trachea and lobar bronchi.
1.1.4 Muscles of Respiration
During inhalation, negative pressure at the pleura draws air in through the oro- and nasopharynx to the respiratory zone for gas exchange. The negative pleural pressure is primarily generated by contraction and flattening of the diaphragm. Inhalation can also be aided by accessory muscles, largely being the external intercostals, sternocleidomastoid, and scalenes which stabilize, lift, and expand the rib cage.
Expiration is a passive process during quiet breathing, moving air out of the thorax by relaxation and elastic recoil of the lungs and diaphragm. However, during active breathing, exhalation can be supported by contraction of the internal intercostals (pulling the ribs down) and abdominal muscles (contracting the abdominal compartment to elevate the diaphragm).
1.2 How Lung Function Is Based on Structure
1.2.1 Conditioning and Host Defense
Before gas can be exchanged with the blood, air from the atmosphere must be conditioned for hospitable delivery to the sensitive alveoli. The epithelium of the conducting airways plays a critical role in preconditioning air for exchange. The relatively dry air of the atmosphere must be humidified before delivery to the alveoli. The respiratory epithelium of the trachea and bronchi contain goblet cells that produce epithelial lining fluid, containing mucus and watery secretions that act to warm and humidify the air. Large air pollutants are filtered at the nares. The epithelial lining fluid of the trachea and bronchi acts to trap particles, and the trachea’s ciliated epithelium transports it up toward the pharynx, where it is then swallowed or expectorated. This is a key defense mechanism to protect the lung from pollutants and infection.
1.2.2 Gas Delivery to the Alveoli
During quiet breathing, about 500 mL of air is inhaled. However, because of the anatomical dead space of about 150 ml in the conducting zone, not all of this volume is delivered to the alveoli. For this reason, it is important to understand the different static lung volumes (see Chap. 3). With normal quiet breathing, the volume of each breath is termed tidal volume. The vital capacity (VC) is the amount of air moved after maximal inhalation and exhalation. Functional residual capacity (FRC) is the amount of air left in the lungs after quiet exhalation. However, because complete collapse of the alveoli and conducting zone does not occur even after maximal expiration, there is a residual volume (RV) that still remains in the lungs (Fig. 1.7). Residual volume (and FRC) cannot be assessed by simply measuring airflow at the mouth (i.e., spirometry); therefore more advanced pulmonary function testing techniques are needed to derive these volumes (see Lung Volume Measurement). Total lung capacity (TLC) is a total volume of air in the lungs, the sum of vital capacity and residual volume.

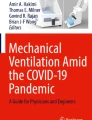
Lung volumes and capacities. A spirogram (volume vs. time) of an individual who is first breathing quietly (reading from left to right), then takes a maximal inhalation to total lung capacity (TLC), then exhales slowly to residual volume (RV), and then returns to quiet breathing. On the right are the four lung volumes: inspiratory reserve volume (IRV), tidal volume (TV), expiratory reserve volume (ERV), and RV. Lung capacities are the combination of lung volumes and are as follows: TLC shown here as RV + ERV + TV + IRV, inspiratory capacity (IC) shown here as TV + IRV, functional residual capacity (FRC) shown here as ERV + RV, and vital capacity shown here as IRV + TV + ERV
1.2.3 Gas Exchange at the Alveoli
The alveolar/capillary interface is the site of gas exchange. The alveolar epithelium contains two cell types: (1) type 1 pneumocytes (95% of alveolar area) (these are very thin flat cells through which gas exchange occurs) and (2) type 2 pneumocytes (5% of alveolar area) (these secrete surfactant to maintain alveolar stability and contribute to host defense in the lung). The type 1 pneumocytes are in extremely close proximity to the vascular endothelium of the capillary (~0.25 μm) through which gases can easily cross. The rapid branching of the respiratory tree leads to an exponential increase in the total cross-sectional surface area for exchange to occur. This in turn decreases the velocity of air moving across the alveoli and permits sufficient time for gas exchange within the capillary bed. Equilibrium between the alveolar gas and blood in the capillary happens extremely quickly, so efficient that each red blood cell fully takes up oxygen in only about 0.25 s of the approximately 0.75 s it spends in the capillary bed.
1.2.4 Drivers of Respiration
The control center for respiration is located in the respiratory center in the medulla in the brainstem (See Chap. 9). Neurons in the medulla contain pacemaker cells that are self-excitatory and stimulate the diaphragm and external intercostals via the phrenic nerve. Higher cortical centers aid in the control of respiration to permit airflow through the vocal cords to allow speech. Respiratory drive is modulated by feedback from stretch receptors in the lungs via the vagus nerve, central chemoreceptors responding to changes in pH and CO2, peripheral chemoreceptors in the aortic arch via vagus nerve, and carotid bodies via glossopharyngeal nerve, the latter two responding to changes in O2, CO2, and pH. These chemoreceptors are ultimately responsible for respiratory drive maintaining homeostasis of the blood, ensuring adequate oxygen delivery, and metabolic waste elimination.
1.3 Components of Pulmonary Function Testing
One of the first steps in the evaluation of pulmonary pathology is assessment of pulmonary function. While static imaging can give us clues to structural morphology, they offer little information of the dynamic function of the lungs. Pulmonary function testing (PFT) is a series of tests, most often performed in a PFT lab, which evaluates the global function of the lungs. There are three primary goals of pulmonary function testing: (1) assessment of airflow obstruction, (2) measurement of lung volumes, and (3) assessment of diffusion of gases across the alveoli/capillary interface. Additionally, 6-min walk testing (6MWT), incremental and endurance shuttle walk testing (ISWT, ESWT), and cardiopulmonary exercise testing (CPET) can offer a broader assessment of the cardiac, pulmonary, and peripheral circulatory interactions, helpful in the evaluation of dyspnea. Finally, tests of respiratory muscle strength and drive may additionally be helpful in the evaluation of disease state.
1.3.1 Spirometry
Spirometry is performed by breathing through a sealed mouthpiece (with closed nares) to measure how much and how quickly airflow is generated by the lungs. Most often, airflow is measured using a pneumotachometer, based on the measured pressure drop across a fine metal screen. This generates data on flow and calculated volume. Three of the most critical outputs from spirometry are (1) the volume of forced air exhaled in the first one second (FEV1); (2) the total volume of air that can be forcefully exhaled voluntarily, the forced vital capacity (FVC); and (3) the ratio of FEV1/FVC. These offer a global assessment of how much and how fast air can be exhaled from the lungs, which is essential in the evaluation of airflow obstruction (e.g., asthma, COPD).
Using spirometry, flow-volume loops are also generated (Fig. 1.8). These graphical depictions describe the normal pattern of airflow during an entire forced respiratory cycle (inhalation and exhalation), plotting flow on the y-axis and volume on the x-axis. The flow-volume loop pattern can take on characteristic shapes based on certain pathologies. Slowly emptying airways, intra- and extrathoracic airway obstruction, and vocal cord dysfunction are a few of the helpful characteristic patterns that can be evaluated on flow-volume loops (see Chap. 7).

Flow-volume loop. Example of normal flow-volume loop
1.3.2 Lung Volume Measurement
As spirometry can only measure the amount of air forcibly exhaled, assessment of the residual air (RV and FRC) or total lung volume (TLC) is not possible with this method. As changes in lung volumes are a common finding in obstructive lung disease (e.g., hyperinflation, increased TLC; air trapping, increased RV), interstitial lung disease (decreased TLC), and obesity (decreased ERV), additional techniques are needed to measure the various lung volumes for accurate diagnostics.
Lung volumes are most commonly measured by two techniques, (1) body plethysmography and (2) closed-circuit inert gas dilution. Body plethysmography is based on Boyle’s law (P1V1 = P2V2) by placing the patient in an airtight box and having them breathe against a closed shutter after quiet exhalation. Change in the box pressure between inhalation and exhalation permits calculation in the change in volume in the box. This change in volume is the FRC. By doing other breathing maneuvers such as inspiratory capacity and vital capacity, calculations of RV and TLC can be performed. Lung volumes can also be measured using the inert gas washout technique. This method capitalizes on the conservation of mass principle (C1V1 = C2V2) to determine lung volumes. A known volume and concentration of gas (usually helium) is quietly inhaled over a series of breaths. After equilibrium has been reached, the concentration of gas at end exhalation is measured, permitting calculation of FRC, RV, and TLC (see Chap. 3).
1.3.3 Diffusing Capacity
Measurement of diffusion capacity enables a combined assessment of the area and thickness of the blood-gas interface as well as assessment of pulmonary capillary volume. In most circumstances, carbon monoxide (CO) is used as it is a diffusion-limited gas and therefore freely diffuses across the blood-gas interface and does not have a potential to reach diffusion limitation as oxygen does (see Chap. 6). The laws of diffusion state the volume of gas that diffuses across a membrane is proportional to the area for exchange and inversely proportional to the thickness of the membrane. Thus measuring the exhaled volume (partial pressure) of CO following a known volume of inhaled CO, over a known time, provides a combined assessment of the alveolar surface area and thickness of the interstitium, termed diffusing capacity (DLCO). Diffusing capacity is helpful for the diagnosis and evaluation of pulmonary diseases with loss of alveolar surface area (e.g., emphysema), increased interstitial thickness (e.g., pulmonary fibrosis), or loss of capillary volume (e.g., pulmonary hypertension).
1.3.4 Exercise Testing
A relatively simple, yet standardized and robust, assessment of one’s pulmonary reserve can be achieved by performing a 6-min walk test (6MWT). It does not require any specific instruments and can easily be performed in almost any location. Patients walk on flat ground at a self-paced rate for 6 min, and the distances traveled are measured. It provides a combined global functional assessment of the integrated pulmonary, cardiac, and peripheral circulatory systems. Another important field exercise test is the shuttle walk test, which is classically considered as two different tests, the incremental shuttle walk test (ISWT) and the endurance shuttle walk test (ESWT). Both tests are commonly used outside the United States, where the ISWT is a good measure of maximal exercise capacity and the ESWT provides information on exercise endurance. While the 6MWT, ISWT, and ESWT do not provide specific assessment of the individual physiological systems, more complex testing via cardiopulmonary exercise testing (CPET) can provide useful information on the individual limitations of each of these systems (cardiac, pulmonary, circulatory), helpful for the advanced evaluation of dyspnea (see Chap. 12).
1.3.5 Tests of Respiratory Drive and Muscle Strength
Pulmonary function tests are also available to assess various aspects of the neuromuscular contribution to breathing. Specifically, the drive to breathe in response to hypoxia and hypercapnia is assessed by measuring the change in minute ventilation in response to progressive hypoxemia or hypercapnia, respectively. An overall measure of drive to breathe is also assessed by measuring the inspiratory pressure that occurs within the first 100 ms of inhalation, termed the “P100” or “P0.1.” The function of the respiratory muscles themselves is usually assessed by measuring the maximal inspiratory and maximal expiratory pressures (MIP, MEP).
1.3.6 What Is on the Horizon?
New technologies are being developed and tested to advance and supplement the current landscape of pulmonary function testing. As spirometry is effort dependent and requires cooperation, a newer technology is the forced oscillation technique (FOT) which uses small amplitude pressure waves superimposed on normal breathing to assess airflow obstruction and small airway disease. FOT can be helpful in diagnoses in the pediatric population, as it requires little cooperation (see Chap. 8). Multiple-breath nitrogen washout (MBNW) is another emerging technique that can be used to calculate the lung clearance index (LCI) that measures global ventilation inhomogeneity but also is able to compartmentalize the ventilation heterogeneity into conducting airways (Scond) and more peripheral acinar airways (Sacin). This has potential to serve as a highly sensitive marker for assessing changes in airway status in diseases such as asthma, cystic fibrosis, and lung transplantation.
1.3.7 What Are We Trying to Achieve with the Report?
While no single diagnosis can be made with PFTs alone, they are designed to aid in the diagnosis as well as follow the response to therapy and the progression of disease. The raw data from PFTs are compiled to generate a report. The report provides physiologic analysis and interpretation of the findings, often with a differential diagnosis of disease processes that may cause the physiologic alterations. In interpreting these findings, the limitations of PFTs must be considered. PFTs are a critical tool utilized in the management of pulmonary disease. However, they should be interpreted with consideration of the patient’s presentation, history, physical exam, radiologic, and other findings.
1.4 Conclusion
To properly understand and interpret pulmonary function testing, knowledge of structural and functional interactions of the pulmonary system is needed. Respiration is modulated by central and peripheral chemoreceptors that provide feedback to the muscle of respiration to augment respiratory depth and rate. These muscles generate negative pleural pressure that draws air through the conducting zones of the lung to alveoli where gas exchange occurs. Pulmonary circulation supports delivery of deoxygenated blood and metabolites to the lung. Pulmonary disease can occur along any portion of this complex physiologic process, and pulmonary function tests play a vital role in management of pulmonary disease. The most common pulmonary tests are (1) spirometry, providing information primarily on airflow obstruction and lung volumes; (2) plethysmography or He dilution, measuring total lung volumes; and (3) diffusing capacity, measured using CO to assess overall gas exchange property of the lung. Pulmonary function testing is critical in the diagnosis, and evaluation of progression, and response to therapy in pulmonary disease.
Selected References
Berry CE, Wise RA. Interpretation of pulmonary function test: issues and controversies. Clin Rev Aller Immunol. 2009;37:173–80.
Blakemore WS, Forster RE, Morton JW. Ogilvie CM. A standardized breath holding technique for the clinical measurement of the diffusing capacity of the lung for carbon monoxide. J Clin Invest. 1957;36:1–17.
Bokov P, Delclaux C. Interpretation and use of routine pulmonary function tests: spirometry, static lung volumes, lung diffusion, arterial blood gas, methacholine challenge test and 6-minute walk test. La Revue de medecine interne. 2016;37:100–10.
Coates AL, Peslin R, Rodenstein D, Stocks J. Measurement of lung volumes by plethysmography. Eur Respir J. 1997;10:1415–27.
Flesch JD, Dine CJ. Lung volumes: measurement, clinical use, and coding. Chest. 2012;142:506–10.
Hyatt RE, Black LF. The flow-volume curve. A current perspective. Am Rev Respir Dis. 1973;107:191–9.
Permutt S, Martin HB. Static pressure-volume characteristics of lungs in normal males. J Appl Physiol. 1960;15:819–25.
Suarez CJ, Dintzis SM, Frevert CW. 9 - Respiratory. Comparative anatomy and histology. San Diego: Academic Press; 2012. p. 121–34.
Sylvester JT, Goldberg HS, Permutt S. The role of the vasculature in the regulation of cardiac output. Clin Chest Med. 1983;4:111–26.
Vaz Fragoso CA, Cain HC, Casaburi R, et al. Spirometry, static lung volumes, and diffusing capacity. Respir Care. 2017;62:1137–47.
Woodson BT. A method to describe the pharyngeal airway. Laryngoscope. 2015;125:1233–8.
Zeballos RJ, Weisman IM. Behind the scenes of cardiopulmonary exercise testing. Clin Chest Med. 1994;15:193–213.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2018 Springer International Publishing AG, part of Springer Nature
About this chapter

Cite this chapter
Thiboutot, J., Thompson, B.R., Brown, R.H. (2018). Introduction to the Structure and Function of the Lung. In: Kaminsky, D., Irvin, C. (eds) Pulmonary Function Testing. Respiratory Medicine. Humana Press, Cham. https://doi.org/10.1007/978-3-319-94159-2_1
Download citation
DOI: https://doi.org/10.1007/978-3-319-94159-2_1
Published:
Publisher Name: Humana Press, Cham
Print ISBN: 978-3-319-94158-5
Online ISBN: 978-3-319-94159-2
eBook Packages: MedicineMedicine (R0)