
Abstract
There is no doubt that for many years the threat of weapons of mass destruction (WMD) imposes a great concern on citizens as well as on nation leaders. President Bush recognized the possibility of a secret and sudden attack with chemical or nuclear weapons as the greatest threat before humanity [1]. Since the first use of chemical agents in modern era during World War I, very few examples were documented where non-conventional weapon (NCW) was used by a state. However, in the Middle-East region in recent years several chemical attacks have been carried out in Syria by the government forces against their opponents, and in the 1980s by Iraq forces against Kurd civilians. The response of the international community against these incidents was much more significant than the one given after conventional attacks that caused a higher death toll along the years of fighting. This reflects the fear and different attitude that people and governments have towards the use of NCW. The September 11, 2001 terror attack in New York was the turning point of modern terrorism. The large number of casualties, the serious economic damage, and the psychological effects of this “mega-terrorism event” were unprecedented. It was expected that this achievement of a single terror attack would encourage terror groups to mimic it by attempting more conventional mega-terrorism attacks, or using non-conventional materials that would cause the same effect [2]. Although seemingly NCW can be considered an ideal choice for terrorist organizations, only very few terrorist attacks using these materials have been carried out in the past [3]. Non-conventional mass-casualty events (MCE) may be caused by toxicological, radiation, or biological agent dissemination. The MCE may be of natural cause, like a global viral flu event (e.g., the Spanish flu in 1918–1920 with millions of deaths) or a MCE after a terrorism act like the Anthrax envelope scare in Boca Raton, Florida in 2001. Best known chemical incidents in a civilian setup are the attacks carried out in Japan by the Aum Shinrikyo (Supreme Trust) group in 1994–1995. In the Tokyo subway attack in 1995 which involved releasing sarin nerve gas, twelve were killed and thousands injured. In 2007, multiple terrorist bombings had been reported in Iraq using chlorine gas. Recently in 2018, a former Russian spy and his daughter were supposedly poisoned in London by a potent nerve gas. Toxicological incidents can occur not just by a terrorist act but also and even more often as an accident, for example an explosion in a chemical factory producing hazardous materials, or a road accident of a truck transferring such materials. Radiological materials can find their way to terrorist organizations that might use them to make a “dirty bomb.” This low-tech radiological weapon is actually a conventional explosive bomb with a radiation side effect. Although the radiation effect will probably be negligible compared to a nuclear bomb, it can induce a heavy emotional impact and neutralize large contaminated areas. Until now, only few terrorist attacks using radiation materials have been reported. In 1995 and 1998, two attempts of dirty bombs use by a Chechen group were thwarted. Another case is the radiation poisoning of Alexander Litvinenko, a former KGB agent, by ingestion of Polonium∗210. A radiation event may also be the result of an accident in a nuclear plant, in a medical isotopes imaging institution, or in a laboratory using radiation materials. In all the forms of non-conventional events, the victims may suffer from the combination of conventional and non-conventional injuries, or either one of these types of injury. Bio-terrorism is even rarer though it is also very tempting to terrorists to use. Different US security organizations as well as other governments share a global war against terror. That includes the fight to prevent the possible use of NCW by terror organizations. The efforts and resources are aimed on the four premises of deterrence, prevention, defense, and consequence management [4]. The fact that the incidental use of NCW is relatively so scarce is encouraging and emphasizes the vital continuous need for international supervision of the development, manufacture, and marketing of NCW, and for coordinated steps to prevent access by unauthorized groups to these agents. Unfortunately, there is always a chance that the ability and the motivation of a terrorist group will meet and will result in translating the potential into reality. The probability of such an event has even increased in the last decade after the disintegration of states like Libya, Iraq, and Syria that made their military NCW arsenal easily available to different terror organizations. In most if not all NCW attacks, the nation health system is almost immediately involved. As a consequence of the described situation, the civilian health system must be prepared to non-conventional incidents. This chapter delineates the challenges, preparedness, special equipment, and organizational requirements that a medical center faces when dealing with a non-conventional MCE.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


14.1 Background
There is no doubt that for many years the threat of weapons of mass destruction (WMD) imposes a great concern on citizens as well as on nation leaders. President Bush recognized the possibility of a secret and sudden attack with chemical or nuclear weapons as the greatest threat before humanity [1]. Since the first use of chemical agents in modern era during World War I, very few examples were documented where non-conventional weapon (NCW) was used by a state. However, in the Middle-East region in recent years several chemical attacks have been carried out in Syria by the government forces against their opponents, and in the 1980s by Iraq forces against Kurd civilians. The response of the international community against these incidents was much more significant than the one given after conventional attacks that caused a higher death toll along the years of fighting. This reflects the fear and different attitude that people and governments have towards the use of NCW. The September 11, 2001 terror attack in New York was the turning point of modern terrorism. The large number of casualties, the serious economic damage, and the psychological effects of this “mega-terrorism event” were unprecedented. It was expected that this achievement of a single terror attack would encourage terror groups to mimic it by attempting more conventional mega-terrorism attacks, or using non-conventional materials that would cause the same effect [2]. Although seemingly NCW can be considered an ideal choice for terrorist organizations, only very few terrorist attacks using these materials have been carried out in the past [3]. Non-conventional mass-casualty events (MCE) may be caused by toxicological, radiation, or biological agent dissemination. The MCE may be of natural cause, like a global viral flu event (e.g., the Spanish flu in 1918–1920 with millions of deaths) or a MCE after a terrorism act like the Anthrax envelope scare in Boca Raton, Florida in 2001. Best known chemical incidents in a civilian setup are the attacks carried out in Japan by the Aum Shinrikyo (Supreme Trust) group in 1994–1995. In the Tokyo subway attack in 1995 which involved releasing sarin nerve gas, twelve were killed and thousands injured. In 2007, multiple terrorist bombings had been reported in Iraq using chlorine gas. Recently in 2018, a former Russian spy and his daughter were supposedly poisoned in London by a potent nerve gas. Toxicological incidents can occur not just by a terrorist act but also and even more often as an accident, for example an explosion in a chemical factory producing hazardous materials, or a road accident of a truck transferring such materials. Radiological materials can find their way to terrorist organizations that might use them to make a “dirty bomb.” This low-tech radiological weapon is actually a conventional explosive bomb with a radiation side effect. Although the radiation effect will probably be negligible compared to a nuclear bomb, it can induce a heavy emotional impact and neutralize large contaminated areas. Until now, only few terrorist attacks using radiation materials have been reported. In 1995 and 1998, two attempts of dirty bombs use by a Chechen group were thwarted. Another case is the radiation poisoning of Alexander Litvinenko, a former KGB agent, by ingestion of Polonium∗210. A radiation event may also be the result of an accident in a nuclear plant, in a medical isotopes imaging institution, or in a laboratory using radiation materials. In all the forms of non-conventional events, the victims may suffer from the combination of conventional and non-conventional injuries, or either one of these types of injury. Bio-terrorism is even rarer though it is also very tempting to terrorists to use. Different US security organizations as well as other governments share a global war against terror. That includes the fight to prevent the possible use of NCW by terror organizations. The efforts and resources are aimed on the four premises of deterrence, prevention, defense, and consequence management [4]. The fact that the incidental use of NCW is relatively so scarce is encouraging and emphasizes the vital continuous need for international supervision of the development, manufacture, and marketing of NCW, and for coordinated steps to prevent access by unauthorized groups to these agents. Unfortunately, there is always a chance that the ability and the motivation of a terrorist group will meet and will result in translating the potential into reality. The probability of such an event has even increased in the last decade after the disintegration of states like Libya, Iraq, and Syria that made their military NCW arsenal easily available to different terror organizations. In most if not all NCW attacks, the nation health system is almost immediately involved. As a consequence of the described situation, the civilian health system must be prepared to non-conventional incidents. This chapter delineates the challenges, preparedness, special equipment, and organizational requirements that a medical center faces when dealing with a non-conventional MCE.
14.2 General Considerations
Terrorist act or an accident in an industrialized area may result in combined conventional and non-conventional injuries that may affect tens to thousands of people if it happens in a heavily populated area. The number of victims and the severity of their injuries depend on the population density, the type of agent, its quantity, its toxicity, and the meteorological conditions at the time of incident. Explosion and fire aggravate the agent effects, making the rescue efforts more complicated. Non-conventional incidents are fortunately rare but this fact just strengthen the need for awareness of health systems to such possibility and to prepare to it, and it requires the awareness of the medical teams in order to promptly identify an event once it occurs and to modify the management accordingly. As is true to all types of MCE, timely and rapid organization of the emergency medical services (EMS) and medical centers is crucial for an efficient and successful response. Medical centers should map and evaluate the risks of non-conventional event in their area. For example, the presence of a nuclear plant, medical or university laboratories using radiation compounds, traffic of trucks or trains loaded with hazardous materials, concrete threat of terrorism, etc. It is important to appoint a team to be in charge of organizing the standard operating procedures (SOP) protocols for each type of MCE, to assimilate and implement the knowledge and guidelines among the medical, paramedical, logistic, and assisting teams, and on keeping the preparedness of the hospital by performing periodical drills. It is important to remember that although it is recommended to follow the basic principles of MCE any single medical center needs to prepare its own SOP and the way it organizes and controls the situation by making the local necessary adaptations. Variables like the topography of the admitting area, available personnel in different daily times, size of the treatment area, capacity of the hospital, number of victims that can be managed in a single wave, mechanical ventilators availability, capacity of blood bank, availability of surgical rooms, intensive care beds, options for secondary evacuation of patients to other facilities, and so on may affect the way a certain hospital will establish its plan. The accepted evaluation in Israel is that the admitting surge capability of a hospital in a single wave of victims of MCE should be 20% of the total hospital beds during regular activity. The working assumption is that the admitting hospital itself is not contaminated. However, there are two scenarios for the initial management of non-conventional event. An “overt exposure situation” when it is clear from the pre-hospital phase that the injured are also contaminated by a toxic or radiological substance, as opposed to an “unknown exposure situation” when the fact of contamination is not initially identified. In the second scenario, patients enter the emergency department normally and contaminate the entire area and those who come in contact with them. Clear separation marked by a colored line on the floor should be made to sign the border between “dirty” and “clean” areas. The victims should be evacuated from the contaminated scene as fast as possible. Lifesaving procedures, undressing, cleansing, and treatment with antidote (if appropriate) will be done en route. Resources should not be expended on patients who have experienced a cardiac or respiratory arrest if there are large numbers of casualties requiring care above the capabilities of the health providers. Special care is given to health providers’ safety. Once a definite diagnosis has been made that a hazardous material is involved, special precautions should be followed including wearing specific protective gear for team members who come in contact with contaminated victims. It should be remembered that communication between team members that wear protective gear including gas masks and between this team and the person who controls the event may be problematic. Another special issue in coping with non-conventional event is that it is expected that a large number of healthy worried citizens and people suffering from acute stress reaction would flood the health system.
14.3 Toxicological/Chemical Event
EMS transfer casualties to the hospital, usually after the first decontamination process if available. This process at the scene is appropriate only in stable patients. Patients sustaining immediate life-threatening condition will be entered into a resuscitation bay without decontamination. A resuscitation area is allocated adjacent to the ambulance unloading point, or, as it is the case in our medical center, in a pre-designed “dirty” area inside the shock-trauma room. In such a case that part of the room becomes contaminated and is separated from the other bays. The team in the “dirty” area works wearing protective gear. Following the initial resuscitation, wet cleansing is performed and the patient will be transferred across to the “clean” areas of the emergency room for further treatment. The diagnosis and identification of involvement of toxic material can be based on early information from the scene or based on the clinical presentation of the first arriving patients. Upon the recognition of a toxic material an immediate contact is made with the toxicology expert, if there is one in the hospital, or with a National Toxicology Center to get more information about the hazardous material, its toxicity, special risks and the need for special protective gear, and the availability of an antidote. Another source of information (in Israel) may be the IDF Medical Corps and/or the Home-front Command. Updated contact routes to these agents must be available in the folder for this type of event. Since it is possible that a large number of patients will arrive prior to making the diagnosis of a toxic event, the entire emergency room could become contaminated. It is advisable to prepare for such situations a secondary remote area that will be able to serve for treating later on patients who underwent cleansing. All patients arriving to the hospital must be undressed prior to entering the emergency department. Undressing reduces the exposure to the toxic material by 90%. All contaminated clothes should be collected in HAZMAT plastic bags. After underdressing, the injured undergo wet cleansing. This is done in designated pre-installed external showers. Lying patients will be cleansed on fenestrated gurneys that allow drainage of the contaminated fluids. The body is washed out for 2–4 min and the eyes are flushed with water for 5 min. In a case that the treating team members complain on symptoms suggestive an exposure to toxic material, they should be managed like any other victim. Dry decontamination with absorbent materials as Fuller’s earth powder is indicated in cases of non-vaporizing phospho-organics or mustard gas. Wet decontamination will follow the dry (Figs. 14.1 and 14.2). Treatment with the appropriate antidote is given to all victims with symptoms. It is recommended to have a stockpile of automatic injectors of atropine and toxogonin in the emergency supplies of the hospital for phospho-organic compound events. Traumatic injuries should be treated as usual after completing the decontamination process.

Dry decontamination of a chemical material victim. A drill at Soroka University Medical Center

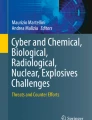
A paramedical staff personnel with bioprotective gear transferring a “patient” in an isolation chamber. A drill at Soroka University Medical Center
14.4 Radiation Event
The management is based on the protocols of a regular MCE with special emphasis on the unique characteristics of this scenario including monitoring and protection of health providers, and the monitoring, decontamination, and treatment of the victims. The management of patients who have been exposed to radiation should preferably be in designated centers with capabilities to provide complicated treatment for radiation burns, internal contamination, or for serious hematological outcome of the sub-acute phase of severe exposure including bone marrow transplantation. Resembling chemical event, radiological event may be “overt” or “unknown.” Due to the possibility of a dirty bomb it is now the instruction in Israel and the routine protocol at the Soroka Medical Center to monitor with hand-held radiation detectors every first 3–5 patients who arrive in MCE, to rule out the exposure to radioactive materials. The detectors are posted at the station of the triage nurse and nurses are trained to use them. The psychological effects of a radiation event are extreme and it is expected to receive an unusually large number of worried people and patients with acute stress reactions, so the medical center must be ready with supplementary teams of psychologists and social workers to support these patients. The victims might suffer from several types of damage which include conventional injuries, external radiation, internal radiation, and combined injuries. External radiation exposes the entire body or parts of it to ionizing radiation. The risks for the victim in the short term include acute radiation disease in cases of whole body exposure, and radiation burns in local exposures. The risks in the long term include increased risk for malignancy, harms to offspring, and tissue damage along the tract of the radiation. In these situations, there is no risk to the environment remote from the site of exposure or to the treating teams. In such situations there is no need for decontamination of the patients or to protect the team with special gear. External radioactive contamination is caused by the presence of radioactive material on the body. It may be contaminated liquid, powder, or shell fragments. The risk for the victim is to absorb the external contamination into the body through the respiratory system, the gastrointestinal tract, or through damaged skin. It can also cause local continuous injury to the skin. There is a mild to moderate risk to contaminate the environment and the team although the medical risk for the health providers is low. As a result, it is required to undress the patients as it reduces 90% of the contamination. The undressing should be done gently and the contaminated clothing sealed off in HAZMAT bags. The decontamination process must be also gentle to prevent sprinkling of water on other people and the contaminated water is collected in large plastic bags to prevent further environmental contamination. Team members that act in the “dirty” section at the admitting area including a triage physician, radiation controllers, and nurses that undress and decontaminate the patients should wear protective gear first. Teams that work in the “dirty” bays of the shock-trauma room where they manage the emergent cases that did not undergo initially undressing are also wearing protective gear. Team members who work in the contaminated areas should wear radiation dosimeters. Lifesaving procedures like intubation, decompression of a tension pneumothorax, or control of major bleeding are in priority to decontamination. The contaminated zone floor is covered by special PVC sheaths and these zones are separated from the clean areas by a colored line. It is strictly forbidden for personnel to cross the line. Once the management of a contaminated patient is completed and the patient is now clean, he is transferred from the team in the “dirty” area to another team in the clean zone. Internal contamination happens when radiating material enters the body through the respiratory system, the gastrointestinal tract, or damaged skin. The material is then partly accumulated and partly secreted from the body. The risk to the victim is to develop malignancies, damage to offspring, and rarely severe destruction of target organs. The risk to the team is very low and especially results from direct contact with contaminated secretions. The risk to environment is very low due to dilution of the victim’s secretions. Nevertheless, in the acute phase the assumption is that there is also an external contamination so it is required to wear protective gear and to decontaminate the victims. In later phases of the management, it is recommended to collect secretions in order to prevent potential environmental contamination, and to attempt to quantify the internal radioactive load. Using specific antidotes should be considered. In the past years, scientists have been seeking and testing new potential molecules that could be used to decorporate radionuclides in order to treat an internal contamination involving one or several radionuclides [5]. Patients and personnel that attend a radiation incident should receive Lugol iodine pills. Specific medical treatment for internal radioactive contamination may not be available routinely in most hospitals and it is part of the national preparedness to supply these agents to the medical centers that deal with a radiation event. In cases of combined conventional and radiation injuries, the patients should be treated as in regular trauma situations after the decontamination of the patients. The surgical management of radioactive shrapnel requires special attention. The radiation controllers measure the amount of radiation and give directives to the surgical team about safe distance from the agent and safe exposure time, for eventual team replacement. If radiation dose is not excessive, a lead apron and a set of double gloves is enough to protect the surgeon. Contaminated fragments are collected in special vials as all other radioactive materials for disposal.
14.5 Biological Event
This chapter refers only to a biological event that is generated by human usually as a terror act. A biological attack can cause severe mortality, morbidity, disability, impairment of normal life, and anxiety. The incident may progress into a prolonged crisis. The systematic response should aim at lifesaving, prevention of progressive spreading of the causative agent, and minimization of the effects on the routine life of the entire population. The significance of a biological event is far away from the medical center where it was identified. It becomes actually a national and even an international problem. In a case that the event is overt, for example a suspected envelope had been opened in a crowded office; the admitting team should be protected. Rapid identification of the causative agent is very important because the next steps of the management are dependent on it. Anthrax which is considered as one of the preferred infectious agents for biological warfare does not require the isolation of patients. Other diseases may require much complicated management including isolation of patients in special sections, negative pressure rooms, and transferring patients in specified chambers that provide total isolation (Fig. 14.3). Attempt must be made in order to identify all carriers and sick people as early as possible. These efforts are far beyond the medical center itself. Hospital SOP in a biological event is derived according to the magnitude of the event. In a limited event, the identification of contaminated patients is based on high suspicion of the nurses and physicians in the emergency room based on the symptoms and findings of patients. The suspected individuals are isolated in dedicated area (bio-event room) in the emergency room, the health providers who come in contact with the patients must wear protective gear, and all blood and other human secretions are sent to laboratory tests in biohazard plastic bags. Empiric treatment is started immediately and should be switched to targeted treatment as soon as the definitive diagnosis is made. The institutional infectious disease experts should be promptly involved in the management of the event, and the ministry of health should be informed. The victims are hospitalized in dedicated isolation rooms. In cases of MCE, the entire emergency room is transformed into a “bio emergency room” considering all sections are contaminated. In addition, due to the large numbers of victims a department or even several departments are designated as epidemic hospitalization ward(s).

Wet decontamination of a chemical material victim. A drill at Soroka University Medical Center
References
President Bush outlines Iraqi threat. October 2002. https://georgewbush-whitehouse.archives.gov/news/releases/2002/10/20021007-8.html.
Schweitzer Y. The age on non-conventional terrorism. Strateg Assess. 2003;6(1):26–31. http://www.inss.org.il/publication/the-age-of-non-conventional-terrorism/.
Kurz A. Non-conventional terrorism: availability and motivation. Strateg Assess. 2005;7(4):29–35. http://www.inss.org.il/publication/non-conventional-terrorism-availability-and-motivation/.
Moodie M. Reducing the biological threat: new thinking, new approaches. Special report 5. Washington: Chemical Biological Arms Control Institute (CBACI); 2003.
Steliou K, Faller DV, Pinkert CA, Irwin MH, Moos WH. Bioprotective carnitinoids: lipoic acid, butyrate, and mitochondria-targeting to treat radiation injury: mitochondrial drugs come of age. Drug Dev Res. 2015;76(4):167–75. https://doi.org/10.1002/ddr.21258.
Author information
Authors and Affiliations
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2020 Springer Nature Switzerland AG
About this chapter

Cite this chapter
Shaked, G., Czeiger, D., Sebbag, G. (2020). Preparedness to Non-conventional Incidents in the Civilian Medical Arena. In: Kluger, Y., Coccolini, F., Catena, F., Ansaloni, L. (eds) WSES Handbook of Mass Casualties Incidents Management. Hot Topics in Acute Care Surgery and Trauma. Springer, Cham. https://doi.org/10.1007/978-3-319-92345-1_14
Download citation
DOI: https://doi.org/10.1007/978-3-319-92345-1_14
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-92344-4
Online ISBN: 978-3-319-92345-1
eBook Packages: MedicineMedicine (R0)