
Abstract
Anxiety disorders are the most prevalent types of psychiatric disorders in the USA, affecting both children and adults at staggering rates. Moreover, roughly 25% of adolescents will be diagnosed with an anxiety disorder in his or her lifetime, suggesting that primary care physicians are more than likely to encounter these individuals on a frequent basis. Along these lines, it is imperative that primary care physicians recognize the symptomology endemic to anxiety and related disorders in children and adolescents. This chapter highlights the importance of recognizing the signs and symptoms of anxiety and related disorders in children and adolescents, differential diagnoses in children and adolescents, pharmacologic and behavioral interventions for managing anxiety and related symptoms, key measures available in assessing anxiety and related symptoms, and when to refer to other mental health providers.
Access provided by CONRICYT-eBooks. Download chapter PDF
Similar content being viewed by others


Keywords
- Anxiety disorders
- Separation anxiety
- Social anxiety
- Generalized anxiety
- Primary care
- Cognitive behavioral therapy
- CBT
- SSRIs
- SNRIs
- Benzodiazepines
Introduction
Anxiety disorders are the most prevalent types of psychiatric disorders in the USA, affecting both children and adults at staggering rates. Recognition of these disorders in the primary care setting can set the stage for timely diagnosis and appropriate therapeutic interventions as well as prevent potential misdiagnosis of mental illnesses with overlapping symptoms. There can be significant distress and impairment associated with anxiety disorders, and effective treatment can be life changing. Given the targeted nature of this text, this chapter will focus on the anxiety disorders that are most likely to be encountered in the pediatric primary care setting: social anxiety disorder, separation anxiety disorder, and generalized anxiety disorder.
Brief Review of Epidemiology and Pathophysiology
In the USA, anxiety disorders are the most common psychiatric conditions in both adults and children, affecting roughly 40 million Americans [1,2,3]. Though anxiety disorders are very treatable, only one-third of those suffering from an anxiety disorder receive treatment [4]. Moreover, 25% of adolescents will be diagnosed with an anxiety disorder in his or her lifetime [5]. Though anxiety symptomology is relatively consistent in its phenotypic expression , there are undoubtedly variations in the manifestation of these symptoms in children and adolescents for a number of reasons including developmental factors , cognitive factors , differences in child-specific antecedents (“triggers”)/maintenance factors , and other factors that vary from patient to patient.
Diagnosis and Key Components of History
Anxiety disorders share more commonalities in presentation than disparities. Thus, children and adolescents presenting with separation anxiety, social anxiety, and worry (GAD) often present in a consistent fashion. All three of these disorders are often manifested through school refusal or premature departure from school [6], somatic complaints (stomachaches, heart palpitations, hot/cold flushes), irritability, sleep disturbance, restlessness, frequent reassurance seeking toward their parents, and avoidance behavior [6].
Significant alteration from previous observations of functioning is an important component to identify when assessing the child or adolescent’s history since caregiver report is essential in aiding diagnosis. Since children of anxious parents are three to seven times more likely than children of non-anxious parents to have an anxiety disorder [1, 7, 8], being mindful of parental anxiety and potential parental modeling of distress is an important consideration when assessing child anxiety. Diagnostic criteria for all anxiety and related disorders require the symptoms to cause significant distress and impairment.
Separation Anxiety Disorder
Separation anxiety disorder is characterized by excessive anxiety about being away from a loved one, particularly a caregiver. The child is often worried about a negative event happening to the caregiver or a negative event happening to the child. A child with normal separation concerns may express “missing” the caregiver when he/she goes on an extended business trip, whereas a child suffering from separation anxiety frets about the absence of a caregiver for an extended period of time on a frequent basis, even during the most mundane situations (e.g., if the child is invited to a sleepover, the child is at school and parent is driving several hours away for work, or the parent is away from the child for a few hours). The child with separation anxiety may also frequently worry about being kidnapped or refuse to attend school due to anxiety about something bad happening to the caregiver. Additionally, the child with separation anxiety may also experience nightmares and seek frequent reassurance about the parent’s whereabouts.
Social Anxiety Disorder
Social anxiety disorder involves a persistent fear and anxiety about social situations where negative evaluation may occur. Though it is normal to be wary of strangers and novel situations (such as when meeting a new person or being nervous about speaking in front of the class), the socially anxious child may do any of the following: cry excessively about presenting in front of the class to the point of being sick and not attending school, avoid sporting events due to anxiety about being made fun of by peers, have very little social interaction with peers in general, and complain of somatic complaints weeks in advance before a presentation. Social anxiety may also manifest as significant performance anxiety before participating in sporting though the socially anxious child “plays well” during practice.
Generalized Anxiety Disorder
Generalized anxiety disorder is characterized by significant anxiety that leads to excessive worry. Normal concerns that are not driven by chronic levels of anxiety lead to effective problem solving. For example, a child experiencing normal levels of anxiety may worry about an upcoming exam but view the anxiety as an emotion that is helpful by prompting the child to study. However, the child with chronic worry may worry about a number of areas, even if things are going well. For example, the worried child may worry about getting to school on time, worry about making mistakes on assignments, become “frozen” when making everyday decisions, and seek frequent reassurance from a caregiver about whether he/she will be able to engage in certain activities when on a trip. The worried child also experiences sleep disturbance, difficulty concentrating, fatigue, and irritability.
Confounders and Comorbidities
Due to the restlessness and impaired concentration often associated with both anxiety and impulsivity, ADHD is a significant differential diagnosis for anxiety in children and adolescents. Though restlessness is a symptom of both ADHD and anxiety, anxiety-associated restlessness is associated with more subjective distress, somatic complaints, and avoidance behaviors. The inattention often found in ADHD tends to be more consistent, particularly in school settings. Difficulty concentrating as a symptom of anxiety, however, tends to be the result of the mind being occupied by worried thoughts about school, loved ones, social relationships, and other factors. Depression is a frequent comorbid diagnosis with anxiety disorders in children and adolescents. Determining whether symptoms of depression are present in addition to anxiety is paramount when assessing the child or adolescent.
Anxiety in children commonly manifests with somatic symptoms such as headaches, abdominal pain, shortness of breath, chest pain, and dizziness. A thorough medical workup should be performed on each patient, and medical problems such as migraine headaches, celiac disease, Gastroesophageal reflux disease (GERD), mitral valve prolapse, asthma, and other medical disorders should be ruled out rather than assuming the symptoms are solely manifestations of anxiety. Comorbidity with such conditions and anxiety can most certainly occur, and children with chronic medical issues are at increased risk for mental illness.
Substance use should always be a consideration. Intoxication with stimulant prescription or street drugs and withdrawal from sedatives such as opiates to benzodiazepines to alcohol can very much mirror anxiety symptoms. If benzodiazepines are being abused, there may even be interdose anxiety that the patient is experiencing. In certain patients, marijuana use can precede the onset of severe anxiety symptoms [9]. Patients with substance use disorders will many times not have the usual triggers that are associated with typical anxieties in children and adolescents. Symptoms may also be greatly out of proportion to what is typically seen and quite treatment resistant [10].
Screening and Measures
Given the frequent comorbidity of anxiety and depression, screening for the other is recommended whenever there is clinical suspicion of either. Table 11.1 displays commonly used screening assessment tools for anxiety and depression in children and adolescents. Additionally, all youth with anxiety symptoms should be screened for trauma, depression, and substance use disorders. Please refer to Fig. 15.1 in this text’s Substance Use Disorder (SUD) chapter for the CRAFFT, the recommended SUD screening tool.

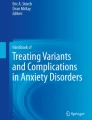
CBT model: the bidirectional relationship between thoughts, feelings/physical sensations, and behaviors
Initial Management
Psychosocial and Behavioral Interventions
Behaviorally, it is important to reiterate the importance of eliminating avoidance behavior when managing anxiety and related disorders in children and adolescents. Avoidance works in the short-term, so it can be very reinforcing. The problem is that it is associated with significant impairment and robs the youth of the opportunity to realize that things would not turn out as badly as the youth thought they would. Thus, attending school, giving speeches in front of classmates, interacting with others, and eliminating worry concerns are necessary targets of treatment. Though the child or adolescent may report that he/she is unable to function in the particular social situation, assure the caregiver that gradual “exposure” back into the currently feared situation will be essential in eliminating significant distress and impairment.
Ideally, this is achieved in collaboration with a mental health professional trained in cognitive behavioral therapy (CBT), the gold standard psychological intervention for anxiety disorders (see Fig. 11.1). Of note, in collaborative care models, depending on licensure, training, and state regulations, the behavioral care manager may be able to initiate psychotherapy. Psychotherapy can be helpful as children who are prone to anxiety and related symptoms struggle in two specific areas: (a) negative, unrealistic thoughts about themselves, their emotions, and the world around them and (b) attempts to avoid anxiety-provoking situations as well as strong, negative emotions. As such, many children with anxiety have thoughts that include “thinking errors” that create more anxiety than necessary in many harmless situations. Examples include “mind reading” (e.g., “they will think I’m an idiot”), fortune telling (e.g., “I’m going to fail the exam”), and catastrophizing (e.g., “this always happens to me!” or “this is the worst paper ever!”).
CBT contains an effective treatment component known as cognitive restructuring that teaches the child or adolescent that thoughts are “guesses” not “facts” in addition to understanding the connections between the thought, feeling/physical sensations, and resultant behaviors. Additionally, Socratic questions can be used to assist the child or adolescent in challenging unhelpful thoughts and creating more flexible thoughts used to ward off anxiety. Examples include “What’s the evidence that this negative event will occur?” “Is the negative prediction being driven by anxiety?” “Is the patient 100% sure this negative outcome will occur?” “What’s the worst that can happen and can the patient cope with that?” “What’s happened in the past?”
Relaxation and mindfulness techniques can be additionally helpful in alleviating much of the physiological arousal associated with anxiety and worry. Of note, this text’s Depression chapter includes a brief discussion of some apps that may be helpful adjuncts in these interventions. A mindfulness approach can be very helpful in assisting a child or adolescent to focus on the present moment rather than engage in worry, avoidance, or other behaviors driven by distressing emotional states. One strategy in assisting the child or adolescent with being more aware of his or her emotion in real time, or anchoring technique, is called nonjudgmental awareness. The child or adolescent begins with a few diaphragmatic breaths (e.g., inhale for 4 s, hold the breath for 5 s, and exhale for 6 s) followed by simply becoming “aware” of one’s thoughts, feelings/physical sensations, and behaviors as they are occurring in the present moment.
Finally, one of the most significant factors in effectively managing anxiety in children and adolescents is to provide the caregivers information about helpful strategies to implement at home. Please see Table 11.2 for key points to include while you are educating the patient’s family.
Pharmacologic Interventions
In the pharmacological treatment of anxiety in children, the goal is to decrease the overall burden of anxiety. While medications are certainly not the center of treatment for children, they can be helpful in decreasing the anxiety to the point where the patient can start to face it in their day-to-day life and deal with it in therapy. In child psychiatry, the mantra for medication treatment is “Start low, go slow.” This helps to minimize potential side effects of medications. Youth with anxiety disorders may be even more distressed by physical side effects than their anxiety disorder, particularly in the window before therapeutic effect has taken place.
Selective serotonin reuptake inhibitor (SSRI) antidepressants are first-line psychiatric medications for anxiety disorders in children and adolescents. Unfortunately, SSRIs and most of the other treatments for anxiety typically do not work immediately, and it is important to set expectations about the timeframe for effect and what patients should expect. Treating anxiety with medications is not like treating ADHD, where there is an almost immediate robust response to a therapeutic dose. At the onset of treatment, parents and children should be told that these medications must be taken daily, will work better over time, and may take 2–3 weeks to show any effect and up to 6 weeks to show their full effects at a given dose. As long as there are no unbearable side effects, it is important to keep taking the medication consistently to see if a response is achieved and push through the doses. Despite the daunting nature of the list of possible side effects, most people tolerate SSRIs and serotonin-norepinephrine re-uptake inhibitors (SNRIs) very well. Table 11.3 provides a quick reference for information about SSRIs.
Please note that due to the relative dearth of studies regarding medication in children and adolescents compared to studies in adults, pediatric prescribing is often “off label.” While this is acceptable and often quite necessary, it must be explained to parents and patients ahead of time [17]. Of note, all antidepressants used in children and adolescents carry a black box warning from the FDA regarding suicidal thoughts and behaviors. Please refer to the Pharmacologic Interventions section of this text’s Depression chapter as well as this text’s Medicolegal Issues in Prescribing Medications to Children and Adolescents chapter for additional information when starting an antidepressant in a child, adolescent, or young adult for any reason. The Depression chapter includes a discussion of common antidepressant side effects, their associated black box warning regarding suicidal ideation, and Table 10.6, which includes talking points for parents about initiation of antidepressants.
Selective Serotonin Reuptake Inhibitors (SSRIs)
Due to their demonstrated efficacy in treating anxiety disorders and the fact that they are relatively well tolerated, SSRIs are the most widely used medications for anxiety disorders in children and adolescents. Common medication class side effects include headaches, nausea, vomiting, light-headedness, appetite changes, weight changes, sedation, palpitations, increased blood pressure, tremor, akathisia, sexual dysfunction, lose stool, and constipation. Monitoring for serotonin syndrome is indicated, especially when using higher doses and whenever there is polypharmacy.
Serotonin-Norepinephrine Reuptake Inhibitors (SNRIs)
Two of the medications in this class are FDA approved for anxiety disorders in children and adolescents; however, SNRIs may not be as effective or well tolerated for comorbid child and adolescent depression as fluoxetine, an SSRI medication [25]. Common class side effects include headaches, nausea, vomiting, light-headedness, appetite changes, weight changes, sedation, palpitatvions, increased blood pressure, tremor, akathisia, sexual dysfunction, lose stool, and constipation. Monitoring for serotonin syndrome is indicated, especially when using higher doses and whenever there is polypharmacy.
Additional Medication Classes for Consideration
After first-line, FDA-approved treatments with relatively benign side effect profiles have been tried and have either not worked or caused intolerable side effects, alternative agents may be pursued. Note that the risk/benefit ratio and course of treatment necessitating these choices should be reviewed with families prior to their use.
Tricyclic antidepressants (TCAs) have plentiful studies supporting their use in anxiety disorders; however, overall they appear to be more effective in adults than in children and adolescents. They can be helpful for patients who have failed SSRIs and SNRIs. TCAs, however, are “dirtier” drug in that they tend to modulate receptors outside of serotonin and norepinephrine, such as anticholinergic receptors and histamine receptors. This can give them therapeutic advantages but also leaves them more prone to side effects, some of which are serious. TCAs used in children and adolescents include clomipramine, desipramine, and imipramine. Of note, TCAs can be fatal in overdose, which is an issue of clinical significance given the high rates of depression and anxiety comorbidity.
Benzodiazepines may interfere with learning, and they are also potential substances of abuse. Additionally, controlled trials do not support the use of benzodiazepines in children for anxiety [26, 27]. For these reasons, benzodiazepines are typically used either as short-term interventions for adjunctive treatment or for severe, functionally impairing anxiety symptoms. Compared to adults, adolescents are vulnerable to misusing benzodiazepines due to less well-developed executive functioning, decision-making, and impulse control. Also, the increased risk of death with the combination of benzodiazepines and other drugs of abuse, opiates in particular given the recent opioid epidemic, should be weighed prior to use. If there is a history of substance use/abuse in the patient, benzodiazepines should be avoided. Note that children, especially younger children, are more likely to have a paradoxical reaction to benzodiazepines . As with all drugs with the potential for abuse, formulations with faster onset and shorter duration of action can be more problematic.
When to Refer
Two primary factors determine when it is appropriate to refer the child or adolescent for additional treatment options. First, a referral is warranted when parental report indicates that the symptoms have created significant personal distress and impairment in the child’s functioning. This may be indicated by parental observation, teacher report, a decline in academic functioning, restricted social relationships, an increase in risky behavior, isolation, and other behaviors that are abnormal based on the caregiver’s typical observations. Second, subjective distress as noted by the child or adolescent would indicate an additional reason to refer. Additionally, if initial interventions in the primary care setting do not yield an adequate treatment response, referral should be initiated.
Key Considerations for Follow-Up
Monitoring the effectiveness of treatment is an inexact science. As patients feel better, they generally report feeling calmer and less stressed. Additionally, at the time of diagnosis and treatment initiation, it is good to identify target symptoms to follow, such as somatic complaints, days of school achieved, number and severity of panic attacks in a given time span, improvement in sleep, or other markers that can be documented. As anxiety has likely kept patients from participating in their general interests and activities, a return to these exploits is seen as a great sign of progress. Rating scales can also be used at the beginning of treatment and along the course of treatment in order to measure the anxiety at baseline and its improvement as treatment moves forward. Short rating scales can be done in the waiting room prior to each appointment.
Determining whether the caregiver has followed recommendations for additional treatment is a key consideration when following up with the anxious child or adolescent. Considering there is a familial transmission of anxiety [1, 7, 8], inquiring as to whether the family has considered psychological and/or psychiatric treatment is essential due to the debilitating nature of avoidance behavior and functional impair- ment in the anxious family. Table 11.4 includes some key points for parental/family education about anxiety in children and adolescents.
Summary
Anxiety disorders in children and adolescents often first present in the primary care setting. Recognizing the symptoms early can lead to early interventions and decrease distress and impairment of function . Symptoms of anxiety can alter a child’s cognitive, behavioral, and physical state and lead to avoidance behaviors that are then reinforced by the short-term relief from anxiety they provide. Addressing avoidance is a key aspect of psychosocial treatment. While psychotherapeutic and behavioral interventions are the first-line therapeutic modalities for addressing anxiety symptoms, psychopharmacology can be helpful and, when symptoms are severe, is indicated. Comorbid depression is common with anxiety disorders, and all youth with anxiety disorders should be screened for SUDs and trauma.
References
Chapman LK, Petrie J, Vines L, Durrett E. The co-occurrence of anxiety disorders in African American parents and their children. J Anxiety Disord. 2012;26(1):65–70.
Greenburg PE, Tamar S, Kessler RC, Finkelstein SN, Berndt ER, Davidson JR, et al. The economic burden of anxiety disorders in the 1990s. J Clin Psych. 1999;60(4):27–435.
Issakidis C, Sanderson K, Corry J, Andrews G, Lapsley H. Modeling the population cost-effectiveness of current and evidenced-based optimal treatment for anxiety disorders. Psych Med. 2004;34(1):19–35.
Young AS, Klap R, Shoai R, Wells KB. Persistent depression and anxiety in the United States: prevalence and quality of care. Psychiatr Serv. 2008;59(12):1391–8.
Costello EJ, Mustillo S, Erkanli A, Keeler G, Angold A. Prevalence and development of psychiatric disorders in childhood and adolescents. Arch Gen Psychiatry. 2003;60:837–44.
Kearney CA, Albano AM. When children refuse school: a cognitive-behavioral approach. Treatments that work. Oxford: Oxford University Press; 2007.
Chapman LK, Kertz SJ, Zurlage MM, Woodruff-Borden J. A confirmatory factor analysis of specific phobia domains in African American and Caucasian American young adults. J Anxiety Disord. 2008;22(5):763–71.
Chapman LK, Kertz SJ, Woodruff-Borden J. A structural equation model analysis of perceived control and psychological distress on worry among African American and European American young adults. J Anxiety Disord. 2009;23:69–76.
Duperrouzel J, Hawes SW, Lopez-Quintero C, Pacheco-Colon I, Comer J, Gonzalez R. The association between adolescent cannabis use and anxiety: a parallel process analysis. Addict Behav. 2017;78:107–13.
Martin A, Scahill L, Kratochvil CJ. Pediatric psychopharmacology. Principals and practice. Oxford: Oxford University Press; 2011. 38-49, 480-515.
Pagano M, Murphy JM, Pedersen M, et al. Screening for psychosocial problems in 4–5 year olds during routine EPSDT examinations: validity and reliability in a Mexican-American sample. Clin Pediatr. 1996;35(3):139–46.
Kassam-Adams N. The acute stress checklist for children (ASC-Kids): development of a child self-report measure. J Trauma Stress. 2006;19(1):129–39.
Chorpita BF, Tracey SA, Brown TA, Collica TJ, Barlow DH. Assessment of worry in children and adolescents: an adaptation of the Penn State Worry Questionnaire. Behav Res Ther. 1997;35(6):569–81.
Chorpita BF, Yim LM, Moffitt CE, Umemoto LA, Francis SE. Assessment of symptoms of DSM-IV anxiety and depression in children: a revised child anxiety and depression scale. Behav Res Ther. 2000;38:835–55.
Birmaher B, Brent DA, Chiappetta L, Bridge J, Monga S, Baugher M. Psychometric properties of the screen for child anxiety related emotional disorders (SCARED): a replication study. J Am Acad Child Adolesc Psychiatr. 1999;38:1230–6.
Spence SH. Structure of anxiety symptoms among children: a confirmatory factor-analytic study. J Abnorm Psych. 1997;106(2):280–97.
Martin A, Volkmar FR. Lewis’s child and adolescent psychiatry, a comprehensive textbook. Philadelphia: Lippincott Williams & Wilkins; 2007. p. 509–531,568.
Dulcan MK, editor. Depressive and disruptive mood dysregulation disorders. 2nd ed. Washington: American Psychiatric Association Publishing; 2016.
Birmaher B, Brent D. Practice parameter for the assessment and treatment of children and adolescents with depressive disorders. J Am Acad Child Adolesc Psychiatry. 2007;46(11):1503–26.
Martin A, Volkmar FR, Lewis M. Lewis’s child and adolescent psychiatry: a comprehensive textbook. Philadelphia: Wolters Kluwer Health/Lippincott Williams & Wilkins; 2007.
Labbate LAF, Maurizio R, Rosenbaum JF, Arana GW. Handbook of psychiatric drug therapy. Philadelphia: Lippincott Williams & Wilkins (LWW); 2009.
Valenstein M, Hyungjin M, et al. Antidepressant agents and suicide death among US Department of veterans affairs patients in depression treatment. J Clin Psychopharmacol. 2012;32(3):346–53. https://doi.org/10.1097/JCP.0b013e3182539f11.
Mrakotsky C, Masek B, Biederman J, et al. prospective open-label pilot trial of mirtazapine in children and adolescents with social phobia. J Anxiety Disord. 2008;22:88–97.
Stawn JR, Mills JA, Cornwall GJ, Mossman SA, Varney ST, Keshin BR, Croaarkin PE. J Child Adolesc Psychopharmacol. 2018;28(1):2–9. https://doi.org/10.1089/cap.2017.0060. Epub 2017 Aug 28.
Cipriania A, Del Zhou X, Giovane C, et al. Comparative efficacy and tolerability of antidepressants for major depressive disorder in children and adolescents: a network meta-analysis. Lancet. 2016;388(10047):881–90. https://doi.org/10.1016/S0140-6736(16)30385-3. Epub 2016 Jun 8.
Bernstein GA, Garfinkel BD, Borchardt CM. Comparative studies of pharmacotherapy for school refusal. J Am Acad Child Adolesc Psychiatry. 1990;29:773–81 [PubMed].
Graae F, Milner J, Rizzotto L, et al. Clonazepam in childhood anxiety disorders. J Am Acad Child Adolesc Psychiatry. 1994;33:372–6 [PubMed].
Author information
Authors and Affiliations
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2018 Springer International Publishing AG, part of Springer Nature
About this chapter

Cite this chapter
Chapman, L.K., Nichols, A. (2018). Anxiety. In: Vinson, S., Vinson, E. (eds) Pediatric Mental Health for Primary Care Providers. Springer, Cham. https://doi.org/10.1007/978-3-319-90350-7_11
Download citation
DOI: https://doi.org/10.1007/978-3-319-90350-7_11
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-90349-1
Online ISBN: 978-3-319-90350-7
eBook Packages: MedicineMedicine (R0)