
Abstract
Evidence from animal studies indicates the importance of the dorsomedial and medial pontine tegmentum and the ventromedial medulla in maintaining muscle tone inhibition during REM sleep; however, the symptoms in animals with lesions in these areas do not fully mimic the symptoms of human REM sleep behavior disorder (RBD). This chapter summarizes the findings in our laboratory and offers a hypothesis on the neural network involved in the modulation of motor activity in sleep, the neural structures participating in the generation of RBD, and a hypothetical link between RBD and Parkinsonism.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others

Keywords
1 Introduction
REM sleep behavior disorder (RBD) is characterized by dream-enacting motor behaviors during REM sleep, which is normally quiescent with a display of brief myoclonic twitches amid prevailing muscle paralysis throughout the body. The majority of older adult RBD patients in one series experienced episodes of punching (87%), kicking (82%), falling out of bed (77%), gesturing (73%), or knocking over the nightstand (67%) during vivid dreams. Nearly all patients also reported vocalizations, most commonly talking (96%), screaming (90%), and moaning (64%). In both men and women, about 60% of patients and 20% of bed partners had sustained injuries [1]. Long before RBD was formally described as a parasomnia in humans in 1986 [2], the polygraphic hallmark of this disease, REM sleep without atonia, had been extensively studied in animals. These studies were pioneered by Michel Jouvet, who first identified the physiological features including muscle atonia during REM sleep (or “paradoxical sleep” as coined by Jouvet) in the cat in 1959 and described the “oneiric” or hallucinatory behaviors during REM sleep in those cats that recovered from bilateral electrolytic lesions of the dorsolateral pontine tegmentum, which included locus coeruleus and adjacent areas [3]. The abnormal behaviors during REM sleep in the cat elicited by lesions in pontine tegmentum range from simple movements such as body jerks to more complex, coordinated behaviors of hissing, piloerection, pouncing, attacking non-existing prey, walking, and running.
2 Brainstem Circuitry for REM Sleep Atonia
The level of tonic activity in skeletal muscles, except for the diaphragm and extraocular muscles, is low in NREM sleep and minimal in REM sleep. Cranial and spinal motor nuclei receive extensive projections from the caudal brainstem, the medulla and the pons (Fig. 42.1). Magoun and Rhines [4] first showed that the medial and lateral portion of the medulla has inhibitory and excitatory effects on motor activity, respectively. Electrical stimulation of the medial medulla inhibits both phasic and tonic motor activities such as flexor patellar and blink reflexes, motor responses induced by stimulation of the motor cortex, and muscle tone in the decerebrate animal. On the other hand, stimulation of the lateral medulla increases the patellar reflex [4]. The medullary inhibitory area in the cat includes the nucleus gigantocellularis (NGC) in the dorsal and the nucleus magnocellularis (NMC; nucleus gigantocellularis alpha in the rodents) in the ventral rostral medial medulla, as well as the nucleus paramedianus (NPM) in the caudal medial medulla. The motor inhibitory area is not limited to the medial medulla but extends to the medial pons and the ventral midbrain [5]. Muscle tone is decreased with electrical stimulation of the medial pons (the pontine inhibitory area (PIA)), the rostral ventral paralemniscal field of the pons, the pedunculopontine nucleus (PPT), the retrorubral nucleus, or the substantia nigra [5].

A hypothetical neural circuit and transmitters involved in the control of REM sleep atonia . Solid and dashed lines represent excitatory and inhibitory effects on the target site. Glutamatergic and cholinergic activation of the pontine inhibitory area (PIA) elicits muscle atonia, which results from a combination of activation of GABAergic and glycinergic neurons in the nucleus magnocellularis (NMC) of the rostral ventromedial medulla and inactivation of noradrenergic neurons in the pontine locus coeruleus and medullary raphe serotonergic neurons. The pontine glutamatergic and cholinergic innervations originate from the ventral mesopontine junction (VMPJ) and pedunculopontine nucleus (PPT). Neurons in the VMPJ and PPT also project to the NMC, as well as to the nucleus paramedianus (NPM) of the caudal medial medulla. IO inferior olivary nucleus, LC locus coeruleus, NGC nucleus gigantocellularis, P pyramidal tract, PAG periaqueductal gray, R medullary raphe nucleus, unknown (E) and unknown (I): transmitter that exerts excitatory and inhibitory effect on the target site
Anatomically, the NMC receives glutamatergic projections from the PIA (Fig. 42.1), the ventral paralemniscal tegmental field, the retrorubral nucleus, and the caudal ventral mesencephalic reticular formation [6]. The NPM receives cholinergic projections from the PPT and dorsolateral tegmental nucleus [7]. Three distinct areas, the glutamatergic-receptive NMC, the cholinergic-receptive NPM , and the glutamatergic-/cholinergic-insensitive NGC, can be identified by their motor response to chemical injections into the medial medulla (Fig. 42.2). Injection of non-NMDA receptor agonists, AMPA, and kainic acid into the NMC or injection of acetylcholine into the NPM elicits muscle atonia in decerebrate animals [8, 9]. These effects can be reversed by their antagonists, 6-cyano-7-nitroquinoxaline-2,3-dione (CNQX) and 6-cyano-7-dinitroquinoxaline-2,3-dione (DNQX) injected into the NMC or atropine injected into the NPM [9, 10]. The induced suppression of muscle tone by chemical injection has also been observed in the behaving animal.

Schematic map of pontomedullary inhibitory areas . Electrical stimulation produced atonia at all the points mapped. The upper and bottom panels represent glutamatergic and cholinergic agonist injection, respectively. Filled symbols (circles and triangles) represent points at which drug injections decreased muscle tone. Open circles represent points at which drug injections increased or produced no change in muscle tone. 4V fourth ventricle, 5ME mesencephalic trigeminal tract, 6 abducens nucleus, 7G genu of the facial nerve, PG pontine gray, PT pyramidal tract, SO superior olivary nucleus, T nucleus of the trapezoid body, TB trapezoid body (From Lai and Siegel, J Neurosci 8: 4790–4796, 1988)
Glutamate injected into the NMC or acetylcholine injected into the NPM in wakefulness decreases muscle tone and suppresses eye movement without changing EEG activity in the chronic cat [10], suggesting that neuronal activity of the NMC and NPM is involved in the control of eye movement and motor activity, but not the EEG activity in sleep. Furthermore, the suppression of eye movement and muscle tone, resembling NREM sleep, by activation of NMC or NPM, indicates that neurons of the medial medulla may start to increase firing in NREM sleep resulting in a quiescent state of motor activity. The increased medial medullary neuronal activity continues and reaches its maximum in REM sleep. REM-on neurons have been recorded in the NMC and NPM [11]. In addition to the inhibition of tonic motor activity, the NMC may also be involved in the control of phasic motor activity. Microinjection of an NMDA agonist into the NMC elicits phasic motor events including rhythmic locomotor-like activity in the decerebrate animals , and this effect can be attenuated by d,l-2-amino-5-phosphonovaleric acid (APV) [8, 9].
The PIA receives cholinergic projections from the PPT and glutamatergic projections from the retrorubral nucleus and the PPT (Fig. 42.1) [12]. In contrast to the medial medulla, which can only be activated by either glutamatergic (NMC) or cholinergic (NPM) agonist, the PIA can be activated by both glutamatergic and cholinergic agonists (Fig. 42.2). AMPA or kainic acid injected to the PIA generates muscle atonia, whereas NMDA injected into it increases muscle tone. The pontine inhibitory and excitatory effects on motor activity can be blocked by CNQX/DNQX and APV, respectively [8]. Injection of cholinergic agonists, carbachol and acetylcholine, into the PIA elicits muscle atonia in decerebrate animals [8, 9]. However, muscle atonia induced by activation of the PIA can be reversed by the glutamatergic antagonist, γ-d-glutamylglycine, injected into the NMC, indicating that PIA activation-induced muscle atonia is mediated through the NMC [10] (Fig. 42.2). Indeed, anatomical study using retrograde transport tracer WGA-HRP combined with glutamate immunohistochemistry showed that glutamatergic neurons of the PIA project to the NMC [6]. Using unit recording combined with antidromic stimulation, Sakai et al. [13] demonstrated that REM-on cells of the pons activate neuronal activity of the NMC during REM sleep. Furthermore, NMC lesions result in REM sleep without atonia [14]. Inactivation of the PIA fails to reduce the inhibitory effect of the NMC stimulation on motor activity [4, 15], indicating that activation of NMC alone is capable of suppressing muscle tone.
The major facilitatory systems in the caudal brainstem projecting to the motor nuclei consist of the lateral portion of the medulla [4], medullary raphe nuclei [16], and noradrenergic locus coeruleus [17]. Inactivation of the facilitatory system may thus suppress muscle tone, as it is seen during cataplectic attacks [18]. However, activation of the inhibitory system or inactivation of the facilitatory system alone may not be sufficient to generate and maintain global muscle atonia during REM sleep. Using the decerebrate preparation and dialysate collection and HPLC analysis, electrical or chemical stimulation was applied in the PIA or NMC; while extracellular fluid was collected from the spinal ventral horn and hypoglossal nucleus by microdialysis, Lai et al. [19, 20] and Kodama et al. [21] demonstrated that an increase in inhibitory neurotransmitters, GABA and glycine, and a decrease in excitatory neurotransmitters, norepinephrine and serotonin, are found in the spinal ventral horn and hypoglossal nucleus.
These results clearly indicated that a combination of activation of the inhibitory system and inactivation of the facilitatory system is required in initiating and maintaining global muscle atonia in REM sleep (Fig. 42.1). The source of GABA and glycine may be the NMC. It has been shown that GABAergic and glycinergic neurons of the NMC project to the spinal cord [22]. The decrease in norepinephrine release in the spinal ventral horn and hypoglassal nucleus may result from the cessation of neuronal firing in the locus coeruleus. Activation of the PIA or NMC has been shown to inhibit neuronal activity of the locus coeruleus [23], which projects to the spinal cord [17]. The decrease in serotonin release during PIA or NMC stimulation may result from activation of the NMC GABAergic neuronal activity , which in turn inhibits the firing of raphe serotonergic spinal projecting neurons [16].
3 Brainstem Regions Involved in RBD Generation
While evidence strongly supports the idea that the integrity of the PIA-NMC-spinal ventral horn pathway is required for generating muscle tone suppression during REM sleep, the symptoms of the animals with lesions in this pathway do not fully mimic the symptoms of human RBD. First, idiopathic RBD patients have no change or sometimes longer total time in REM sleep [2], whereas PIA- or NMC-lesioned animals often show massive reduction in REM sleep and/or in the duration of REM sleep episodes [24, 25]. Second, the abnormal motor symptoms in PIA- or NMC-lesioned animals seemed to be limited to REM sleep episodes, while phasic motor activities in NREM sleep, such as periodic limb movements (PLMs) or increased phasic twitches, are prevalent in RBD patients [26]. Thus, an animal model of RBD that expresses all the characteristics of RBD in humans is critically important for understanding the mechanisms underlying all of the manifestations of RBD.
3.1 The Caudal Ventral Mesopontine Junction
Based on our study of decerebrate animals, we have speculated that the ventral mesopontine junction (VMPJ) may be involved in the generation of RBD. The VMPJ includes the caudal portion of the dopaminergic retrorubral nucleus, substantia nigra, and ventral tegmental area (VTA), as well as the ventral paralemniscal tegmental field of the pons. Electrical stimulation of the caudal part of the VMPJ (C-VMPJ) including the ventral paralemniscal tegmental field of the pons and caudal retrorubral nucleus of the midbrain not only suppresses muscle tone during stimulation but also elicits stepping-like activity during interstimulations [5]. Neurotoxic or mechanical lesions of the C-VMPJ generate rhythmic motor activity in the decerebrate animal [27]. Motor hyperactivity induced by lesions of the C-VMPJ can be blocked by APV, a NMDA antagonist, injected into the NMC [28] indicating dysfunction of the C-VMPJ may result in hyperactivity of the NMDA receptors in the NMC, which in turn elicit phasic motor activity. This observation led to the hypothesis that the C-VMPJ plays an important role in the modulation of tonic and phasic motor activity during sleep.
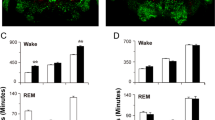
We tested our hypothesis by performing neurotoxic lesions in otherwise intact cats. A small volume (0.5 μL) of high concentration (0.5 M) of NMDA was injected into the C-VMPJ (Fig. 42.3). Sleep and motor activity recordings were performed before and after C-VMPJ lesions. Motor activities including reflex activities, blinking, and walking, as well as behaviors including eating and drinking in wakefulness, appeared normal in the cats after C-VMPJ lesions. However, motor hyperactivities in both NREM and REM sleep were observed after C-VMPJ lesions. Though basal muscle tone remained low, an increase in phasic twitches in the leg, either unilaterally or bilaterally, during NREM sleep has been observed after C-VMPJ lesions. The changes in phasic leg twitches in NREM sleep can be divided into the early (first week after lesion) and late (after the first week of lesion) phases. Leg twitches in the early phase appeared as irregular and nonperiodic; they are called isolated leg movements (ILM) . Then, the isolated leg movements in NREM sleep gradually became more regular and periodic during the late phase of the lesion. Thus, the number of ILM gradually decreased in the late phase after lesion. In contrast, PLMs gradually increased, reached the plateau level at 30 days after lesion, and continued throughout the entire 4-month period of recording.

Photomicrograph showing the lesion area (blue arrow) in a cat . Lesions of the ventral paralemniscal tegmental field produce an increase in phasic motor activity in both NREM and REM sleep , REM sleep without atonia, and RBD-like activity. CNF cuneiform nucleus, FTP paralemniscal tegmental field, ICC central nucleus of the inferior colliculus, ICX external cortex of the inferior colliculus
During REM sleep in these cats, muscle activity appeared as a mixture of intermittent atonia and high muscle tone. PLMs in REM sleep, which are never seen in the normal animals, have also been seen in C-VMPJ-lesioned animals. Simple motor activity or more complex behaviors, such as jerking, kicking and extending of the leg, raising and moving of the head, and lifting of the body, were observed in REM sleep. This abnormal REM sleep behavior, which resembled RBD seen in humans, lasted for 20–62 seconds in each episode. Furthermore, the total time in both NREM and REM sleep was not changed in C-VMPJ-lesioned animals [29]. Taken together, the C-VMPJ-lesioned animals express an unaltered total time in NREM and REM sleep, an increase in PLMs or isolated leg movements in NREM sleep, a mixture of atonia and muscle tone in REM sleep, PLMs in REM sleep, and behavior expressions in REM sleep resembling symptoms in RBD patients.
Thus, the C-VMPJ may play an important role in the neuropathology in RBD. Indeed, abnormality of the ventral pons, but not the dorsolateral pons , has been reported in idiopathic RBD patients [26, 30] (Chap. 9 discusses lesional RBD). Severe neural degeneration in the ventral pons is also reported in olivopontocerebellar atrophy patients, who also develop RBD [31].
3.2 The Ventral External Cortex of the Inferior Colliculus (VICX)
The VICX receives inputs not only from acoustic structures such as the superior olivary complex, nuclei of the lateral lemniscus , cochlear nucleus and auditory cortex but also from motor regulating structures including globus pallidus and substantia nigra pars lateralis (SNL) [32]. Neurons from the VICX project to the extrapyramidal system that includes the superior colliculus, pontine nucleus, posterior thalamus, cerebellum, and SNL [33]. Animal studies show that neuronal activity of the C-VMPJ and VICX [34] correlates with vocalization. Electrical stimulations in the VICX increase muscle tone [35]. Both vocalizations and increased muscle tone are seen during dream-enacting motor behavior in REM sleep in RBD patients. Since an extensive reciprocal innervation between C-VMPJ and the VICX, as well as an abnormal auditory brainstem response wave V, which recorded in the inferior colliculus area, have been reported in RBD patients (see citations in [36]), we therefore tested whether the VICX also participates in the generation of RBD. Baclofen, a GABAB receptor agonist, when microinfused into the VICX, elicits a significant increase in REM sleep and motor activity in both NREM and REM sleep. PLMs are significantly increased in NREM sleep. REM sleep atonia is intermingled with high muscle tone. RBD-like activities, such as movements of head, leg, and tail and body jerks, are observed in REM sleep during baclofen infusion and 2 hours post-infusion. Low doses of baclofen infused into the VICX have no effect on sleep-wake pattern and motor activity in sleep. In contrast, high-dose saclofen , a GABAB receptor antagonist, suppresses PLMs in NREM sleep when microinfused into the VICX [36]. The baclofen-VICX-generated RBD-like activity in the rat may be mediated through the anatomical connection to the C-VMPJ.
3.3 Sublaterodorsal Tegmental Nucleus of the Rat and Peri-locus Coeruleus α of the Cat
In addition to the rostral ventral pons and caudal ventral midbrain (the caudal VMPJ) in the generation of RBD, the dorsal lateral pons may also participate in the generation of motor hyperactivity in REM sleep. The nucleus in the dorsal lateral pons has been named sublaterodorsal tegmental nucleus (SLD) in the rodent or peri-locus coeruleus α (peri-LCα) in the cat and human. Neurons in the peri-LCα/SLD have been well documented to be involved in REM sleep control. Sakai et al. [13] demonstrated that peri-LCα REM-on neurons, whose activity specifically increased in REM sleep, project to the rostroventral medulla of the NMC, which in turn projects to the spinal cord. The REM-on cells of the peri-LCα/SLD are glutamatergic [37]. Activation of the peri-LCα/SLD by cholinergic or glutamatergic agonists elicited muscle atonia in the decerebrate cat [8, 9]. In contrast, inactivation of the peri-LCα/SLD produced motor hyperactivity in REM sleep in the chronic animals. Adeno-associated viral vectors carrying hairpin (sh)RNAs against Slc17a6 mRNA (AAV-shvGluT2), a RNA inhibitor targeting vesicular glutamate transporter 2 (vGluT2), injected into the SLD causes REM sleep without atonia, as well as increased phasic motor activities in REM sleep [37].
These motor-behavioral abnormalities in REM sleep seen in the rat with inactivated SLD glutamatergic neurons resemble those found in RBD patients. However, a significant decrease in REM sleep, which is never seen in RBD patients, was observed in the rat after AAV-shvGluT2 injected to the SLD [37]. Furthermore, phasic motor activity in NREM sleep was not reported in the SLD AAV-shvGluT2-injected rat. Thus, disturbance or destruction of SLD glutamatergic neurons may only play a role in the generation of abnormal motor events in REM sleep but not the other components of RBD seen in human patients.
4 Hypothetical Link Between Parkinsonism and RBD
It has been shown that idiopathic RBD is a risk factor for developing α-synuclein-related neurodegenerative diseases, such as Parkinson’s disease, multiple system atrophy, and Lewy body dementia. Clinical evidence shows that RBD is diagnosed in 90% multiple system atrophy patients [38] and 50% Parkinson’s disease patients [39]. Indeed, patients may be diagnosed simultaneously with Parkinsonian disorders and RBD or diagnosed with RBD before developing Parkinsonian disorders or vice versa [38, 40]. Physiological studies show a prolonged latency of auditory-evoked potential brainstem wave V recorded in RBD, Parkinson’s disease [41], and multiple system atrophy [42] patients. Auditory brainstem response waves I–IV interpeak latencies are also significantly prolonged in Parkinson’s disease patients [41]. Loss of the dopaminergic neurons in the substantia nigra and noradrenergic neurons in the locus coeruleus has been observed in both Parkinsonism and RBD patients [40]. Transcranial brain sonography assesses that substantia nigra hyperechogenicity exists in both Parkinsonism and RBD patients [43]. Reduced dopamine transporter in the striatum has been also detected in Parkinsonism and RBD patients [44]. However, the reasons for these overlapping symptoms and disease progression have not been explained anatomically.
Alpha-synuclein, a presynaptic protein, is the major component of neuronal Lewy bodies and Lewy neurites. Physiologically, α-synuclein may play an important role in the maintenance and stabilization of fully mature synapses [45]. Pathological changes of α-synuclein result in the loss of its ability to bind to the synaptic vesicle. Abnormal aggregation of α-synuclein forms Lewy bodies and Lewy neurites and leads to synaptic dysfunction and neuron death [46]. Recent studies demonstrate that aggregated α-synuclein can be transmitted from neuron to neuron via anatomical connection [47, 48]. Synthetic α-synuclein preformed fibrils, which act as the seed and cause the aggregation and fibrillization of soluble endogenous α-synuclein, injected into the striatum. Luk et al. [47] report that Lewy bodies and Lewy neurites time and neural connectivity dependently spread from the striatum to the cortex, the thalamus, and the substantia nigra. A caudo-rostral spreading of aggregated α-synuclein has also been reported. With recombinant adeno-associated virus carrying human α-synuclein injected into the vagus nerve, Ulusoy et al. [48] demonstrates that Lewy bodies and Lewy neurites are synaptically transmitted sequentially from the vagus nerve to the vagus motor nucleus of the medulla, the dorsal and ventral nuclei of the lateral lemniscus, the rostral ventral paralemniscal tegmental field of the pons, substantia nigra of the midbrain, and histaminergic system of the diencephalon.
The neural network of Lewy body and Lewy neurite transmission is consistent with clinical findings showing abnormal substantia nigra and structures involved in vocalization and auditory responses, in the nuclei of lateral lemniscus and inferior colliculus. This pathway is also consistent with our animal studies showing RBD is induced by lesions of the C-VMPJ (the rostral ventral paralemniscal tegmental field, Figs. 42.3 and 42.4) in the cat and by VICX-baclofen infusion in the rat (Fig. 42.4). Thus, the C-VMPJ and VICX may play a critical role not only in the generation of RBD but also in the development of Parkinsonism (Fig. 42.4). The upstream connections from the brainstem to the forebrain may originate in the VICX. Anatomical studies show reciprocal innervation between VICX and substantia nigra [33], which in turn reciprocally connect to the striatum. The C-VMPJ may participate in the downstream connection. Reciprocal innervation between the C-VMPJ and NMC, the NMC and the nucleus of the solitary tract, as well as the C-VMPJ and the nucleus of the solitary tract has also been reported [49, 50].

Hypothetical link between Parkinsonism and RBD. Toxic substances ingested into the gut may cause the degeneration of sensory fibers which project to the nucleus of the solitary tract and to the vagus motor nucleus. Similarly, the toxic substances may, via respiration, enter into the olfactory system. Lewy bodies and Lewy neurites formed in the nucleus solitary tract/vagus motor nucleus and olfactory bulb sequentially propagate from neuron to neuron. Depending on the neural structures affected by Lewy bodies and Lewy neurites, patients may develop RBD and then Parkinsonism or vice versa. See the text for the details. The pink and blue areas represent the ventral external cortex of the inferior collicus and the caudal ventral mesopontine junction area, respectively. GP globus pallidus, IC inferior colliculus, MRF mesencephalic reticular formation, NST/X nucleus solitary tract/vagus motor, SC superior colliculus, SN substantia nigra, ST striatum
We hypothesize that neuronal degeneration can be initiated in either part of the central nervous system and progressively extend to the caudal or rostral part of the brain. Patients may be diagnosed with RBD first and then developed Parkinsonism when neurodegeneration begins in the C-VMPJ . Lewy bodies and Lewy neurites in the C-VMPJ are then propagated rostrally to the VICX , substantia nigra, and striatum. Alternatively, Lewy bodies and Lewy neurites may caudo-rostrally and rostro-caudally serve as a conduit from the vagus motor nucleus and the olfactory bulb. Thus, Parkinsonism and RBD may be diagnosed simultaneously. In contrast, when patients were diagnosed with Parkinson’s disease first and then develop RBD, it may be a result of differential timing in the progression of Lewy body and Lewy neurite transmission from the rostral to the caudal brain and from the caudal to the rostral brain, with the prorogation rate from the olfactory bulb to the substantia nigra being higher than from the vagus motor nucleus to the C-VMPJ.
Conclusions
Muscle atonia in REM sleep results from the activation of the medial pontomedullary reticular formation, which in turn activates the NMC GABAergic and glycinergic neurons and inhibits medullary raphe serotonergic and pontine locus coeruleus noradrenergic neuronal activity. The neurodegeneration of the medial pontomedullary reticular formation causes solely REM sleep without atonia and abnormal motor activity in REM sleep. In contrast, the rostral part of the brainstem is not only involved in the modulation of tonic muscle activity in REM sleep via the connection of PIA-NMC pathway, but also in the inhibition of phasic motor activity in NREM and REM sleep. Dysfunction of the rostral brainstem, the C-VMPJ and VICX, elicits RBD. Anatomical connections innervating the C-VMPJ and VICX may play an important role in the development of Parkinsonism in idiopathic RBD patients and vise versa.
References
Fernandez-Arcos A, Iranzo A, Serradell M, Gaig C, Santamaria J. The clinical phenotype of idiopathic rapid eye movement sleep behavior disorder at presentation: a study in 203 consecutive patients. Sleep. 2016;39(1):121–32.
Schenck CH, Bundlie SR, Ettinger MG, Mahowald MW. Chronic behavioral disorders of human REM sleep: a new category of parasomnia. Sleep. 1986;9(2):293–308.
Jouvet M, Delorme F. Locus coeruleus et sommeil paradoxal. Compt Rend Soc Biol. 1965;159:895–9.
Magoun HW, Rhines R. An inhibitory mechanism in the bulbar reticular formation. J Neurophysiol. 1946;9:165–71.
Lai YY, Siegel JM. Muscle tone suppression and stepping produced by stimulation of midbrain and rostral pontine reticular formation. J Neurosci. 1990;10(8):2727–34.
Lai YY, Clements JR, Wu XY, Shalita T, Wu JP, Kuo JS, Siegel JM. Brainstem projections to the ventromedial medulla in cat: retrograde transport horseradish peroxidase and immunohistochemical studies. J Comp Neurol. 1999;408(3):419–36.
Shiromani PJ, Lai YY, Siegel JM. Descending projections from the dorsolateral pontine tegmentum to the paramedian reticular nucleus of the caudal medulla in the cat. Brain Res. 1990;517(1–2):224–8.
Lai YY, Siegel JM. Pontomedullary glutamate receptors mediating locomotion and muscle tone suppression. J Neurosci. 1991;11(9):2931–7.
Hajnik T, Lai YY, Siegel JM. Atonia-related regions in the rodent pons and medulla. J Neurophysiol. 2000;84(4):1942–8.
Lai YY, Siegel JM. Medullary regions mediating atonia. J Neurosci. 1988;8(12):4790–6.
Siegel JM, Wheeler RL, McGinty DJ. Activity of medullary reticular formation neurons in the unrestrained cat during waking and sleep. Brain Res. 1979;179(1):49–60.
Lai YY, Clements JR, Siegel JM. Glutamatergic and cholinergic projections to the pontine inhibitory area identified with horseradish peroxidase retrograde transport and immunohistochemistry. J Comp Neurol. 1993;336(3):321–30.
Sakai K, Kanamori N, Jouvet M. [Neuronal activity specific to paradoxical sleep in the bulbar reticular formation in the unrestrained cat]. C R Seances Acad Sci D. 1979;289(6):557–61.
Schenkel E, Siegel JM. REM sleep without atonia after lesions of the medial medulla. Neurosci Lett. 1989;98(2):159–65.
Kodama T, Lai YY, Siegel JM. Suppression of muscle tone by the medulla: distinct roles of nucleus gigantocellularis and magnocellularis. Program No. 300, Soc Neurosci Abstract; 2010.
White SR, Neuman RS. Facilitation of spinal motoneurone excitability by 5-hydroxytryptamine and noradrenaline. Brain Res. 1980;188(1):119–27.
Lai YY, Strahlendorf HK, Fung SJ, Barnes CD. The actions of two monoamines on spinal motoneurons from stimulation of the locus coeruleus in the cat. Brain Res. 1989;484(1–2):268–72.
Wu MF, Gulyani SA, Yau E, Mignot E, Phan B, Siegel JM. Locus coeruleus neurons: cessation of activity during cataplexy. Neuroscience. 1999;91(4):1389–99.
Lai YY, Kodama T, Siegel JM. Changes in monoamine release in the ventral horn and hypoglossal nucleus linked to pontine inhibition of muscle tone: an in vivo microdialysis study. J Neurosci. 2001;21(18):7384–91.
Lai YY, Kodama T, Schenkel E, Siegel JM. Behavioral response and transmitter release during atonia elicited by medial medullary stimulation. J Neurophysiol. 2010;104(4):2024–33.
Kodama T, Lai YY, Siegel JM. Changes in inhibitory amino acid release linked to pontine-induced atonia: an in vivo microdialysis study. J Neurosci. 2003;23(4):1548–54.
Holstege JC, Bongers CM. A glycinergic projection from the ventromedial lower brainstem to spinal motoneurons. An ultrastructural double labeling study in rat. Brain Res. 1991;566(1–2):308–15.
Mileykovskiy BY, Kiyashchenko LI, Kodama T, Lai YY, Siegel JM. Activation of pontine and medullary motor inhibitory regions reduces discharge in neurons located in the locus coeruleus and the anatomical equivalent of the midbrain locomotor region. J Neurosci. 2000;20(22):8551–8.
Sanford LD, Morrison AR, Mann GL, Harris JS, Yoo L, Ross RJ. Sleep patterning and behaviour in cats with pontine lesions creating REM without atonia. J Sleep Res. 1994;3(4):233–40.
Shouse MN, Siegel JM. Pontine regulation of REM sleep components in cats: integrity of the pedunculopontine tegmentum (PPT) is important for phasic events but unnecessary for atonia during REM sleep. Brain Res. 1992;571(1):50–63.
Schenck CH, MW M. A polysomnographic, neurologic, psychiatric, and clinical outcome report on 70 consecutive cases with REM sleep behavior disorder (RBD): sustained clonazepam efficacy in 89.5% of 57 treated patients. Clev Clin J Med. 1990;57(Suppl):S9–S23.
Lai YY, Siegel JM. Brainstem-mediated locomotion and myoclonic jerks. I. Neural substrates. Brain Res. 1997;745(1–2):257–64.
Lai YY, Siegel JM. Brainstem-mediated locomotion and myoclonic jerks. II. Pharmacological effects. Brain Res. 1997;745(1–2):265–70.
Lai YY, Hsieh KC, Nguyen D, Peever J, Siegel JM. Neurotoxic lesions at the ventral mesopontine junction change sleep time and muscle activity during sleep: an animal model of motor disorders in sleep. Neuroscience. 2008;154(2):431–43.
Mazza S, Soucy JP, Gravel P, Michaud M, Postuma R, Massicotte-Marquez J, Decary A, Montplaisir J. Assessing whole brain perfusion changes in patients with REM sleep behavior disorder. Neurology. 2006;67(9):1618–22.
Salva MA, Guilleminault C. Olivopontocerebellar degeneration, abnormal sleep, and REM sleep without atonia. Neurology. 1986;36(4):576–7.
Coleman JR, Clerici WJ. Sources of projections to subdivisions of the inferior colliculus in the rat. J Comp Neurol. 1987;262(2):215–26.
Yasui Y, Nakano K, Kayahara T, Mizuno N. Non-dopaminergic projections from the substantia nigra pars lateralis to the inferior colliculus in the rat. Brain Res. 1991;559(1):139–44.
Sugiyama Y, Shiba K, Nakazawa K, Suzuki T, Hisa Y. Brainstem vocalization area in guinea pigs. Neurosci Res. 2010;66(4):359–65.
Juch PJ, Schaafsma A, van Willigen JD. Brainstem influences on biceps reflex activity and muscle tone in the anaesthetized rat. Neurosci Lett. 1992;140(1):37–41.
Hsieh KC, Nguyen D, Siegel JM, Lai YY. New pathways and data on rapid eye movement sleep behaviour disorder in a rat model. Sleep Med. 2013;14(8):719–28.
Valencia Garcia S, Libourel P-A, Lazarus M, Grassi D, Luppi P-H, Fort P. Genetic inactivation of glutamate neurons in the rat sublaterodorsal tegmental nucleus recapitulates REM sleep behavior disorder. Brain. 2017;140:414–28.
Plazzi G, Corsini R, Provini F, Pierangeli G, Martinelli P, Montagna P, Lugaresi E, Cortelli P. REM sleep behavior disorders in multiple system atrophy. Neurology. 1997;48(4):1094–7.
Wetter TC, Collado-Seidel V, Pollmacher T, Yassouridis A, Trenkwalder C. Sleep and periodic leg movement patterns in drug-free patients with Parkinson’s disease and multiple system atrophy. Sleep. 2000;23(3):361–7.
Schenck CH, Bundlie SR, Mahowald MW. Delayed emergence of a Parkinsonian disorder in 38% of 29 older men initially diagnosed with idiopathic rapid eye movement sleep behaviour disorder. Neurology. 1996;46(2):388–93.
Shalash AS, Hassan DM, Elrassas HH, Salama MM, Mendez-Hernandez E, Salas-Pacheco JM, Arias-Carrion O. Auditory- and vestibular-evoked potentials correlate with motor and non-motor features of Parkinson’s disease. Front Neurol. 2017;8:55.
Kodama Y, Ieda T, Hirayama M, Koike Y, Ito H, Sobue G. Auditory brainstem responses in patients with autonomic failure with Parkinson’s disease and multiple system atrophy. J Auton Nerv Syst. 1999;77(2–3):184–9.
Shin HY, Joo EY, Kim ST, Dhong HJ, Cho JW. Comparison study of olfactory function and substantia nigra hyperechogenicity in idiopathic REM sleep behavior disorder, Parkinson’s disease and normal control. Neurol Sci. 2013;34(6):935–40.
Walker Z, Costa DC, Walker RW, Lee L, Livingston G, Jaros E, Perry R, McKeith I, Katona CL. Striatal dopamine transporter in dementia with Lewy bodies and Parkinson disease: a comparison. Neurology. 2004;62(9):1568–72.
Murphy DD, Rueter SM, Trojanowski JQ, Lee VM. Synucleins are developmentally expressed, and alpha-synuclein regulates the size of the presynaptic vesicular pool in primary hippocampal neurons. J Neurosci. 2000;20(9):3214–20.
Volpicelli-Daley LA, Luk KC, Patel TP, Tanik SA, Riddle DM, Stieber A, Meaney DF, Trojanowski JQ, Lee VM. Exogenous alpha-synuclein fibrils induce Lewy body pathology leading to synaptic dysfunction and neuron death. Neuron. 2011;72(1):57–71.
Luk KC, Kehm V, Carroll J, Zhang B, O’Brien P, Trojanowski JQ, Lee VM. Pathological alpha-synuclein transmission initiates Parkinson-like neurodegeneration in nontransgenic mice. Science. 2012;338(6109):949–53.
Ulusoy A, Rusconi R, Perez-Revuelta BI, Musgrove RE, Helwig M, Winzen-Reichert B, Di Monte DA. Caudo-rostral brain spreading of alpha-synuclein through vagal connections. EMBO Mol Med. 2013;5(7):1119–27.
Manaker S, Fogarty PF. Raphespinal and reticulospinal neurons project to the dorsal vagal complex in the rat. Exp Brain Res. 1995;106(1):79–92.
Rinaman L. Ascending projections from the caudal visceral nucleus of the solitary tract to brain regions involved in food intake and energy expenditure. Brain Res. 2010;1350:18–34.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2019 Springer International Publishing AG, part of Springer Nature
About this chapter

Cite this chapter
Lai, YY., Hsieh, KC., Siegel, J.M. (2019). Animal Models of REM Sleep Behavior Disorder. In: Schenck, C., Högl, B., Videnovic, A. (eds) Rapid-Eye-Movement Sleep Behavior Disorder. Springer, Cham. https://doi.org/10.1007/978-3-319-90152-7_42
Download citation
DOI: https://doi.org/10.1007/978-3-319-90152-7_42
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-90151-0
Online ISBN: 978-3-319-90152-7
eBook Packages: MedicineMedicine (R0)