
Abstract
Several dimensions of commuting influence perceived stress, such as impedance (a measure of distance and time which is impacted by the number of transport nodes), and control over and predictability of commuting. Research into commuting mode and stress has generated mixed results. The case study in this chapter used baseline survey data from a 3-year workplace travel plan intervention. Workplace travel plans aim to promote active and sustainable forms of transport and reduce driving to work. An on-line cross-sectional survey of staff travel behaviour was conducted in September 2011 at Liverpool Hospital in Sydney, Australia. A total of 675 respondents provided data on the items of interest for this analysis (travel behaviour, self-reported stress, occupation type, demographics). Approximately one in six respondents (15%) actively commuted to work (walking 4%, cycling 2% or using public transport 9%). There was a large (15%) difference between active commuters’ (10.1%) and drivers’ (25%) perceptions that the commute to work was more stressful than the rest of their day that remained statistically significant (adjusted odds ratio 0.35, 95% confidence interval 0.17–0.73) after adjusting for factors including gender, age, physical activity levels and occupational type (clinical vs non-clinical). These findings support international research which has shown that active travel to work may be less stressful than car commuting.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
1 Elements of the Quality of Life Concept Explored in This Case Study
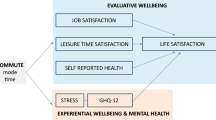
This chapter presents a case study of an investigation into the relationship between stress, and the daily commute to work by car and by active modes of transport (Rissel et al. 2014b). Stress is an aspect of quality of life, often investigated singularly, and at other times embedded alongside other indicators of quality of life to measure affect or aspects of mental wellbeing. This chapter specifically explores stress as it relates directly to the psychological health component of quality of life (Novaco and Gonzalez 2009).
Several dimensions of the commuting situation influence perceived stress, such as impedance (a measure of distance and time which is impacted by the number of transport nodes), and control over and predictability of commuting. In this case study, perceptions of stress is compared between commuters who travel to work by car and by active modes.
2 Definition of the Problem
In developing and developed countries the majority of the world’s citizens now live in urban areas (WHO/UN-HABITAT 2010). Although evidence suggests the steep rise in private motor vehicle ownership that occurred over the last 60 years in most developed countries has plateaued, (Newman and Kenworthy 2015) the global trend is still toward private car ownership growing faster than any other form of transport (Dargay et al. 2007). In many countries cars are currently the dominant form of transport for trips to work (Newman and Kenworthy 2015). Commuting to work by car contributes negligible physical activity (Ding et al. 2014; Petrunoff et al. 2013b). Public health advocates are concerned about this because physical inactivity has reached a state of what has been described as global pandemic. Physical inactivity, it is a major risk factor for chronic diseases including ischemic heart disease, stroke, diabetes and some cancers, and is the fourth leading risk factor for death worldwide (Kohl et al. 2012).
As well as reducing opportunities for physical activity, this global increase in car ownership and urbanisation inevitably creates greater traffic congestion, if more cars traveling on existing road infrastructure within the built environment. Traffic impedance, personal control over the journey, and predictability of the work commute are all factors contributing to stress of the commuting trip (Gottholmseder et al. 2009). Commuting to work by car may be more stressful than other modes of travel because of the impedance associated with traffic congestion that is largely avoided by active travel modes (Novaco and Gonzalez 2009). In previous research, car commuters have report higher stress levels than other transport mode users, (Gatersleben and Uzzell 2007; Legrain et al. 2015).
Other research has found that public transport users also report stress, but are more likely to reported greater boredom (Gatersleben and Uzzell 2007). Part of the reason for this may be due to distance travelled, with longer distances, greater than 30 min, associated with higher amounts of perceived stress and poorer life satisfaction (Gottholmseder et al. 2009; St-Louis et al. 2014; Wheatley 2014). The findings are however mixed and other studies have shown commuting times over 60 min to be less stressful and indeed variable, according to residential location and time (Hansson et al. 2011; Mattisson et al. 2016). In the case of public transport, social and entertainment technologies may be helping to counteract potential stress and boredom (Ettema et al. 2012). Much more needs to be understood about the relationship between stress and commuting, particularly in regards to the variability across different transport environments, travel modes and work employment situations.
3 Explanation of Why the Problem Is Important
There is an urgent need to consider how to incorporate physical activity into our daily lives and one promising way to do this is to promote active commuting to work (Petrunoff et al. 2016a). Active commuting, allows people to participate in amounts of physical activity that are important for maintaining health (Petrunoff et al. 2013b; Sahlqvist et al. 2012; Yang et al. 2012). Walking and cycling are inherently active forms of commuting. Using public transport to travel to work can also be considered active commuting when the journey between the worksite or home and the public transport interchange includes for example a 10-min brisk walk each way (WHO 2010). If active travel options are not available and workers have little choice but to commute by car, then stress-related health issues and associated healthcare costs can only increase.
Strong evidence supports that adults who change from inactive transport to more active forms of transport significantly reduce their cardiovascular disease risk (Celis-Morales et al. 2017; Gordon-Larsen et al. 2009; Møller et al. 2011; Wennberg et al. 2006; Xu et al. 2013). Good evidence also suggests active travel can lead to significant reductions in body mass index (weight in kilograms divided by height in meters squared – a population measure used to classify people’s weight).(Flint and Cummins 2015; Martin et al. 2015; Mytton et al. 2016; Sato et al. 2007; Sugiyama et al. 2012, 2013; Wanner et al. 2012; Wen et al. 2006; Xu et al. 2013) While important as a way of achieving physical activity, interventions to encourage active commuting, as an alternative to car-based travel might also reduce stress and have positive effects on overall mental health (Ohta et al. 2007; Rissel et al. 2014a, b) as well as improve wellbeing more broadly (Crane et al. 2014).
The workplace setting is a valid place to promote active travel since in many developed countries the majority of adults travel to a workplace, (OECD 2013) and the trip is generally repetitious. A large proportion of journeys to work which are made by private motor vehicles are relatively short distances of less than 5 km and could be made by walking and cycling modes, or supported by public travel for longer distances (BTS 2013; Goodman 2013). A shift from driving private motor vehicles towards active travel to workplace settings could achieve population level increases in physical activity, lead to associated reductions in chronic disease risk, and a large decrease in traffic volume.
The workplace setting is also a valid target for active travel interventions as a way to improve workplace health. Workforce well-being is affected by many factors, such as job demand and control, support, organisational justice and the effort–reward balance; as well as personal factors such as health, socioeconomic and other demographics (Nieuwenhuijsen et al. 2010). The association between perceived stress and work productivity, absenteeism and presenteeism is well recognised, and attention has focused on workplace interventions to manage stress and improve employee health (Bhui et al. 2012; Jacobson et al. 1996; Noblet and LaMontagne 2006). This is important given mental illness is a significant global disease burden. Stress-related workers compensation claims are estimated to cost Australia between $10 and 20 billion in loss of work productivity and participation (Safe, Work, & Australia 2013).
Research into the association between work productivity and stress has tended to focus only on the stress accumulated within the work environment. The contribution of the commute to work to workplace stress is often under-recognised or ignored in studies investigating workplace stress, productivity and absenteeism. To some extent this is attributable to the perception that how individuals get to work is a personal choice, and that individual attitudes and perceptions towards transportation affect transport choices (Friman et al. 2017; Popuri et al. 2011). Yet it must be recognised that the commuting stress transfer beyond the individual to impact work and home life (Novaco and Gonzalez 2009). The relationship between stress reported by workers therefore needs to be considered holistically, and that includes an assessment of how the journey to work might contribute to that stress. This case study aims to address this gap in the literature and explore the association between perceptions of work-related stress and the work commute.
4 Steps Taken to Address the Problem
The case study in this chapter used baseline survey data from a 3-year workplace travel plan intervention. Workplace travel plans aim to promote active and sustainable forms of transport and reduce driving to work. Workplace travel plans can achieve between 10% and 20% reductions in driving to work, (Bamberg and Möser 2007; Cairns et al. 2010; De Gruyter et al. 2018; Hosking et al. 2010; Macmillan et al. 2013; Marsden et al. 2011). Some studies have also demonstrated significant increases in active travel to work, (Brockman and Fox 2011; Petrunoff et al. under review) but only one robust experimental study of these effects (Higgins 1996). Workplace travel plans are a delivery mechanism for actions which often include policy (e.g. parking management policy, public transport ticket subsidies), infrastructure (e.g. provision of end of trip facilities, creation of maps) and behaviour change programs (e.g. cycling and walking programs) (Enoch 2012).
There is no internationally accepted term for workplace travel plans. The term is used in Australia, New Zealand, the United Kingdom, Singapore and some other countries. In North America they are sometimes referred to as travel demand management plans and in some parts of Europe and Scandinavia site-based mobility management plans. In some regions they can be required as a condition of planning consent for new or expanded developments typically occupied by medium-large organisations (Rye et al. 2011a, b; Wynne 2015). However, even where systematic government support for their adoption exists, take-up of these promising interventions has been modest, which has led experts to recommend they be marketed to organisations in terms of their benefit to the organisation (Enoch 2012; Petrunoff et al. 2017).
The baseline study included the quality of life construct of stress to assess the relationship between stress and commuting to work by different transport modes (Rissel et al. 2014a, b). Data on reductions in stress and links to associated gains in productivity may assist with engaging these organisations to adopt and support the implementation of travel plans.
4.1 Research Design
An on-line cross-sectional survey of staff travel behaviour was conducted in September 2011 at Liverpool Hospital in Sydney, Australia (Petrunoff et al. 2013a). The survey was part of a larger study that was repeated in three annual follow-up surveys (Petrunoff et al. 2016b).
4.2 Setting and Context
Liverpool Hospital is in an outer metropolitan area of Liverpool, south-west Sydney, Australia and is a principal referral teaching hospital. Liverpool Hospital was in the second stage of a major re-development when the travel plan was being developed. The re-development plans forecast the number of staff and hospital beds increasing by approximately one-third between 2006 and 2016, to cope with the increasing health demands of the growing population of the area, identified as one of two ‘growth centres’ by state government planning departments. At the time the study commenced, the Hospital was well serviced by heavy rail, with two stations within 10-min easy walking distance. Hospital staff also had access to an extensive bus network. There were significant gaps in the cycling network in the immediate surrounds of the hospital (see Fig. 10.1). A more detailed of the regional level cycling network map which clearly shows these gaps is available at a web link in references (Rissel 2010).


Liverpool hospital access guide showing local transport context
4.3 Survey Methods
An email was sent to all staff (approximately n = 3200) via existing staff communication channels. The survey was a self-administered online questionnaire (Qualtrics 2017). All staff were invited via email to participate in the survey, which was supported by the hospital General Manager. A flyer promoting the survey was distributed to all staff via the mail room, posters were placed around the hospital and a prize incentive offered to encourage participation. The survey ran for 2 weeks, with a reminder sent 7 days after the survey started. Paper copies of the survey were made available to General Services staff who did not have regular access to work emails.
Participants were asked: “How did you travel to work this week? (If you used more than one form of transport, show the method used for the longest (distance) part of the journey)”. Response options for each day of the week were walked, cycled, drove a car, car passenger, bus, ferry, train, taxi, truck, motorbike or scooter, worked at home, other, and I did not go to work. This question was tested with a sub-sample of staff and was shown to be valid and reliable (Petrunoff et al. 2013b).
Walking, cycling and public transport categories were considered “active travel.” Public transport users were included here because this typically included an approximate 10-min walk to major bus and train interchanges. Car categories including car as a driver or passenger, motorbike and scooter were considered “non-active travellers” since for the majority of car drivers their commute was likely to be inactive, and this was demonstrated using objective accelerometer data with a sub-sample of staff in the survey validation study (Petrunoff et al. 2013b). Participants were categorised as “active travellers” overall if they travelled using an active travel mode on half or more of the working days recorded in their travel diary.
Participants were also asked about the relative stress of their commute: “Compared to other parts of your day, how stressful do you find the journey to and from work?” with response options being “More stressful”, “Less stressful” or “About the same”. Demographic information (age, sex, and whether they had mainly a clinical or administrative role) was also collected, as was the amount of physical activity over the previous week (using the International Physical Activity Questionnaire-short version) (Booth et al. 2003). Transport-related physical activity was included in the measurement of physical activity. Total moderate to vigorous physical activity time has been used to assess adequate physical activity, which is defined as 150 min/week for consistency with international physical activity guidelines.
Statistical methods were used to test the strength of associations between the different commute modes to work and participants’ self-reported levels of stress after adjusting for differences in some of the factors which could impact the results. Specifically, Chi square statistics were also used to examine the association between demographic characteristics of the sample and travel mode to work. Then, logistic regression was used to investigate the association of travel mode to work with self-reported stress (“more stressful” vs “about the same”/“less stressful”), adjusting for age, sex, clinical or non-clinical role, and adequate weekly physical activity (150 min/week). Odds ratios (ORs) and adjusted odds ratios (AORs) with 95% confidence intervals (CIs) were estimated as a measure of strength of association.
5 Findings
5.1 Participant Characteristics and Travel Behaviour
Table 10.1 below shows the characteristics of hospital staff who participated in the survey by active travel status. Overall 804 hospital employees participated in the initial survey (25% response rate), while 675 respondents provided data on the items of interest for this analysis. Approximately one in six respondents (15%) actively commuted to work (walking 4%, cycling 2% or using public transport 9%). Active travelers were almost twice as likely to be older than middle aged (i.e. greater than 55 years), and 60% more likely to work in an administrative rather than a clinical role.
Comparing respondents in the survey to the Sydney region, overall Sydney has a low level of active travel to work, but it varies by proximity to the central business district. Inner city areas have the highest levels of walking (10.1%) and cycling (2.2%) journeys to work (Zander et al. 2013a, b). In the outer areas of Sydney, where this study was conducted, active commuting is much lower at 2.6% of journey being by walking and 0.59% of journeys by bicycle (Zander et al. 2013a, b).
5.2 Stress and the Work Commute
One in five respondents (20.5%) said that compared to the rest of their working day, their commute was more stressful. When compared between car commuters and active travel commuters, car commuters reported a higher level of stress, with 26.1% saying the commute trip was more stressful than the rest of their day, while active commuters reported a lower rate of stress (10.1% saying the trip was more stressful than the rest of their day).
Table 10.2 shows that after adjusting for the individual’s gender, age physical activity levels and occupational role; active commuters were significantly less likely to report that their commute to work was more stressful than the rest of their day than car commuters. This result was highly statistically significant (AOR 0.35, 95% CI 0.17–0.73). Interestingly, age, sex, physical activity and occupational role were not associated with reporting a greater amount of stress on the journey to work.
6 Lessons Learned
The large (15%) difference between active commuters’ and car commuters perceptions that the commute to work was more stressful than the rest of their day remained statistically significant after adjusting for factors including gender, age, physical activity levels and occupational type (clinical vs non-clinical). These findings support international research which has shown that active travel to work may be less stressful than car commuting. Car commuting stress has been found to be associated with increased negative moods on arrival at work and the home, lower tolerance threshold, cognitive impairment, greater illness and work absenteeism, job instability and a negative effect on overall life satisfaction (Novaco and Gonzalez 2009). Many of the impedances that have been associated with car commuting stress, such as traffic congestion, have lower impact on active travel modes of transport. For example, in a UK study, where commuting by private car was found to be stressful, walking and cycling by comparison, were found to be relaxing and exciting experiences (Gatersleben and Uzzell 2007).
This case study sought to adjust for the different influences of age, gender, physical activity and the nature of respondents’ jobs which might have influence both on their commuting choices and the level of stress they might experience within the work environment. The sample of participants included in this survey were slightly disparate so that active travelers were more likely to be older and have an administrative role. Our data do not answer questions about whether administrative or clinical staff have more stressful jobs, and this may prove to be important in determining the relative stress of mode of travel. Whilst the regression model did adjust for clinical versus non-clinical roles, and a simplistic view may be that some clinical roles might be quite stressful due to high job demands, these roles may also have high levels of job control so on balance the levels of stress may in fact be as high as some administrative roles which have both a high job demand and low levels of perceived job control. We do not have an occupational delineation that allows us to describe in more detail the nature of the work respondents did. Such a study may consider the job demand and job control aspects of different work roles to attain a holistic understanding of stress within the workplace and enroute to work and to better determine the impact of stress and the role of active travel (Jones and Bright 2001).
One of the strengths of this case study is that it was the first time that the association of different travel modes with self-reported stress was confirmed in the Australian transport context. However, the findings of the case study presented was limited by being just one snapshot in time, and this prohibits the assertion of causal relationship. The generalisability of the study findings are also limited due to the study being conducted among hospital staff in southwest Sydney, where the results may be specific to the south-western Sydney transport context. Although, transport studies are always strongly influenced by the local transport and geographical contexts, and these contexts have been described in this chapter and in journal articles associated with the study so that readers can decide if the results are applicable to their local settings (Petrunoff et al. 2013a, 2016a, 2017) The results are also consistent with studies in the USA and other car-centric countries, and add to this relatively sparse area of research (Gatersleben and Uzzell 2007; Gottholmseder et al. 2009). Another limitation was that the sample consisted mostly of women, which is typical of healthcare services in Australia. Women in Australia are less likely to be active commuters than men, (Rissel et al. 2014a) so active travel rates may be lower than in other workplaces.
Assessing the association between active travel mode with self-reported stress with the work commute has important public health implications. A positive relationship between active commuting and lower levels of stress during the commute to work is likely to necessitate support for allocation of funding of infrastructure, policies and programs which support active commuting. This will also have implications for health and wellbeing within the workplace and may lead to greater work productivity and reduced absenteeism however these findings need to be assessed over time.
The findings of this case study form part of a larger piece of research to evaluate the effects of the 3-year workplace travel plan to encourage hospital workers to commute to work by active travel means. The study concluded that a workplace travel plan which included strategies to encourage active travel to work achieved significant increases in active travel (Petrunoff et al. 2016). How interventions like workplace travel plans might impact quality of life beyond the construct of stress is a question which may be investigated as part of future research.
While these findings support the evidence that commuting to work by car is more stressful than other modes of travel the next step is to be able to test the causal association by following participants over time to track these effects and, to determine how important transport for the work commute is to health outcomes such as mental health and cardiovascular disease. This will allow for other factors that cannot be attributed to the role of physical activity to be investigated, such as enjoying the scenery, lack of frustration, or letting the mind drift while travelling, all of which are important factors in why people travel (Mokhtarian et al. 2015; Ory and Mokhtarian 2005).
Stress is an important measure for further consideration in how we value travel and appraise transport options. Increasingly, transport appraisals value transport based on satisfaction with the transport journey as a measure of transport-related wellbeing (Cantwell et al. 2009). This is good, yet investigations of the relationship between the journey to work and quality of life from a health perspective are rare, (Crane et al. 2016) and quality of life measures which capture the health effects of the various transport modes tend to be unsuitable for transport studies, as they are focused primarily on clinical-based measures of physical functioning. Likewise a narrow focus on transport satisfaction to inform policy is a limitation and disregards the larger benefits of active travel to quality of life. To progress in an understanding of the journey to work, transport options and our quality of life, we need to better understand the impact at a broader level, considering not only transport and life satisfaction but measures of life experience such as stress and enjoyment (Rissel et al. 2016).
References
Bamberg, S., & Möser, G. (2007). Why are work travel plans effective? Comparing conclusions from narrative and meta-analytical research synthesis. Transportation, 34(6), 647–666. https://doi.org/10.1007/s11116-007-9121-0.
Bhui, K. S., Dinos, S., Stansfeld, S. A., & White, P. D. (2012). A synthesis of the evidence for managing stress at work: A review of the reviews reporting on anxiety, depression, and absenteeism. Journal of Environmental and Public Health, 2012, 515874.
Booth, M. L., Ainsworth, B. E., Pratt, M., Ekelund, U., Yngve, A., Sallis, J. F., & Oja, P. (2003). International physical activity questionnaire: 12-country reliability and validity. Medicine and Science in Sports and Exercise, 195(9131/03), 3508–1381.
Brockman, R., & Fox, K. R. (2011). Physical activity by stealth? The potential health benefits of a workplace transport plan. Public Health, 125(4), 210–216. https://doi.org/10.1016/j.puhe.2011.01.005.
BTS. (2013). 2012/13 household travel survey summary report 2013 release. NSW: Bureau of Transport Statistics. Retrieved from https://www.transport.nsw.gov.au/sites/default/files/media/documents/2017/HTS%20Report%20Sydney%202012-13.pdf
Cairns, S., Newson, C., & Davis, A. (2010). Understanding successful workplace travel initiatives in the UK. Transportation Research Part A: Policy and Practice, 44(7), 473–494. https://doi.org/10.1016/j.tra.2010.03.010.
Cantwell, M., Caulfield, B., & O’Mahony, M. (2009). Examining the factors that impact public transport commuting satisfaction. Journal of Public Transportation, 12(2), 1.
Celis-Morales, C. A., Lyall, D. M., Welsh, P., Anderson, J., Steell, L., Guo, Y., … Gill, J. M. R. (2017). Association between active commuting and incident cardiovascular disease, cancer, and mortality: Prospective cohort study. BMJ, 357. https://doi.org/10.1136/bmj.j1456
Crane, M., Rissel, C., Standen, C., & Greaves, S. (2014). Associations between the frequency of cycling and domains of quality of life. Health Promotion Journal of Australia, 25(3), 182–185. https://doi.org/10.1071/HE14053.
Crane, M., Rissel, C., Greaves, S., & Gebel, K. (2016). Correcting bias in self-rated quality of life: An application of anchoring vignettes and ordinal regression models to better understand QoL differences across commuting modes. Quality of Life Research, 25(2), 257–266. https://doi.org/10.1007/s11136-015-1090-8.
Dargay, J., Gately, D., & Sommer, M. (2007). Vehicle ownership and income growth, worldwide: 1960–2030. The Energy Journal, 28(4), 143–170. https://doi.org/10.2307/41323125.
De Gruyter, C., Rose, G., Currie, G., Rye, T., & van de Graaff, E. (2018). Travel plans for new developments: A global review. Transport Reviews, 38(2), 142–161.
Ding, D., Gebel, K., Phongsavan, P., Bauman, A. E., & Merom, D. (2014). Driving: A road to unhealthy lifestyles and poor health outcomes. PLoS One, 9(6), e94602. https://doi.org/10.1371/journal.pone.0094602.
Enoch, M. (2012). The development of the travel plan. In M. Enoch (Ed.), Sustainable transport, mobility management and travel plans. Surrey: Ashgate Publishing Limited.
Ettema, D., Friman, M., Gärling, T., Olsson, L. E., & Fujii, S. (2012). How in-vehicle activities affect work commuters’ satisfaction with public transport. Journal of Transport Geography, 24, 215–222.
Flint, E., & Cummins, S. (2015). Does active commuting protect against obesity in mid-life? Cross-sectional, observational evidence from UK Biobank. The Lancet, 386(Supplement 2), S8. https://doi.org/10.1016/S0140-6736(15)00846-6.
Friman, M., Olsson, L. E., Ståhl, M., Ettema, D., & Gärling, T. (2017). Travel and residual emotional well-being. Transportation Research Part F: Traffic Psychology and Behaviour, 49, 159–176.
Gatersleben, B., & Uzzell, D. (2007). Affective appraisals of the daily commute comparing perceptions of drivers, cyclists, walkers, and users of public transport. Environment and Behavior, 39(3), 416–431.
Goodman, A. (2013). Walking, cycling and driving to work in the English and Welsh 2011 census: Trends, socio-economic patterning and relevance to travel behaviour in general. PLoS One, 8(8), e71790. https://doi.org/10.1371/journal.pone.0071790.
Gordon-Larsen, P., Boone-Heinonen, J., Sidney, S., Sternfeld, B., Jacobs, D. R., Jr., & Lewis, C. E. (2009). Active commuting and cardiovascular disease risk: The CARDIA study. Archives of Internal Medicine, 169(13), 1216–1223.
Gottholmseder, G., Nowotny, K., Pruckner, G. J., & Theurl, E. (2009). Stress perception and commuting. Health Economics, 18(5), 559–576.
Hansson, E., Mattisson, K., Björk, J., Östergren, P.-O., & Jakobsson, K. (2011). Relationship between commuting and health outcomes in a cross-sectional population survey in southern Sweden. BMC Public Health, 11(1), 834.
Higgins, T. (1996). How do we know employer-based transportation demand management works? The need for experimental design. Transportation Research Record: Journal of the Transportation Research Board, 1564, 54–59.
Hosking, J., Macmillan, A., Connor, J., Bullen, C., & Ameratunga, S. (2010). Organisational travel plans for improving health. Cochrane Database of Systematic Reviews (Online), 3, CD005575.
Jacobson, B. H., Aldana, S. G., Goetzel, R. Z., Vardell, K., Adams, T. B., & Pietras, R. J. (1996). The relationship between perceived stress and self-reported illness-related absenteeism. American Journal of Health Promotion, 11(1), 54–61.
Jones, F., & Bright, J. (2001). Stress: Myth, theory and research. London: Prentice Hall.
Kohl, H. W., 3rd, Craig, C. L., Lambert, E. V., Inoue, S., Alkandari, J. R., Leetongin, G., & Kahlmeier, S. (2012). The pandemic of physical inactivity: Global action for public health. The Lancet, 380(9838), 294–305. https://doi.org/10.1016/S0140-6736(12)60898-8.
Legrain, A., Eluru, N., & El-Geneidy, A. M. (2015). Am stressed, must travel: The relationship between mode choice and commuting stress. Transportation Research Part F: Traffic Psychology and Behaviour, 34, 141–151.
Macmillan, A. K., Hosking, J., Connor, J. L., Bullen, C., & Ameratunga, S. (2013). A Cochrane systematic review of the effectiveness of organisational travel plans: Improving the evidence base for transport decisions. Transport Policy, 29(0), 249–256. https://doi.org/10.1016/j.tranpol.2012.06.019.
Marsden, A., Tunny, G., & Fitzgibbons, A. (2011). Evaluation of the travel smart local government and workplace programs. Retrieved from Perth, Western Australia: http://www.transport.wa.gov.au/mediaFiles/active-transport/AT_TS_P_Evaluation_LocalGov_Workplace.pdf
Martin, A., Panter, J., Suhrcke, M., & Ogilvie, D. (2015). Impact of changes in mode of travel to work on changes in body mass index: Evidence from the British Household Panel Survey. Journal of Epidemiology and Community Health, 69(8), 753–761. https://doi.org/10.1136/jech-2014-205211.
Mattisson, K., Jakobsson, K., Håkansson, C., & Cromley, E. (2016). Spatial heterogeneity in repeated measures of perceived stress among car commuters in Scania, Sweden. International Journal of Health Geographics, 15(1), 22.
Mokhtarian, P. L., Salomon, I., & Singer, M. E. (2015). What moves us? An interdisciplinary exploration of reasons for traveling. Transport Reviews, 35(3), 250–274.
Møller, N. C., Østergaard, L., Gade, J. R., Nielsen, J. L., & Andersen, L. B. (2011). The effect on cardiorespiratory fitness after an 8-week period of commuter cycling—A randomized controlled study in adults. Preventive Medicine, 53(3), 172–177.
Mytton, O. T., Panter, J., & Ogilvie, D. (2016). Longitudinal associations of active commuting with body mass index. Preventive Medicine, 90, 1–7. https://doi.org/10.1016/j.ypmed.2016.06.014.
Newman, P., & Kenworthy, J. (2015). Urban transportation patterns and trends in global cities. In The end of automobile dependence: How cities are moving beyond car-based planning (pp. 33–76). Washington, DC: Island Press/Center for Resource Economics.
Nieuwenhuijsen, K., Bruinvels, D., & Frings-Dresen, M. (2010). Psychosocial work environment and stress-related disorders, a systematic review. Occupational Medicine, 60(4), 277–286.
Noblet, A., & LaMontagne, A. D. (2006). The role of workplace health promotion in addressing job stress. Health Promotion International, 21(4), 346–353.
Novaco, R. W., & Gonzalez, O. I. (2009). Commuting and well-being. In Y. Amichai-Hamburger (Ed.), Technology and well-being (Vol. 3, pp. 174–205). New York: Cambridge University Press.
OECD. (2013). OECD skills outlook 2013. OECD Publishing.
Ohta, M., Mizoue, T., Mishima, N., & Ikeda, M. (2007). Effect of the physical activities in leisure time and commuting to work on mental health. Journal of Occupational Health, 49(1), 46–52.
Ory, D. T., & Mokhtarian, P. L. (2005). When is getting there half the fun? Modeling the liking for travel. Transportation Research Part A: Policy and Practice, 39(2), 97–123.
Petrunoff, N., Rissel, C., Wen, L. M., Xu, H., Meikeljohn, D., & Schembri, A. (2013a). Developing a hospital travel plan: Process and baseline findings from a western Sydney hospital. Australian Health Review, 37(5), 579–584. 10.1071/AH13006.
Petrunoff, N., Xu, H., Rissel, C., Wen, L. M., & van der Ploeg, H. (2013b). Measuring workplace travel behaviour: Validity and reliability of survey questions. Journal of Environmental and Public Health, 2013, 6. https://doi.org/10.1155/2013/423035.
Petrunoff, N., Rissel, C., & Wen, L. M. (2016a). The effect of active travel interventions conducted in work settings on driving to work: A systematic review. Journal of Transport & Health, 3(1), 61–76. https://doi.org/10.1016/j.jth.2015.12.001.
Petrunoff, N., Wen, L. M., & Rissel, C. (2016b). Effects of a workplace travel plan intervention encouraging active travel to work: outcomes from a three year time-series study. Public Health, 135, 38–47.
N. Petrunoff, L.M. Wen, C. Rissel, (2016) Effects of a workplace travel plan intervention encouraging active travel to work: outcomes from a three-year time-series study. Public Health 135:38-47
Petrunoff, N., Rissel, C., & Wen, L. M. (2017). “If You Don’t Do Parking Management.. Forget Your Behaviour Change, It’s Not Going to Work.”: Health and transport practitioner perspectives on workplace active travel promotion. PLoS One, 12(1), e0170064.
Popuri, Y., Proussaloglou, K., Ayvalik, C., Koppelman, F., & Lee, A. (2011). Importance of traveler attitudes in the choice of public transportation to work: Findings from the Regional Transportation Authority Attitudinal Survey. Transportation, 38(4), 643–661.
Qualtrics. (2017). Qualtrics survey software. Retrieved from www.qualtrics.com
Rissel, C. (2010). Cycling connecting communities: Bicycle route map for fairfield and liverpool. Retrieved from https://cyclingconnectingcommunities.files.wordpress.com/2010/08/bicycle-route-map-fairfield-liverpool-2010.pdf
Rissel, C., Greenaway, M., Bauman, A., & Wen, L. M. (2014a). Active travel to work in New South Wales 2005–2010, individual characteristics and association with body mass index. Australian and New Zealand Journal of Public Health, 38(1), 25–29.
Rissel, C., Petrunoff, N., Wen, L., & Crane, M. (2014b). Travel to work and self-reported stress: Findings from a workplace survey in south west Sydney, Australia. Journal of Transport & Health, 1(1), 50–53.
Rissel, C., Crane, M., Wen, L. M., Greaves, S., & Standen, C. (2016). Satisfaction with transport and enjoyment of the commute by commuting mode in inner Sydney. Health Promotion Journal of Australia, 27(1), 80–83.
Rye, T., Green, C., Young, E., & Ison, S. (2011a). Using the land-use planning process to secure travel plans: An assessment of progress in England to date. Journal of Transport Geography, 19(2), 235–243. https://doi.org/10.1016/j.jtrangeo.2010.05.002.
Rye, T., Welsch, J., Plevnik, A., & de Tommasi, R. (2011b). First steps towards cross-national transfer in integrating mobility management and land use planning in the EU and Switzerland. Transport Policy, 18(3), 533–543. https://doi.org/10.1016/j.tranpol.2010.10.008.
Safe, Work, & Australia. (2013). The incidence of accepted workers' compensation claims for mental stress in Australia. Canberra: Safe Work Australia. Retrieved from https://www.safeworkaustralia.gov.au/system/files/documents/1702/the-incidence-accepted-wc-claims-mental-stress-australia.pdf
Sahlqvist, S., Song, Y., & Ogilvie, D. (2012). Is active travel associated with greater physical activity? The contribution of commuting and non-commuting active travel to total physical activity in adults. Preventive Medicine, 55(3), 206–211.
Sato, K. K., Hayashi, T., Kambe, H., Nakamura, Y., Harita, N., Endo, G., & Yoneda, T. (2007). Walking to work is an independent predictor of incidence of type 2 diabetes in Japanese men: The Kansai Healthcare Study. Diabetes Care, 30(9), 2296–2298.
St-Louis, E., Manaugh, K., van Lierop, D., & El-Geneidy, A. (2014). The happy commuter: A comparison of commuter satisfaction across modes. Transportation Research Part F: Traffic Psychology and Behaviour, 26, 160–170.
Sugiyama, T., Ding, D., & Owen, N. (2012). Sitting in cars for commuting and adults’ weight gain over four years. Journal of Science and Medicine in Sport, 15, S72. https://doi.org/10.1016/j.jsams.2012.11.173.
Sugiyama, T., Ding, D., & Owen, N. (2013). Commuting by car: Weight gain among physically active adults. American Journal of Preventive Medicine, 44(2), 169–173.
Wanner, M., Gotschi, T., Martin-Diener, E., Kahlmeier, S., & Martin, B. W. (2012). Active transport, physical activity, and body weight in adults: A systematic review. American Journal of Preventive Medicine, 42(5), 493–502. https://doi.org/10.1016/j.amepre.2012.01.030.
Wen, L. M., Orr, N., Millett, C., & Rissel, C. (2006). Driving to work and overweight and obesity: Findings from the 2003 New South Wales Health Survey, Australia. International Journal of Obesity, 30(5), 782–786. https://doi.org/10.1038/sj.ijo.0803199.
Wennberg, P., Lindahl, B., Hallmans, G., Messner, T., Weinehall, L., Johansson, L., … Jansson, J. H. (2006). The effects of commuting activity and occupational and leisure time physical activity on risk of myocardial infarction. European Journal of Cardiovascular Prevention & Rehabilitation, 13(6), 924–930.
Wheatley, D. (2014). Travel-to-work and subjective well-being: A study of UK dual career households. Journal of Transport Geography, 39, 187–196.
WHO. (2010). Global recommendations on physical activity for health. Geneva: World Health Organisation.
WHO/UN-HABITAT. (2010). Hidden cities: Unmasking and uncovering health inequities in urban cities. Geneva: World Health Organisation. Retreived from http://www.who.int/kobe_centre/publications/hiddencities_media/who_un_habitat_hidden_cities_web.pdf
Wynne, L. (2015). Can we integrate land-use and transport planning? An investigation into the use of travel planning regulation. Paper presented at the 21st International Conference on Urban Transport and the Environment, Spain. http://www.witpress.com/elibrary/wit-transactions-on-the-built-environment/146/34078
Xu, H., Wen, L. M., & Rissel, C. (2013). The relationships between active transport to work or school and cardiovascular health or body weight: A systematic review. Asia-Pacific Journal of Public Health, 25(4), 298–315. https://doi.org/10.1177/1010539513482965.
Yang, L., Panter, J., Griffin, S. J., & Ogilvie, D. (2012). Associations between active commuting and physical activity in working adults: Cross-sectional results from the Commuting and Health in Cambridge study. Preventive Medicine, 55(5), 453–457.
Zander, A., Rissel, C., & Bauman, A. (2013a). Cycling to work in sydney: Analysis of journey-to-work census data from 2001 and 2011. Camperdown: University of Sydney. Retrieved from http://sydney.edu.au/medicine/public-health/prevention-research/news/Cycling%20to%20work%20in%20Sydney%202001%202011_b.pdf
Zander, A., Rissel, C., Rogers, K., & Bauman, A. (2013b). Walking to work in Sydney: Analysis of journey-to-work Census data from 2001 and 2011. Camperdown: University of Sydney. Retrieved from http://sydney.edu.au/medicine/public-health/prevention-research/news/reports/Walking%20to%20work%202001-2011.pdf
Acknowledgments
We wish to convey our appreciation to members of the South Western Sydney and Sydney Health Promotion Services, who supported implementation of the main intervention study. Thanks also to the executives and staff from Liverpool Hospital in Sydney, who supported the study.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2018 Springer International Publishing AG, part of Springer Nature
About this chapter
Cite this chapter
Petrunoff, N., Crane, M., Rissel, C. (2018). A Case Study Exploring Associations of Quality of Life Measures with Car and Active Transport Commute Modes in Sydney. In: Friman, M., Ettema, D., Olsson, L.E. (eds) Quality of Life and Daily Travel. Applying Quality of Life Research. Springer, Cham. https://doi.org/10.1007/978-3-319-76623-2_10
Download citation
DOI: https://doi.org/10.1007/978-3-319-76623-2_10
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-76622-5
Online ISBN: 978-3-319-76623-2
eBook Packages: Social SciencesSocial Sciences (R0)