
Abstract
Healthcare sector had been recently witnessing lean concepts deployment. In order to enable effective implementation of lean concept in the healthcare domain, a structural model needs to be developed. The goal of this study is to analyze the relationship between lean constructs and healthcare performance. The model had been developed with five constructs and 20 measurement variables. The model was developed through the literature on lean deployment in healthcare unit and responses from healthcare experts. Forty-five responses were collected from healthcare experts. Partial least square (PLS) based Structural equation modeling (SEM) approach had been used for analysis. Based on the simulation results, it was found that “management” is the most driving enabler which influences people, process, technology, and other resources of the healthcare unit. The reliability of the developed model has been tested using Cronbach’s alpha and composite reliability. The study presents an attempt to develop a statistical model for lean concepts deployment so as to enhance healthcare performance.
Access provided by CONRICYT-eBooks. Download chapter PDF
Similar content being viewed by others

Keywords
1 Introduction
Lean concepts were initially applied in the manufacturing sector. During recent years, service sectors have started to adopt lean practices to reduce service cost. But, lean applications in healthcare sector have not been fully explored. Healthcare practices are subjected to developments in terms of increased number of patients, lower waiting time, and cost-effective procedures. The cost of healthcare procedures is increasing at a rapid rate (Vegting et al. 2012; Reijula and Tommelein 2012; Shazali et al. 2013). There exists a need to reduce costs and increase their efficiency, by providing an improved service with reduced service cost to the customer. Adoption of lean concepts in health care is one of the prime ways to achieve the need for improved service level. In order to enable effective deployment of lean in healthcare applications, a statistical model needs to be developed depicting the interrelationship between the constructs. The research objective of the study reported in this chapter is to identify appropriate lean constructs and to develop a statistical model linking the relation between lean concepts implementation and performance improvements. In this context, this chapter presents a study in which five constructs and 20 indicators are being developed based on literature review. Based on expert inputs, the model has been developed and analyzed using Structural equation modeling approach. The practical inferences are being derived. This chapter is organized as follows: Introduction section is followed by literature review, methodology, SEM model development, Inferences from SEM model, and conclusions.
2 Literature Review
The literature has been reviewed from the perspectives of Lean concepts deployment in healthcare domain and studies on modeling with reference to the healthcare sector.
2.1 Review on Lean Concepts Deployment in the Healthcare Sector
Dahlgaard et al. (2011) developed a conceptual model to assess, measure, diagnose, and improve healthcare organizations. Five universities and five hospitals in Denmark were considered in the study. Based on the response from employees and management, ILL index (Innovativeness, Learning, and Lean) was calculated to measure the level of excellence prevailing in healthcare units.
de Souza and Pidd (2011) studied the similarities and differences in implementing lean concepts in the manufacturing sector and healthcare sector. They discussed the factors that hinder the successful implementation of lean practices in the healthcare sectors. Some of the barriers they have shown are resistance to change, management hierarchy, professional skills, and performance measurement methods.
Radnor et al. (2012) performed four multilevel case studies on lean implementation in the English National Health Service (NHS). It was observed that the healthcare sectors lacked in embracing broad lean thinking for system-wide benefits. Gitlow et al. (2013) analyzed the factors that contribute to preventing medical accidents in healthcare units. A model was developed to suggest “Standard Best Practices” in healthcare units.
Costa and Godinho Filho (2016) carried out a literature-based study. One hundred and seven research papers in lean healthcare were evaluated and recent trends were identified. In the study, lean implementation in health care in different countries was analyzed. It was observed that 5S and Value Stream Mapping (VSM) were the most frequently used lean tools in the healthcare sector.
Hussain et al. (2016) conducted a study to assist the deployment of lean in healthcare delivery system. In the study, Analytical Hierarchical Process (AHP) was used to decompose complex, unstructured issues prevailing in lean healthcare and organize them into a set of components in a multilevel hierarchical form. Twenty-one healthcare wastes were identified and ranked based on the responses from experienced healthcare professionals.
Setijono et al. (2010) conducted a study in Swedish emergency ward to find the best number of surgeons and doctors to be employed so as to reduce patients’ Non-Value Added Time (NVAT) and Total Time in the System (TTS). An ARENA model of the patient service cycle was developed and simulated to infer the results. Thirteen percent reduction of patients’ NVAT was achieved in the study.
Jorma et al. (2016) studied the benefits of lean concept implemented in healthcare for managing the treatment process. They have done a questionnaire survey with 248 responders working in the healthcare sector for analyzing the response regarding the implementation of lean in health care. From the survey, they got positive responses regarding benefits of successful implementation of lean tools and techniques.
Lindskog et al. (2016) aimed toward finding the extent of lean practices implementation in health care. Multiple linear regression models have been used to study the extent of implementation of lean tools. They concluded that VSM, 5S, and standardized work lean tools that can enhance the working condition of employees in the healthcare sector.
Kovacevic et al. (2016) reviewed the lean tools and techniques that have been successfully implemented in the healthcare sectors. They reviewed the benefits of most frequently used lean tools, namely 5S, VSM, Kaizen, and Visual management. They found several benefits of implementing lean tools. They are reduction in patient average waiting time, significant improvement in flow time, and reduction in manpower.
Eriksson et al. (2016) conducted semi-structured interviews in two Swedish hospitals to understand practitioners perception on lean deployment. It was observed that lean implementation being a bottom-up approach often reflected in conflicting ideas with top management which usually follows top-down approach. The study emphasized the necessity to frame lean practices that have consensus from both technical experts and top management.
2.2 Review of Modeling Studies in Healthcare Sector
Hussey and Eagan (2007) used SEM methodology to validate the developed environmental performance model on environmental management systems in Small and Medium Enterprises (SMEs). From the results, it was observed that “leadership” greatly influences “environmental planning” and “environmental management” which in turn greatly influences “environmental results”.
Hussey and Eagan (2007) developed a model to understand the factors influencing customer satisfaction in the healthcare sector. “High performance work system”, “service quality”, “customer orientation” were identified as the critical factors. The model was statistically validated using SEM approach. It was observed that “High performance work system” acted as the key driving factor which significantly influenced “customer orientation” and “service quality”. It was also observed that all factors significantly influenced in providing better customer satisfaction.
Martín-Consuegra et al. (2007) analyzed the interaction among price fairness, customer satisfaction, loyalty, and their overall impact on price acceptance by the customers. A service industry in the airline sector was identified as the case unit to collect the responses. Based on the responses, a path model was developed which indicated the factor relationship that influenced price acceptance by the customers. SEM approach was used to validate the model. It was observed that price fairness greatly influenced customer satisfaction and loyalty; customer satisfaction has significant influence on loyalty; price fairness, customer satisfaction, and loyalty had combined significant influence on price acceptance.
Chahal and Bala (2012) studied the interrelations among factors influencing service brand equity in the healthcare sector. SEM approach was used to analyze the data collected from 206 respondents. It was observed that brand loyalty and perceived quality had a significant influence on brand equity. Brand image was found to be mediating variable which had an indirect effect on brand equity through brand loyalty.
Hussain et al. (2016) discussed the successful lean practices implemented in the healthcare sector. They have shown a case study of a public healthcare system situated in Abu Dhabi. They also discussed seven wastes associated with lean practices in health care along with 21 sub-waste. Their aim was to prioritize the influential waste with the help of Analytical Hierarchy Process (AHP) and selection of waste minimization technique. They found that transportation waste and inventory waste are the most critical wastes pertaining to the healthcare sector.
Tarhini et al. (2017) analyzed the effect of cultural values at the individual level on user’s acceptance of e-learning. Responses were collected from 569 undergraduate and postgraduate students regarding their usage of e-learning tools. A statistical model was developed and validated using SEM approach. “Quality of work life”, “Uncertainty avoidance”, “Subjective norms”, and “Behavioral intention” were the four cultural dimensions considered in the study. It was observed that all four constructs had a significant influence on “Technology acceptance level”.
Patri and suresh (2017) aimed toward finding the relationship between factors influencing implementation of lean practices in health care. They made a hierarchy structure of considered factors using Interpretive Structural Modeling. Ranking of factors was done based on the driving power and dependence power of factors. From the analysis, they found that leadership is the most important factor in successful implementation of lean practices in the healthcare sector.
Mitchell et al. (2017) aimed toward finding the relationship between size of the hospital, patient comorbidity and time to customer in hospital, i.e., time difference between admission and discharge with the help of SEM. They concluded that patient comorbidity had a great influence on timing of infection.
Zhao et al. (2017) studied the direct and indirect effects of socioeconomic status on rectal cancer risk in patients. Dietary patterns were collected among 39 food groups from the people of Newfoundland and Labrador. SEM approach was used in the study and the results showed that dietary pattern greatly influenced socioeconomic status among people which in turn greatly influenced the risk of acquiring rectal cancer.
2.3 Research Gaps
Though there are certain studies reported on lean concepts adoption in the healthcare domain, and statistical modeling for lean concepts adoption is attempted, there exists a potential for developing a statistical model linking lean concepts adoption and operational performance.
3 Methodology
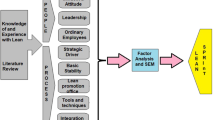
The methodological steps are shown in Fig. 1. Critical parameters that influence lean deployment in the healthcare sector were identified as constructs. Based on the literature review and inputs from healthcare practitioners, measured variables corresponding to each construct were developed and a model depicting the interrelations between constructs was being developed. The model developed entails five constructs and 20 measured variables. A case healthcare unit in the Tamil Nadu state of India is identified for the study. Forty-five responses were collected from healthcare practitioners of the case healthcare unit for the developed SEM model. The model is then tested for “reliability” and the results are obtained by simulating the model.

Methodology
4 Development of Statistical Model Using SEM
Structural Equation Modeling (SEM) is a multivariate statistical approach that is used to analyze structural relationships. It combines factor analysis and multiple regression analysis for analysis of the structural relationship between measured variables and latent constructs. Multiple relationships among factors present in the model and their combined interaction effect can be simultaneously estimated using SEM in a single analysis.
4.1 PLS-SEM
Partial Least Squares (PLS) approach to SEM is highly beneficial for basic investigation. It is an alternative to covariance-based SEM. It is used for problems involving formative indicators, small sample size, and non-normal data. It includes two sub-models: measurement and structural model. Measurement model depicts relationships between observed data and latent variables; whereas structural model indicates relationships between latent variables. PLS-SEM is used to explore, analyze, and test the conceptual models and theory.
4.2 Cronbach’s Alpha
Cronbach’s alpha is a measure of internal consistency, i.e., the measurement of closeness between set of items belonging to a group. If alpha value is high, it implies that the measure is non-unidimensional. It is a measure of scale reliability. Apart from internal consistency measurement, it is desired to provide evidence that the subject scale is unidimensional, further analyses can be performed. Based on research studies, it was found that the value of Cronbach’s alpha of 0.7 or higher is preferred.
4.3 Composite Reliability
The composite reliability is typically parameter examined when PLS is applied as analysis method. It is the measure of internal consistency. It is a measure of overall reliability of a set of heterogeneous but similar items.
In SEM model, the constructs used can be classified into two types namely: endogenous and exogenous constructs. Endogenous constructs are equivalent to dependent variables and exogenous constructs are equivalent to independent variables used in multiple regression model.
The following steps are involved in building the model:
Step 1: Defining individual construct—proper definition has to be given for each construct theoretically.
Step 2: Developing the measurement model—it is made to show the relationship between exogenous variables and endogenous variable, here an arrow has to be drawn from measured variable to construct.
Step 3: Design the model to provide empirical results: here, the model has to be designed by minimizing the identification problem. This can be done by using rank condition and order condition method.
Step 4: Specify the structure model: Here, the structural path has to be drawn in between constructs. In this model, an arrow cannot enter into the exogenous construct. For representing the structural relationship between any two constructs, a single-headed arrow has to be used.
Step 5: Examine the structural model validity—Chi-Square test has been used to validate the structural model.
The model developed entails five constructs and 20 measured variables. The constructs and variables are developed through the literature on lean deployment in health care and responses from healthcare experts and academicians. Table 1 shows the constructs and their corresponding measured variables being identified. Constructs are being identified as Management people, process, technology and lean performance. For example, Management Construct consists of Variables such as Top management support, Organizational structure and Incentives and training program.
Forty-five responses were collected from healthcare experts in the case healthcare unit. Structure of the model developed, results of the model’s composite reliability, Cronbach’s alpha values of the constructs pertaining to the SEM model and inferential results from model simulation are shown in Figs. 2, 3, 4 and 5 respectively. Figure 2 shows the relationship between the constructs and its associated latent variables. The model consists of five constructs namely People, Management, Process, Technology and Lean Performance. Indicator reliability and internal consistency reliability are the two main reliability constraints that are to be checked. The reliability values are computed in SmartPLS by using the command Calculate ≫ PLS algorithm. Indicator reliability is computed as cronbach’s alpha value and internal consistency reliability is computed as composite reliability value. The indicator reliability value and internal consistency reliability value must be greater than 0.7 for accepting the construct. If the values are found to be less than 0.7, further scale refinement has to done by either increasing the sample size or by altering the input values. Figures 3 and 4 show the obtained composite reliability values and Cronbach’s alpha values for the developed structural model. Figure 5 shows the cumulative path values of the latent variables based on the significance of relationships among the constructs.

Snapshot depicting relationship among constructs

Composite reliability of the developed SEM model

Cronbach’s alpha values of the developed SEM model

SEM results for depicting the significance of relationships among constructs
Composite reliability test and Cronbach’s alpha test are conducted to find the reliability of the developed SEM model. From the simulation results, it is observed that “management” is the most driving enabler which significantly influences “people”, “process”, “technology” and other resources present in the healthcare unit. It is also observed that “people”, “process”, and “technology” individually have significant influence in deploying lean practices in the healthcare sector.
5 Practical Implications
The developed model enabled the medical practitioners and experts to systematically develop the statistical model linking the identified Constructs and operational performance. The study also enabled the identification of most driving enablers for lean concepts adoption in healthcare domain.
6 Conclusions
The main principle of lean is to eliminate waste activities which can be carried out by identifying critical and bottleneck stations in the process flow and bringing remedial measures so as to achieve a seamless flow for the overall process. From a healthcare perspective, lean practices can reduce patient waiting time, reduce patient stay in healthcare unit, increase visibility of the activities involved in health care, reduces medical defects, increases morale of staffs and practitioners in healthcare units, and reduces the cost involved in providing the service without compromising the quality of service being delivered. Unlike in manufacturing sector, lean practices which initially had its inception in shop floor cannot be directly adopted to service sector like healthcare services. In the present study, the critical factors influencing lean deployment in the healthcare sector is identified and their effect on establishing lean in health care is validated using SEM approach. It is observed that all four constructs namely, “management”, “people”, “process”, and “technology” have a significant influence on the successful deployment of lean in the healthcare sector. It is also observed that “management” being the prime driving factor has significant contribution in enhancing “people”, “process”, “technology” constructs, and other resources used in providing the healthcare service.
7 Limitations and Future Work
The study is focused on a single healthcare unit. In future, more number of studies could be conducted with reference to various other healthcare units to improve the practical validity of the approach. In the present study, 20 factors are considered. In future, number of factors could be increased to deal with managerial advancements in healthcare domain. Also, a structural model could be developed based on ISM approach and the model could further be statistically validated using SEM.
References
Bhasin, S. (2011). Measuring the Leanness of an organisation. International Journal of Lean Six Sigma, 2(1), 55–74.
Chahal, H., & Bala, M. (2012). Significant components of service brand equity in healthcare sector. International Journal of Health Care Quality Assurance, 25(4), 343–362.
Costa, L. B. M., & Godinho Filho, M., (2016). Lean healthcare: Review, classification and analysis of literature. Production Planning & Control, 27(10), 823–836.
Dahlgaard, J. J., Pettersen, J., & Dahlgaard-Park, S. M. (2011). Quality and lean health care: A system for assessing and improving the health of healthcare organisations. Total Quality Management & Business Excellence, 22(6), 673–689.
Dellve, L., Williamsson, A., Strömgren, M., Holden, R. J., & Eriksson, A. (2015). Lean implementation at different levels in Swedish hospitals: The importance for working conditions and stress. International Journal of Human Factors and Ergonomics, 3(3–4), 235–253.
de Souza, L. B., & Pidd, M. (2011). Exploring the barriers to lean health care implementation. Public Money & Management, 31(1), 59–66.
Doolen, T. L., & Hacker, M. E. (2005). A review of lean assessment in organizations: An exploratory study of lean practices by electronics manufacturers. Journal of Manufacturing systems, 24(1), 55–67.
Eriksson, N., Müllern, T., Andersson, T., Gadolin, C., Tengblad, S., & Ujvari, S. (2016). Involvement drivers: A study of nurses and physicians in improvement work. Quality Management in Healthcare, 25(2), 85–91.
Gitlow, H., “Amy” Zuo, Q., Ullmann, S. G., Zambrana, D., Campo, R. E., Lubarsky, D., et al. (2013). The causes of never events in hospitals. International Journal of Lean Six Sigma, 4(3), 338–344.
Hussain, M., Malik, M., & Al Neyadi, H. S. (2016). AHP framework to assist lean deployment in Abu Dhabi public healthcare delivery system. Business Process Management Journal, 22(3), 546–565.
Hussey, D. M., & Eagan, P. D. (2007). Using structural equation modeling to test environmental performance in small and medium-sized manufacturers: Can SEM help SMEs? Journal of Cleaner Production, 15(4), 303–312.
Jorma, T., Tiirinki, H., Bloigu, R., & Turkki, L. (2016). Lean thinking in Finnish healthcare. Leadership in Health Services, 29(1), 9–36.
Kovacevic, M., Jovicic, M., Djapan, M., & Zivanovic-Macuzic, I. (2016). Lean thinking in healthcare: Review of implementation results. International Journal for Quality Research, 10(1).
Lindskog, P., Hemphälä, J., Eklund, J., & Eriksson, A. (2016). Lean in healthcare: Engagement in development, job satisfaction or exhaustion? Journal of Hospital Administration, 5(5), 91.
Martín-Consuegra, D., Molina, A., & Esteban, Á. (2007). An integrated model of price, satisfaction and loyalty: An empirical analysis in the service sector. Journal of Product & Brand Management, 16(7), 459–468.
Mazzocato, P., Savage, C., Brommels, M., Aronsson, H., & Thor, J. (2010). Lean thinking in healthcare: A realist review of the literature. Quality and Safety in Health Care, 19(5), 376–382.
Mitchell, B. G., Anderson, M., & Ferguson, J. K. (2017). A predictive model of days from infection to discharge in patients with healthcare-associated urinary tract infections: A structural equation modelling approach. Journal of Hospital Infection, 97(3), 282–287.
Patri, R., & Suresh, M. (2017). Factors influencing lean implementation in healthcare organizations: An ISM approach. International Journal of Healthcare Management, 1–13. https://doi.org/10.1080/20479700.2017.1300380.
Radnor, Z. J., Holweg, M., & Waring, J. (2012). Lean in healthcare: The unfilled promise? Social Science and Medicine, 74(3), 364–371.
Reijula, J., & Tommelein, I. D. (2012). Lean hospitals: A new challenge for facility designers. Intelligent Buildings International, 4(2), 126–143.
Setijono, D., Mohajeri Naraghi, A., & Pavan Ravipati, U. (2010). Decision support system and the adoption of lean in a swedish emergency ward: Balancing supply and demand towards improved value stream. International Journal of Lean Six Sigma, 1(3), 234–248.
Sharma, V., Dixit, A. R., & Qadri, M. A. (2015). Impact of lean practices on performance measures in context to Indian machine tool industry. Journal of Manufacturing Technology Management, 26(8), 1218–1242.
Shazali, N. A., Habidin, N. F., Ali, N., Khaidir, N. A., & Jamaludin, N. H. (2013). Lean healthcare practice and healthcare performance in Malaysian healthcare industry. International Journal of Scientific and Research Publications, 3(1), 1–5.
Tarhini, A., Hone, K., Liu, X., & Tarhini, T. (2017). Examining the moderating effect of individual-level cultural values on users’ acceptance of E-learning in developing countries: A structural equation modeling of an extended technology acceptance model. Interactive Learning Environments, 25(3), 306–328.
Vegting, I. L., van Beneden, M., Kramer, M. H. H., Thijs, A., Kostense, P. J., & Nanayakkara, P. W. (2012). How to save costs by reducing unnecessary testing: Lean thinking in clinical practice. European Journal of Internal Medicine, 23(1), 70–75.
Vinodh, S., & Chintha, S. K. (2011). Leanness assessment using multi-grade fuzzy approach. International Journal of Production Research, 49(2), 431–445.
Vinodh, S., & Joy, D. (2012). Structural equation modelling of lean manufacturing practices. International Journal of Production Research, 50(6), 1598–1607.
Wahab, A. N. A., Mukhtar, M., & Sulaiman, R. (2013). A conceptual model of lean manufacturing dimensions. Procedia Technology, 11, 1292–1298.
Zhao, J., Zhu, Y., & Wang, P. (2017). Examining the direct and indirect effects of socioeconomic status (SES) on colorectal cancer risk using structural equation modeling. European Journal of Cancer, 72, S56.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2018 Springer International Publishing AG
About this chapter

Cite this chapter
Vinodh, S., Dhakshinamoorthy, A.M. (2018). Application of Structural Equation Modeling for Analysis of Lean Concepts Deployment in Healthcare Sector . In: Davim, J. (eds) Progress in Lean Manufacturing. Management and Industrial Engineering. Springer, Cham. https://doi.org/10.1007/978-3-319-73648-8_4
Download citation
DOI: https://doi.org/10.1007/978-3-319-73648-8_4
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-73647-1
Online ISBN: 978-3-319-73648-8
eBook Packages: EngineeringEngineering (R0)