
Abstract
Canonical thyroid hormone (TH) signaling results from the interaction of T3 with nuclear receptors and stimulation or repression target genes. Ligand (T3) availability is under tight control of several intracellular checkpoints, which enable target cells to modify their own T3 fingerprint. A crucial step of intracellular T3 metabolism is catalyzed by the deiodinases. These enzymes can, within the single cell, enhance (D1 and D2) or reduce (D3) T3 concentrations. Thyroid hormone transport within the target cells is also a limiting step of thyroid hormone action. Various specific transporters have been isolated for the entrance and the clearance of the iodothyronines and constitute a complex system of active transport of THs inside and outside the cells. Concerted modulation of the different TH regulating factors is responsible for a spatiotemporal precise adaptation of the hormonal signal to the different cell-specific requirements.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others

Keywords
Introduction
Canonical thyroid hormone (TH) signaling results from the interaction of T3 with nuclear receptors and stimulation or repression of target genes. Ligand (T3) availability is under tight control of several intracellular checkpoints, which enable target cells to modify their own T3 fingerprint. A crucial step of intracellular T3 metabolism is catalyzed by the deiodinases. These enzymes can, within the single cell, enhance (D1 and D2) or reduce (D3) T3 concentrations. Thyroid hormone transport within the target cells is also a limiting step of thyroid hormone action. Various specific transporters have been isolated for the entrance and the clearance of the iodothyronines and constitute a complex system of active transport of THs inside and outside the cells. Concerted modulation of the different TH regulating factors is responsible for a spatiotemporal precise adaptation of the hormonal signal to the different cell-specific requirements.
Peripheral Metabolism of Thyroid Hormones
The thyroid gland accumulates iodide from the circulation to produce the thyroid hormones T4 and T3. These are iodinated molecules that exert diffuse and pleiotropic effects in vertebrates. Although both molecules are biologically active, T3 is the most active thyroid hormone that can bind to thyroid hormone receptors and regulate the expression of thyroid hormone-regulated genes [1]. T4 (levothyroxine) is a pro-hormone that must be converted into T3 (triiodothyronine) to be active (Fig. 1). A consequence of this process is that there are two sources of T3, one directly produced and secreted by the thyroid gland and one derived from tissue conversion of T4 into T3. Of note, the human thyroid produces less than 20% of the body’s T3 (about 30 μg/die) and peripheral conversion is responsible for 80% of it [2]. Thyroid-generated T3 (about 5 μg/die) is obtained partly via intracellular thyroglobulin digestion and partly via intrathyroidal T4-to-T3 conversion. These two processes produce thyroidal secretion of both T4 and T3 in a molar range of approximately15–11:1; this ratio may change depending on such conditions as iodine supplementation or thyroid disease. The conversion of T4 to T3 occurs consequent to the removal of an outer-ring iodine on T4 (known as “5′-deiodination”) which is catalyzed by two enzymes, deiodinases type 1 and type 2 (D1 and D2) [3]. Importantly, these enzymes are expressed in a tissue-specific fashion and are independently regulated to enable different tissues to modulate their “thyroid status” (i.e., to regulate the percentage of saturation of thyroid hormone receptor in the single cell) irrespective of serum thyroid hormone levels. 5′-Deiodination by D1 and D2 can increase intracellular T3 levels thereby potentially leading to intracellular thyrotoxicosis. In the opposite direction, type 3 deiodinase (D3) is considered the physiological inactivator of thyroid hormones because it catalyzes the conversion of T4 and T3 into inactive products (rT3 and T2) via a 5-deiodination reaction. This process locally produces a state of relative hypothyroidism.

Thyroid hormones landscape . Thyroid hormones T3 and T4, produced by the thyroid gland, are transported by the plasma to each target tissue where they can be activated or inactivated by deiodinases. Only the active form, T3, can bind receptors thereby activating or repressing the expression of target genes
Deiodination and Deiodinases
Every cell in the body is a potential target of thyroid hormones, which regulate the metabolism, growth, and differentiation. In healthy conditions, the thyroid gland produces about 80% of the body’s T4 and about 20% of the body’s T3. However, T3 is considered the only bioactive thyroid hormone because it has a much stronger affinity for thyroid receptors than the other iodothyronines.
Conversion of T4 to T3 by deiodination is the first step of thyroid hormone action and not only is regulated by the thyroid but is also catalyzed within target cells by a family of three seleno-proteins, the iodothyronine deiodinases, that catalyze the reductive dehalogenation of iodothyronines, which is the major metabolic pathway regulating thyroid hormone action at pre-receptoral level [1, 3]. Depending on whether deiodination occurs on the inner (IDR) or outer ring (ODR) of the iodothyronine substrate, deiodination results in an activating pathway, or inactivating pathway, respectively. The rare amino acid selenocysteine (Sec) is essential for the dehalogenation reaction [4], as demonstrated by the finding that replacement of selenocysteine-cysteine drastically reduces the affinity of all three deiodinases for their substrates [3]. The main features of the deiodinases are shown in Table 1.
Type 1 deiodinase (D1) catalyzes both inner- and outer-ring deiodination mainly in the liver, kidney, and thyroid. D1-dependent deiodination is the only deiodination highly sensitive to inhibition by PTU [5]—a finding that led to the first demonstration of the specificity of the T4-to-T3 conversion [6]. The human Dio1 gene consists of four exons. The selenocysteine codon is located in exon 2 and the selenocysteine insertion sequence (SECIS) element is located in the fourth exon [7]. The Dio1 gene encodes a protein of 27 kDa, and the molecular mass of the solubilized wild-type enzymes is about 50–60 kDa, which suggested that, like the other two enzymes, D1 forms homodimers in its native form thanks to integral membrane residues [8].
Thanks to its tissue-specific expression, D1 contributes to the regulation of systemic T3 levels by providing a significant portion of the circulating plasma T3 in euthyroid vertebrates, including humans [9,10,11]. In hyperthyroid conditions, increased thyroidal D1 activity is the first cause of the elevated T3 concentrations observed in hyperthyroid patients. Apart from hyperthyroidism, D1 plays critical roles in the non-thyroidal illness syndrome (NTIS) and in several human neoplasias [7]. Although the pathogenesis of NTIS is still controversial and some observations seem to question the effective roles played by deiodinases in the low T3 levels in illness [12, 13], it has been demonstrated that the peripheral T4-to-T3 conversion is reduced in illness due to a decrease in both hepatic/renal D1 activity and skeletal muscle D2 activity, which in turn increases the levels of rT3 and T2 [14, 15].
Besides its canonic deiodination activity , D1 modulates the clearance of TH [16]. Indeed, D1 has a remarkable substrate preference for reverse T3 (rT3) as well as for sulfated iodothyronines and could act as a scavenger to recycle iodine to enable the thyroid homeostatic production of THs [16]. Accordingly, in D1KO mice, iodothyronines escape deiodination and are massively excreted with a marked loss of the associated iodine, which demonstrates that D1 serves to recycle iodine within the organism and might be particularly important in an iodine deficiency setting [16].
Type 2 deiodinase (D2) mediates primarily outer-ring deiodination, and given its high affinity for T4, it is considered the main activator of T3 at peripheral level [17]. The human D2 protein is approximately 31 kDa and contains a hydrophobic NH2 terminus and two selenocysteine residues, one in the active center and the other located close to the 3′ end of D2 mRNA [3, 18].
The activity of D2 has been extensively studied in brain and brown adipose tissues (BATs), where the D2-mediated T4-to-T3 conversion is an essential component of thyroid hormone action. In the brain, D2 is expressed in astrocytes, which convert T4 into T3 for the brain requirement by producing more than 75% of the nuclear T3 in the cerebral cortex in rat [2]. In the fetus, the brain almost entirely relies on the T3 generated locally by D2, while systemic T3 plays a critical role in the late postnatal and adult stages [19]. Such a finely tuned regulation of D2 activity correlates with T3’s highly sensitive requirement of TH in the developmental period and shows how deiodinases can activate or inactivate TH in specific extraglandular tissues, in a spatial and temporal regulated fashion.
In brown adipose tissue (BAT) , D2 is barely expressed in normal conditions but increases 10-fold–50-fold during cold exposure [20]. In vivo, BAT-specific D2 expression is essential for adaptive thermogenesis. Indeed, despite normal plasma T3 concentrations, cold-exposed D2KO mice are hypothermic and cold-intolerant due to impaired BAT thermogenesis, and they survive only by compensatory shivering which results in acute weight loss [20]. Accordingly, in vitro, brown adipocytes from D2KO mice have a markedly attenuated susceptibility to sympathetic stimuli by norepinephrine and forskolin, which induced only modest lipolysis, UCP1 mRNA, and O2 consumption due to impaired cAMP generation [20].
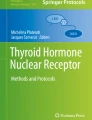
Recent findings have shown that D2 plays a role also in the skeletal muscle. Although it has long been known that D2 is expressed in the muscle [21], its biological role in the muscle has only recently been demonstrated because of its low levels [22, 23]. We recently demonstrated that D2 is required for normal mouse skeletal muscle differentiation of muscle stem cells (satellite cells) and regeneration (Fig. 2). The regenerative ability of mice lacking D2 and D2-null satellite cells is sharply delayed and can be rescued in vitro by T3 treatment. Furthermore, more sensitive assays of muscle D2 activity have shown that D2 is present and higher in slow than in fast muscles [24, 25].

Role of D2 and the local production of T3 in myogenesis and satellite cell differentiation. Quiescent satellite cells (MSC) can be activated by a stimulus such as a trauma and, once activated, undergo a program of regeneration-differentiation which is tightly regulated by T3. Type 2 deiodinase is positively regulated by the transcriptional factor FoxO3a and is upregulated during muscle differentiation. T3 activation by D2 increases MyoD expression and enables proper differentiation of myofibers
Type 3 deiodinase (D3) has only inner-ring deiodination ability, thus preventing T4 activation and terminating T3 action, which is the main physiological inactivation of thyroid hormone action [26]. Human and mouse Dio3 genes comprise a single exon, coding for a protein of 278 residues, with a molecular mass of about 32 kDa, including a selenocysteine-encoding TGA in the catalytic pocket and an SECIS element in the 3’UTR [27]. A unique aspect of D3 is its high expression in developmental tissues and its absence in almost all adult tissues (with the exception of the skin and brain). Therefore, studies on D3 have focused on its role during development and have shown that D3 action is critical to protect the fetus from excessive exposure to active thyroid hormone [28]. However, studies conducted in the last two decades have shown that D3 expression is reactivated in specific pathophysiological contexts correlated with hyperproliferation conditions, such as tissue repair [29,30,31], inflammation [32], and cancer [33, 34]. Akin to fetal growth, most of these conditions are characterized by an elevated proliferation rate and cell growth, thereby introducing the new concept of D3 as oncofetal protein [26]. One of the most robust indications that many cancer cells reactivate D3 expression came from the discovery of the impressively low serum levels of THs found in patients with juvenile and adult hemangiomas, which was classified as “consumptive hypothyroidism ” since it was discovered that by producing high levels of D3, the inactivation rate of thyroid hormone in the tumor exceeded the secretory capacity even of the thyroid gland, thus resulting in hypothyroidism [35, 36]. Later, two similar examples in basal cell carcinomas (BCC) of the skin and in colon cancer showed that D3 expression and activity were much higher in these two epithelial tumors than in the relative normal tissue. D3 inactivation in BCC and in colon cancer drastically reduces tumorigenesis both in vivo and in vitro. Importantly, the Shh/Gli2 pathway, miR21 pathway, and the Wnt-/β-catenin pathway are positive regulators of D3 expression in these two neoplasias, which highlight the relevance of D3 in oncogenic networks [26, 37].
Heart failure and several cardiac disorders are accompanied by alterations in TH levels and D3 expression [38, 39]. D3 is significantly induced during severe heart failure, and the fetal program is reactivated [40]. The finding of direct regulation of D3 transcription by the hypoxia-inducible factor (HIF-1α) reinforced the concept of D3 as a critical TH regulator in the cardiac-specific hypothyroid condition that follows myocardial infarct [38].
D3 also participates in the innate immune response by reducing T3 bioavailability and probably by supplying iodine required by myeloperoxidase to enable inflammatory cells to kill microbes [41]. Extensive studies carried out by Boelen and Fliers have shown that inflammation is often associated with low serum TH levels and with changes in the expression of liver D1 and D3 and of muscle D2 and D3 [32]. Both acute and chronic inflammation are marked by high D3 expression in neutrophils that infiltrate infected organs, predominantly polymorphonuclear cells and granulocytes, suggesting that enhanced degradation of T3 during inflammation may contribute to such a process, although the underlying mechanism is not yet known [42,43,44]. Similarly, D3 has been suggested as one of the effectors contributing to the pathogenesis of NTIS by reducing circulating TH levels during chronic illness [45]. Indeed, reactivation of D3 activity has been reported in the liver and skeletal muscle of critically ill patients, and moreover, high D3 levels were found in skeletal muscle biopsies from patients with septic shock and NTIS [46]. Importantly, D3 expression in these contexts positively correlates with serum rT3 [47] and negatively correlates with the serum T3/rT3 ratio [45].
Liver regeneration is a classic example of D3 reactivation associated with cellular proliferation. After keratectomy of 70% of the liver, quiescent liver cells reenter the cell cycle (G1 phase) and start a proliferation phase as the first step of liver regeneration [48]. These early regeneration events are characterized by reactivation of many fetal genes, which are not expressed in normal adult liver [48, 49]. D3 is among these genes [29]. D3 activity indeed was increased tenfold 20 h after partial hepatectomy in mice and was associated with a decrease in D1; BrdU levels, marker of proliferation, correlate with D3 activity. Importantly, serum T3 and T4 levels decreased and reached minimum levels 36 h after partial hepatectomy, thereby coinciding with the peak in D3 activity and BrdU incorporation [29].
The elucidation of the role played by deiodinases in all the above-reported biological processes revealed the importance of the deiodinases in the homeostasis of thyroid hormone action and opened the possibility of exploiting deiodination to specifically modulate TH action in local circumstances and to overcome alterations of circulating hormone levels.
Transporters
The lipophilic biochemical nature of thyroid hormones has long supported the notion that passive diffusion across the plasma membrane is sufficient to enable thyroid hormones to bypass the bilayer of the eukaryotic plasma membrane. Only three decades ago did it emerge that specific carrier-mediated mechanisms of active transport are necessary for thyroid hormones [50]. Subsequently, many transporter families were identified, among which, monocarboxylate transporters (MCT 1–10), organic anion-transporting polypeptides (OATP) , the L-type amino acid transporters LAT1 and LAT2, and bile acid transporters [51, 52]. These transporters mediate TH uptake in an energy- and Na+-dependent manner [53], and together with deiodinase action, this represents a critical pre-receptoral step in the control of TH availability in the cell.
Evidence of the physiological relevance of the MCT8 transporter came from the discovery of patients carrying the MCT8 mutation who had elevated serum T3 levels and severe psychomotor retardation, thereby indicating that MCT8 plays a pivotal role in brain development [54, 55]. Male MCT8-null patients are affected by the Allan-Herndon-Dudley syndrome (AHDS) , which is an X-linked inherited brain disorder that causes severe neurologic dysfunctions [54, 55]. It also causes central hypotonia, muscular hypoplasia, spastic tetraplegia, and a global delayed development and myelination [56]. The observation that fibroblasts from AHDS-affected patients, associated with intracellular hypothyroidism, increased D2 activity and elevated TSH levels demonstrates that the absence of MCT8 generates a state of relative insensitivity to thyroid hormone. The clinical symptoms associated with AHDS indicate that the MCT8-expressing neurons are in a hypothyroid state consequent to the inactivating mutations in MCT8 [56,57,58,59].
Mice models of MCT8 knockout only partially recapitulate the TH-associated abnormalities of MCT8-mutant patients [59,60,61]. Indeed, unlike the severe neurological phenotype of patients with MCT8 mutations, both male and female MCT8 KO mice have a very mild neurologic phenotype. Nevertheless, MCT8 knockout animals fully recapitulate the alterations in circulating TH levels of AHDS patients, namely, impaired brain T3 uptake and decreased brain levels of T4 and T3. Unexpectedly, the liver and kidneys were in a thyrotoxic situation: increased T4 and T3 uptake and elevated T4 and T3 levels [59]. A second mouse model, lacking both MCT8 and OATP1C1 transporters, was much more similar to AHDS in terms of brain abnormalities [62], thus indicating partial overlapping of the functions of thyroid hormone transporters in the brain. MCT8/OATP1C1 KO mice showed similar alterations in peripheral TH homeostasis to those of MCT8 KO mice. Importantly, the uptake of T3 and T4 was much lower in the double KO mice than in the single mutant MCT8 KO and OATP1C1 KO mice, and, moreover, the double KO mice displayed pronounced abnormalities and compromised differentiation of GABAergic interneurons in the cerebral cortex [62].
Studies by Heuer [63] and Bernal [64] elegantly illustrated that the brain regulates its T3 supply by differentially expressing specific transporters and deiodinases (Fig. 3). Their model starts with the passage of T4 by OATP1C1 through the blood-brain barrier and the uptake of T4 in astrocytes. Subsequently, astrocytes activate a D2-mediated T4-to-T3 conversion and release T3, which is available for the uptake into the neurons by MCT8. Finally, neurons can degrade T3 by the action of type 3 deiodinase. Overall, this complex regulation exemplifies how the finely tuned expression of TH modulators can closely control TH action in a spatial- and time-dependent manner and reveals the unique function of MCT8 and OATP1C1 in mediating the passage of T3 into the central nervous system.

Complex role of transporters and deiodinases in thyroid hormone metabolism in the central nervous system. T3 and T4 from the circulation can pass the blood-brain barrier. Upon entering the brain, T4 reaches the astrocytes via Oatp1c1-mediated transport. In the astrocytes, D2-mediated deiodination produces the active hormone T3, which can enter the neurons via MCT8-mediated transport
It is important to note that intracellular TH availability depends not only on its rate of uptake but also on the rate of TH efflux, which also occurs via active transport across the plasma membrane. All the transporters identified so far are capable of bidirectional transport, which involves both the intra- and extracellular exchanges [52].
Role of Deiodinases and Regulation of Local TH Metabolism
Local Thyroid Hormone Metabolism
Appropriate levels of thyroid hormones are required in all tissues in many pathophysiological conditions. Consequently, it is not surprising that correct spatial and temporal expression of the three deiodinases, receptors, and transporters is an essential condition in healthy humans. The wide-ranging actions of local modulation of TH must therefore be exquisitely regulated at different levels. Many regulators of deiodinase expression and activity have been discovered in the last two decades. The first regulator of deiodinase expression and activities are the same TH substrates, as classical homeostatic feedback mechanism. T3 levels positively regulate D1 expression at a transcriptional level (the D1 promoter comprises two thyroid hormone-responsive regions [TREs] ) [65, 66]. D2 expression is closely controlled by T4 at both transcriptional and posttranscriptional level [67]. D3 expression is also T3- dependent being positively regulated by TH and thus represents a powerful homeostatic mechanism of TH inactivation in thyrotoxic states [68]. Besides T3, other endocrine factors regulate D1 transcription, namely, GH [69], TSH [70], and glucocorticoids [71, 72].
D2 expression is cAMP-dependent as elegantly demonstrated in BAT [20]. CREB controls D2 transcription via a canonic CRE binding site located in the human Dio2 promoter [73]. Tissue-specific D2 expression in the thyroid and heart is under the control of tissue-specific transcriptional factors TTF-1 (in thyroid cells) [74], Nkx-2.5, and GATA4 in cardiomyocytes [75]. Furthermore, NF-kB increases D2 expression, which highlights the involvement of deiodinases in pathological contexts [76]. Unlike D1 and D3, D2 mRNA expression thus not strictly correlates with protein synthesis due to a prominent posttranscriptional machinery that regulates D2 stability [77]. Proteasomal degradation tightly controls D2 protein degradation, thereby considerably shortening D2 half-life to only 120 min [67]. Extensive studies have revealed a specific degradation machinery constituted by ubiquitination-deubiquitination enzymes that govern this type of regulation of D2 stability [33, 67, 78,79,80]. A more recent study showed that D2 and D3 activity, and thereby thyroid hormone signaling, can be modulated by the Sonic hedgehog (Shh) protein [79], which is a highly potent proliferation promoting morphogen [81].
There is a close correlation between changes in the level of D3 mRNA and changes in D3 activity, which indicates that D3 is primarily modulated at transcriptional level. Various agents are able to regulate D3 expression both in vitro and in vivo. First, the different growth factors EGF, FGF, TPA, serum, and phorbol esters modulate D3 expression [1, 82]. Importantly, D3 has been demonstrated to be under the control of critical morphogens controlling development and tumorigenesis. The first such demonstration was the discovery by Huang et al. that TGF-β stimulates D3 transcription via a Smad2/4- or 3/4-dependent pathway [83]. Subsequently, the Shh and Wnt pathways were found to be critical mediators of D3 and TH action in BCC and colon cancer [33, 34].
Plasmatic Thyroid Hormone Metabolism
At the plasma level, the deiodinases represent an important homeostatic mechanism that acts as the first line of defense when thyroid function is impaired or when the supply of iodine is not sufficient to maintain plasma T3 (and T4) level constant. In this context, during hypothyroidism or iodine deficiency, the T3-producing enzyme D2 is upregulated, while the levels of the inactivating D3 are reduced.
Under normal conditions, D2 is the major producer of plasmatic T3, whereas D1 contributes a minimal amount. Kinetics studies indicate that the T3 generated by D1 (mostly in the liver and kidney) can rapidly exit the cell and equilibrate with plasma probably because of the subcellular plasmatic localization of the enzyme. Vice versa, T3 generated by D2 is located in the nucleus and perhaps, for this reason, remains within the cell for a longer time (approximately 8 h). D1–D2 induce a positive flow of T3 that exits the cells and enters the circulation, while D3 reduces the amount of thyroid hormones that, being intracellularly degraded, do not return to the circulation. Type 2 deiodinase is a highly processive enzyme, with a very short half-life (about 30 min). It is expressed in the skeletal muscle, pituitary, brain, BAT, and reproductive tract.
Given the diffuse D2 expression, it is likely that multiple tissues collectively contribute to the daily T3 production via the D2 pathway. A mouse strain with a targeted deletion (Dio2 knockout mouse) had no gross phenotypic abnormalities, and development and reproductive function appeared normal, except for mild growth retardation (9%). Serum T4 and TSH levels were both significantly elevated (40% and 100%, respectively), which suggests that the pituitary gland is resistant to the feedback effect of plasma T4. Human diseases due to mutations in the Dio2 gene have not been identified. However, three single nucleotide polymorphisms (SNPs) have been identified in the human population. The best characterized of these (Thr92Ala) at codon 92 (rs225014) is quite common in various ethnic groups. The D2-Ala mutant isoform results from a nonconservative A→G variation in position 274 of the DIO2 gene coding region [16] that determines the presence of an alanine in position 92 of the D2 protein, thus altering the first amino acid of an 18 amino acid loop critical for D2 recognition by its ubiquitinating complex [17]. The prevalence of the homozygous expression of D2-Ala in the general population ranges between 12.7 and 16.4% [15]. Although the threonine residue in position 92 is not phylogenetically conserved, D2-Ala mutants have been related to various clinical conditions all suggestive of impaired TH action, i.e., insulin resistance and type 2 diabetes mellitus, mental retardation and low IQ [18], and altered bone metabolism [19]. Although extensive data indicate that the action of D2-Ala is defective in a clinical setting, the few studies that have investigated its enzymatic activity reported conflicting results.
The serum active thyroid hormones (T3 and FT3) are quite stable in the circulation over time, apart from a nocturnal peak in TSH secretion, despite a relatively short half-life (approximately 12–18 h). The combined potent homeostatic control mediated by the hypothalamus-pituitary-thyroid axis and the deiodinases ensures that T3 levels remain stable in humans for days, weeks, or months. Notably, the deiodinases represent an efficient tool with which to preserve serum T3 levels during disease or adverse conditions given the inverse relationship between D2 and D3 observed during hypo-/hyperthyroidism. While D2 (the T3-producing enzyme) is negatively regulated by T3, the opposite applies to D3. This condition results in enhanced T3 production during hypothyroidism (and also during iodine deficiency) helped by a decreased TH clearance due to reduced D3 activity. The net effect is a synergic action mediated by deiodinase which help, together with the HPT axis, to maintain serum T3 levels within normal range.
Animal Models
Genetic mouse models of deiodinase deficiency have been instrumental in understanding the role of these enzymes in terms of developmental processes and of the complexes processes governing the systemic local control of TH action in adult tissues. However, paradigms of deiodinase actions have been challenged by the complex and somewhat unexpected phenotypes of D1, D2, and double D1–D2KO mice (reviewed by Galton et al. [84]). Surprisingly, both D1KO and D2KO but also double D1–D2KO mice have normal serum T3 levels and general health, growth, and reproductive capacity, thus challenging the generally accepted concept that the T4-to-T3 conversion induced by double D1–D2 deiodination is the major pathway to maintain normal T3 levels in the thyroid and extra-thyroidal districts. However, studies of D2KO mice reveal that peripheral control of the T4-to-T3 conversion is altered in genetic D2 depletion as demonstrated by abnormal TSH regulation [85], impaired adaptive thermogenesis [20], auditory dysfunction [86], and altered muscle regeneration [22]. D3KO mice had impaired fertility, significant perinatal mortality, and impaired growth [87]. The most prominent feature of this mouse model is a greatly altered thyroid status and physiology, which highlights the pivotal role of the D3 enzyme in this setting and in the maintenance of the HPT axis. Indeed, overexposure of the D3KO mouse to excessive levels of TH in utero and during the first weeks of perinatal life disrupts the HPT axis, with a subsequent hypothyroidism in the adult life. Strikingly, the HPT axis alterations in this mouse model resemble those observed in children born to mothers affected by hyperthyroidism during pregnancy [88].
All the complexities observed in the these animals might be explained by the alterations of the central control of thyroid hormones consequent to altered levels of deiodinases during the developmental period, which complicate the assessment of the functional roles of these enzymes in the adulthood. Consequently, investigations are now focusing on the use of conditional and tissue-specific knockout animals, which enable targeting of deiodinase expression to specific tissues at specific times. It is important to recall that the thyroid physiology of rodents differs considerably from that of humans, which partially explains the differences in phenotype between animal models and humans.
References
Gereben B, Zavacki AM, Ribich S, Kim BW, Huang SA, Simonides WS, Zeold A, Bianco AC. Cellular and molecular basis of deiodinase-regulated thyroid hormone signaling. Endocr Rev. 2008;29:898–938.
Crantz FR, Silva JE, Larsen PR. An analysis of the sources and quantity of 3,5,3′-triiodothyronine specifically bound to nuclear receptors in rat cerebral cortex and cerebellum. Endocrinology. 1982;110:367–75.
Bianco AC, Salvatore D, Gereben B, Berry MJ, Larsen PR. Biochemistry, cellular and molecular biology, and physiological roles of the iodothyronine selenodeiodinases. Endocr Rev. 2002;23:38–89.
St Germain DL, Galton VA. The deiodinase family of selenoproteins. Thyroid. 1997;7:655–68.
Oppenheimer JH, Schwartz HL, Surks MI. Propylthiouracil inhibits the conversion of L-thyroxine to L-triiodothyronine. An explanation of the antithyroxine effect of propylthiouracil and evidence supporting the concept that triiodothyronine is the active thyroid hormone. J Clin Invest. 1972;51:2493–7.
Leonard JL, Rosenberg IN. Thyroxine 5′-deiodinase activity of rat kidney: observations on activation by thiols and inhibition by propylthiouracil. Endocrinology. 1978;103:2137–44.
Maia AL, Berry MJ, Sabbag R, Harney JW, Larsen PR. Structural and functional differences in the dio1 gene in mice with inherited type 1 deiodinase deficiency. Mol Endocrinol. 1995;9:969–80.
Curcio-Morelli C, Gereben B, Zavacki AM, Kim BW, Huang S, Harney JW, Larsen PR, Bianco AC. In vivo dimerization of types 1, 2, and 3 iodothyronine selenodeiodinases. Endocrinology. 2003;144:937–46.
Visser TJ, van den Hout-Goemaat NL, Docter R, Hennemann G. Radio-immunoassay of thyroxine in unextracted serum. Neth J Med. 1975;18:111–5.
Chopra IJ. A study of extrathyroidal conversion of thyroxine (T4) to 3,3′,5-triiodothyronine (T3) in vitro. Endocrinology. 1977;101:453–63.
Kaplan MM, Utiger RD. Iodothyronine metabolism in rat liver homogenates. J Clin Invest. 1978;61:459–71.
O'Mara BA, Dittrich W, Lauterio TJ, St Germain DL. Pretranslational regulation of type I 5′-deiodinase by thyroid hormones and in fasted and diabetic rats. Endocrinology. 1993;133:1715–23.
Debaveye Y, Ellger B, Mebis L, Darras VM, Van den Berghe G. Regulation of tissue iodothyronine deiodinase activity in a model of prolonged critical illness. Thyroid. 2008;18:551–60.
Chopra IJ. Clinical review 86: Euthyroid sick syndrome: is it a misnomer? J Clin Endocrinol Metab. 1997;82:329–34.
Peeters RP, van der Geyten S, Wouters PJ, Darras VM, van Toor H, Kaptein E, Visser TJ, Van den Berghe G. Tissue thyroid hormone levels in critical illness. J Clin Endocrinol Metab. 2005;90:6498–507.
Schneider MJ, Fiering SN, Thai B, Wu SY, St Germain E, Parlow AF, St Germain DL, Galton VA. Targeted disruption of the type 1 selenodeiodinase gene (Dio1) results in marked changes in thyroid hormone economy in mice. Endocrinology. 2006;147:580–9.
Larsen PR, Silva JE, Kaplan MM. Relationships between circulating and intracellular thyroid hormones: physiological and clinical implications. Endocr Rev. 1981;2:87–102.
Buettner C, Harney JW, Larsen PR. The 3′-untranslated region of human type 2 iodothyronine deiodinase mRNA contains a functional selenocysteine insertion sequence element. J Biol Chem. 1998;273:33374–8.
Croteau W, Davey JC, Galton VA, St Germain DL. Cloning of the mammalian type II iodothyronine deiodinase. A selenoprotein differentially expressed and regulated in human and rat brain and other tissues. J Clin Invest. 1996;98:405–17.
de Jesus LA, Carvalho SD, Ribeiro MO, Schneider M, Kim SW, Harney JW, Larsen PR, Bianco AC. The type 2 iodothyronine deiodinase is essential for adaptive thermogenesis in brown adipose tissue. J Clin Invest. 2001;108:1379–85.
Salvatore D, Bartha T, Harney JW, Larsen PR. Molecular biological and biochemical characterization of the human type 2 selenodeiodinase. Endocrinology. 1996;137:3308–15.
Dentice M, Marsili A, Ambrosio R, Guardiola O, Sibilio A, Paik JH, Minchiotti G, DePinho RA, Fenzi G, Larsen PR, et al. The FoxO3/type 2 deiodinase pathway is required for normal mouse myogenesis and muscle regeneration. J Clin Invest. 2010;120:4021–30.
Salvatore D, Simonides WS, Dentice M, Zavacki AM, Larsen PR. Thyroid hormones and skeletal muscle--new insights and potential implications. Nat Rev Endocrinol. 2014;10:206–14.
Ramadan W, Marsili A, Larsen PR, Zavacki AM, Silva JE. Type-2 iodothyronine 5’deiodinase (D2) in skeletal muscle of C57Bl/6 mice. II. Evidence for a role of D2 in the hypermetabolism of thyroid hormone receptor alpha-deficient mice. Endocrinology. 2011;152:3093–102.
Marsili A, Ramadan W, Harney JW, Mulcahey M, Castroneves LA, Goemann IM, Wajner SM, Huang SA, Zavacki AM, Maia AL, et al. Type 2 iodothyronine deiodinase levels are higher in slow-twitch than fast-twitch mouse skeletal muscle and are increased in hypothyroidism. Endocrinology. 2010;151:5952–60.
Dentice M, Salvatore D. Deiodinases: the balance of thyroid hormone: local impact of thyroid hormone inactivation. J Endocrinol. 2011;209:273–82.
Salvatore D, Low SC, Berry M, Maia AL, Harney JW, Croteau W, St Germain DL, Larsen PR. Type 3 lodothyronine deiodinase: cloning, in vitro expression, and functional analysis of the placental selenoenzyme. J Clin Invest. 1995;96:2421–30.
Marsh-Armstrong N, Huang H, Remo BF, Liu TT, Brown DD. Asymmetric growth and development of the Xenopus laevis retina during metamorphosis is controlled by type III deiodinase. Neuron. 1999;24:871–8.
Kester MH, Toussaint MJ, Punt CA, Matondo R, Aarnio AM, Darras VM, Everts ME, de Bruin A, Visser TJ. Large induction of type III deiodinase expression after partial hepatectomy in the regenerating mouse and rat liver. Endocrinology. 2009;150:540–5.
Dentice M, Ambrosio R, Damiano V, Sibilio A, Luongo C, Guardiola O, Yennek S, Zordan P, Minchiotti G, Colao A, et al. Intracellular inactivation of thyroid hormone is a survival mechanism for muscle stem cell proliferation and lineage progression. Cell Metab. 2014;20:1038–48.
Li WW, Le Goascogne C, Ramauge M, Schumacher M, Pierre M, Courtin F. Induction of type 3 iodothyronine deiodinase by nerve injury in the rat peripheral nervous system. Endocrinology. 2001;142:5190–7.
Boelen A, Kwakkel J, Alkemade A, Renckens R, Kaptein E, Kuiper G, Wiersinga WM, Visser TJ. Induction of type 3 deiodinase activity in inflammatory cells of mice with chronic local inflammation. Endocrinology. 2005;146:5128–34.
Dentice M, Luongo C, Huang S, Ambrosio R, Elefante A, Mirebeau-Prunier D, Zavacki AM, Fenzi G, Grachtchouk M, Hutchin M, et al. Sonic hedgehog-induced type 3 deiodinase blocks thyroid hormone action enhancing proliferation of normal and malignant keratinocytes. Proc Natl Acad Sci U S A. 2007;104:14466–71.
Dentice M, Luongo C, Ambrosio R, Sibilio A, Casillo A, Iaccarino A, Troncone G, Fenzi G, Larsen PR, Salvatore D. beta-catenin regulates deiodinase levels and thyroid hormone signaling in colon cancer cells. Gastroenterology. 2012;143:1037–47.
Huang SA, Tu HM, Harney JW, Venihaki M, Butte AJ, Kozakewich HP, Fishman SJ, Larsen PR. Severe hypothyroidism caused by type 3 iodothyronine deiodinase in infantile hemangiomas. N Engl J Med. 2000;343:185–9.
Huang SA, Fish SA, Dorfman DM, Salvatore D, Kozakewich HP, Mandel SJ, Larsen PR. A 21-year-old woman with consumptive hypothyroidism due to a vascular tumor expressing type 3 iodothyronine deiodinase. J Clin Endocrinol Metab. 2002;87:4457–61.
Di Girolamo D, Ambrosio R, De Stefano MA, Mancino G, Porcelli T, Luongo C, Di Cicco E, Scalia G, Vecchio LD, Colao A, et al. Reciprocal interplay between thyroid hormone and microRNA-21 regulates hedgehog pathway-driven skin tumorigenesis. J Clin Invest. 2016;126:2308–20.
Simonides WS, Mulcahey MA, Redout EM, Muller A, Zuidwijk MJ, Visser TJ, Wassen FW, Crescenzi A, da-Silva WS, Harney J, et al. Hypoxia-inducible factor induces local thyroid hormone inactivation during hypoxic-ischemic disease in rats. J Clin Invest. 2008;118:975–83.
Wassen FW, Schiel AE, Kuiper GG, Kaptein E, Bakker O, Visser TJ, Simonides WS. Induction of thyroid hormone-degrading deiodinase in cardiac hypertrophy and failure. Endocrinology. 2002;143:2812–5.
Rajabi M, Kassiotis C, Razeghi P, Taegtmeyer H. Return to the fetal gene program protects the stressed heart: a strong hypothesis. Heart Fail Rev. 2007;12:331–43.
Siegel E, Sachs BA. In vitro leukocyte uptake of 131-I labeled iodide, thyroxine and triiodothyronine, and its relation to thyroid function. J Clin Endocrinol Metab. 1964;24:313–8.
Boelen A, Kwakkel J, Vos XG, Wiersinga WM, Fliers E. Differential effects of leptin and refeeding on the fasting-induced decrease of pituitary type 2 deiodinase and thyroid hormone receptor beta2 mRNA expression in mice. J Endocrinol. 2006;190:537–44.
Boelen A, Wiersinga WM, Fliers E. Fasting-induced changes in the hypothalamus-pituitary-thyroid axis. Thyroid. 2008;18:123–9.
Boelen A, Kwakkel J, Wieland CW, St Germain DL, Fliers E, Hernandez A. Impaired bacterial clearance in type 3 deiodinase-deficient mice infected with Streptococcus pneumoniae. Endocrinology. 2009;150:1984–90.
Peeters RP, Wouters PJ, Kaptein E, van Toor H, Visser TJ, Van den Berghe G. Reduced activation and increased inactivation of thyroid hormone in tissues of critically ill patients. J Clin Endocrinol Metab. 2003;88:3202–11.
Rodriguez-Perez A, Palos-Paz F, Kaptein E, Visser TJ, Dominguez-Gerpe L, Alvarez-Escudero J, Lado-Abeal J. Identification of molecular mechanisms related to nonthyroidal illness syndrome in skeletal muscle and adipose tissue from patients with septic shock. Clin Endocrinol. 2008;68:821–7.
Peeters RP, Wouters PJ, van Toor H, Kaptein E, Visser TJ, Van den Berghe G. Serum 3,3′,5′-triiodothyronine (rT3) and 3,5,3′-triiodothyronine/rT3 are prognostic markers in critically ill patients and are associated with postmortem tissue deiodinase activities. J Clin Endocrinol Metab. 2005;90:4559–65.
Fausto N. Liver regeneration. J Hepatol. 2000;32:19–31.
Tanimizu N, Miyajima A. Molecular mechanism of liver development and regeneration. Int Rev Cytol. 2007;259:1–48.
Hennemann G, Krenning EP, Polhuys M, Mol JA, Bernard BF, Visser TJ, Docter R. Carrier-mediated transport of thyroid hormone into rat hepatocytes is rate-limiting in total cellular uptake and metabolism. Endocrinology. 1986;119:1870–2.
Friesema EC, Ganguly S, Abdalla A, Manning Fox JE, Halestrap AP, Visser TJ. Identification of monocarboxylate transporter 8 as a specific thyroid hormone transporter. J Biol Chem. 2003;278:40128–35.
Visser WE, Friesema EC, Jansen J, Visser TJ. Thyroid hormone transport in and out of cells. Trends Endocrinol Metab. 2008;19:50–6.
Hennemann G, Docter R, Friesema EC, de Jong M, Krenning EP, Visser TJ. Plasma membrane transport of thyroid hormones and its role in thyroid hormone metabolism and bioavailability. Endocr Rev. 2001;22:451–76.
Friesema EC, Grueters A, Biebermann H, Krude H, von Moers A, Reeser M, Barrett TG, Mancilla EE, Svensson J, Kester MH, et al. Association between mutations in a thyroid hormone transporter and severe X-linked psychomotor retardation. Lancet. 2004;364:1435–7.
Dumitrescu AM, Liao XH, Best TB, Brockmann K, Refetoff S. A novel syndrome combining thyroid and neurological abnormalities is associated with mutations in a monocarboxylate transporter gene. Am J Hum Genet. 2004;74:168–75.
Visser WE, Visser TJ. Finding the way into the brain without MCT8. J Clin Endocrinol Metab. 2012;97:4362–5.
Friesema EC, Jansen J, Heuer H, Trajkovic M, Bauer K, Visser TJ. Mechanisms of disease: psychomotor retardation and high T3 levels caused by mutations in monocarboxylate transporter 8. Nat Clin Pract Endocrinol Metab. 2006;2:512–23.
Visser WE, Friesema EC, Visser TJ. Minireview: thyroid hormone transporters: the knowns and the unknowns. Mol Endocrinol. 2011;25:1–14.
Wirth EK, Roth S, Blechschmidt C, Holter SM, Becker L, Racz I, Zimmer A, Klopstock T, Gailus-Durner V, Fuchs H, et al. Neuronal 3′,3,5-triiodothyronine (T3) uptake and behavioral phenotype of mice deficient in Mct8, the neuronal T3 transporter mutated in Allan-Herndon-Dudley syndrome. J Neurosci. 2009;29:9439–49.
Trajkovic M, Visser TJ, Mittag J, Horn S, Lukas J, Darras VM, Raivich G, Bauer K, Heuer H. Abnormal thyroid hormone metabolism in mice lacking the monocarboxylate transporter 8. J Clin Invest. 2007;117:627–35.
Dumitrescu AM, Liao XH, Weiss RE, Millen K, Refetoff S. Tissue-specific thyroid hormone deprivation and excess in monocarboxylate transporter (mct) 8-deficient mice. Endocrinology. 2006;147:4036–43.
Mayerl S, Visser TJ, Darras VM, Horn S, Heuer H. Impact of Oatp1c1 deficiency on thyroid hormone metabolism and action in the mouse brain. Endocrinology. 2012;153:1528–37.
Heuer H, Maier MK, Iden S, Mittag J, Friesema EC, Visser TJ, Bauer K. The monocarboxylate transporter 8 linked to human psychomotor retardation is highly expressed in thyroid hormone-sensitive neuron populations. Endocrinology. 2005;146:1701–6.
Bernal J. Thyroid hormones and brain development. Vitam Horm. 2005;71:95–122.
Toyoda N, Zavacki AM, Maia AL, Harney JW, Larsen PR. A novel retinoid X receptor-independent thyroid hormone response element is present in the human type 1 deiodinase gene. Mol Cell Biol. 1995;15:5100–12.
Jakobs TC, Schmutzler C, Meissner J, Kohrle J. The promoter of the human type I 5′-deiodinase gene--mapping of the transcription start site and identification of a DR+4 thyroid-hormone-responsive element. Eur J Biochem. 1997;247:288–97.
Botero D, Gereben B, Goncalves C, De Jesus LA, Harney JW, Bianco AC. Ubc6p and ubc7p are required for normal and substrate-induced endoplasmic reticulum-associated degradation of the human selenoprotein type 2 iodothyronine monodeiodinase. Mol Endocrinol. 2002;16:1999–2007.
Esfandiari A, Gagelin C, Gavaret JM, Pavelka S, Lennon AM, Pierre M, Courtin F. Induction of type III-deiodinase activity in astroglial cells by retinoids. Glia. 1994;11:255–61.
Alcantara MR, Salvatori R, Alcantara PR, Nobrega LM, Campos VS, Oliveira EC, Oliveira MH, Souza AH, Aguiar-Oliveira MH. Thyroid morphology and function in adults with untreated isolated growth hormone deficiency. J Clin Endocrinol Metab. 2006;91:860–4.
Pekary AE, Berg L, Santini F, Chopra I, Hershman JM. Cytokines modulate type I iodothyronine deiodinase mRNA levels and enzyme activity in FRTL-5 rat thyroid cells. Mol Cell Endocrinol. 1994;101:R31–5.
Menjo M, Murata Y, Fujii T, Nimura Y, Seo H. Effects of thyroid and glucocorticoid hormones on the level of messenger ribonucleic acid for iodothyronine type I 5′-deiodinase in rat primary hepatocyte cultures grown as spheroids. Endocrinology. 1993;133:2984–90.
Van der Geyten S, Darras VM. Developmentally defined regulation of thyroid hormone metabolism by glucocorticoids in the rat. J Endocrinol. 2005;185:327–36.
Canettieri G, Franchi A, Sibilla R, Guzman E, Centanni M. Functional characterisation of the CRE/TATA box unit of type 2 deiodinase gene promoter in a human choriocarcinoma cell line. J Mol Endocrinol. 2004;33:51–8.
Gereben B, Salvatore D, Harney JW, Tu HM, Larsen PR. The human, but not rat, dio2 gene is stimulated by thyroid transcription factor-1 (TTF-1). Mol Endocrinol. 2001;15:112–24.
Dentice M, Morisco C, Vitale M, Rossi G, Fenzi G, Salvatore D. The different cardiac expression of the type 2 iodothyronine deiodinase gene between human and rat is related to the differential response of the Dio2 genes to Nkx-2.5 and GATA-4 transcription factors. Mol Endocrinol. 2003;17:1508–21.
Zeold A, Doleschall M, Haffner MC, Capelo LP, Menyhert J, Liposits Z, da Silva WS, Bianco AC, Kacskovics I, Fekete C, et al. Characterization of the nuclear factor-kappa B responsiveness of the human dio2 gene. Endocrinology. 2006;147:4419–29.
Gereben B, Goncalves C, Harney JW, Larsen PR, Bianco AC. Selective proteolysis of human type 2 deiodinase: a novel ubiquitin-proteasomal mediated mechanism for regulation of hormone activation. Mol Endocrinol. 2000;14:1697–708.
Dentice M, Luongo C, Elefante A, Ambrosio R, Salzano S, Zannini M, Nitsch R, Di Lauro R, Rossi G, Fenzi G, et al. Pendrin is a novel in vivo downstream target gene of the TTF-1/Nkx-2.1 homeodomain transcription factor in differentiated thyroid cells. Mol Cell Biol. 2005;25:10171–82.
Dentice M, Bandyopadhyay A, Gereben B, Callebaut I, Christoffolete MA, Kim BW, Nissim S, Mornon JP, Zavacki AM, Zeold A, et al. The hedgehog-inducible ubiquitin ligase subunit WSB-1 modulates thyroid hormone activation and PTHrP secretion in the developing growth plate. Nat Cell Biol. 2005;7:698–705.
Curcio-Morelli C, Zavacki AM, Christofollete M, Gereben B, de Freitas BC, Harney JW, Li Z, Wu G, Bianco AC. Deubiquitination of type 2 iodothyronine deiodinase by von Hippel-Lindau protein-interacting deubiquitinating enzymes regulates thyroid hormone activation. J Clin Invest. 2003;112:189–96.
Ingham PW, McMahon AP. Hedgehog signaling in animal development: paradigms and principles. Genes Dev. 2001;15:3059–87.
Gereben B, Zeold A, Dentice M, Salvatore D, Bianco AC. Activation and inactivation of thyroid hormone by deiodinases: local action with general consequences. Cell Mol Life Sci. 2008;65:570–90.
Huang SA, Mulcahey MA, Crescenzi A, Chung M, Kim BW, Barnes C, Kuijt W, Turano H, Harney J, Larsen PR. Transforming growth factor-beta promotes inactivation of extracellular thyroid hormones via transcriptional stimulation of type 3 iodothyronine deiodinase. Mol Endocrinol. 2005;19:3126–36.
Galton VA, Schneider MJ, Clark AS, St Germain DL. Life without thyroxine to 3,5,3′-triiodothyronine conversion: studies in mice devoid of the 5′-deiodinases. Endocrinology. 2009;150:2957–63.
Schneider MJ, Fiering SN, Pallud SE, Parlow AF, St Germain DL, Galton VA. Targeted disruption of the type 2 selenodeiodinase gene (DIO2) results in a phenotype of pituitary resistance to T4. Mol Endocrinol. 2001;15:2137–48.
Ng L, Goodyear RJ, Woods CA, Schneider MJ, Diamond E, Richardson GP, Kelley MW, Germain DL, Galton VA, Forrest D. Hearing loss and retarded cochlear development in mice lacking type 2 iodothyronine deiodinase. Proc Natl Acad Sci U S A. 2004;101:3474–9.
Hernandez A, Martinez ME, Fiering S, Galton VA, St Germain D. Type 3 deiodinase is critical for the maturation and function of the thyroid axis. J Clin Invest. 2006;116:476–84.
Dussault JH, Coulombe P, Walker P. Effects of neonatal hyperthyroidism on the development of the hypothalamic-pituitary-thyroid axis in the rat. Endocrinology. 1982;110:1037–42.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2019 Springer International Publishing AG, part of Springer Nature
About this chapter

Cite this chapter
Dentice, M., Salvatore, D. (2019). Deiodination and Peripheral Metabolism of Thyroid Hormone. In: Luster, M., Duntas, L., Wartofsky, L. (eds) The Thyroid and Its Diseases. Springer, Cham. https://doi.org/10.1007/978-3-319-72102-6_5
Download citation
DOI: https://doi.org/10.1007/978-3-319-72102-6_5
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-72100-2
Online ISBN: 978-3-319-72102-6
eBook Packages: MedicineMedicine (R0)