
Abstract
Caries in permanent teeth is still the most prevalent disease worldwide. However, there are numerous reports about a caries decline with respect to caries prevalence and caries experience (DMFT or dmft scores). The most pronounced caries decline has been noticed in 12-year-old children in industrialized countries. These reports might obstruct the view on the epidemiological caries development in the primary dentition, which is not as successful as in the permanent dentition. Regarding the age groups of 3-year-old or even younger children, there are only limited data. These data show considerable differences in caries prevalence, but consistently a caries decline, even of widely varying magnitude. In 5- to 7-year-old children there is indeed an obvious trend for a caries decline over the last decades. However, this decline is only weak since around the year 2000, and in some countries there are indications for a halt or even a reversal of the caries decline in the primary dentition in this age group. The data for 12-year-old children demonstrate a distinct caries decline, which has continued through all last decades and reached DMFT values of 0.5 or less in some countries. However, parallel to the caries decline, there is an increasingly stronger caries polarization. Analytical caries epidemiology provides strong indications for an enhancement of the caries decline by placing fissure sealants. This effect seems to be particularly important in children with low SES background who benefit from this caries preventive measure to higher extents than other children.
Access provided by CONRICYT-eBooks. Download chapter PDF
Similar content being viewed by others

Keywords
- Caries epidemiology
- Caries prevalence
- Caries experience
- DMFT
- Caries decline
- Caries polarization
- Socioeconomic status
- Fissure sealants
1.1 Introduction
Dental caries is frequently cited as an oral disease with both declining prevalence and average experience. However, taking the whole distribution and severity of caries worldwide into consideration, it turns out that caries in permanent teeth is still the most prevalent condition worldwide, affecting 2.4 billion people, and that untreated caries in deciduous teeth is the tenth most prevalent condition [1]. Globally, the prevalence of untreated caries over all age groups seems to have been static between 1990 and 2010. However, there are considerable variations between regions and countries, and the manifestation of cavitating caries seems to shift from childhood to adulthood [1].
Caries prevalence and caries experience are key figures of oral health in children and other age groups. While the caries prevalence is defined as the percentage of persons in the respective cohort which shows any finding of caries (untreated or treated by restorations or extractions), the caries experience reflects the mean number of such caries affected teeth in a cohort.
Caries experience is expressed as DMFT index which is the average sum of caries affected teeth. The respective teeth exhibit unrestored caries (D = “decayed”) and restored dentin caries (F = “filled”) or are extracted due to caries (M = “missing”). The teeth are added per individual, the average sum gives the DMFT in a cohort, age cohort or population.
When presenting and discussing trends in caries epidemiology, some general features and limitations regarding the published figures have to be recollected. Most epidemiological data regarding caries are derived from clinical investigations under field conditions, and x-ray findings are not included [2]. In addition, caries scoring is most often restricted to lesions with the involvement of dentin [3]. Limiting the notated caries to such defects overlooks earlier caries stages like initial lesions or those confined to the enamel. Although modern understanding of caries starts at the first noticeable levels of the disease and although the restriction of epidemiological caries scoring has been considered inappropriate [4], the majority of all caries epidemiological studies worldwide still follow this WHO recommended matter. As a consequence, caries will be underscored to an unknown degree. However, as this approach has been followed since decades, it makes the respective studies comparable. Thus, also trend lines can be concluded from these studies with sufficient validity.
The most comprehensive international collection of data on caries prevalence and experience exists for 12-year-olds. This age group is chosen for caries epidemiological surveys as recommended by WHO [3]. Other age groups which are frequently considered in caries epidemiological reports are 3-year-old (2 to 4 years) and 6-year-old (5 to 7 years) children (Country/Area Profile Project 2017 [5]).
In general, both the caries prevalence and the caries experience show a distinct decline in children in many industrialized countries during the last decades. In a number of countries, this caries decline has been demonstrated on the basis of nationally representative surveys. However, it has to be recognized that the successful story of caries decline regards mainly the permanent dentition but not, at least not to the same magnitude, the primary dentition.
Modern caries epidemiology is not only primarily observational and descriptive but also attempts to explain the observed trends by reporting associations with caries relevant variables (analytical epidemiology [2]). Such parameters can be caries etiological factors, preventive measures, behavior, attitudes, and more. For example, caries burden can be related to the presence of fissure sealants. Based on analytical epidemiological approaches, the main reason for the caries decline is judged to be the widespread availability of fluoride. In addition, the increasing application rates of fissure sealants are a further cause for the reduced caries burden in children in some countries.
In the following pages, descriptions of the trends in caries prevalence and experience in different age cohorts in a range of industrialized countries will be given. The main data sources are publications of the Country/Area Profile Project [5] and the OECD [6]. The data selection is based on the availability of nationwide surveys if possible. However, in some countries local surveys have been conducted which are commonly cited as national reports. Furthermore, it should be taken into account that the exact age groups which have been examined differ between some countries. For these reasons the trend lines are not to be used for comparisons between countries. However, as in the included countries epidemiological field studies have been conducted repeatedly, robust conclusions about trends in caries prevalence, experience, and distribution can be drawn.
1.2 3-Year-Old Children
There is common agreement that the prevalence and extent of caries later in life are based on caries in the very early years of childhood, and many dental health problems are caused by inappropriate oral health behavior or life conditions during this time. However, there are only limited data regarding the age groups of 3-year-old or even younger children. The respective reports give mainly data about the prevalence of caries-affected children.
Table 1.1 summarizes data about the caries prevalence in 3-year-old children from countries with repeated surveys. Obviously, the caries prevalence in this age group differs considerably between the different countries. However, in each of these countries, there is a decline in caries prevalence in this age group, even though with widely varying magnitude. In Germany, regional examinations have revealed caries prevalences between 10 and 15% in 3-year-old children from 2000 to 2010 [7]. Hitherto unpublished data from the German city Hamburg show a distinct decline from 32.2 to 15.8% in the period between 1977 and 2006 (Schiffner, unpublished). A considerable decline is also reported from Sweden, with a caries prevalence of 4% in 2011 [5]. Trends in Australia, Poland, and the USA are also declining, but to a less marked degree [5].
1.3 6-Year-Old Children (Primary Dentition)
Data about caries prevalence and experience in the primary dentition of 6-year-old children are available in greater numbers of reports. While the official WHO reference age group are 5-year-old children [3], the majority of countries reports about 6- or 7-year-old children. This is due to the fact that in many countries school starts with 6 years and thus makes it easier to conduct surveys from this age on.
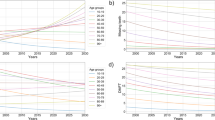
Figure 1.1a, b reflects the trends in caries experience (dmft or dft) in 5- to 7-year-old children in different countries worldwide (Data source: [5, 8]). Again it should be mentioned that these figures are constructed to exhibit trends, not to compare different countries, as the age groups, the nationwide representativeness, and the caries index (dmft or dft) are different.


There is an obvious trend for a caries decline in 5- to 7-year-old children (Fig. 1.1a). However, going closer into detail with respect to the years since 2000, it has to be conceded that there is only a weak decline (Fig. 1.1b). In addition, there are indications for a halt or even a reversal of the caries decline in the primary dentition in some countries in this age group.
1.4 12-Year-Old Children (Permanent Dentition)
There is a huge number of reports about oral health and caries in 12-year-old children, who are an important WHO reference age group [3]. Caries prevalence and experience have been reported for this age group since decades. The country selection for this age group used in this review follows the sample of the 6-year-olds. The data demonstrate a distinct caries decline. However, it should be mentioned that in a comprehensive worldwide perspective, the decline is not convincing, at least not since 2000. Calculation of a global DMFT in 12-year-old children in fact shows a decline from 2.4 in 1980 to 1.9 in 2015, but regarding the years 2001 and 2004, even lower global DMFT values of 1.7 and 1.6, respectively, have been presented [9]. The inconsistent epidemiological development of the caries burden is due to increasing caries scores in some parts of the world, while in industrialized countries a decline predominates.
The declining trend of caries experience (DMFT) in 12-year-olds is illustrated in Fig. 1.2a, b, which are based on different data sources [5, 6, 8, 10]. Again, these illustrations cannot be used for comparisons between countries, but to carve out a trend. There is a strong caries decline over the observation period (Fig. 1.2a). The statement of a caries decline is also valid when going into detail and focusing on the development since approximately the year 2000 (Fig. 1.2b): Even in those countries who had reached low DMFT values of about 1.0 around 2000, a further decline can be observed since then.

As an example for the strong caries decline in 12-year-old children in industrialized countries, the figures from Germany can be used. In Germany, nationwide representative oral health studies have repeatedly been conducted since 1989, using the method of cross-sectional studies. The surveys conducted in the years 1997 and 2005 and the recent study from 2014 (“Fifth German Oral Health Study”) have used the same examination criteria [11]. Due to this maximization of methodological consistency, a range of validated comparisons is permitted.
In 2014, the teeth of 81.3% of the 12-year-old children in Germany were found to be free of dentine caries experience (DMFT = 0). In comparison to the preceding surveys, showing caries prevalence rates of 41.8% in 1997 and 70.1% in 2005, this means a massive improvement in oral health. Caries experience in 2014 as expressed by the DMFT value averaged 0.5 in this cohort of children which is one of the lowest figures for caries experience hitherto reported worldwide [5]. Caries experience has decreased considerably as compared with the former surveys from 1997 (mean DMFT = 1.7) and 2005 (mean DMFT = 0.7).
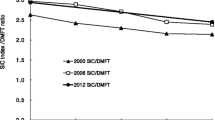
Regarding many industrialized countries, the strong caries decline in the permanent dentition of 12-year-olds is particularly striking when being compared with the epidemiological trend in the primary dentition of 5- to 7-year-olds. In the majority of all countries which have published reports about both age groups, the decline in the elder age group’s permanent dentition is much more pronounced than that in the primary dentition. As an example, Fig. 1.3 illustrates the different degrees of caries decline in German school children [12]. This difference is remarkable as the examination in both age groups was performed according to the same study protocol by the same investigators. Obviously caries preventive measures show their effect in 12-year-old children to a high extent, while the more or less same measures are of less pronounced effectiveness in the primary dentition of younger children.

Comparison of the trends in caries experience in 6- to 7-year-old children (primary dentition) and in 12-year-old children (permanent dentition) according to school-based samples in Germany [12]
1.5 Caries Polarization
The statement of the declining caries burden in children does not apply for all children. Parallel to the average decline, the phenomenon of the caries polarization becomes more and more apparent. Caries polarization means that not all individuals participate in the gain of oral health, but that a small group is not involved in this positive development and exhibits many more carious teeth than the majority of the age group [2]. The caries distribution and thus the polarization follow the socioeconomic status (SES) of the children and their families in many countries, with members of the lower social classes experiencing more caries and exhibiting more extracted teeth [2, 13,14,15]. Even if also children from families with low SES can exhibit improvements of their oral conditions (as shown, e.g., in 12-year-olds in Germany), the caries experience is still higher in these children and often shows higher portions of untreated caries. In the cited German study, children with high SES have a DMFT as low as 0.3, while children with low social background average out at a DMFT of 0.7 [11].
The parallel trend of a caries decline and a stronger polarization is exemplified by the representative German surveys (Table 1.2). Not only the caries prevalence and experience in 12-year-old children have declined but also the risk group which was constantly defined as all children with DMFT >2. As the percentage of these children has fallen from 21.5 to 6.1%, but as these children in all surveys account for nearly two thirds of all DMF teeth of the entire sample, this means a distinct sharpening of caries polarization.
1.6 Association Between Caries Decline and Fissure Sealing
Some comprehensive epidemiological studies also report about the prevalence and mean number of fissure sealants and relate these figures in an approach of analytical epidemiology to caries experience.
Regarding the German Oral Health Studies, one explanation of the significant decline in caries seems to be the increased use of fissure sealing. In 2014, a total of 70.3% of the children had at least one fissure-sealed tooth—an increase of 17.4% points over 1997, when 52.9% of the children had at least one sealed fissure (Table 1.2 [11]). In the 12-year-old children exhibiting fissure sealants, the mean number of sealed teeth has risen from 3.6 to 4.0 during this time period. The presence of fissure sealants turns out to be strongly related to caries experience in the 2014 survey: Children with at least one sealed fissure have an average DMFT score of just 0.3, while children without any sealant exhibit a DMFT value of 0.9 [11]. In comparison with the earlier study from 2005, the difference in caries experience between children with and without at least one sealed fissure has clearly increased, as the caries decline is particularly strong in children with sealed teeth (Fig. 1.4).

Caries experience (DMFT) in 12-year-old German children related to the presence of at least one fissure sealed tooth in 2005 and 2014 [11]
In the context of the social background of the German 12-year-old children, it is remarkable that children with low SES background have less frequent sealants than middle- or upper-class children (64.6 vs. 72.1% vs. 74.7%) and that the mean number of sealed teeth in children with any sealant also differs in relation to SES (3.7 vs. 4.0 vs. 4.3) [11]. However, the caries experience reducing effect of sealing fissures is clearly detectable also in children with low SES: In the representative German survey, the lower-class children with at least one fissure sealant exhibit a DMFT of 0.3, equaling the value of the whole sample and giving evidence for the importance of the sealing measure. In the publication of the Fifth German Oral Health Studies, it is concluded that the greatest oral health gain by sealing fissures is realized in children with low SES and that this measure is able to reduce the commonly noticed differences in caries burden between children with different SES [11].
The same importance of placing dental sealants has recently been estimated for children in the USA [16]. Comparing data for 6- to 11-year-old children from the National Health and Nutrition Examination Survey (NHANES) 2011–2014 with 1999–2004 NHANES data, the authors find an increase in sealant use prevalence by 16.2% points to 38.7% among children from low-income families. However, this is still less than in high-income children. In this study, low-income children without sealants had almost three times more cavities in permanent first molars compared with children with sealants (0.82 decayed or filled first molars vs. 0.29). The authors estimate that providing sealants to all low-income children would prevent 3.4 million cavities in the USA over 4 years [16].
References
Kassebaum NJ, Bernabé E, Dahiya M, Bhandari B, Murray CJL, Marcenes W. Global burden of untreated caries. J Dent Res. 2015;94:650–8.
Schiffner U. Epidemiology of caries and noncarious defects. In: Meyer-Lückel H, Paris S, Ekstrand K, editors. Caries management – science and clinical practice. Stuttgart: Thieme; 2013. p. 118–32.
World Health Organization. Oral health surveys: basic methods. Geneva: World Health Organization; 2013.
Pitts NB. Diagnostic tools and measurements – impact on appropriate care. Community Dent Health. 1992;10:1–9.
Country/Area Profile Project (CAPP). Country oral health profiles. https://www.mah.se/CAPP/Country-Oral-Health-Profiles/. Accessed 24 April 2017.
Organisation for Economic Co-operation and Development (OECD) Health Status: Dental health. 2016. https://stats.oecd.org/index.aspx?DataSetCode=HEALTH_STAT. Accessed 2 May 2017.
Treuner A, Splieth C. Frühkindliche Karies – Fakten und Prävention. Zahnarztl Mitt. 2013;103(17):44–50. http://www.zm-online.de/hefte/Fruehkindliche-Karies-Fakten-und-Praevention_139858.html#1. Accessed 27 April 2017.
Ha DH, Roberts-Thomson KF, Arrow P, Peres KG, Do LG. Children’s oral health status in Australia, 2012–14. In: Do LG, Spencer AJ, editors. Oral health of Australian children: The National Child Oral Health Study 2012–14. Adelaide: University of Adelaide Press; 2016. p. 86–152. www.adelaide.edu.au/press. Accessed 2 May 2017.
Malmö University Global DMFT for 12-year-olds: 2015. 2015. https://www.mah.se/CAPP/Country-Oral-Health-Profiles/According-to-Alphabetical/Global-DMFT-for-12-year-olds-2011/. Accessed 2 May 2017.
Australian Institute of Health and Welfare. Oral health and dental care in Australia - Key facts and figures 2015. Canberra, Cat. no. DEN 229. 2016. http://www.aihw.gov.au/WorkArea/DownloadAsset.aspx?id=60129554609. Accessed 28 April 2017.
Schiffner U. Krankheits- und Versorgungsprävalenzen bei Kindern (12-Jährige): Karies, Erosionen, Molaren-Inzisiven-Hypomineralisationen. In: Jordan AR, Micheelis W, editors. Fünfte Deutsche Mundgesundheits-Studie (DMS V). Cologne: Deutscher Ärzte-Verlag; 2016. p. 231–68.
Pieper K. Epidemiologische Begleituntersuchungen zur Gruppenprophylaxe 2009. DAJ [Deutsche Arbeitsgemeinschaft für Jugendzahnpflege], Bonn; 2010.
Truin GJ, König KG, Bronkhorst EM, Frankenmolen F, Mulder J, van’t Hof MA. Time trends in caries experience of 6- and 12-year-old children of different socioeconomic status in The Hague. Caries Res. 1998;32:1–4.
Burt BA, Eklund SA. Dentistry, dental practice and the community. 6th ed. St. Louis: Elsevier Saunders; 2005.
Schwendicke F, Dörfer CE, Schlattmann P, Foster Page L, Thomson WM, Paris S. Socioeconomic inequality and caries: a systematic review and meta-analysis. J Dent Res. 2015;94:10–8.
Griffin SO, Wei L, Gooch BF, Weno K, Espinoza L. Vital signs: dental sealant use and untreated tooth decay among U.S. school-aged children. MMWR Morb Mortal Wkly Rep. 2016;65:1141–5.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2018 Springer International Publishing Switzerland
About this chapter

Cite this chapter
Schiffner, U. (2018). Trends in Caries Epidemiology in Children. In: Bekes, K. (eds) Pit and Fissure Sealants. Springer, Cham. https://doi.org/10.1007/978-3-319-71979-5_1
Download citation
DOI: https://doi.org/10.1007/978-3-319-71979-5_1
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-71978-8
Online ISBN: 978-3-319-71979-5
eBook Packages: MedicineMedicine (R0)