
Abstract
The heterogeneity of salivary gland disease presents unique challenges for the pathologist, radiologist, and treating clinician in their pursuit of optimal patient care. Clinical history, physical exam, and information provided by imaging studies such as ultrasound, contrast-enhanced computed tomography, or magnetic resonance imaging with contrast, as well as fine-needle aspiration (FNA) contribute to the development of a management plan that can range from observation to limited or extensive surgical resection and possible adjuvant therapy. FNA has an established role in salivary gland diagnostics because it is able to provide valuable information regarding the nature of the salivary gland lesion. It is also quick, well tolerated with very few complications, and lends itself to rapid onsite evaluation when used in conjunction with clinical assessment and imaging studies. The clinical utility to surgical specialists of The Milan System for Reporting Salivary Gland Cytopathology can be summarized in clarity of communication, correlation and stratification of risk of malignancy, and definition of a management algorithm.
Access provided by CONRICYT-eBooks. Download chapter PDF
Similar content being viewed by others


Keywords
General Background
The heterogeneity of salivary gland disease presents unique challenges for the pathologist, radiologist, and treating clinician in their pursuit of optimal patient care. Clinical history, physical exam, and information provided by imaging studies such as ultrasound, contrast-enhanced computed tomography (CT) Fig. 9.1 [1], or magnetic resonance imaging (MRI) with contrast as well as fine-needle aspiration (FNA) all contribute to the development of a management plan that can range from observation to limited or extensive surgical resection and possible adjuvant therapy [2,3,4,5,6]. FNA has a well-established role in salivary gland diagnostics. Cytomorphology is able to provide valuable information regarding the nature of the salivary gland lesion . FNA is quick, and well tolerated with very few complications. It also lends itself to rapid on-site evaluation (ROSE) when used in conjunction with clinical assessment and imaging studies, and can significantly improve triage of the patient for definitive therapy [3].

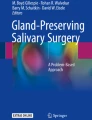
Axial CT with intravenous contrast of a superficial left parotid gland tumor . The mass measures 1.2 cm, has sharp margins, and shows slight enhancement. Fine needle aspiration of the mass showed a pleomorphic adenoma (From Faquin and Powers [1], with permission)
An understanding of the diagnostic challenges that cytopathologists face when assessing a salivary FNA can be extrapolated from the World Health Organization (WHO ) classification of salivary neoplasms, which has over 40 different entities based on histological features [7]. Because of significant morphologic overlap of some entities, it is unavoidable that at times only a morphological description of the FNA will be provided to the treating clinician without a specific diagnosis [2]. This mandates that a clear line of communication exists between cytopathologist and the treating clinician to ensure that the patient receives the correct management. It is in this context that a uniform reporting system for salivary gland cytology is most beneficial. The clinical utility of The Milan System for Reporting Salivary Gland Cytopathology to surgical specialists can be summarized as follows:
-
Standardizes reporting and clarity of communication
-
Correlates and stratifies the cytologic diagnosis with a risk of malignancy (ROM)
-
Facilitates the use of a management algorithm
-
Is relevant, transferable, and practical for institutions with variable experience and expertise in salivary gland cytology
-
Facilitates quality assurance review and clinical audits by setting standards (e.g., the proportion of inadequate samples less than 10%) as well as providing a potential outcome measure for further research
Clinical Management Considerations: Overview for the Parotid and Submandibular Glands
There are several key questions that the clinician should address when developing a clinical management strategy for salivary gland lesions :
-
Do I need any additional information, clarification, or staging radiologic scans prior to formulating a definitive treatment plan?
For masses involving the parotid gland, nearly all patients should have cross-sectional imaging performed preoperatively (CT or MRI with contrast). This is done to determine the extent of the lesion (superficial and/or deep lobe involvement) and the probability of complete resection of the primary tumor with facial nerve preservation in cases where this is possible. In a few patients with small (1 cm or less), well-defined lesions that are lateral in the parotid gland and with a benign cytologic diagnosis (i.e., “Neoplasm: Benign”), cross-sectional imaging may not be necessary. Patients with clinical scenarios that indicate the possibility of nerve involvement by tumor should undergo specific assessment for cranial nerve involvement (using MRI and/or CT). Patients with malignant disease should also have imaging that assesses the regional lymph node groups (CT or MRI with contrast), and the most likely sites of distant metastasis should be studied (CT of chest with contrast or skull base to mid-thigh positron emission tomography [PET]/CT).
-
Does this case need to be discussed in a multidisciplinary setting with early involvement of the medical or radiation oncologist for treatment planning?
In both small and large institutions , the use of a multidisciplinary discussion should be considered for any salivary gland lesion that is not unequivocally benign.
-
Does the lesion need to be surgically removed or can it be safely monitored clinically?
In certain scenarios, asymptomatic benign lesions with a low risk of malignant transformation, such as a Warthin tumor or a deep lobe pleomorphic adenoma in an elderly patient, may be managed by clinical observation. This can include selected cases when the patient wishes to avoid the possible risk of facial nerve injury.
-
If I am considering monitoring the lesion , do I need any further investigations to be sure that this is a safe option?
Some lesions may require serial imaging or repeat FNA . This will vary, depending on the individual patient scenario. Tumors in locations not easily assessed on physical exam could be imaged serially until a “growth rate” is determined, at which time the interval between studies may be lengthened. Tumors with indeterminate cytology (e.g., “Salivary Gland Neoplasm of Uncertain Malignant Potential [SUMP ]”) that appear to be benign based on their clinical presentation could undergo repeat FNA after a period of observation. Lastly, benign or indeterminate tumors under observation that show a change in their clinical status, such as rapid growth after a period of stability or the onset of new symptoms such as pain or facial nerve weakness, should undergo repeat FNA to help further define the evolving tumor.
-
When surgical intervention is indicated, what is the minimal necessary procedure needed to adequately manage the tumor?
The presurgical evaluation should address the possibility of postoperative facial nerve dysfunction and contour defect that may be required to completely remove the tumor and leave the patient with the smallest possible risk of recurrence. In the case of parotid malignancies, the procedure may span the spectrum from superficial parotidectomy to subtotal or total parotidectomy. In all cases, the facial nerve is preserved unless it is impossible to separate it from the tumor without leaving gross disease behind. In cases of malignancy, when considering nerve sacrifice, a balance must be reached between the morbidity of resection and the possibility of eventual therapeutic failure and patient mortality if gross disease is left behind to be controlled with adjuvant radiation or chemoradiation.
-
Do I need to consent the patient for an increased risk of nerve injury or sacrifice and the donor site morbidity of a nerve graft?
This topic is the centerpiece of the process of informed consent . For patients with large but clearly benign tumors, the low risk of permanent and significant nerve injury should be discussed. In any patient with the possibility of malignancy, the potential of nerve sacrifice, graft harvest, nerve defect reconstruction and nerve transfer should be discussed with the patient. The possibility of eyelid procedures as well as static procedures to maintain midface tone should also be discussed.
-
Is a neck dissection indicated?
Patients with clinical evidence of cervical lymph node involvement will undergo therapeutic neck dissection in nearly all cases. Patients without known neck disease may undergo elective neck dissection, depending upon either the preoperative FNA evaluation, or the findings of intraoperative frozen section, or both. The authors accept that the use of frozen section is highly variable internationally and needs to be interpreted by an expert pathologist; however, it may facilitate the management decision. The best time to perform a neck dissection is at the time of primary site surgery. Alternatively, the decision of how to manage the neck and the treatment modality (neck dissection versus radiation) may be made after formal histological assessment of the primary lesion. Patients who do not have a diagnosis of malignancy prior to surgery, due either to an inaccessible site of lesion for FNA or an equivocal cytological diagnosis, may have the decision made to proceed with neck dissection based upon the intraoperative frozen section diagnosis rendered on the primary parotid lesion. Patients with low-grade malignancies such as low-grade mucoepidermoid carcinoma can be followed clinically without neck dissection if the clinical and radiological evaluations both indicate that the neck is free of metastatic disease. Patients with higher grade pathology (e.g., salivary duct carcinoma or high-grade mucoepidermoid carcinoma) are candidates for elective selective neck dissection.
-
Will I require the use of intraoperative frozen section to address prior indeterminate cytology such as “Atypia of Undetermined Significance (AUS) ,” “Neoplasm: SUMP,” “Suspicious for Malignancy,” or “Non-Diagnostic” FNA ?
In some institutions intraoperative frozen section is used as an important adjunct to the preoperative cytological diagnosis . This involves sending a partial parotidectomy specimen containing the entire tumor to an expert pathologist. It is important not to breach the capsule by performing an incisional biopsy, as this risks tumor spillage and the associated increased risk of recurrence. When used, frozen section has a role in the assessment of the completeness of surgical resection margins and clearance of nerve margins in cases with nerve invasion. Frozen section can be helpful in clarifying what may have been an equivocal cytological diagnosis by defining the histologic classification, tumor grade, and extent of invasion. Clinicians are cautioned that frozen sections have their own sets of artifacts and limitations to consider. The impact on decision making on neck management is addressed in the prior section.
Management Options by Milan System Diagnostic Category
Non-Diagnostic
Management
-
Repeat FNA . If the first FNA was by palpation, then consider ultrasound guidance (USG).
-
If the second FNA is also Non-Diagnostic despite USG and adequate sample preparation, consider alternative investigations. First, perform cross-sectional imaging with contrast enhanced CT or MRI if not already obtained. Second, if the MRI or CT or clinical picture shows features concerning for malignancy or if there is still doubt as to the nature of the lesion, consider USG core needle biopsy (CNB), open biopsy (both controversial due to the inherent risk of tumor spillage), or formal surgical excision.
-
If the sample is “cyst contents only,” completely aspirate the cyst contents under USG. If a solid component remains, it should be resampled. If the lesion disappears completely, then repeat US +/− FNA in 3–4 months . The FNA would be repeated in cases where US shows a recurrent lesion.
Non-Neoplastic
The majority of “Non-Neoplastic” lesions are managed non-surgically.
Management
-
Lesions that are clearly non-neoplastic on FNA may be followed with either serial physical examinations, cross-sectional imaging, or a combination of both to assure stability. Any change in either the clinical exam or imaging could warrant repeat sampling to confirm no change in cytological status.
-
USG for the FNA is important for non-neoplastic cases to help avoid sampling errors, which are not uncommon in this diagnostic category. If the FNA findings do not provide sufficient diagnostic information to explain clinical and radiologic findings, repeat FNA; the possible use of CNB, open biopsy, or surgical resection could be considered.
-
MRI or CT is useful to assess the lesion serially and to assess regional lymph nodes.
Atypia of Undetermined Significance (AUS)
Management
-
Repeat FNA. If the first FNA was performed by palpation, then consider USG FNA.
-
Regular clinical follow-up with duration interval to be determined based upon clinical suspicion; every 3–6 months is a general rule of thumb.
-
Cross-sectional imaging with contrast enhanced MRI or CT.
-
CNB, open biopsy, or surgical resection should be considered for this lesion when the clinical presentation is concerning for malignancy. Examples would be a painful mass that lacks signs of inflammation, a concurrent facial nerve weakness or paralysis, or a prior history of cutaneous malignancy.
Neoplasm
-
Benign
-
Salivary Gland Neoplasm of Uncertain Malignant Potential (SUMP)
Management (General)
-
Complete resection of the tumor with a narrow cuff of normal tissue as a margin (this can be as narrow as 1–2 cell layers thick). For tumors with an unequivocal preoperative FNA diagnosis of “Benign,” no frozen section is necessary.
-
Given the increased risk of a low-grade malignancy in the SUMP category, surgical resection is indicated. Intraoperative frozen section can be used for more definitive histologic classification and to help inform any decisions pertaining to possible neck dissection. For SUMP parotid lesions, the type of parotidectomy will depend upon the size and location of the tumor. However, a nerve dissecting parotidectomy with nerve preservation is the most oncologically safe option.
-
For SUMP lesions involving the submandibular glands (SMG), excision should be performed removing the entire gland in a suprafascial plane. Frozen section can be performed to determine malignancy and to assist in the decision to perform a selective neck dissection for intermediate and high-grade malignancies. Because SMGs have a higher proportion of malignant neoplasms, one should consider placing the skin incision low enough to facilitate a neck dissection if needed.
Benign Neoplasm Management Summary
Parotid gland lesions :
-
Cross-sectional imaging (MRI or CT) in nearly all cases to determine extent of the lesion, reserving only very small lesions with clearly palpable borders to be managed without preoperative imaging.
-
Complete excision of the lesion with either extracapsular dissection or nerve dissecting parotidectomy with nerve preservation. Lesions in the superficial or lateral lobe would undergo superficial parotidectomy; those in the deep lobe would require resection of the deep lobe lesion often with preservation of the superficial portion of the gland. Sparing the superficial portion of the gland helps to minimize the postoperative contour defect.
-
A subset of patients who are medically inoperable or who are unable to accept the risk of nerve injury might be clinically followed without surgical management.
SMG lesions
-
Cross-sectional imaging (MRI or CT) with SMG surgical resection in suprafascial plane.
SUMP Management Summary
Parotid gland lesions :
-
Cross-sectional imaging (MRI or CT) to assess neck preoperatively and nerve-preserving parotidectomy.
-
Nerve sparing surgical resection unless clinically not indicated (such as a medically inoperable patient).
-
Consider performing frozen section to better define the histologic classification and determine if neck dissection is indicated.
SMG lesions :
-
Cross-sectional imaging (MRI or CT) preoperatively with SMG resection in suprafascial plane.
-
Ensure that neck incision is low enough to facilitate neck dissection.
-
Consider frozen section to better define the histologic classification and determine if neck dissection is indicated in the primary setting.
Suspicious for Malignancy
Management (General)
-
Salivary gland lesions in this diagnostic category have a high ROM and mandate cross-sectional imaging for the purposes of assessing the extent of the lesion and staging prior to surgical resection. Chest imaging should be performed to rule out metastatic disease.
-
It is important to assess the need for elective neck dissection at the time of primary surgical resection versus adjuvant radiotherapy to address the primary site and upper cervical lymph nodes. Not all malignant tumors require an elective neck dissection. Based upon the classic works of Frankenthaler et al. [4] and Armstrong et al. [2] the indications for elective neck dissection are: tumor >4 cm; high-grade histology; extraglandular extension, and neurological deficit.
-
Frozen section of the primary salivary gland tumor with a preoperative cytology “Suspicious for Malignancy” can be used to help inform the decision to perform an elective neck dissection for cases that are clinically and radiologically negative.
-
A therapeutic neck dissection of levels II–IV should be planned for cases with clinical or radiographic evidence of neck disease preoperatively or when the preoperative cytology is “Suspicious for Malignancy.” Intraoperative frozen section of the primary salivary gland tumor can be used to confirm that neck dissection is necessary in this setting.
-
The extent of neck dissection is largely determined by the location and stage of neck disease. Dissection of levels II-IV is almost always required.
Suspicious for Malignancy Management Summary
-
Preoperative staging contrast-enhanced MRI or CT of the neck and imaging of the chest
-
Parotid gland lesions :
-
Nerve-preserving parotidectomy with complete excision of the lesion.
-
Consent patient for the increased risk of nerve dysfunction and possibility that nerve cannot be separated from tumor. The surgeon may choose to use intraoperative frozen section to confirm malignancy before sacrificing the facial nerve.
-
Consent patient that nerve may need to be sacrificed in exceptional circumstances and reanimation procedures performed.
-
If imaging suggests a malignant process, nerve sparing parotidectomy with complete tumor excision should be performed. Some institutions use frozen section evaluation. If the frozen section is positive for malignancy and pathological nodes are identified, then concurrent comprehensive neck dissection is performed, sparing nonlymphatic structures (internal jugular vein, sternocleidomastoid muscle, spinal accessory nerve) if possible. For tumors >4 cm in greatest dimension, high-grade features on frozen section of the primary site, extraglandular extension on imaging or noted intraoperatively, or preoperative facial weakness, perform elective selective neck dissection for the clinically and radiographically N0 neck.
-
-
For institutions that do not routinely use frozen section, the decision to manage the neck is made once formal histological assessment of the primary site has been performed. In cases of malignancy, the decision to offer radiation therapy or further surgery (i.e., neck dissection) is made by an informed patient in a multidisciplinary setting. If indicated, neck dissection is performed as a second procedure.
-
SMG lesions
-
If clinical and contrast enhanced MRI or CT features appear benign without possible nodal disease, consider removal of the gland in a suprafascial plane with a low neck incision to facilitate neck dissection. Frozen section should be performed. If findings are consistent with an intermediate or high-grade malignancy, selective neck dissection may be performed.
-
If contrast enhanced MRI or CT indicates a malignant process, the frozen section shows primary submandibular gland malignancy, and pathological nodes are present, perform selective neck dissection.
-
Malignant
In the clinical management of clearly “Malignant” salivary gland lesions , a definitive classification of a specific malignant histologic tumor type, including grade (low- versus high-grade), provides important information for clinical decision making. When a definitive classification is not possible, information about tumor grade is still useful. Low- versus intermediate- versus high-grade classification may be useful to the clinician in determining the extent of surgery required at the primary site and the likelihood that a neck dissection would be needed. For high-grade malignancies involving the deep lobe, a total parotidectomy is necessary. For lateral lesions, controversy exists regarding the extent of surgery with some surgeons electing to perform a total parotidectomy to optimize surgical clearance and others performing a superficial parotidectomy with the knowledge that the patient will be receiving postoperative radiotherapy. In addition, a subcategory of “metastatic” would also be informative for the managing clinician. Parotid gland lymph nodes are a common site for metastases from cutaneous primaries, and these patients often require a concurrent neck dissection. If a lesion is metastatic from a non-cutaneous source , PET-CT may be indicated to locate a primary site of origin.
Management Summary
-
Presurgical staging MRI or CT neck plus CT neck and chest
-
Parotid gland lesions:
-
For low-grade with no clinical or radiographic evidence of involved neck nodes and no other indicators for neck dissection (as mentioned above), perform nerve sparing parotidectomy with complete tumor excision.
-
For intermediate- or high-grade and negative for involved neck nodes, perform nerve-preserving total parotidectomy and elective selective neck dissection.
-
For intermediate- or high-grade and evidence of involved neck nodes, perform nerve-preserving total parotidectomy and selective neck dissection.
-
Consent patient for the increased risk of nerve dysfunction and possibility that nerve cannot be separated from tumor. The surgeon may choose to use intraoperative frozen section to confirm malignancy before sacrificing the facial nerve.
-
Consent patient that nerve may need to be sacrificed and reanimation procedures performed.
-
-
SMG lesions
-
For low-grade with no clinical or radiographic neck nodes and no other indicators for neck dissection present, perform suprafascial SMG resection.
-
For intermediate- or high-grade tumors, perform suprafascial SMG, and if no clinical or radiographic evidence of involved neck lymph nodes, perform elective neck dissection.
-
For intermediate- or high-grade histology, perform suprafascial SMG resection and if neck shows clinical or radiographic evidence of involved neck lymph nodes, perform selective neck dissection.
-
-
Metastatic
-
Known primary site—management based on primary tumor
-
For cutaneous squamous cell carcinoma, consider nerve-preserving parotidectomy and selective neck dissection if clinically N0.
-
-
Unknown primary site—consider PET-CT to identify the primary site. If identified, management would be based upon specific aspects of the primary cancer. If no primary site is identified and the salivary gland lesion is isolated, it can be managed as a high-grade primary lesion in order to avoid issues related to uncontrolled head and neck malignancy. In such a setting, avoiding facial nerve injury is a priority.
-
Table 9.1 lists the main indications for clinical observation versus operative management; Table 9.2, the indications for neck dissection and the extent of dissection; Table 9.3, the degrees of parotidectomy required; Table 9.4, management of the facial nerve.
References
Faquin WC, Powers CN. Salivary gland cytopathology. In: Rosenthal DL, editor. Essentials in cytopathology, vol. 5. New York: Springer Science + Business Media; 2008.
Armstrong JG, Harrison LB, Thaler HT, Friedlander-Klar H, Fass DE, Zelefsky MJ, et al. The indications for elective treatment of the neck in cancer of the major salivary glands. Cancer. 1992;69(3):615–9.
Bajwa MS, Rose SJ, Mairembam P, Nash R, Hotchen D, Godden D, et al. Feasibility of a novel classification for parotid gland cytology: a retrospective review of 512 cytology reports taken from 4 United Kingdom general hospitals. Head Neck. 2016;38(11):1596–603.
Frankenthaler RA, Byers RM, Luna MA, Callender DL, Wolf P, Goepfert H. Predicting occult lymph node metastasis in parotid cancer. Arch Otolaryngol Head Neck Surg. 1993;119(5):517–20.
Griffith CC, Pai RK, Schneider F, Duvvuri U, Ferris RL, Johnson JT, et al. Salivary gland tumor fine-needle aspiration cytology: a proposal for a risk stratification classification. Am J Clin Pathol. 2015;143(6):839–53.
McGurk M, Thomas BL, Renehan AG. Extracapsular dissection for clinically benign parotid lumps: reduced morbidity without oncological compromise. Br J Cancer. 2003;89(9):1610–3.
WHO classification of head and neck tumours. WHO/IARC classification of tumours, vol. 9. 4th ed. Lyon: World Health Organization/International Agency for Reserch on Cancer; 2017.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2018 Springer International Publishing AG
About this chapter

Cite this chapter
Bajwa, M.S., Nicolai, P., Varvares, M.A. (2018). Clinical Management. In: Faquin, W., et al. The Milan System for Reporting Salivary Gland Cytopathology . Springer, Cham. https://doi.org/10.1007/978-3-319-71285-7_9
Download citation
DOI: https://doi.org/10.1007/978-3-319-71285-7_9
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-71284-0
Online ISBN: 978-3-319-71285-7
eBook Packages: MedicineMedicine (R0)