
Abstract
This chapter reviews the pharmacology of the intravenously administered opioids in the practice of geriatric anesthesiology. These drugs include morphine, meperidine, hydromorphone, fentanyl, sufentanil, and methadone. It is important that anesthesiologists understand the differences in pharmacology of opioids in elderly patients, in order to choose the appropriate drug and titrate precisely to achieve the desired analgesic effects while minimizing the risks of opioid toxicity. The key points for this chapter are as follows: (1) Elderly patients need about half the dose as younger patients, (2) The primary reason is pharmacodynamics (the elderly brain is more sensitive to opioids), (3) The pharmacokinetic changes with age are modest, (4) Studies in elderly animals show reduced numbers of μ receptors with increased age. That does not explain the reduction in dose, as decreased receptor density should decrease sensitivity to opioids. The enhancement in drug effect seen in the clinic is more likely attributable to changes in cyclonucleotide coupling and other downstream changes that occur in aging, and (5) Mepiridine should be used with caution in elderly patients due to its effects on myocardium, pharmacokinetics related to its metabolites, and its delirogenic properties.
Access provided by CONRICYT-eBooks. Download chapter PDF
Similar content being viewed by others


Keywords
- Aging
- Continuous infusion
- Effect site
- Fentayl
- Geriatric anesthesia and analgesia
- Hydromorphone
- Intravenous anesthesia
- Intravenous analgesia
- Meperidine
- Methadone
- Morphine
- Patient controlled analgesia (PCA)
- Postoperative analgesia
- Sufentanil
General Observations
Opioids are among the most effective and the most dangerous of the drugs administered by anesthesiologists. With the growing epidemic of opioid abuse and overdose in the general population, it is important to review the specific consideration for prescribing them in the elderly population. In the United States, between 1993 and 2012, opioid overuse has more than doubled with the elderly population showing some of the largest rates of increase. The World Health Organization proposed a three-step analgesic ladder for the treatment of chronic pain. They recommended starting with acetaminophen and nonsteroidal analgesics, progressing to opioids of intermediate strength, such as codeine, and treating severe pain with strong opioids such as morphine [1]. The Agency for Health Care Policy and Research (now called the Agency for Healthcare Research and Quality) has issued similar guidelines [2]. Particular care must be taken when using opioids in elderly patients. It is nearly tautological that elderly patients are more likely to suffer from chronic diseases than their younger counterparts. Some fortunate individuals remain physically vigorous until very late in life, whereas others seem to deteriorate physically at younger ages. Additionally, the cumulative effects of smoking, alcohol, and environmental toxins can accelerate the deterioration of aging in exposed individuals. Thus, it is not surprising that variability in physiology increases throughout life [3] (see Chap. 1). Increased physiologic variability results in increased pharmacokinetic and pharmacodynamic variability in elderly subjects. The clinical result of this increased variability is an increased incidence of adverse drug reactions in elderly patients [4]. Thus, elderly patients require more careful titration and, where possible and appropriate, therapeutic drug monitoring [5].
The Opioid Receptor
The existence o f an opioid receptor was long suspected because of the high potency and stereoselectivity of pharmacologic antagonists. The biochemical discovery of opioid receptors was independently reported in 1973, by laboratories of Pert [6], Simon [7], and Terenius [8]. The finding of stereoselectivity led to an intense search for endogenous ligands, with identification of encephalin in 1975 [9]. Other endogenous peptide ligands were isolated subsequently [10, 11]. The fact that endogenous opioid ligands differed in their structure and binding sites suggested the existence of different opioid receptor types [12]. Three classes of opioid receptors were identified pharmacologically in the 1980s: μ (mu) [13], δ (delta) [14], and [15] κ (kappa).
Activation of the μ receptor is responsible for both the analgesic efficacy of the frequently used opioids and, unfortunately, for the majority of opioid toxicities. Shortly after characterization of the μ receptor, Pasternak and colleagues [16] demonstrated that there were two populations of opioid receptors: a high-affinity site, associated with analgesia and blocked by naloxazone, and a lower-affinity site, which was not blocked by naloxazone and seemed responsible for morphine lethality. It was subsequently demonstrated that morphine-induced analgesia was mediated by a population of receptors blocked by naloxonazine, which were termed μ1 receptors, whereas morphine-induced ventilatory depression was blocked by a population of receptors that were not affected by naloxonazine, which were termed the μ2 receptors [17, 18]. To further complicate matters, a selective morphine-6-glucuronide antagonist was identified, 3-O-methylnaxtrexone, which had little effect on morphine analgesia [19]. This suggested that there was variability within the μ1 receptor itself. Although identification of a specific μ1 antagonist led to the hope that a μ1-specific agonist could be developed, no such agonist has ever been identified.
Additional evidence for μ receptor subtypes comes from the clinical observation of incomplete cross-tolerance among the opioids in patients [20], so that if a patient is switched from an opioid to which the patient has become tolerant to an “equianalgesic” dosage of another opioid, the potential exists for serious overdose [21]. Additional evidence for multiple μ receptor subtypes comes from variance in the potency for analgesic efficacy and toxicity among patients, such that there is no single opioid that has the best therapeutic window for all patients [21]. An extreme example of differential response to opioids is found in the CXBK mouse, which is insensitive to morphine but has normal sensitivity to fentanyl and morphine-6-glucuronide [22].
The μ opioid subtypes have unique distributions within the body [23]. Specifically, μ1 is expressed in the brain, whereas μ2 is expressed in the brain, gastrointestinal tract, and the respiratory tract [24]. Activation of both μ receptor subtypes acts to decrease calcium and potassium conductance and intracellular adenosine 3′,5′-cyclic monophosphate (cAMP). The recently discovered μ3 receptor is expressed on monocytes, granulocytes, and the vascular endothelium, where it acts to release nitric oxide [25]. Some of the vasodilatation that is associated with opioid administration that has been attributed to histamine release may be attributable to the activation of the μ3 receptor.
The μ receptor is encoded by a single gene Oprm, located on chromosome 10 in the mouse [26, 27] and on chromosome 6 in the human [28]. A variety of polymorphisms of Oprm have been identified in humans, as recently reviewed by Lötsch and Geisslinger [28]. The polymorphism that has generated the most interest has been the substitution of an aspartate for an asparagine in the 118 position, which is abbreviated as the 118A > G SNP. This polymorphism has been associated with a decreased analgesic response to morphine. However, it does not reduce sensitivity to opioid-induced ventilatory depression [29].
The Oprm gene gives rise to a family of μ receptors through selective splicing of the mRNA into μ opioid receptor subtypes [30]. In 1993, the first μ receptor was cloned, MOR-1 [31, 32]. Since then, at least 15 different splice variants of MOR-1 have been identified in mice, all derived from the same Oprm gene [24]. Several splice variants have been identified in humans as well [33]. Splice variants likely give rise to pharmacologically identified subtypes of μ receptors based on the exons that are translated. Unfortunately, mapping between individual splice variants and pharmacologically identified μ subtypes is incomplete. The currently identified splice variants are insufficient to explain the pharmacologic groupings, although this would likely become clearer as additional splice variants are discovered and characterized pharmacologically.
All opioid receptors so far identified are coupled to Gi proteins [34]. At the cellular level, the opioid receptors have an inhibitory effect. When the receptors are occupied by opioid agonists, intracellular cAMP content is reduced. Reduced levels of cAMP both increase the activation of K+ channels and reduce the probability of voltage-gated calcium channels being open. These changes cause hyperpolarization of the membrane potential and thus reduce neuronal excitability [35].
The last 15 years have seen a resurgence of interest in the molecular basis of opioid signaling, driven by the discovery that opioids couple with β-arrestin-2 as well as with Gi proteins. [36] It appears that analgesia is mediated by the Gi pathway, while tolerance, addiction, constipation, and respiratory depression are mediated by the β-arrestin-2 pathway. [37] This discovery led to the search “biased ligands,” opioids that preferentially signal through the Gi pathway, providing analgesia, with reduced signaling through the β-arrestin-2 pathway, mitigating toxicity [38]. Several opioid agonists with minimal activation of the β-arrestin-2 pathway are in active drug development [39, 40]. Initial clinical studies with oliceridine suggest that it has efficacy similar to morphine in a surgical pain model. [41]If these novel “biased” opioids are eventually approved for clinical use, their enhanced safety may render the opioids discussed in this chapter obsolete.
Aging and Opioid Receptors
End-organ sensitivity to various ligands changes with age. Part of this change is from differences at the level of the drug receptor–effector mechanism. For example, Ueno and colleagues [42] examined opioid receptors in young, mature, and aged mice. Aged mice had reduced μ receptor density but increased μ receptor affinity. Hess et al. [43] also observed decreased μ receptor density in rats with advancing age, associated with decreased sensitivity to pain. Similarly, Petkov and colleagues [44] observed decreased enkephalin receptors in aged rats, as well as decreased sensitivity to enkephalin. Aging may induce changes downstream of opioid receptor binding. In studies on opioid receptors in polymorphonuclear leukocytes, Fulop and colleagues [45] have shown that whereas cAMP was reduced on binding in cells from young adult animals, it was increased in cells from aged animals. Hoskins and Ho [46] have shown age-induced changes in the basal activities of adenylate cyclase, guanylate cyclase, cAMP phosphodiesterase, and cyclic guanosine monophosphate phosphodiesterase.
Smith and Gray [47] examined the analgesic response to opioids in young and aged rats. They applied noxious stimulus at two different stimulus intensities. At the low-intensity stimulus (immersing the tail in 50 °C water), there was a trend toward increased sensitivity to opioids in the aged rats, but the difference was not significant. However, when subjected to high-intensity stimulus (immersing the tail in 55 °C water), the aged rats were about twice as sensitive to opioids as the young rats, an effect that was significant.
Other investigators have reached quite different conclusions using similar experimental paradigms (tail flick after immersion in hot water). Van Crugten and colleagues [48] looked at morphine antinociception in aged rats and found no difference in antinociception between aged and adult animals. Hoskins and colleagues [49] found that aged mice were about half as sensitive to morphine as mature adult mice.
In summary, the overall evidence in animal models shows decreased numbers of opioid receptors in aged brains. However, the story about the antinociceptive response to morphine is less clear in animal models, with studies showing increased sensitivity , decreased sensitivity, or no change in sensitivity with advancing age.
Aging and Pain Perception
Pain is a part of daily life for many elderly patients, with about 50% of elderly patients in a community setting having chronic pain with the prevalence being higher among elderly patients in long-term care facilities [50]. Elderly patients are particularly more prone to chronic pain than younger people [51, 52]. However, clinically it seems that pain in elderly subjects is indistinguishable from the experience of pain in younger subjects [53].
There are some interesting differences between young and older subjects in their response to experimental pain. There is some evidence that older patients are more sensitive to experimental pain [54], which may be explained by a reduction in the endogenous analgesic response to pain [55, 56], possibly mediated by reduced production of β-endorphin in response to noxious stimulation [57]. Older patients experience a more prolonged hyperalgesia after capsaicin injection compared with younger subjects [58]. Additionally, older patients seem to also require a higher intensity of noxious stimulation before first reporting pain [56].
Some of the differences between studies may also depend on exactly which pain pathways are activated during the assessment. Chakour and colleagues [59] demonstrated that pain transmission via C fibers was unchanged in young versus elderly subjects. However, there was a substantial reduction in pain transmission via Aδ fibers. Thus, the relative perceptions of pain in elderly subjects versus younger subjects were influenced by the extent of pain transmission via Aδ fibers.
Aging and Risk of Opioid-Related Side Effects
While pain is a common occurrence in the lives of the elderly population, and certainly is of concern in the perioperative period, care must be taken in providing analgesia with opioids because of the alterations in the risk of respiratory depression . In their secondary analysis of a retrospective cohort study, Cepeda and colleagues [60] noted that the risk of opioid-induced ventilatory depression increased with increasing age, with patients 61–70 years of age having 2.8 times the risk of ventilatory depression compared with patients 16–45 years old. Interestingly, in their analysis, they converted all of the opioids into morphine equivalents, and the conversion did not account for the increased potency of opioids in the elderly that will be described subsequently.
Although the risk of respiratory depression from opioids is greater in older people, the same is not true for all opioid side effects. Opioids are among the major causes of postoperative nausea and vomiting , increasing the risk nearly fourfold [59]. In the study by Cepeda et al., age was not a risk factor for nausea and vomiting [60]. In fact, age may actually decrease the risk of nausea and vomiting. Sinclair and colleagues [61] observed a 13% decrease in the risk of postoperative nausea and vomiting with each additional decade of life. This finding is consistent with the findings of Junger and colleagues [62].
The Onset and Offset of Opioid Drug Effect
Onset
The onset of opioid drug effect is determined by the route of delivery, the delivered dose, the pharmacokinetics of the opioid that determine the plasma concentrations over time, and the rate of blood–brain equilibration between the plasma and the site of drug effect. Table 18.1 shows adult pharmacokinetics of fentanyl [63], alfentanil [63], sufentanil [64], remifentanil [65], morphine [66], methadone [67],Footnote 1 meperidine [68],Footnote 2 and hydromorphone [69]. Table 18.1 also shows k e0, the rate constant for blood–effect-site equilibration, fentanyl [63], alfentanil [63], sufentanil [70], remifentanil [65], morphine [66], methadone [71], meperidine [70],Footnote 3 and hydromorphone [72].Footnote 4 Based on these data, it is possible to predict the time course of concentration change in the plasma following an intravenous bolus, as seen in Fig. 18.1. The upper graph in Fig. 18.1 shows the concentration during 24 h following a bolus injection, whereas the lower graph just shows the first 30 min. In both cases, the curves have been normalized to start at 100%, which permits direct comparison of the pharmacokinetics despite differing potencies. As seen in the upper graph, the extremes of plasma elimination are remifentanil, which is ultra fast, and methadone, which has the longest half-life. Alfentanil has the second-shortest half-life among the eight opioids. Fentanyl, meperidine, sufentanil, hydromorphone, and morphine are all clustered in the middle. In particular, note how similar hydromorphone and morphine are when one examines the plasma pharmacokinetics. Approximately the same trend is observed in the first 30 min, although the initial distribution phase of hydromorphone takes it nearly as low as remifentanil in the first 10 min. As will be seen shortly, this is significant in terms of recovery.

The time course of plasma concentration following a bolus of fentanyl, alfentanil, sufentanil, remifentanil, morphine, methadone, meperidine, and hydromorphone, based on the pharmacokinetics shown in Table 18.1. The y-axis is the percent of the initial concentration, which by definition is 100% at time 0, permitting display of the relative time courses of these opioids independent of the dose administered
The plasma is not the site of drug effect, and thus the time course of concentration seen in Fig. 18.1 will not reflect the time course of effect-site concentration or behavioral activity. By incorporating the plasma–effect-site equilibration delay into our calculations, we can examine the time course of the onset of drug effect , as shown in Fig. 18.2. In this case, we have normalized the effect-site concentrations to peak effect concentration [73] to again permit comparisons of the time course of drugs independent of the differences in potency. Alfentanil and remifentanil both reach a peak about 1.5 min after bolus injection, although the overall remifentanil drug effect is more evanescent. The peak fentanyl concentration occurs about 3.5 min after bolus injection, whereas the peak sufentanil effect is about 6 min after bolus injection. Methadone and meperidine are nearly indistinguishable following bolus injection, each reaching a peak about 12 min after a bolus. The peak for hydromorphone is 15–20 min after the bolus. Morphine is the outlier in terms of onset. Five minutes after a bolus injection, morphine is at 50% of the peak concentration. However, morphine reaches its peak concentration in the effect site about 90 min after the bolus injection. Table 18.1 shows the time to reach peak concentration for each of the opioids, as well as the volume of distribution at the time of peak effect, which is useful for calculating initial loading doses [74,75,76].

The time course of effect-site concentration following a bolus of fentanyl, alfentanil, sufentanil, remifentanil, morphine, methadone, meperidine, and hydromorphone, based on the pharmacokinetics and rate of plasma–effect-site equilibrium shown in Table 18.1. The curves have been normalized to the peak effect-site concentration, permitting comparison of the relative rate of increase independent of dose. The times to peak effect correspond to those shown in Table 18.1
One clinical applications of the time course of drug effect following bolus injection is to guide programming of the lockout of PCA devices. A 10-min lockout for hydromorphone and methadone is a logical choice, because patients are able to make a decision to redose themselves after reaching peak drug effect. The slower onset of morphine is somewhat problematic, because patients will administer another dose while the prior dose is still reaching peak effect, creating the possibility of stacking bolus doses.
Considerable attention is given to “equianalgesic dosing” of opioids. The calculation of the equianalgesic dose is complicated by the relative intrinsic potency of the opioids, the different pharmacokinetic profiles, and the large differences in the rate of blood–brain equilibration. Table 18.2 shows equianalgesic doses of frequently used opioids, based on the “minimum effective analgesic concentrations” or “MEAC” (also called “MEC”) of fentanyl [77], alfentanil [78], sufentanil,Footnote 5 remifentanil,Footnote 6 morphine [80],Footnote 7 methadone [81], meperidine [82], and hydromorphone [72, 83].Footnote 8 Reflecting anesthesiologists’ familiarity with fentanyl, all of the calculations have been made using fentanyl as the reference opioid. The calculation of an equianalgesic bolus dose depends on when the observation of drug effect is made. For example, because fentanyl has a very rapid onset, and morphine has a very slow onset, 5 mg of morphine has the same effect at 10 min as 50 μg of fentanyl, whereas 60 min after the dose, 1 mg of morphine has the same effect as 50 μg of fentanyl. Similarly, because the drugs accumulate during infusions at different rates, the relative potencies of the opioids change depending on how long the infusion has been running, as shown in Table 18.2.
Figure 18.3 shows the increase in effect-site concentration during a continuous infusion for each of these opioids. As expected, remifentanil increases the fastest, whereas methadone increases the slowest. Note, however, that even after 10 h of drug administration, most of these opioids are only at 60–80% of the eventual steady-state concentration. This speaks to the problem of background infusions for PCA. Even after many hours, patients are not at steady state, and the increasing drug concentration from the background infusion may expose a patient to toxicity 12–24 h after initiation of the infusion. Given the increased sensitivity of elderly patients to the effects of opioids, background infusions are likely a particularly poor choice in this population.

The increase to steady state during an infusion of fentanyl, alfentanil, sufentanil, remifentanil, morphine, methadone, meperidine, and hydromorphone, based on the pharmacokinetics and rate of plasma–effect-site equilibrium shown in Table 18.1. The curves have been normalized to the steady-state effect-site concentration, permitting comparison of the relative rate of increase independent of infusion rate. Only remifentanil and alfentanil are at steady state after 10 h of continuous infusion
Offset
The offset of drug effect is a function of both the pharmacokinetic behavior and the rate of blood–brain equilibration. The “context-sensitive half-time” [73, 84] is a useful way to consider the plasma pharmacokinetic portion of the offset time, as shown in Fig. 18.4. The x-axis on Fig. 18.4 is the duration of an infusion that maintains a steady concentration of drug in the plasma. The y-axis is the time required for the concentrations to decrease by 50% after the infusion is terminated. Remifentanil’s pharmacokinetics are so fast that the context-sensitive half-time blurs right into the x-axis. Perhaps surprisingly, fentanyl is the outlier here. Fentanyl accumulates in fat, and so an infusion that maintains a steady concentration in the plasma winds up giving patients a large dose of fentanyl, resulting in slow recovery. Meperidine similarly shows long recovery. Note that for infusions of less than 10 h, morphine, hydromorphone, and sufentanil are nearly indistinguishable based on the plasma pharmacokinetics.

The “context-sensitive half-time” (50% plasma decrement time) for fentanyl, alfentanil, sufentanil, remifentanil, morphine, methadone, meperidine, and hydromorphone, based on the pharmacokinetics shown in Table 18.1. Remifentanil shows virtually no accumulation over time with continuous infusion s, whereas the offset of fentanyl changes considerably as it is administered to maintain a steady plasma concentration
Once again, we have to consider that the plasma is not the site of drug effect. Therefore, we must consider the 50% effect-site decrement time [73, 85], as shown in Fig. 18.5. Because fentanyl and remifentanil have very rapid plasma–effect-site equilibration, they have changed little between Figs. 18.4 and 18.6. Note , however, the huge change for morphine and hydromorphone. One might have thought from Fig. 18.4 that these drugs would result in rapid offset of drug effect following a continuous infusion . This is clearly not the case, because the blood–brain equilibration delay results in these drugs having far slower offset than alfentanil or sufentanil. The “surprise” here is methadone. One would rarely think of methadone as a reasonable choice for infusion during anesthesia, but the pharmacokinetics of methadone suggest that it might be a reasonable choice for anesthetics of 4 h or less.

The 50% effect-site decrement curves for fentanyl, alfentanil, sufentanil, remifentanil, morphine, methadone, meperidine, and hydromorphone, based on the pharmacokinetics and rate of plasma–effect-site equilibrium shown in Table 18.1. For drugs with rapid plasma–effect-site equilibrium, the 50% effect-site decrement curve closely follows the context sensitive half-time curve. However, for drugs with slow plasma–effect-site equilibration, a 50% decrement in effect-site concentration is considerably slower than a 50% decrement in plasma concentration (e.g., morphine)

The 20% effect-site decrement curves for fentanyl, alfentanil, sufentanil, remifentanil, morphine, methadone, meperidine, and hydromorphone, based on the pharmacokinetics and rate of plasma–effect-site equilibrium shown in Table 18.1. The effect-site levels of all opioids, except morphine, will decrease by 20% quickly when an infusion is terminated. The slower decrease for morphine is because of its slow plasma–effect-site equilibration
Figure 18.6 shows the 20% effect-site decrement curve for these eight opioids. Figure 18.6 speaks to how often one might expect to redose a patient with chronic pain who is titrating the analgesic level to a just-adequate concentration. Because of its slow blood–brain equilibration, morphine would need to be given approximately every 2 h. Hydromorphone, fentanyl, and methadone would need to be given approximately every hour.
Specific Opioids
Morphin e
Morphine has three unique aspects among the opioids frequently used in anesthesia practice: it is an endogenous ligand of the μ receptor, has an active metabolite, and has a very slow onset of effect. Morphine was initially identified in the brains of mice that had never been exposed to exogenous morphine [86]. It has subsequently been found in the brains of cows [87], rats [88], and humans [89]. Codeine has also been identified as an endogenously synthesized substance. However, because codeine is mostly an inactive prodrug of morphine, its presence in the brain does not diminish morphine’s distinction as the only endogenous ligand of the μ receptor that is also a frequently administered drug.
Morphine is metabolized by glucuronidation into two metabolites, morphine-3-glucuronide, which is mostly inactive, and morphine-6-glucuronide, which is itself a potent analgesic [90]. Although the potency of intrathecal morphine-6-glucuronide is 650-fold higher than that of morphine [91], morphine-6-glucuronide crosses the blood–brain barrier very slowly, so slowly that it is unlikely that it contributes to the acute analgesia provided by morphine [92, 93]. However, with chronic administration, the levels of morphine-6-glucuronide will increase to pharmacologically active concentrations [94].
Morphine-6-glucuronide is eliminated by the kidneys [95]. Creatinine clearance is reduced with advancing age, as shown in the often-cited equation of Cockroft and Gault [96]:
This reduction means that the creatinine clearance of an 80-year-old patient will be about half that of a 20-year-old patient. Thus, morphine-6-glucuronide will accumulate more in elderly patients, necessitating a reduction in the dose of chronically administered morphine. Of course, if the patient has renal insufficiency, it might be better to select an opioid without an active metabolite.
The second unique aspect of morphine is the slow onset of effect. The peak effect following a bolus dose of morphine occurs approximately 90 min after the bolus. This has been demonstrated using pupillometry [97,98,99], ventilatory depression [98], and analgesia [99] as measures of morphine drug effect. The likely explanation for this is that morphine is a substrate for P-glycoprotein, which actively transports morphine out of the central nervous system [100].
Figure 18.7 shows a simulation of the analgesic (y-axis > 1) and ventilatory (y-axis < 1) effects of three different morphine doses: a bolus of 0.2 mg/kg, a bolus of 0.2 mg/kg followed by an infusion of 1 mg/70 kg per hour, and repeated boluses of 0.1 mg/kg every 6 h [101]. The solid line is the median prediction, whereas the shaded area represents the 95% confidence bounds. As seen in Fig. 18.7, the time course of analgesia and ventilatory depression is similar, although the analgesia wanes somewhat faster than the ventilatory depression.

Simulated analgesic (y > 1) and ventilatory (y < 1) effects of three different doses of morphine: 0.2 mg/kg (a), 0.2 mg/kg plus an infusion of 1 mg/70 kg/h (b), and a bolus of 0.1 mg/kg every 6 h (c). The analgesic and ventilatory effects peak concurrently, about 90 min after the morphine bolus. Because the concentration versus response relationship is steeper for analgesia than ventilatory depression, the analgesic effect dissipates before the ventilatory depression (Reprinted from Dahan et al. [101]. With permission from Wolters Kluwer Health, Inc.)
It is important to appreciate the slow onset of morphine when titrating to effect. Aubrun and colleagues [102, 103] have advocated postoperative titration of morphine in elderly patients by administering 2–3 mg boluses every 5 min. This is not logical for a drug with a peak effect about 1.5 h after bolus injection. It is surprising that Aubrum and colleagues did not see any toxicity with this approach, given the potential for accumulation with repeated titration of small doses of morphine to effect. However, it does explain why their study is unique in finding that elderly patients require the same amount of opioid as younger patients.
Meperidine
Meperidine, also called “pethidine,” has little role in the management of pain. Meperidine is still a popular drug because of the familiarity of its use, particularly among surgeons and obstetricians. Meperidine is unique among opioids in that it has significant local anesthetic activity [104, 105]. Meperidine has been used as the sole analgesic intrathecally for obstetric anesthesia, but its benefit over a combination of local anesthetic with another opioid is unclear. The only unique perioperative role for meperidine is the treatment of postoperative shivering, in which doses of 10–20 mg are typically effective.
The problems with meperidine are its complex pharmacology and its toxic metabolite. Holmberg and colleagues [106] examined the pharmacokinetics of an intravenous meperidine bolus in young and elderly surgical subjects. They found that elderly patients had reduced meperidine clearance, resulting in a longer half-life for meperidine. There was minimal change in the initial volume of distribution. The clinical implication is that the initial dose of meperidine in elderly subjects should not be reduced based on pharmacokinetics, but meperidine will accumulate in elderly subjects with repeated administration. This makes meperidine a particularly poor choice for administration by PCA in elderly patients [107].
A worrisome aspect of meperidine is the toxic metabolite, normeperidine (or “norpethidine”). In a subsequent study, Holmberg and colleagues examined the renal excretion of both meperidine and normeperidine in elderly surgical patients [108]. Renal excretion was reduced in elderly patients, particularly for normeperidine. The result is that normeperidine will likely accumulate with repeated doses in elderly patients. Because normeperidine is highly epileptogenic, meperidine is probably a poor choice for PCA or other forms of continuous opioid delivery in elderly patients.
Meperidine has several other unique aspects to its pharmacology. It is the only negative inotrope among the opioids [109]. Meperidine also has intrinsic anticholinergic properties, which can result in tachycardia. Elderly patients with coronary artery disease are clearly at risk of adverse events if given drugs that have negative inotropic or positive chronotropic effects.
Last, meperidine is associated with several unusual reactions, including the potential for acute serotonergic syndrome when combined with monoamine oxidase (MAO)-A inhibitors and a significant increase of delirium in elderly patients compared to other opioids [110]. Fortunately, the classic MAO-A inhibitors, phenelzine (Nardil), tranylcypromine (Parnate), and isocarboxazid (Marplan), are now rarely used. Selegiline, often used in Parkinson’s disease, is a weak MAO-B inhibitor and has been implicated in one nonfatal interaction with meperidine [111]. However, given the polypharmacy common in elderly patients, it would seem wise to avoid using meperidine when opioids with more selective pharmacology and inactive metabolites are available.
Hydromorphone
Hydromorphone in many aspects acts as a rapid-onset morphine. However, it lacks the histamine release associated with morphine and does not have active metabolites. There are no studies explicitly examining the role of age in hydromorphone pharmacokinetics or pharmacodynamics. In fact, there are surprisingly few studies examining the perioperative use of hydromorphone. Keeri-Szanto [112] found intraoperative hydromorphone to be approximately eight times more potent than morphine, with a half-life of 4 h versus 5 h for morphine. Kopp et al. [113] investigated whether 4 mg of hydromorphone provided any evidence of preemptive analgesia and found that it did not.
Rapp and colleagues [114] compared hydromorphone PCA to morphine PCA in postoperative patients following lower abdominal surgery. They found that hydromorphone PCA was associated with better mood scores, but with increased incidence of nausea and vomiting. They found that 1 mg of hydromorphone was approximately equianalgesic with 5 mg of morphine. This is about half as potent as suggested by Hill and Zacny [72], who determined that hydromorphone was tenfold more potent than morphine. Although Rapp and colleagues did not specifically study the effects of age, one would expect this ratio to be independent of age in the immediate postoperative period. Because morphine has an active metabolite that accumulates and hydromorphone does not, the apparent potency of morphine relative to hydromorphone may increase with chronic administration.
Lui and colleagues [115] compared epidural hydromorphone to intravenous hydromorphone, both administered by PCA in a double-blind/double-dummy protocol. They found more pruritus in patients receiving epidural hydromorphone, but no differences in postoperative analgesia , bowel function, or patient satisfaction. Overall, hydromorphone in the epidural group was half of that in the intravenous group, indicating that hydromorphone is acting spinally when administered via the epidural route. Hydromorphone and morphine both reach their peak concentrations in the cervical cerebrospinal fluid about 60 min after epidural administration [116], suggesting they have similar potential for delayed ventilatory depression after epidural administration. In a study of obstetric patients, Halpern and colleagues [117] found 0.6 mg of hydromorphone to be clinically indistinguishable from 3 mg of morphine, consistent with the 1: 5 relative potency reported for intravenous hydromorphone and morphine in the postoperative period.
Fentanyl
Fentanyl is among the “cleanest” opioids in terms of pharmacology. It has a rapid onset, predictable metabolism, and inactive metabolites. It is (obviously) the first of the “fentanyl” series of opioids, notable for their rapid metabolism and selective μ potency. It is the only one of the opioids that is available for transdermal and transmucosal delivery, although these methods of administration are being investigated for sufentanil as well.
Bentley et al. [118] studied aging and fentanyl pharmacokinetics in young and elderly groups of patients. They found that fentanyl clearance was decreased among the elderly, resulting in a prolonged half-life.
Scott and Stanski [63] used high-resolution arterial sampling during and after a brief fentanyl infusion to characterize the influence of age on the pharmacokinetics of fentanyl. These investigators did not find any effect of age on the pharmacokinetics of fentanyl or alfentanil, except for a small change in rapid intercompartmental clearance.
The minimal influence of age on the pharmacokinetics of fentanyl was subsequently confirmed by Singleton and colleagues [119]. These investigators found no change in the dose-adjusted concentration of fentanyl between young and elderly patients, except for a transient increase in concentration in elderly individuals at 2 and 4 min after the start of the infusion. These findings are consistent with the decreased rapid intercompartmental clearance reported by Scott and Stanski.
Scott and Stanski used the EEG as a measure of drug effect to estimate the potency of fentanyl [63, 120]. They observed a decrease of approximately 50% in the dose required for 50% of maximal EEG suppression (C50) from age 20 to age 85, as shown in Fig. 18.8. Because the pharmacokinetics of fentanyl seem nearly unchanged by age, it is likely that elderly patients require less fentanyl because of intrinsic increased sensitivity to opioids. Put another way—the elderly brain is twice as sensitive to opioids as a younger brain. This predicts that elderly patients require half of the fentanyl that younger patients require. Because the pharmacodynamics of fentanyl (i.e., the C50) is affected by age, and not the pharmacokinetics, the offset of fentanyl drug effect in elderly patients who receive an appropriately reduced dose of fentanyl should be as fast as it is in younger patients.

The influence of age on the 50% maximal effective dose (C50) of fentanyl, as measured by electroencephalogram depression. Although there is considerable variability, overall there is about a 50% reduction in C50 from age 20 to age 80, reflecting increased brain sensitivity. This has been shown for alfentanil [66] and remifentanil [68] and appears to be a class effect of opioids (Adapted with permission from Scott and Stanski [63]. With permission from American Society for Pharmacology and Experimental Therapeutics)
The 50% reduction in fentanyl suggested by Scott and Stanski’s integrated pharmacokinetic/pharmacodynamic model is in reasonable agreement with an analysis by Martin and colleagues [121] of intraoperative fentanyl utilization. Using the automated electronic record system in place at Duke University Hospital, they found that intraoperative doses of fentanyl decreased by about 10% per decade after age 30.
Other Fentanyl Delivery Systems
Fentanyl is also available in two unique dosage forms : oral transmucosal fentanyl citrate and transdermal fentanyl. Holdsworth and colleagues [122] studied pharmacokinetics and tolerability of a 20-cm2 transdermal fentanyl patch in young and elderly subjects. Plasma fentanyl concentrations were nearly twofold higher in the elderly subjects compared with younger subjects, reflecting either increased absorption or decreased clearance. Given that fentanyl clearance seems unchanged in the elderly, the likely explanation is that transdermal fentanyl absorption is more rapid in elderly patients, possibly because the skin is thinner and poses less of a barrier to fentanyl absorption. The increased concentrations in elderly subjects were associated with increased adverse events—so much so that the patch was removed for the study in every elderly subject, whereas none of the patches were removed in younger subjects.
Davis and colleagues [123] also noted that the time course of absorption of fentanyl through the skin is delayed in the elderly, with subcutaneous fat acting as secondary reservoir leading to prolonged release even after the removal of the patch.
Kharasch and colleagues [124] examined the influence of age on the pharmacokinetics and pharmacodynamics of oral transmucosal fentanyl citrate (the fentanyl “lollipop”). They found no change in the pharmacokinetics of fentanyl with age, including the absorption characteristics of the buccal mucosa. Perhaps unexpectedly, they also found no increase in sensitivity to fentanyl, as measured by pupillary miosis . Thus, in their view, the data do not support reducing the dose of oral transmucosal fentanyl citrate in elderly patients.
Alfentanil
The relationship between opioids and age becomes more complex when we consider alfentanil. Scott and Stanski [63] reported similar findings for alfentanil as previously described for fentanyl. In particular, they did not find any effect of age on the pharmacokinetics of alfentanil, except for a small change in the terminal half-life. Shafer et al. [125] also reported no relationship between age and alfentanil pharmacokinetics. Sitar and colleagues [126] reported a modest decrease in alfentanil clearance and central compartment volume in elderly subjects. In a study that used historical control data, Kent and colleagues [127] also reported a modest decrease in alfentanil clearance with advancing age. Lemmens et al. [128] observed that the pharmacokinetics of alfentanil in men (as studied exclusively by Scott and Stanski) were unaffected by age, whereas the pharmacokinetics in women showed a clear negative correlation between age and clearance.
In an effort to sort out these modestly conflicting results, Maitre et al. [129] pooled alfentanil concentration data from multiple prior studies and performed a population pharmacokinetic analysis to estimate the influence of age and gender on the pharmacokinetics of alfentanil. Maitre et al. found that clearance decreased with age and that the volume of distribution at steady state increased with age, the net effect being a longer terminal half-life with increasing age. That might sound like the end of the story, except that Raemer and colleagues [130] prospectively tested the Maitre et al. pharmacokinetics in two groups of patients, young women and elderly men, using computer-controlled drug administration. In this prospective test, the pharmacokinetics reported by Maitre et al. did not accurately predict the observed plasma alfentanil concentrations. However, pharmacokinetics reported by Scott and Stanski, which predict no influence of age or gender on alfentanil pharmacokinetics, accurately predicted the concentrations in both young women and elderly men. From these results, we can conclude that pharmacokinetics of alfentanil does not change in a clinically significant manner with age.
Although they found no change in pharmacokinetics with age, Scott and Stanski demonstrated that the C50 for EEG depression with alfentanil decreased by 50% in elderly subjects, nearly identical to the increased potency of fentanyl in elderly subjects [66]. This would suggest that, based on pharmacokinetic alterations with age, the dose of alfentanil in elderly patients should be about half of the dose that would be used in younger patients. Unfortunately, subsequent studies by Lemmens et al. [131,132,133], based on clinical endpoints, found no influence of age on the pharmacodynamics of alfentanil. However, Lemmens et al. [134] observed that the alfentanil dose required to maintain adequate anesthesia, when administered by target-controlled infusion, was decreased by approximately 50% in elderly subjects. Thus, Lemmens et al. saw a similar change in dose-response relationship, in that the elderly required half as much opioid as younger subjects, but could not explain it as a pharmacodynamic difference. However, it is a bigger difference in concentration than any of the pharmacokinetic studies would have predicted, and there was no control group—the control group was a historical control group.
Where this leaves us is that there are many studies suggesting that the alfentanil dose in elderly subjects is about half of the dose in younger subjects. The available data suggest that the change is probably pharmacodynamic, but there may be a pharmacokinetic component to the increased sensitivity as well. If the change is mostly pharmacodynamic, perhaps, with a modest change in terminal half-life in elderly subjects, then the offset of alfentanil should be as fast in older subjects as it is in younger subjects, provided the dose has been appropriately reduced.
Sufentanil
Sufentanil is the most potent of the available opioids, with its potency approximately tenfold greater than fentanyl. [79] Age has, at most, only a modest influence on sufentanil pharmacokinetics. Helmers and colleagues [135] found no change in sufentanil pharmacokinetics between young and elderly subjects. Similarly, Gepts and colleagues [136] found no effect of age on sufentanil pharmacokinetics in a complex population analysis. Matteo and colleagues [137] found that the central compartment volume of sufentanil was significantly decreased in elderly patients. This modest pharmacokinetic difference in elderly subjects would be expected to increase the effects of sufentanil in the first few minutes after a bolus dose and not subsequently. However, the elderly patients in Matteo’s study were far more sensitive to sufentanil than the younger subjects. Six of seven elderly patients required naloxone at the end of this study, whereas only one of seven young patients required naloxone. Matteo et al. concluded that elderly patients had increased sensitivity to a given concentration of sufentanil, similar to the increased sensitivity to fentanyl and alfentanil in elderly patients described by Scott and Stanski.
Thus, based on the twofold increase in brain sensitivity to opioids demonstrated for fentanyl and alfentanil in elderly patients, one might expect similar increase in brain sensitivity to sufentanil in elderly patients. Thus, it is surprising that Hofbauer and colleagues [138] did not observe any influence of age on the sufentanil requirement of mechanically ventilated patients in the intensive care unit.
Remifentanil
Remifentanil has the fastest and most predictable metabolism of any of the available opioids. Remifentanil was introduced into clinical practice under Food and Drug Administration guidelines that mandated explicit pharmacokinetic and pharmacodynamic analysis for special populations, including elderly subjects. Thus, the influence of age on remifentanil pharmacokinetics and pharmacodynamics was established in high-resolution trials about three times larger than the trials for fentanyl, alfentanil, or sufentanil. The pharmacokinetic and pharmacodynamic models for remifentanil were reported by Minto and colleagues. [65] In a companion article, Minto et al. [139] used computer simulation to examine the implications of the complex age-related changes on remifentanil dosing. The pharmacokinetics of remifentanil changes with age, as shown in Fig. 18.9. With advancing age, V1, the volume of the central compartment, decreases about 20% from age 20 to 80. Concurrently, clearance decreases about 30% from age 20 to age 80. Figure 18.10 shows the age-related changes in remifentanil pharmacodynamics. As also observed for fentanyl and alfentanil, the C50 for EEG depression is reduced by 50% in elderly subjects, suggesting that remifentanil has about twice the intrinsic potency in elderly subjects as in younger subjects. The t1/2 k e0, half-time of plasma–effect-site equilibration, is also increased in elderly subjects. In the absence of other changes, this would mean that the onset and offset of remifentanil drug effect will be slower in elderly patients.

The influence of age on remifentanil pharmacokinetics. With advancing age, the volume of the central compartment decreases by 50% from age 20 to age 80, and the clearance decreases by 66% (Adapted from Minto et al. [65]. With permission from Wolters Kluwer Health, Inc.)

The influence of age on remifentanil pharmacodynamics. With advancing age, the 50% effective concentration (EC50) declines, reflecting a nearly identical increase in intrinsic potency as seen with fentanyl and alfentanil. Additionally, half-time of blood–brain equilibration (t1/2 k e0) increases (Adapted from Minto et al. [65]. With permission from Wolters Kluwer Health, Inc.)
Figure 18.11 uses computer simulations to examine the time course of blood concentration (solid lines) and effect-site concentration (dashed lines) after a unit bolus of remifentanil. The blood concentrations are higher in elderly subjects because of the smaller central compartment concentration. However, the slower t1/2 k e0 in elderly subjects results in less-rapid equilibration. As a result, the effect-site concentrations in elderly individuals do not increase higher than the effect-site concentrations in young individuals. However, the onset and offset are slower in elderly individuals. For example, in a young individual, the peak drug effect is expected about 90 s after a bolus injection. In an elderly individual, the peak effect is expected about 2–3 min after bolus injection.

Simulations showing the effect-site concentration from identical bolus doses in a 20-, 50-, and 80-year-old subject. The concentrations are highest in the 80-year-old subject because of the reduced size of the central compartment. However, because of the slower blood–brain equilibrium in the 80-year-old subject, the peak effect-site concentration is almost identical in the three simulations. Thus, the smaller V1 is offset by the slower plasma–effect-site equilibration. However, a bolus of remifentanil takes about a minute longer to reach peak effect-site concentrations in elderly subjects (Adapted from Minto et al. [139]. With permission from Wolters Kluwer Health, Inc.)
Figure 18.12 shows the influence of age and weight on remifentanil dosing. As seen in the top graph of Fig. 18.12, elderly subjects need about half of the bolus dose as younger subjects to achieve the same level of drug effect. This is not because of the change in pharmacokinetics. As shown in Fig. 18.11, the peak effect-site levels after a bolus of remifentanil are nearly identical in young and elderly subjects. Rather, the remifentanil bolus is reduced in elderly subjects because of the increased sensitivity of the elderly brain to opioid drug effect, exactly as reported for fentanyl and alfentanil. The bottom graph in Fig. 18.12 shows that elderly subjects require about one-third as rapid an infusion as younger subjects. This reflects the combined influences of the increased sensitivity and the decreased clearance in elderly individuals.

The influence of age and weight on remifentanil bolus dose and infusion rates. Bolus doses should be reduced by 50% in elderly subjects, reflecting the increased brain sensitivity. Infusion rates should be reduced by 66%, reflecting the combined effects of increased brain sensitivity and decreased clearance. LBM lean body mass (Adapted from Minto et al. [139]. With permission from Wolters Kluwer Health, Inc.)
As seen in Fig. 18.12, the influence of weight on remifentanil dosing is considerably less than the influence of age. We point this out because anesthesiologists reflexively adjust remifentanil infusions to body weight, but seem reluctant to make an adequate reduction in infusion rate for elderly individuals.
Figure 18.13 shows the time required for decreases in effect-site concentration of 20%, 50%, and 80% as a function of remifentanil infusion duration. These would be the “20% effect-site decrement time,” the “50% effect-site decrement time,” and the “80% effect-site decrement time,” respectively. For each decrement time, the expected relationship is shown for a 20-year-old patient and an 80-year-old patient. Figure 18.13 suggests that elderly patients can be expected to recover from remifentanil about as fast as younger subjects, provided the dose has been appropriately reduced (e.g., Fig. 18.12).

The 20%, 50%, and 80% effect-site decrement curves for 20- and 80-year-old subjects. Provided remifentanil dose is adequately reduced, as shown in this figure, there should be little difference in the awakening time as a function of age
The unique features of remifentanil are its rapid clearance and rapid k e0, resulting in a rapid onset and offset of drug effect. It is tempting to speculate that these characteristics will make remifentanil an easy drug to titrate and that clinicians will not need to consider patient covariates such as advanced age when choosing a dosing regimen. However, the rapid onset of drug effect may be accompanied by rapid onset of adverse events such as apnea and muscle rigidity. The rapid offset of drug effect can result in patients who are in severe pain at a time when the anesthesiologist is ill-equipped to deal with the problem, for example, when the patient is in transit to the recovery room. It is thus important that anesthesiologists understand the proper dose adjustment required for the elderly. By adjusting the bolus and infusion doses, the anesthesiologist can hope to avoid the peaks and valleys in remifentanil concentration that might expose elderly patients to risk. When the proper adjustment is made, the variability in remifentanil pharmacokinetics is considerably less than for any other intravenous opioid. This makes remifentanil the most predictable opioid for treatment of the elderly.
Methadone
Methadone has several distinguishing characteristics, including having the longest terminal half-life and being supplied as a racemic mixture with surprising stereospecific pharmacology. As shown in Table 18.1 and as evident in Fig. 18.1, the terminal half-life of methadone is approximately 1 day [66]. As a result, it will take nearly a week of methadone dosing to reach steady state. When methadone is used as a chronic analgesic, particularly in elderly patients, the patient and physician must be made aware that steady state will not be reached for several days, requiring vigilance for accumulation to toxicity during the “run-in” titration of methadone for analgesia. Also, adequate arrangements for rescue analgesia must be available during the period before steady-state levels.
Methadone’s another unique feature is that it is supplied as a racemate with two enantiomers. l-Methadone is an opioid agonist, whereas d-methadone is an N-methyl-D-aspartate (NMDA) antagonist [140]. The potency of the d-methadone in blocking NMDA is such that, at clinically used doses, it may be effective in attenuating opioid tolerance and preventing central sensitization (hyperalgesia) [141, 142]. There are no specific studies examining the pharmacokinetics and pharmacodynamics of methadone in elderly subjects. However, as the increased brain sensitivity to opioid drug effect seems to be a class effect for opioids, it seems prudent to reduce methadone doses by about 50% in elderly patients compared with younger patients. Additionally, the NMDA-blocking activity of d-methadone may provide some analgesic synergy between the enantiomers.
The sustained effect of methadone and the combination of μ opioid agonism and NMDA antagonism suggest that methadone may be a good choice for postoperative analgesia. However, methadone must be used with great caution for the treatment of acute pain following surgery. The very long half-life may lead to delayed respiratory depression several days after surgery. Additionally, methadone is associated with QT prolongation, which may lead to fatal arrhythmia [143]. The risk of arrhythmia is particularly concerning with outpatient use of methadone, where the concentrations may be rising in an unmonitored setting. These concerns are highlighted in the black box warning on the methadone product insert. The risks and benefits of methadone for acute pain control following surgery must be carefully considered and likely limit the utility of methadone as an oral analgesic following hospital discharge.
Patient-Controlled Anesthesia
PCA devices are very effective means to provide postoperative analgesia in elderly patients (see Chap. 28). Lavand’Homme and De Kock [144] have reviewed the use of PCA in the elderly. They observed that poor pain management places elderly patients at risk of confusion and outright delirium, and this may be associated with poorer clinical outcomes. They emphasized that increased monitoring and individualization of dosage are essentials in PCA management of elderly patients. They also observed that elderly patients may need additional time to become familiar with PCA devices and that the devices will become ineffective if elderly patients become confused or agitated.
Macintyre and Jarvis [145] examined morphine PCA in elderly patients and observed that age is the best predictor of postoperative morphine requirements . They found that the average PCA morphine use in the first 24 h after surgery was approximately 100−age. However, they also emphasized that the dose needed to be individualized, because there was tenfold variation in the dose in each age category.
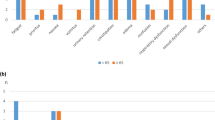
This is similar to the results of Woodhouse and Mather [146]. They found that elderly patients required significantly less fentanyl and morphine administered by PCA following surgery. They also identified a similar trend for meperidine, but it was less steep and characterized by higher variability. As seen in Fig. 18.14, elderly patients required about half as much morphine and fentanyl as younger subjects, consistent with the “50% reduction” suggestion at the beginning of the chapter.

Twenty-four-hour cumulative patient-controlled analgesia opioid administration as a function of age. Morphine and fentanyl both show the expected reduction in dose of about 50%, as predicted by the pharmacokinetic/pharmacodynamic modeling. Meperidine (pethidine) is more variable, perhaps reflecting its more complex pharmacology, or the stimulating effects of normeperidine (Reprinted from Woodhouse and Mather [147]. With permission from John Wiley & Sons)
Gagliese and colleagues [146] also found an approximately 50% reduction in PCA opioid use in elderly patients. In their study, patients in the younger group (average age = 39) expected more severe pain than those in the older group (average age = 67). However, both groups obtained similar efficacy from their PCA devices and expressed similar levels of satisfaction with PCA as a means of managing postoperative analgesia . The average 24 h dose of morphine (or morphine equivalents) in the younger patients was 67 mg at the end of day one and 44 mg at the end of day two. In the older patients, the average dose was 39 mg at the end of day 1 and 28 mg at the end of day 2. In an accompanying editorial, Ready [148] emphasized that patients must be able to understand and participate in their care, emphasizing the need to individualize therapy for elderly patients in whom a cognitive assessment might be appropriate before using PCA.
It is reasonable that other interventions, such as nerve blocks, infusions of local anesthetic, and adjuvant analgesic therapy, be combined with PCA to provide adequate analgesia at the lowest possible opioid dose in elderly patients (see Chaps. 19 and 28). Beattie et al. [149] have reported that ketorolac effectively reduces morphine doses in elderly subjects. In this case, the reduced opioid requirement must be balanced against the risk of gastric bleeding and fluid retention induced by ketorolac. However, in appropriate patients, one or two doses of ketorolac are associated with only modest risk and would be expected to provide significant synergy with morphine [150, 151].
Suggested Guidelines for Chronic Opioids in the Elderly
The subject of opioids in the management of chronic pain in the elderly has been extensively reviewed [152, 153]. A few basic principles will be emphasized here:
-
1.
In general, opioids should be reserved for those elderly patients in whom less-toxic alternatives, such as acetaminophen and nonsteroidal antiinflammatory drugs, have proven ineffective.
-
2.
It is best to start with the weaker opioids, such as codeine, and titrate to effect. The stronger opioids should be reserved for patients whose symptoms are inadequately treated by weaker opioids.
-
3.
Careful monitoring during the initial dose titration is absolutely essential, particularly with opioids or delivery systems associated with long half-lives and time to steady state, such as methadone, oral sustained-release preparations, and transdermal fentanyl.
-
4.
Opioid-induced constipation may be reduced by the use of a peripheral opioid antagonist, such as alvimopan [154] and methylnaltrexone [155].
-
5.
Elderly patients are at increased risk of drug interactions (see Chap. 21). The risk of drug interactions particularly precludes the use of chronic meperidine in elderly patients. However, opioids should be used with great caution if combined with any drugs that decrease consciousness (e.g., benzodiazepines). Figure 18.15 shows the interaction between remifentanil and propofol on ventilation in healthy volunteers as reported by Nieuwenhuijs and colleagues [156]. Propofol and remifentanil individually have modest effects on ventilation; however, when combined (solid triangles), they demonstrate profound depression of ventilation. This effect will be exaggerated in elderly patients because of the increased sensitivity to opioid drug effects.
Fig. 18.15 
The interaction between remifentanil and propofol on ventilation demonstrates a class effect for opioid/hypnotic synergy. In this figure, propofol very slightly changes the slope of the CO2 versus ventilation curve, and remifentanil very slightly changes the apnea threshold without changing the slope. However, the combination of propofol and remifentanil (triangles, lower right) profoundly displaces both the slope and the apneic threshold (Reprinted from Nieuwenhuijs et al. [156]. With permission from Wolters Kluwer Health, Inc.)
-
6.
Elderly patients are at increased risk of confusion in response to opioids.
-
7.
Rotation of opioids may permit lower doses to be used, because of the incomplete cross-tolerance and individual differences in analgesic versus toxicity profiles among individuals.

Conclusion
Opioids are used for balanced general anesthesia and are appropriate for both acute and chronic pain in elderly patients, particularly when nonopioid analgesics have failed to provide adequate pain relief. Elderly patients, on average, need about half the dose of opioids as younger patients to achieve the same level of analgesic effect. The biologic basis for the increased brain sensitivity (pharmacodynamic increased potency) to opioids in elderly patients is not completely understood. Elderly patients have factors that place them at increased risk of opioid toxicity, including increased pharmacologic variability, frequent polypharmacy, noncompliance with dosage regimens, and impaired renal and hepatic function.
Notes
- 1.
Data extensively reanalyzed to obtain volume and clearance estimates.
- 2.
Original data provided by S. Bjorkman and fit using population model to create estimates in Table 18.1.
- 3.
Based on a time to peak of 8.5 min in goats ()! It is not great, but it is the best onset data available.
- 4.
Based on a time to peak effect of 15–20 min.
- 5.
- 6.
Scaled to fentanyl based on the relative EEG potency of fentanyl and remifentanil [65].
- 7.
he MEC range given by Dahlstrom was 6–31 ng/mL, with a mean of 16 ng/mL. We chose 8 ng/mL, at the lower end of the reported range, because the average value of 16 ng/mL predicted equianalgesic morphine that seemed excessive.
- 8.
This was the most difficult potency to determine from the literature. Hill and Zacny documented a tenfold bolus dose potency difference versus morphine, which was the final basis for calculating this number and is similar to the value suggested by the Coda paper.
References
Ventafridda V, Tamburini M, Caraceni A, De Conno F, Naldi F. A validation study of the WHO method for cancer pain relief. Cancer. 1987;59:850–6.
Jacox A, Carr DB, Payne R. New clinical-practice guidelines for the management of pain in patients with cancer. N Engl J Med. 1994;330:651–5.
Bafitis H, Sargent F. Human physiological adaptability through the life sequence. J Gerontol. 1977;32:402–10.
Klein U, Klein M, Sturm H, et al. The frequency of adverse drug reactions as dependent upon age, sex and duration of hospitalization. Int J Clin Pharmacol Biopharm. 1976;13:187–95.
Crooks J. Aging and drug disposition—pharmacodynamics. J Chronic Dis. 1983;36:85–90.
Pert CB, Snyder SH. Opiate receptor: demonstration in nervous tissue. Science. 1973;179:1011–4.
Simon EJ, Hiller JM, Edelman I. Stereospecific binding of the potent narcotic analgesic (3H) Etorphine to ratbrain homogenate. Proc Natl Acad Sci U S A. 1973;70:1947–9.
Terenius L. Characteristics of the “receptor” for narcotic analgesics in synaptic plasma membrane fraction from rat brain. Acta Pharmacol Toxicol (Copenh). 1973;33:377–84.
Hughes J, Smith TW, Kosterlitz HW, Fothergill LA, Morgan BA, Morris HR. Identification of two related pentapeptides from the brain with potent opiate agonist activity. Nature. 1975;258:577–80.
Li CH, Chung D. Isolation and structure of an untriakontapeptide with opiate activity from camel pituitary glands. Proc Natl Acad Sci U S A. 1976;73:1145–8.
Goldstein A, Tachibana S, Lowney LI, Hunkapiller M, Hood L. Dynorphin-(1–13), an extraordinarily potent opioid peptide. Proc Natl Acad Sci U S A. 1979;76:6666–70.
Martin WR, Eades CG, Thompson JA, Huppler RE, Gilbert PE. The effects of morphine- and nalorphine-like drugs in the nondependent and morphine-dependent chronic spinal dog. J Pharmacol Exp Ther. 1976;197:517–32.
Chang KJ, Cooper BR, Hazum E, Cuatrecasas P. Multiple opiate receptors: different regional distribution in the brain and differential binding of opiates and opioid peptides. Mol Pharmacol. 1979;16:91–104.
Robson LE, Kosterlitz HW. Specific protection of the binding sites of D-Ala2-D-Leu5-enkephalin (delta-receptors) and dihydromorphine (mu-receptors). Proc R Soc Lond B Biol Sci. 1979;205:425–32.
Schulz R, Wuster M, Krenss H, Herz A. Selective development of tolerance without dependence in multiple opiate receptors of mouse vas deferens. Nature. 1980;285:242–3.
Pasternak GW, Childers SR, Snyder SH. Opiate analgesia: evidence for mediation by a subpopulation of opiate receptors. Science. 1980;208:514–6.
Ling GS, Spiegel K, Nishimura SL, Pasternak GW. Dissociation of morphine’s analgesic and respiratory depressant actions. Eur J Pharmacol. 1983;86:487–8.
Ling GS, Spiegel K, Lockhart SH, Pasternak GW. Separation of opioid analgesia from respiratory depression: evidence for different receptor mechanisms. J Pharmacol Exp Ther. 1985;232:149–55.
Brown GP, Yang K, King MA, et al. 3-Methoxynaltrexone, a selective heroin/morphine-6beta-glucuronide antagonist. FEBS Lett. 1997;412:35–8.
Crews JC, Sweeney NJ, Denson DD. Clinical efficacy of methadone in patients refractory to other mu-opioid receptor agonist analgesics for management of terminal cancer pain. Case presentations and discussion of incomplete cross-tolerance among opioid agonist analgesics. Cancer. 1993;72:2266–72.
Mercadante S. Opioid rotation for cancer pain: rationale and clinical aspects. Cancer. 1999;86:1856–66.
Chang A, Emmel DW, Rossi GC, Pasternak GW. Methadone analgesia in morphine-insensitive CXBK mice. Eur J Pharmacol. 1998;351:189–91.
Abbadie C, Rossi GC, Orciuolo A, Zadina JE, Pasternak GW. Anatomical and functional correlation of the endomorphins with mu opioid receptor splice variants. Eur J Neurosci. 2002;16:1075–82.
Cadet P. Mu opiate receptor subtypes. Med Sci Monit. 2004;10:MS28–32.
Stefano GB, Hartman A, Bilfinger TV, et al. Presence of the mu3 opiate receptor in endothelial cells. Coupling to nitric oxide production and vasodilation. J Biol Chem. 1995;270:30290–3.
Kozak CA, Filie J, Adamson MC, Chen Y, Yu L. Murine chromosomal location of the mu and kappa opioid receptor genes. Genomics. 1994;21:659–61.
Belknap JK, Mogil JS, Helms ML, et al. Localization to chromosome 10 of a locus influencing morphine analgesia in crosses derived from C57BL/6 and DBA/2 strains. Life Sci. 1995;57:PL117–24.
Lötsch J, Geisslinger G. Are mu-opioid receptor polymorphisms important for clinical opioid therapy? Trends Mol Med. 2005;11:82–9.
Romberg RR, Olofsen E, Bijl H, et al. Polymorphism of mu-opioid receptor gene (OPRM1:c.118A > G) does not protect against opioid-induced respiratory depression despite reduced analgesic response. Anesthesiology. 2005;102:522–30.
Pasternak GW. Multiple opiate receptors: deja vu all over again. Neuropharmacology. 2004;47(Suppl 1):312–23.
Chen Y, Mestek A, Liu J, Hurley JA, Yu L. Molecular cloning and functional expression of a mu-opioid receptor from rat brain. Mol Pharmacol. 1993;44:8–12.
Wang JB, Imai Y, Eppler CM, Gregor P, Spivak CE, Uhl GR. Mu opiate receptor: cDNA cloning and expression. Proc Natl Acad Sci U S A. 1993;90:10230–4.
Pan YX, Xu J, Mahurter L, Xu M, Gilbert AK, Pasternak GW. Identification and characterization of two new human mu opioid receptor splice variants, hMOR-1O and hMOR-1X. Biochem Biophys Res Commun. 2003;301:1057–61.
Connor M, Christie MD. Opioid receptor signalling mechanisms. Clin Exp Pharmacol Physiol. 1999;26:493–9.
North RA. Opioid actions on membrane ion channels. In: Herz A, editor. Opioids. Handbook of experimental pharmacology, vol. 104. Berlin: Springer-Verlag; 1993. p. 773–97.
Bohn LM, Lefkowitz RJ, Gainetdinov RR, Peppel K, Caron MG, Lin FT. Enhanced morphine analgesia in mice lacking beta-arrestin 2. Science. 1999;286:2495–8.
Raehal KM, Walker JK, Bohn LM. Morphine side effects in beta-arrestin 2 knockout mice. J Pharmacol Exp Ther. 2005;314:1195–201.
DeWire SM, Yamashita DS, Rominger DH, Liu G, Cowan CL, Graczyk TM, Chen XT, Pitis PM, Gotchev D, Yuan C, Koblish M, Lark MW, Violin JD. A G protein-biased ligand at the μ-opioid receptor is potently analgesic with reduced gastrointestinal and respiratory dysfunction compared with morphine. J Pharmacol Exp Ther. 2013;344:708–17.
Soergel DG, Subach RA, Burnham N, Lark MW, James IE, Sadler BM, Skobieranda F, Violin JD, Webster LR. Biased agonism of the μ-opioid receptor by TRV130 increases analgesia and reduces on-target adverse effects versus morphine: a randomized, double-blind, placebo-controlled, crossover study in healthy volunteers. Pain. 2014;155:1829–35.
Manglik A, Lin H, Aryal DK, McCorvy JD, Dengler D, Corder G, Levit A, Kling RC, Bernat V, Hübner H, Huang XP, Sassano MF, Giguère PM, Löber S, Da Duan, Scherrer G, Kobilka BK, Gmeiner P, Roth BL, Shoichet BK. Structure-based discovery of opioid analgesics with reduced side effects. Nature. 2016;537:185–90.
Viscusi ER, Webster L, Kuss M, Daniels S, Bolognese JA, Zuckerman S, Soergel DG, Subach RA, Cook E, Skobieranda F. A randomized, phase 2 study investigating TRV130, a biased ligand of the μ-opioid receptor, for the intravenous treatment of acute pain. Pain. 2016;157:264–72.
Ueno E, Liu DD, Ho IK, Hoskins B. Opiate receptor characteristics in brains from young, mature and aged mice. Neurobiol Aging. 1988;9:279–83.
Hess GD, Joseph JA, Roth GS. Effect of age on sensitivity to pain and brain opiate receptors. Neurobiol Aging. 1981;2:49–55.
Petkov VV, Petkov VD, Grahovska T, Konstantinova E. Enkephalin receptor changes in rat brain during aging. Gen Pharmacol. 1984;15:491–5.
Fulop T Jr, Kekessy D, Foris G. Impaired coupling of naloxone sensitive opiate receptors to adenylate cyclase in PMNLs of aged male subjects. Int J Immunopharmacol. 1987;9(6):651–7.
Hoskins B, Ho IK. Age-induced differentiation of morphine’s effect on cyclic nucleotide metabolism. Neurobiol Aging. 1987;8:473–6.
Smith MA, Gray JD. Age-related differences in sensitivity to the antinociceptive effects of opioids in male rats. Influence of nociceptive intensity and intrinsic efficacy at the mu receptor. Psychopharmacology. 2001;156:445–53.
Van Crugten JT, Somogyi AA, Nation RL, Reynolds G. The effect of old age on the disposition and antinociceptive response of morphine and morphine-6 betaglucuronide in the rat. Pain. 1997;71:199–205.
Hoskins B, Burton CK, Ho IK. Differences in morphine-induced antinociception and locomotor activity in mature adult and aged mice. Pharmacol Biochem Behav. 1986;25:599–605.
Ayers E, Warmington M, Reid MC. Chronic pain perspectives: managing chronic pain in older adults: 6 steps to overcoming medication barriers. J Fam Pract. 2012;61:S16–21.
Helme RD, Gibson SJ. The epidemiology of pain in elderly people. Clin Geriatr Med. 2001;17:417–31.
Verhaak PF, Kerssens JJ, Dekker J, Sorbi MJ, Bensing JM. Prevalence of chronic benign pain disorder among adults: a review of the literature. Pain. 1998;77:231–9.
Sorkin BA, Rudy TE, Hanlon RB, Turk DC, Stieg RL. Chronic pain in old and young patients: differences appear less important than similarities. J Gerontol. 1990;45:P64–8.
Edwards RR, Fillingim RB. Age-associated differences in responses to noxious stimuli. J Gerontol A Biol Sci Med Sci. 2001;56:M180–5.
Edwards RR, Fillingim RB, Ness TJ. Age-related differences in endogenous pain modulation: a comparison of diffuse noxious inhibitory controls in healthy older and younger adults. Pain. 2003;101:155–65.
Washington LL, Gibson SJ, Helme RD. Age-related differences in the endogenous analgesic response to repeated cold water immersion in human volunteers. Pain. 2000;89:89–96.
Casale G, Pecorini M, Cuzzoni G, de Nicola P. Betaendorphin and cold pressor test in the aged. Gerontology. 1985;31:101–5.
Zheng Z, Gibson SJ, Khalil Z, Helme RD, McMeeken JM. Age-related differences in the time course of capsaicininduced hyperalgesia. Pain. 2000;85:51–8.
Chakour MC, Gibson SJ, Bradbeer M, Helme RD. The effect of age on A delta- and C-fibre thermal pain perception. Pain. 1996;64:143–52.
Cepeda MS, Farrar JT, Baumgarten M, Boston R, Carr DB, Strom BL. Side effects of opioids during short-term administration: effect of age, gender, and race. Clin Pharmacol Ther. 2003;74:102–12.
Sinclair DR, Chung F, Mezei G. Can postoperative nausea and vomiting be predicted? Anesthesiology. 1999;91:109–18.
Junger A, Hartmann B, Benson M, et al. The use of an anesthesia information management system for prediction of antiemetic rescue treatment at the postanesthesia care unit. Anesth Analg. 2001;92(5):1203–9.
Scott JC, Stanski DR. Decreased fentanyl/alfentanil dose requirement with increasing age: a pharmacodynamic basis. J Pharmacol Exp Ther. 1987;240:159–66.
Hudson RJ, Bergstrom RG, Thomson IR, Sabourin MA, Rosenbloom M, Strunin L. Pharmacokinetics of sufentanil in patients undergoing abdominal aortic surgery. Anesthesiology. 1989;70:426–31.
Minto CF, Schnider TW, Egan T, et al. The influence of age and gender on the pharmacokinetics and pharmacodynamics of remifentanil. I. Model development. Anesthesiology. 1997;86:10–23.
Lotsch J, Skarke C, Schmidt H, Liefhold J, Geisslinger G. Pharmacokinetic modeling to predict morphine and morphine-6-glucuronide plasma concentrations in healthy young volunteers. Clin Pharmacol Ther. 2002;72:151–62.
Inturrisi CE, Colburn WA, Kaiko RF, Houde RW, Foley KM. Pharmacokinetics and pharmacodynamics of methadone in patients with chronic pain. Clin Pharmacol Ther. 1987;41:392–401.
Bjorkman S. Reduction and lumping of physiologically based pharmacokinetic models: prediction of the disposition of fentanyl and pethidine in humans by successively simplified models. J Pharmacokinet Pharmacodyn. 2003;30:285–307.
Drover DR, Angst MS, Valle M, et al. Input characteristics and bioavailability after administration of immediate and a new extended-release formulation of hydromorphone in healthy volunteers. Anesthesiology. 2002;97:827–36.
Qiao GL, Fung KF. Pharmacokinetic-pharmacodynamic modelling of meperidine in goats (II): modelling. J Vet Pharmacol Ther. 1994;17:127–34.
Inturrisi CE, Portenoy RK, Max MB, Colburn WA, Foley KM. Pharmacokinetic-pharmacodynamic relationships of methadone infusions in patients with cancer pain. Clin Pharmacol Ther. 1990;47:565–77.
Hill JL, Zacny JP. Comparing the subjective, psychomotor, and physiological effects of intravenous hydromorphone and morphine in healthy volunteers. Psychopharmacology. 2000;152:31–9.
Shafer SL, Varvel JR. Pharmacokinetics, pharmacodynamics, and rational opioid selection. Anesthesiology. 1991;74:53–63.
Shafer SL, Gregg KM. Algorithms to rapidly achieve and maintain stable drug concentrations at the site of drug effect with a computer-controlled infusion pump. J Pharmacokinet Biopharm. 1992;20:147–69.
Henthorn TK, Krejcie TC, Shanks CA, Avram MJ. Time-dependent distribution volume and kinetics of the pharmacodynamic effector site. J Pharm Sci. 1992;81:1136–8.
Wada DR, Drover DR, Lemmens HJ. Determination of the distribution volume that can be used to calculate the intravenous loading dose. Clin Pharmacokinet. 1998;35:1–7.
Gourlay GK, Kowalski SR, Plummer JL, Cousins MJ, Armstrong PJ. Fentanyl blood concentration-analgesic response relationship in the treatment of postoperative pain. Anesth Analg. 1988;67:329–37.
Lehmann KA, Ribbert N, Horrichs-Haermeyer G. Postoperative patient-controlled analgesia with alfentanil: analgesic efficacy and minimum effective concentrations. J Pain Symptom Manag. 1990;5:249–58.
Scott JC, Cooke JE, Stanski DR. Electroencephalographic quantitation of opioid effect: comparative pharmacodynamics of fentanyl and sufentanil. Anesthesiology. 1991;74:34–42.
Dahlstrom B, Tamsen A, Paalzow L, Hartvig P. Patient-controlled analgesic therapy. Part IV. Pharmacokinetics and analgesic plasma concentrations of morphine. Clin Pharmacokinet. 1982;7:266–79.
Gourlay GK, Willis RJ, Wilson PR. Postoperative pain control with methadone: influence of supplementary methadone doses and blood concentration-response relationships. Anesthesiology. 1984;61:19–26.
Mather LE, Glynn CJ. The minimum effective analgetic blood concentration of pethidine in patients with intractable pain. Br J Clin Pharmacol. 1982;14:385–90.
Coda B, Tanaka A, Jacobson RC, Donaldson G, Chapman CR. Hydromorphone analgesia after intravenous bolus administration. Pain. 1997;71:41–8.
Hughes MA, Glass PS, Jacobs JR. Context-sensitive half-time in multicompartment pharmacokinetic models for intravenous anesthetic drugs. Anesthesiology. 1992;76:334–41.
Youngs EJ, Shafer SL. Pharmacokinetic parameters relevant to recovery from opioids. Anesthesiology. 1994;81:833–42.
Gintzler AR, Gershon MD, Spector S. A nonpeptide morphine-like compound: immunocytochemical localization in the mouse brain. Science. 1978;199:447–8.
Goldstein A, Barrett RW, James IF, et al. Morphine and other opiates from beef brain and adrenal. Proc Natl Acad Sci U S A. 1985;82:5203–7.
Donnerer J, Oka K, Brossi A, Rice KC, Spector S. Presence and formation of codeine and morphine in the rat. Proc Natl Acad Sci U S A. 1986;83:4566–7.
Cardinale GJ, Donnerer J, Finck AD, Kantrowitz JD, Oka K, Spector S. Morphine and codeine are endogenous components of human cerebrospinal fluid. Life Sci. 1987;40:301–6.
Lotsch J, Geisslinger G. Morphine-6-glucuronide: an analgesic of the future? Clin Pharmacokinet. 2001;40:485–99.
Paul D, Standifer KM, Inturrisi CE, Pasternak GW. Pharmacological characterization of morphine-6 beta-glucuro-nide, a very potent morphine metabolite. J Pharmacol Exp Ther. 1989;251:477–83.
Lotsch J, Kobal G, Stockmann A, Brune K, Geisslinger G. Lack of analgesic activity of morphine-6-glucuronide after short-term intravenous administration in healthy volunteers. Anesthesiology. 1997;87(6):1348–58.
Lotsch J, Kobal G, Geisslinger G. No contribution of morphine-6-glucuronide to clinical morphine effects after short-term administration. Clin Neuropharmacol. 1998;21:351–4.
Wolff T, Samuelsson H, Hedner T. Morphine and morphine metabolite concentrations in cerebrospinal fluid and plasma in cancer pain patients after slow-release oral morphine administration. Pain. 1995;62:147–54.
Portenoy RK, Foley KM, Stulman J, et al. Plasma morphine and morphine-6-glucuronide during chronic morphine therapy for cancer pain: plasma profiles, steady-state concentrations and the consequences of renal failure. Pain. 1991;47:13–9.
Cockcroft DW, Gault MH. Prediction of creatinine clearance from serum creatinine. Nephron. 1976;16:31–41.
Lotsch J, Skarke C, Schmidt H, Grosch S, Geisslinger G. The transfer half-life of morphine-6-glucuronide from plasma to effect site assessed by pupil size measurement in healthy volunteers. Anesthesiology. 2001;95:1329–38.
Skarke C, Jarrar M, Erb K, Schmidt H, Geisslinger G, Lotsch J. Respiratory and miotic effects of morphine in healthy volunteers when P-glycoprotein is blocked by quinidine. Clin Pharmacol Ther. 2003;74:303–11.
Skarke C, Darimont J, Schmidt H, Geisslinger G, Lotsch J. Analgesic effects of morphine and morphine-6-glucuronide in a transcutaneous electrical pain model in healthy volunteers. Clin Pharmacol Ther. 2003;73:107–21.
Letrent SP, Polli JW, Humphreys JE, Pollack GM, Brouwer KR, Brouwer KL. P-glycoprotein-mediated transport of morphine in brain capillary endothelial cells. Biochem Pharmacol. 1999;58:951–7.
Dahan A, Romberg R, Teppema L, Sarton E, Bijl H, Olofsen E. Simultaneous measurement and integrated analysis of analgesia and respiration after an intravenous morphine infusion. Anesthesiology. 2004;101:1201–9.
Aubrun F, Monsel S, Langeron O, Coriat P, Riou B. Postoperative titration of intravenous morphine in the elderly patient. Anesthesiology. 2002;96:17–23.
Aubrun F, Bunge D, Langeron O, Saillant G, Coriat P, Riou B. Postoperative morphine consumption in the elderly patient. Anesthesiology. 2003;99:160–5.
Wagner LE 2nd, Eaton M, Sabnis SS, Gingrich KJ. Meperidine and lidocaine block of recombinant voltage-dependent Na+ channels: evidence that meperidine is a local anesthetic. Anesthesiology. 1999;91:1481–90.
Wolff M, Olschewski A, Vogel W, Hempelmann G. Meperidine suppresses the excitability of spinal dorsal horn neurons. Anesthesiology. 2004;100:947–55.
Holmberg L, Odar-Cederlof I, Boreus LO, Heyner L, Ehrnebo M. Comparative disposition of pethidine and norpethidine in old and young patients. Eur J Clin Pharmacol. 1982;22:175–9.
Seifert CF, Kennedy S. Meperidine is alive and well in the new millennium: evaluation of meperidine usage patterns and frequency of adverse drug reactions. Pharmacotherapy. 2004;24:776–83.
Odar-Cederlof I, Boreus LO, Bondesson U, Holmberg L, Heyner L. Comparison of renal excretion of pethidine (meperidine) and its metabolites in old and young patients. Eur J Clin Pharmacol. 1985;28:171–5.
Huang YF, Upton RN, Rutten AJ, Mather LE. The hemodynamic effects of intravenous bolus doses of meperidine in conscious sheep. Anesth Analg. 1994;78:442–9.
Fong HK, Sands LP, Leung JM. The role of postoperative analgesia in delirium and congnitive decline in elderly patients: a systematic review. Anesth Analg. 2006;102:1255–66.
Zornberg GL, Bodkin JA, Cohen BM. Severe adverse interaction between pethidine and selegiline. Lancet. 1991;337:246.
Keeri-Szanto M. Anaesthesia time/dose curves IX the use of hydromorphone in surgical anaesthesia and postoperative pain relief in comparison to morphine. Can Anaesth Soc J. 1976;23:587–95.
Kopp A, Wachauer D, Hoerauf KH, Zulus E, Reiter WJ, Steltzer H. Effect of preemptive hydromorphone administration on postoperative pain relief—a randomized controlled trial. Wien Klin Wochenschr. 2000;112:1002–6.
Rapp SE, Egan KJ, Ross BK, Wild LM, Terman GW, Ching JM. A multidimensional comparison of morphine and hydromorphone patient-controlled analgesia. Anesth Analg. 1996;82:1043–8.
Liu S, Carpenter RL, Mulroy MF, et al. Intravenous versus epidural administration of hydromorphone. Effects on analgesia and recovery after radical retropubic prostatectomy. Anesthesiology. 1995;82:682–8.
Brose WG, Tanelian DL, Brodsky JB, Mark JB, Cousins MJ. CSF and blood pharmacokinetics of hydromorphone and morphine following lumbar epidural administration. Pain. 1991;45:11–5.
Halpern SH, Arellano R, Preston R, et al. Epidural morphine vs hydromorphone in post-caesarean section patients. Can J Anaesth. 1996;43:595–8.
Bentley JB, Borel JD, Nenad RE Jr, Gillespie TJ. Age and fentanyl pharmacokinetics. Anesth Analg. 1982;61:968–71.
Singleton MA, Rosen JI, Fisher DM. Pharmacokinetics of fentanyl in the elderly. Br J Anaesth. 1988;60:619–22.
Scott JC, Ponganis KV, Stanski DR. EEG quantitation of narcotic effect: the comparative pharmacodynamics of fentanyl and alfentanil. Anesthesiology. 1985;62:234–41.
Martin G, Glass PS, Breslin DS, et al. A study of anesthetic drug utilization in different age groups. J Clin Anesth. 2003;15:194–200.
Holdsworth MT, Forman WB, Killilea TA, et al. Transdermal fentanyl disposition in elderly subjects. Gerontology. 1994;40:32–7.
Davis MP, Srivastava M. Demographics, assessment and management of pain in the elderly. Drugs Aging. 2003;20:23–57.
Kharasch ED, Hoffer C, Whittington D. Influence of age on the pharmacokinetics and pharmacodynamics of oral transmucosal fentanyl citrate. Anesthesiology. 2004;101:738–43.
Shafer A, Sung ML, White PF. Pharmacokinetics and pharmacodynamics of alfentanil infusions during general anesthesia. Anesth Analg. 1986;65:1021–8.
Sitar DS, Duke PC, Benthuysen JL, Sanford TJ, Smith NT. Aging and alfentanil disposition in healthy volunteers and surgical patients. Can J Anaesth. 1989;36:149–54.
Kent AP, Dodson ME, Bower S. The pharmacokinetics and clinical effects of a low dose of alfentanil in elderly patients. Acta Anaesthesiol Belg. 1988;39:25–33.
Lemmens HJ, Burm AG, Hennis PJ, Gladines MP, Bovill JG. Influence of age on the pharmacokinetics of alfentanil. Gender dependence. Clin Pharmacokinet. 1990;19:416–22.
Maitre PO, Vozeh S, Heykants J, Thomson DA, Stanski DR. Population pharmacokinetics of alfentanil: the average dose-plasma concentration relationship and interindividual variability in patients. Anesthesiology. 1987;68:59–67.
Raemer DB, Buschman A, Varvel JR, et al. The prospective use of population pharmacokinetics in a computer driven system for alfentanil. Anesthesiology. 1990;73:66–72.
Lemmens HJ, Burm AG, Bovill JG, Hennis PJ. Pharmacodynamics of alfentanil as a supplement to nitrous oxide anaesthesia in the elderly patient. Br J Anaesth. 1988;61:173–9.
Lemmens HJ, Bovill JG, Hennis PJ, Burm AG. Age has no effect on the pharmacodynamics of alfentanil. Anesth Analg. 1988;67:956–60.
Lemmens HJ, Burm AG, Bovill JG, Hennis PJ, Gladines MP. Pharmacodynamics of alfentanil. The role of plasma protein binding. Anesthesiology. 1992;76:65–70.
Lemmens HJ, Bovill JG, Burm AG, Hennis PJ. Alfentanil infusion in the elderly. Prolonged computer-assisted infusion of alfentanil in the elderly surgical patient. Anaesthesia. 1988;43:850–6.
Helmers JH, van Leeuwen L, Zuurmond WW. Sufentanil pharmacokinetics in young adult and elderly surgical patients. Eur J Anaesthesiol. 1994;11:181–5.
Gepts E, Shafer SL, Camu F, et al. Linearity of pharmacokinetics and model estimation of sufentanil. Anesthesiology. 1995;83:1194–204.
Matteo RS, Schwartz AE, Ornstein E, Young WL, Chang WJ. Pharmacokinetics of sufentanil in the elderly surgical patient. Can J Anaesth. 1990;37:852–6.
Hofbauer R, Tesinsky P, Hammerschmidt V, et al. No reduction in the sufentanil requirement of elderly patients undergoing ventilatory support in the medical intensive care unit. Eur J Anaesthesiol. 1999;16:702–7.
Minto CF, Schnider TW, Shafer SL. The influence of age and gender on the pharmacokinetics and pharmacodynamics of remifentanil. II. Model application. Anesthesiology. 1997;86:24–33.
Shimoyama N, Shimoyama M, Elliott KJ, Inturrisi CE. d-Methadone is antinociceptive in the rat formalin test. J Pharmacol Exp Ther. 1997;283:648–52.
Davis AM, Inturrisi CE. d-Methadone blocks morphine tolerance and N-methyl-D-aspartate-induced hyperalgesia. J Pharmacol Exp Ther. 1999;289:1048–53.
Callahan RJ, Au JD, Paul M, Liu C, Yost CS. Functional inhibition by methadone of N-methyl-D-aspartate receptors expressed in Xenopus oocytes: stereospecific and subunit effects. Anesth Analg. 2004;98:653–9.
Alinejad S, Kazemi T, Zamani N, Hoffman RS, Mehrpour O. A systematic review of the cardiotoxicity of methadone. EXCLI J. 2015;14:577–600.
Lavand’Homme P, De Kock M. Practical guidelines on the postoperative use of patient-controlled analgesia in the elderly. Drugs Aging. 1998;13:9–16.
Macintyre PE, Jarvis DA. Age is the best predictor of postoperative morphine requirements. Pain. 1996;64:357–64.
Gagliese L, Jackson M, Ritvo P, Wowk A, Katz J. Age is not an impediment to effective use of patient-controlled analgesia by surgical patients. Anesthesiology. 2000;93:601–10.
Woodhouse A, Mather LE. The influence of age upon opioid analgesic use in the patient-controlled analgesia environment. Anaesthesia. 1997;52:949–55.
Ready LB. PCA is effective for older patients, but are there limits? Anesthesiology. 2000;93:597–8.
Beattie WS, Warriner CB, Etches R, et al. The addition of continuous intravenous infusion of ketorolac to a patient-controlled analgetic morphine regime reduced postoperative myocardial ischemia in patients undergoing elective total hip or knee arthroplasty. Anesth Analg. 1997;84:715–22.
Malmberg AB, Yaksh TL. Pharmacology of the spinal action of ketorolac, morphine, ST-91, U50488H, and L-PIA on the formalin test and an isobolographic analysis of the NSAID interaction. Anesthesiology. 1993;79:270–81.
Lashbrook JM, Ossipov MH, Hunter JC, Raffa RB, Tallarida RJ, Porreca F. Synergistic antiallodynic effects of spinal morphine with ketorolac and selective COX and COX2-inhibitors in nerve-injured rats. Pain. 1999;82:65–72.
Gloth FM. Pain management in older adults: prevention and treatment. J Am Geriatr Soc. 2001;49:188–99.
Wilder-Smith OH. Opioid use in the elderly. Eur J Pain. 2005;9:137–40.
Taguchi A, Sharma N, Saleem RM, et al. Selective postoperative inhibition of gastrointestinal opioid receptors. N Engl J Med. 2001;345:935–40.
Kurz A, Sessler DI. Opioid-induced bowel dysfunction: pathophysiology and potential new therapies. Drugs. 2003;63:649–71.
Nieuwenhuijs DJ, Olofsen E, Romberg RR, et al. Response surface modeling of remifentanil-propofol interaction on cardiorespiratory control and bispectral index. Anesthesiology. 2003;98:312–22.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2018 Springer International Publishing AG
About this chapter

Cite this chapter
Whitener, S., McEvoy, M.D., Shafer, S.L., Flood, P. (2018). The Pharmacology of Intravenous Opioids. In: Reves, J., Barnett, S., McSwain, J., Rooke, G. (eds) Geriatric Anesthesiology. Springer, Cham. https://doi.org/10.1007/978-3-319-66878-9_18
Download citation
DOI: https://doi.org/10.1007/978-3-319-66878-9_18
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-66877-2
Online ISBN: 978-3-319-66878-9
eBook Packages: MedicineMedicine (R0)