
Abstract
The past decade witnessed a rapid introduction of new anticoagulation agents to prevent and treat venous thromboembolism (VTE). The use of heparin and warfarin had been the standard practice, although new classes of drugs which directly target the enzymatic activity of thrombin and factor Xa have become more popular. Achieving higher levels of specificity and predictability and better patient compliance were the aims of most recent developments in anticoagulation agents to meet the needs of a wider population. This chapter discusses the clinical and practical use of both parenteral and oral anticoagulants and their risks and benefits particularly for managing VTE.
Access provided by CONRICYT-eBooks. Download chapter PDF
Similar content being viewed by others


Keywords
- Anticoagulants
- Heparin
- Warfarin
- Parenteral direct thrombin inhibitors
- Direct oral anticoagulants
- Dabigatran
- Apixaban
- Rivaroxaban
- Edoxaban
-
1.
Direct oral anticoagulants are the current standard of care for treatment of VTE and are increasingly being used instead of vitamin K antagonists.
-
2.
Direct oral inhibitors of factor Xa have less bleeding complication compared to coumadin.
-
3.
Idarucizumab, ciraparantag, and andexanet alfa are specific antidotes that are undergoing clinical trials and could potentially make the use of direct oral anticoagulants safer.
Introduction
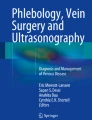
Hemostasis consists of a series of reactions that lead to the formation of fibrin and generation of an insoluble clot that strengthens the plug of platelets that halts the bleeding [1]. This process involves complex mechanisms at the cellular level (platelets) and the protein level (coagulation factors). The coagulation cascade is divided into the intrinsic, extrinsic, and the common pathways. The end product of this cascade activates thrombin which converts fibrinogen to fibrin (Fig. 21.1) [1]. Anticoagulation agents are the mainstay of prophylaxis and treatment of venous thromboembolism (VTE) . The various anticoagulation agents affect hemostasis by targeting different factors of the cascade. They typically prevent formation of new clot, its propagation, and embolization. Unlike thrombolytic agents which are administered to break down the thrombus by activating plasmin, anticoagulation agents achieve various levels of delayed thrombus resolution by allowing the innate lysis mechanisms to function. This chapter gives an overview of the anticoagulation agents and is divided based on the route of administration parenteral vs oral (Table 21.1).

Schematic view of the coagulation cascade and different targets of anticoagulant agents. Direct inhibitors specifically inhibit activated target coagulation factors (red and blue arrows), while traditional anticoagulants affect several coagulation factors indirectly (HMW high molecular weight, LMWH low molecular weight heparin, UFH unfractionated heparin)
Parenteral Anticoagulants
Heparin
Heparins are large water soluble polysaccharides which mainly act through blocking the activated intrinsic pathway. Heparin is also referred to as unfractionated heparin (UFH) to differentiate it from other lower molecular weight derivatives discussed below. It acts by catalyzing the binding of antithrombin III (a serine protease inhibitor) to serine protease coagulation factors (IIa, IXa, Xa, XIa, and XIIa) which results in immediate inactivation of coagulation cascade either in vivo or in vitro [2, 3]. Heparin can be administered intravenously (IV) or subcutaneously (SC). The half-life is approximately 2 h and the metabolism is through hepatic or reticuloendothelial system . The half-life is dose dependent with higher doses having longer half-life. At higher doses, the reticuloendothelial system binding sites become saturated, and clearance by hepatic metabolism is typically slower. Its use is safe without dose adjustment in patients with renal failure.
The effect is monitored through partial thromboplastin time (PTT) or activated clotting time (ACT) measurement [4, 5]. The major advantage of UFH is its short half-life, which is especially useful in patients in whom hour-to-hour control of the intensity of anticoagulation is desired. UFH is dosed to achieve a target activated PTT of 60–80 s. The most popular nomogram uses an initial bolus of 80 U/kg, followed by an initial infusion rate of 18 U/kg/h. Heparins’ specific structure inhibits them from placental exchange and makes them drugs of choice in pregnant patients who need anticoagulation.
Heparin is commonly used for inpatient treatment of venous and arterial thromboembolism. The main side effects are bleeding and heparin-induced thrombocytopenia (HIT) , but osteoporosis and hypersensitivity have been also reported [6]. There are some important limitations in UFH use. First, it has a narrow therapeutic range window, with the risk of either bleeding or inadequate anticoagulation. This limitation was illustrated in the Enoxaparin and Thrombolysis in Reperfusion for Acute Myocardial Infarction Treatment Thrombolysis in Myocardial Infarction (ExTRACT TIMI) 25 trial [7, 8]. This randomized clinical trial enrolled 20,506 patients with myocardial infarction and showed significant decrease in the composite of death, nonfatal reinfarction, or urgent revascularization in patients treated with enoxaparin compared to UFH . This difference was thought to be due partly to low predictability of dose-response and difficulty to stay in the therapeutic zone with UFH. Guervil et al. have demonstrated that aPTT monitoring was outside the therapeutic range in 60% of the time in patients who were receiving the UFH infusion [9].
Heparin is not suited for outpatient therapy because of the absence of an oral formulation. There is also a risk for thrombus extension during heparin therapy due to low effect on activated thrombin which has bound to factor Xa or fibrin in the formed thrombus. UFH anticoagulant effects can be reversed by protamine sulfate. Usually 1 mg of protamine sulfate is used to neutralize up to 100 units of heparin. Neutralization occurs in less than 5 min after IV administration through complexing with heparin and its inactivation [10].
Low Molecular Weight Heparins
Low molecular weight heparins (LMWHs) are fragments of UFH that exhibit less binding to plasma proteins and endothelial cells. Therefore, LMWHs have a greater bioavailability, a more predictable dose-response especially with weight-based dosing, and a longer half-life. No monitoring or dose adjustment is needed unless the patient is markedly obese or has chronic kidney disease. Due to their size, they are less likely but still have a significant chance of HIT. This group has more activity against factor Xa, and their levels can be monitored more efficiently by anti-factor Xa assay rather than PTT. Protamine sulfate has limited antidote effect against LMWH. Currently available LMWHs in the USA are enoxaparin, dalteparin, and tinzaparin [11]. They are different in molecular weight and manufacturing methods. Both enoxaparin and dalteparin have been used widely in VTE and share similarity in efficacy and safety profile; however drug administration can be incommodious. After initial drug selection, it is preferable not to try using different LMWHs interchangeably, since they have a different tendency to affect factor Xa versus factor IIa (enoxaparin has approximately 50% more anti-Xa effect compared to dalteparin with similar anti-IIa effect) [12].
Fondaparinux
Fondaparinux, a selective antithrombin III-mediated anti-Xa pentasaccharide, is administered as a weight-based once-daily subcutaneous injection in a prefilled syringe. No laboratory monitoring is required routinely. In certain populations (renal impairment, pregnancy, obesity, children), monitoring can be achieved using anti-factor Xa assay which is currently the gold standard for monitoring LMWH and fondaparinux therapy [13]. Target anti-factor Xa levels may be different in each laboratory due to variability in the type of used assays and titration curves [10]. Target level of 0.25–0.35 units/mL was recommended for anti-Xa based on the study in patients with renal impairment due to bleeding complications associated with anti-Xa between 0.45 and 0.8 units/mL [14, 15]. Fondaparinux is synthesized in a laboratory and, unlike LMWH or UFH, is not derived from animal products . It does not cause heparin-induced thrombocytopenia.
Heparin-Induced Thrombocytopenia
UFH has the largest size compared to other heparins and hence most likely to cause HIT. It is a serious antibody-mediated reaction resulting from irreversible aggregation of platelets. Currently, the term HIT is used without any dividing to describe only the immune-mediated reaction [16]. It can occur in up to 5% of patients who use UFH or LMWH. Patients who develop HIT typically are noted to have more than 50% decrease in platelet count within 5–10 days after initiation of heparin without an alternative cause. They are at risk of developing a new thrombus (heparin-induced thrombocytopenia and thrombosis [HITT] ). The assumption of diagnosis of HIT requires immediate discontinuation of any heparin product and initiation of alternative anticoagulants, typically a parenteral direct thrombin inhibitor [17]. Confirmation can be reached by HIT antibody testing immunoassay (ELISA) or functional assay like serotonin release assay (SRA) [18]. HIT or HITT may be delayed and can occur up to several weeks after discontinuation of heparin [19, 20].
Direct Thrombin Inhibitors
Parenteral direct thrombin inhibitors (DTIs) block thrombin and prevent its cleaving effect on fibrinogen [21]. The drugs developed in this group are bivalirudin, argatroban, and lepirudin. Lepirudin was taken off the market in 2012. This section will focus on argatroban and bivalirudin. DTIs have no interaction with heparin platelet factor 4 (PF4) antibodies. These drugs are useful for the treatment of venous thromboembolism in the setting of HIT [22, 23]. Despite their benefits, development of this class of drugs was slower than many other classes probably due to lack of investment and research funding. One of the reasons of this disinterest is their short-term use and route of administration which results in narrow target population . On the other hand, the popularity of heparins and their high safety and efficacy profile limited the development of alternative parenteral DTIs [24]. The two main disadvantages are lack of antidote and difficulty in monitoring [25, 26]. Parenteral DTIs are also expensive and are usually reserved for patients who cannot receive heparin and LMWHs. Oral DTIs are discussed separately in this chapter.
Argatroban is commonly used for treatment of VTE in patients with HIT, whereas bivalirudin is used as an alternative to heparin in patients with acute coronary syndrome who undergo angiography and intervention [27]. Both drugs, unlike heparin, can inhibit clot-bound thrombin in addition to soluble thrombin. The relatively short half-life of parenteral DTIs necessitates precise monitoring of their level to assure effectiveness and inhibition of side effects. Bivalirudin is now commonly used in the USA as an alternative to heparin alone or heparin and GPIIb/GPIIIa inhibitor in patients with acute coronary syndrome. Compared to heparin, it has demonstrated non-inferiority effect and less major bleeding and no risk of thrombocytopenia [27].
Oral Anticoagulants
Warfarin
Until recently, the vitamin K antagonists (VKAs) were the only oral anticoagulant agents available, and warfarin remains the most commonly prescribed oral anticoagulant worldwide. The main indications of warfarin use include primary and secondary prevention of VTE, prevention of systemic embolism, and stroke in patients with mechanical heart valves and atrial fibrillation (AF) [28]. Warfarin affects coagulation cascade by interfering with γ-carboxylation of vitamin K-dependent clotting factors II, VII, IX, and X. Besides anticoagulation effect , warfarin also plays a role as a procoagulant as it acts against proteins C and S. It is readily absorbed after oral administration, reaching peak concentration within 4 h. It however has significant variability in dose-response across individuals and requires maintenance in a narrow therapeutic range of international normalized ratio (INR) of 2–3 for most indications [29, 30].
The anticoagulant effect of warfarin takes several days to take action; hence concomitant bridging with other anticoagulants such as heparin or LMWH is usually done until the INR reaches therapeutic range. Then warfarin oral administration alone can be continued. Initiation with low-dose warfarin at 5mg has been found to be superior to 10 mg in patients treated with warfarin after heart valve replacement [31, 32]. Conversely, in patients with acute venous thromboembolism, initial administration of warfarin at 10 mg allowed more rapid achievement of therapeutic INR [33]. The current guidelines however suggest initiating VKA therapy with 10 mg daily for the first 2 days followed by dosing based on INR values (Grade 2C) [30].
The patient response to warfarin varies significantly because of genetic factors, comorbidities, the use of concomitant medications, as well as dietary factors, each of which can affect its metabolism. Clinical outcome and efficacy of warfarin are highly associated with patient adherence and the time for which patient’s PT-INR values are maintained within therapeutic range [34]. According to a study by De Caterina et al., patients with an average time >70% in therapeutic range are considered to be at a low risk of a major hemorrhagic or thrombotic event [35]. Patients with a low body weight [36, 37], significant congestive heart failure, liver disease, or concurrent medications with interactions may require lower doses. However, renal clearance does not play a significant role in warfarin elimination [38].
Warfarin is often initiated in the evening, so that an INR can be obtained with morning laboratory testing, allowing time in the afternoon to obtain the results and determine the next dose. This may not be however sufficient time to determine the effect of the drug. Gage suggests that INR testing needs to be done 15 or more hours after first administration [39]. It may be thus better to administer warfarin in the afternoon, if INR testing is done the following morning. The optimal frequency of INR testing to maintain patients within therapeutic range is still unclear, as patients exhibit fluctuations of INR with diet, medications, and adherence. When therapy is just initiated, INR monitoring is done every few days until it is therapeutic. The INR is then usually obtained weekly for 1–2 weeks, to verify dosing by stability of the INR within range. Commonly, testing is then obtained biweekly for one to two times. If the INR remains stable within the therapeutic range and all else remains constant, the duration between tests can be extended to 3 monthly visits. Current guidelines recommend that the frequency of testing should be scheduled to every 12 weeks (Grade 2B) [30].
The major limitation of warfarin is the interaction with drugs and dietary restrictions. Patient education and identification of factors which may lead to over or under-anticoagulation are thus necessary [40]. When combined with low-dose aspirin , nonsteroidal anti-inflammatory drugs (NSAIDs) , or clopidogrel , the risk of bleeding is significantly increased [41, 42]. It is recommended to avoid use of these drugs except when benefit outweighs risk of bleeding [30]. Most drug interactions affecting warfarin involve inhibition of the CYP450 enzymes . Broad-spectrum antibiotics also affect vitamin K production by intestinal flora in malnourished patients with limited stores. Chronic alcohol use can decrease activity of warfarin by increasing clearance, but the presence of concomitant liver disease can potentiate its effect. Patient education is essential to develop a diet with a relatively constant level of vitamin K and to identify foods rich in vitamin K [28].
Intracranial hemorrhage is the most feared bleeding associated with warfarin therapy. In the SPORTIF III and V clinical trials, warfarin was used for prevention of stroke in non-valvular atrial fibrillation (AF) patients and showed a rate of intracranial and subdural hematomas at 0.4%, and the rate of major bleeding was 2.5% per year [43, 44]. The DURAC trial study group in 1994 for patients with VTE concluded that 75% of INR values of their study cohort (1124 patients) were ≥2.0, and 58% were in the therapeutic range. There were eight patients with recurrent VTE (1.3 in 100 patient years; 95% CI, 0.2–1.2). Seventeen hemorrhagic events were recorded (2.8/100 patient years; 95% CI, 0.8–2.2), among which two were fatal (0.3/100 patient years; 95% CI, 0–0.4) [45]. When comparing low-dose warfarin to conventional dose of warfarin, there was no significant difference in frequency of overall bleeding between the two groups (OR, 1.3; 95% CI, 0.8–2.1), and the frequency of recurrent VTE was higher in low-dose warfarin group (OR, 2.8; 95% CI, 1.1–7) [46]. However, after conventional full-dose anticoagulation therapy for 6 months, when patients were followed with low-dose warfarin compared to placebo (PREVENT), 48% risk reduction of recurrent VTE was observed (OR, 0.36; 95% CI, 0.19–0.67) with no significant difference in major bleeding episodes [47]. In a recent meta-analysis of 11 clinical trials (41,015 patients treated for both VTE and AF), safety of warfarin in “high-risk” populations was compared. A significant association with all-cause bleeding and age>75 years (RR,1.62; 95%CI, 1.28–2.05), low body weight (RR, 1.2; 95%CI, 1.03–1.4), and those with impaired renal function (RR, 1.59; 95%CI, 1.3–1.94) was noted [48]. However, its use in patients with end-stage renal disease in a meta-analysis (56,146 patients with ESRD and AF) showed no association with major bleeding (OR, 1.18; 95% CI, 0.82–1.69) or gastrointestinal bleeding (OR, 1.19; 95% CI, 0.81–1.76) [49].
Despite wide usage and sufficient data from clinical trials demonstrating efficacy for a variety of thrombotic and thromboembolic conditions , warfarin is becoming underutilized because its management is cumbersome for both patients and physicians. Besides hemorrhage, warfarin skin necrosis is the most serious adverse effect and is induced by a transient hypercoagulable state. It occurs with intake of warfarin in individuals with congenital or acquired protein C or S deficiency [50, 51]. Affected individuals develop skin lesions which begin as an erythematous macule and if left untreated progress to an indurated lesion before becoming necrotic.
The current guidelines for reversal established by the Ninth American College of Chest Physicians Conference on antithrombotic and thrombolytic therapy recommend [30]:
-
1.
For patients with INR 4.5–10 and no evidence of bleeding, lower the dose or omit one or two doses as needed, monitor more frequently, and resume therapy at a lower dose when INR is in therapeutic range. Routine use of vitamin K is not recommended (Grade 2B).
-
2.
For patients with INR >10 and no evidence of bleeding, oral vitamin K can be administered (Grade 2C).
-
3.
In patients with major bleeding and elevated INR, hold warfarin and rapid reversal of anticoagulation with four-factor prothrombin complex concentrate rather than fresh frozen plasma (Grade 2C).
-
4.
Additional use of vitamin K (5–10 mg) administered by slow IV injection rather than reversal with coagulation factors alone is recommended (Grade 2C).
Oral vitamin K can also be used for reversal, as it was found to lower the INR rapidly in asymptomatic patients who have INR above therapeutic range [52, 53].
Direct Oral Anticoagulants
Several direct oral anticoagulants (DOACs) have been developed to overcome the limitations of heparin and coumadin . Among them, the oral direct thrombin inhibitor dabigatran etexilate (Pradaxa®) and the oral direct activated factor Xa inhibitors rivaroxaban (Xarelto®), apixaban (Eliquis®), and edoxaban (Lixiana®/Savaysa®) are currently approved for anticoagulation as prophylaxis and treatment of VTE, as well as prevention of stroke and embolic events in non-valvular atrial fibrillation.
Unlike VKA which has an indirect role in inhibition of factor synthesis, DOACs directly inhibit either thrombin or factor Xa . DOACs thus have a rapid onset and offset of action. All the DOAC agents are rapidly absorbed following oral administration and have a relatively short half-life (5–17 h). Table 21.2 illustrates the pharmacokinetics of each of the DOAC agents. The disadvantages of dabigatran pharmacodynamics include low bioavailability (6%) despite the presence of prodrug etexilate to enhance its intestinal absorption, high renal clearance (85% of absorbed dose), and low metabolism (<10%, by glucuronidation). On the contrary, factor Xa inhibitors have a good oral bioavailability (>50%); lower renal clearance than dabigatran , although still significant (54–73% of absorbed dose); and high metabolism rate by mainly CYP3A4 activity (rivaroxaban), CYP3A4/CYP3A5 (apixaban), and hydrolysis (edoxaban ) [54].
Since the recent shift to DOACs, four randomized clinical trials have been conducted to study the safety and efficacy of each of these agents compared with VKA therapy [55,56,57,58,59]. The DOACs have proven to be non-inferior to VKA in patients with venous thromboembolism (VTE) [60]. The risk of bleeding with DOACS, and particularly clinically relevant bleeding including intracranial bleeding, is less with DOACs than with VKA therapy. Dabigatran , rivaroxaban , and edoxaban tend to have higher GI bleeding compared to VKA for treatment of atrial fibrillation [61,62,63]. However this has not been the case in patients treated for VTE [64]. Also, the risk of bleeding may be lower with apixaban as compared with the other DOACs [65, 66]. On the other hand, the risk that a major bleeding will be fatal appears to be no higher than VKA therapy [60, 66]. Thus, based on its less bleeding tendency and greater patient convenience while providing similar or superior efficacy, DOACs are currently recommended as first choice of drugs in patients for initial and long-term treatment of VTE in patients without cancer [67] (Table 21.3).
Many patients tend to prefer DOAC over daily subcutaneous injections. DOACs however have a shorter half-life (<24 h) compared to VKA (36–42 h). Also, the anticoagulant effect declines 12–24 h after administration. Therefore, poor patient adherence to DOAC agents may leave them unprotected against VTE [71, 72]. A high level of patient compliance with these drugs is thus a must to demonstrate their efficacy. Laboratory monitoring of DOAC may help but is currently unavailable in most centers. Thus, methods like proper patient education, regular follow-up visits with physicians, and monitoring by pharmacists are necessary [73].
Close observation for food and drug interactions is necessary when initiating treatment with the DOACs or when there is change in concomitant medications as most of the patients involved are elderly with multiple comorbidities. It has been suggested that rivaroxaban should be taken with food as there is a 39% decrease in absorption when administered without food. Also, administration of factor Xa inhibitors with P-glycoprotein, cytochrome P450 enzymes, or CYP3A4-associated drugs (azole antifungals, HIV antiproteases) is generally not recommended due to decreased activity of anticoagulation [74]. The administration of dabigatran with proton pump inhibitors decreases the absorption by 30%; however, no dose adjustment may be needed. Finally, all DOACs have pharmacodynamics correlated to antiplatelet agents and nonsteroidal anti-inflammatory drugs (NSAIDs). This is associated with increased bleeding risk and hence their combined use is discouraged.
An important advantage of DOACs is that the routine lab monitoring is not needed. This is advantageous for both patient convenience and satisfaction. However, this lack of routine monitoring could compromise assessment of anticoagulant adherence. Also, while routine monitoring is not required, physicians need to assess anticoagulation effect to make appropriate treatment decisions [75, 76]. This is especially the case in emergency trauma situations, urgent invasive procedures, major bleeding, drug overdose, renal failure, or liver failure. The activated partial thromboplastin time (aPTT) and prothrombin time (PT) are widely available tests with rapid turnaround times, but they have poor sensitivity and specificity and lack optimal dose-response relationships for monitoring DOACs. The qualitative assays can be used for monitoring but require special laboratories and thus have slower turnaround time.
The European Heart Rhythm Association (EHRA) guidelines recommend clinical assessment and non-coagulation monitoring every 1–6 months for patients taking DOACs but do not recommend any monitoring of coagulation assays [77]. The American College of Chest Physicians has not yet made a recommendation for DOAC monitoring [67, 78].
DOAC pharmacodynamics is highly dependent on renal function. Except for apixaban , these drugs are eliminated by renal clearance. Thus, the drug dosage needs to be significantly modified in case of renal impairment leading to increased bleeding risk. On the other hand, edoxaban plasma levels may be decreased with renal impairment and result in increased risk of ischemic stroke compared to warfarin [55]. Hence, creatinine clearance (CrCl) is an important measure which must be tested at initiation of treatment and at regular intervals afterward. Liver function test is another important parameter that requires frequent monitoring (Table 21.4).
Lack of availability of specific antidotes was one of the major drawbacks for DOACs initially. Recently, highly specific antidote such as idarucizumab, a humanized monoclonal antibody fragment that selectively binds dabigatran, has been approved in 2015 for clinical use in patients with fatal or uncontrolled bleeding. Idarucizumab also is useful for preprocedural anticoagulation management of dabigatran-treated patients as it provides rapid and sustainable reversibility within minutes [83]. The clinical safety and efficacy of idarucizumab are currently being studied in a Phase 3 of a trial enrolling 500 patients. Andexanet alfa is an inactive, recombinant factor Xa agent that binds factor Xa inhibitors, and ciraparantag is a synthetic agent designed to bind fractionated/unfractionated heparins and the currently used DOACs. Currently in Phase 2 clinical trials, ciraparantag (PER977) has demonstrated that a single bolus intravenous injection produces complete and sustained reversal (for 24 h) of edoxaban , 10–30 min after administration [84].
Also as all DOACs are renally excreted, adequate diuresis is another essential step in the management of drug overdose. As protein binding is low with dabigatran , hemodialysis can remove 50–60% of circulating drug. On the contrary, factor Xa inhibitors have high protein binding efficacy and hence dialysis may not help. In case of serious bleeding in a critical organ (intracerebral bleed), there is some evidence to support the role of activated prothrombin complex concentrate (aPCC) of 30–50 U/kg or nonactivated PCC at 50 U/kg to reverse anticoagulation [85]. However, with the recent development of specific reversal agents, the bleeding risk can be brought down further.
Switching Between Anticoagulants
An appropriate INR (≥2) is necessary when switching from DOACs to VKA. It may take 5–10 days before this INR in therapeutic range is obtained. Therefore, they need to be administered concomitantly before complete switching. Close monitoring during the first months is thus recommended. When switching from VKA to DOAC, VKA should be discontinued and DOAC started when INR ≤2.5 [77].
When switching from a parenteral anticoagulant to DOAC, discontinue the parenteral and start DOAC 0–2 h before the next scheduled dose of parenteral LMWH. For transition from DOAC to parenteral anticoagulant, the first dose of parenteral is recommended at the time of next dose of DOAC intake.
Patients Undergoing Surgery or Other Invasive Procedures
Approximately 20–25% patients on DOAC require temporary cessation of anticoagulation for surgery or intervention [86, 87] (Table 21.5).
-
1.
For procedures with low-risk bleeding in patients with normal renal function, it is recommended to discontinue DOACs at least 24 h before elective procedure [85].
-
2.
For procedures with high-risk bleeding and normal renal function, discontinue DOAC at least 48 h before elective procedure.
-
3.
In patients with impaired renal function, the interval needs to increase and is 24 to >48 h in low risk and 48 to >96 h in high risk.
DOACs can be resumed 6–8 h after procedures with immediate and complete hemostasis. Safety of anticoagulation with DOACs was improved; however, the efficacy remained the same when an appropriate first dose of anticoagulation is given after at least 6 h of surgery [88].
Ongoing Trials and Future Directions
The current recommendations stated above are not based on high-quality (Grade 1A) evidence. This highlights the importance for further research to guide VTE treatment decision and choice of anticoagulation. Upcoming clinical trials including VERDICT comparing apixaban with current standard therapy and RAMBLE trial comparing apixaban with rivaroxaban in VTE will further enhance our understanding and help with decision-making.
Several other anticoagulants are currently under development including factor VIII inhibitors, factor IXa inhibitors, factor XI inhibitors, factor XIIa inhibitors, thrombomodulin, polyphosphate inhibitors, protein disulfide isomerase inhibitors, and protease-activated receptor-1 antagonists.
Also, clinical development for additional anti-factor Xa-specific anticoagulant reversal agents is ongoing and may help take care of the main disadvantage of DOACs. Also, their role in the management of emergency bleeding situations and invasive procedures may become better defined. Continued better understanding of platelet aggregation and coagulation pathway of blood continues, and this knowledge can help enhance the search for better targets and safer, highly potent drug individualized for patient use.
References
Davie EW, Fujikawa K, Kisiel W. The coagulation cascade: initiation, maintenance, and regulation. Biochemistry. 1991;30(43):10363–70.
Chuang YJ, et al. Heparin enhances the specificity of antithrombin for thrombin and factor Xa independent of the reactive center loop sequence. Evidence for an exosite determinant of factor Xa specificity in heparin-activated antithrombin. J Biol Chem. 2001;276(18):14961–71.
Stead N, Kaplan AP, Rosenberg RD. Inhibition of activated factor XII by antithrombin-heparin cofactor. J Biol Chem. 1976;251(21):6481–8.
Spinler SA, et al. Anticoagulation monitoring part 2: unfractionated heparin and low-molecular-weight heparin. Ann Pharmacother. 2005;39(7–8):1275–85.
Vandiver JW, Vondracek TG. Antifactor Xa levels versus activated partial thromboplastin time for monitoring unfractionated heparin. Pharmacotherapy. 2012;32(6):546–58.
Nelson-Piercy C. Hazards of heparin: allergy, heparin-induced thrombocytopenia and osteoporosis. Baillieres Clin Obstet Gynaecol. 1997;11(3):489–509.
Gabriel RS, White HD. ExTRACT-TIMI 25 trial: clarifying the role of enoxaparin in patients with ST-elevation myocardial infarction receiving fibrinolysis. Expert Rev Cardiovasc Ther. 2007;5(5):851–7.
Antman EM, et al. Enoxaparin versus unfractionated heparin with fibrinolysis for ST-elevation myocardial infarction. N Engl J Med. 2006;354(14):1477–88.
Guervil DJ, et al. Activated partial thromboplastin time versus antifactor Xa heparin assay in monitoring unfractionated heparin by continuous intravenous infusion. Ann Pharmacother. 2011;45(7–8):861–8.
Protamine sulfate monograph for professionals; 2017. http://www.Drugs.com.
Research, C.f.D.E.a., Postmarket drug safety information for patients and providers – generic enoxaparin questions and answers; 2017.
Hale G, Brenner M. Risks and benefits of low molecular-weight heparin and target-specific oral anticoagulant use for thromboprophylaxis in medically ill patients. Am J Cardiovasc Drugs. 2015;15(5):311–22.
Babin JL, Traylor KL, Witt DM. Laboratory monitoring of low-molecular-weight heparin and fondaparinux. Semin Thromb Hemost. 2017;43(3):261–9.
Jeffrey RF, et al. Anticoagulation with low molecular weight heparin (Fragmin) during continuous hemodialysis in the intensive care unit. Artif Organs. 1993;17(8):717–20.
Clinical use of coagulation tests – UpToDate; 2017. https://www.uptodate.com/contents/clinical-use-of-coagulation-tests?source=see_link§ionName=Anti-factor%20Xa%20activity&anchor=H2326381811#H2326381811.
Kelton JG, Warkentin TE. Heparin-induced thrombocytopenia: a historical perspective. Blood. 2008;112(7):2607–16.
Clinical presentation and diagnosis of heparin-induced thrombocytopenia – UpToDate; 2017. https://www.uptodate.com/contents/clinical-presentation-and-diagnosis-of-heparin-induced-thrombocytopenia.
Guarino ML, et al. New platelet functional method for identification of pathogenic antibodies in HIT patients. Platelets. 2017:1–3.
Warkentin TE. Platelet count monitoring and laboratory testing for heparin-induced thrombocytopenia. Arch Pathol Lab Med. 2002;126(11):1415–23.
Dager WE, et al. Heparin-induced thrombocytopenia: treatment options and special considerations. Pharmacotherapy. 2007;27(4):564–87.
Clarke RJ, et al. Combined administration of aspirin and a specific thrombin inhibitor in man. Circulation. 1991;83(5):1510–8.
Tardy-Poncet B, et al. Argatroban in the management of heparin-induced thrombocytopenia: a multicenter clinical trial. Crit Care. 2015;19:396.
Ginsberg JS, et al. Effects on thrombin generation of single injections of Hirulog in patients with calf vein thrombosis. Thromb Haemost. 1994;72(4):523–5.
van Es N, et al. New developments in parenteral anticoagulation for arterial and venous thromboembolism. Best Pract Res Clin Haematol. 2013;26(2):203–13.
Warkentin TE, Greinacher A, Koster A. Bivalirudin. Thromb Haemost. 2008;99(5):830–9.
Jabr K, et al. Plasma-modified ACT can be used to monitor bivalirudin (Angiomax) anticoagulation for on-pump cardiopulmonary bypass surgery in a patient with heparin-induced thrombocytopenia. J Extra Corpor Technol. 2004;36(2):174–7.
Coppens M, et al. Translational success stories: development of direct thrombin inhibitors. Circ Res. 2012;111(7):920–9.
Ansell J, et al. The pharmacology and management of the vitamin K antagonists: the Seventh ACCP conference on antithrombotic and thrombolytic therapy. Chest. 2004;126(3 Suppl):204s–33s.
Rubin TA, Murdoch M, Nelson DB. Acute GI bleeding in the setting of supratherapeutic international normalized ratio in patients taking warfarin: endoscopic diagnosis, clinical management, and outcomes. Gastrointest Endosc. 2003;58(3):369–73.
Guyatt GH, et al. Executive summary: antithrombotic therapy and prevention of thrombosis, 9th ed: American College of Chest Physicians evidence-based clinical practice guidelines. Chest. 2012;141(2 Suppl):7s–47s.
Crowther MA, et al. A randomized trial comparing 5-mg and 10-mg warfarin loading doses. Arch Intern Med. 1999;159(1):46–8.
Harrison L, et al. Comparison of 5-mg and 10-mg loading doses in initiation of warfarin therapy. Ann Intern Med. 1997;126(2):133–6.
Kovacs MJ, et al. Comparison of 10-mg and 5-mg warfarin initiation nomograms together with low-molecular-weight heparin for outpatient treatment of acute venous thromboembolism. A randomized, double-blind, controlled trial. Ann Intern Med. 2003;138(9):714–9.
Wallentin L, et al. Efficacy and safety of dabigatran compared with warfarin at different levels of international normalised ratio control for stroke prevention in atrial fibrillation: an analysis of the RE-LY trial. Lancet. 2010;376(9745):975–83.
De Caterina R, et al. New oral anticoagulants in atrial fibrillation and acute coronary syndromes: ESC working group on thrombosis – task force on anticoagulants in heart disease position paper. J Am Coll Cardiol. 2012;59(16):1413–25.
Hart R, et al. Impact of body mass index and genetics on warfarin major bleeding outcomes in a community setting. Am J Med. 2017;130(2):222–8.
Mueller JA, et al. Warfarin dosing and body mass index. Ann Pharmacother. 2014;48(5):584–8.
January CT, et al. 2014 AHA/ACC/HRS guideline for the management of patients with atrial fibrillation: a report of the American College of Cardiology/American Heart Association task force on practice guidelines and the Heart Rhythm Society. J Am Coll Cardiol. 2014;64(21):e1–76.
Gage BF, Fihn SD, White RH. Warfarin therapy for an octogenarian who has atrial fibrillation. Ann Intern Med. 2001;134(6):465–74.
Marcucci M, et al. Prophylaxis of venous thromboembolism in elderly patients with multimorbidity. Intern Emerg Med. 2013;8(6):509–20.
Hallas J, et al. Use of single and combined antithrombotic therapy and risk of serious upper gastrointestinal bleeding: population based case-control study. Br Med J. 2006;333(7571):726–8.
Hansen ML, et al. Risk of bleeding with single, dual, or triple therapy with warfarin, aspirin, and clopidogrel in patients with atrial fibrillation. Arch Intern Med. 2010;170(16):1433–41.
Albers GW, et al. Ximelagatran vs warfarin for stroke prevention in patients with nonvalvular atrial fibrillation: a randomized trial. JAMA. 2005;293(6):690–8.
Olsson SB. Stroke prevention with the oral direct thrombin inhibitor ximelagatran compared with warfarin in patients with non-valvular atrial fibrillation (SPORTIF III): randomised controlled trial. Lancet. 2003;362(9397):1691–8.
Schulman S. Quality of oral anticoagulant control and treatment in Sweden. Duration of anticoagulation (DURAC) trial study group. J Intern Med. 1994;236(2):143–52.
Kearon C, et al. Comparison of low-intensity warfarin therapy with conventional-intensity warfarin therapy for long-term prevention of recurrent venous thromboembolism. N Engl J Med. 2003;349(7):631–9.
Ridker PM, et al. Long-term, low-intensity warfarin therapy for the prevention of recurrent venous thromboembolism. N Engl J Med. 2003;348(15):1425–34.
Di Minno MN, Ambrosino P, Dentali F. Safety of warfarin in “high-risk” populations: a meta-analysis of randomized and controlled trials. Thromb Res. 2017;150:1–7.
Tan J, et al. Warfarin use and stroke, bleeding and mortality risk in patients with end stage renal disease and atrial fibrillation: a systematic review and meta-analysis. BMC Nephrol. 2016;17(1):157.
Conway EM, et al. Suppression of hemostatic system activation by oral anticoagulants in the blood of patients with thrombotic diatheses. J Clin Invest. 1987;80(6):1535–44.
McGehee WG, et al. Coumarin necrosis associated with hereditary protein C deficiency. Ann Intern Med. 1984;101(1):59–60.
Crowther MA, et al. Oral vitamin K produces a normal INR within 24 hours of its administration in most patients discontinuing warfarin. Haematologica. 2005;90(1):137–9.
Crowther MA, et al. Oral vitamin K lowers the international normalized ratio more rapidly than subcutaneous vitamin K in the treatment of warfarin-associated coagulopathy. A randomized, controlled trial. Ann Intern Med. 2002;137(4):251–4.
Gomez-Outes A, et al. Direct-acting oral anticoagulants: pharmacology, indications, management, and future perspectives. Eur J Haematol. 2015;95(5):389–404.
Buller HR, et al. Edoxaban versus warfarin for the treatment of symptomatic venous thromboembolism. N Engl J Med. 2013;369(15):1406–15.
Buller HR, et al. Oral rivaroxaban for the treatment of symptomatic pulmonary embolism. N Engl J Med. 2012;366(14):1287–97.
Bauersachs RM, et al. Rivaroxaban versus enoxaparin/vitamin K antagonist therapy in patients with venous thromboembolism and renal impairment. Thromb J. 2014;12:25.
Agnelli G, et al. Oral apixaban for the treatment of acute venous thromboembolism. N Engl J Med. 2013;369(9):799–808.
Schulman S, et al. Dabigatran versus warfarin in the treatment of acute venous thromboembolism. N Engl J Med. 2009;361(24):2342–52.
Castellucci LA, et al. Clinical and safety outcomes associated with treatment of acute venous thromboembolism: a systematic review and meta-analysis. JAMA. 2014;312(11):1122–35.
Jones WS, et al. Efficacy and safety of rivaroxaban compared with warfarin in patients with peripheral artery disease and non-valvular atrial fibrillation: insights from ROCKET AF. Eur Heart J. 2014;35(4):242–9.
Giugliano RP, et al. Edoxaban versus warfarin in patients with atrial fibrillation. N Engl J Med. 2013;369(22):2093–104.
Holster IL, et al. New oral anticoagulants increase risk for gastrointestinal bleeding: a systematic review and meta-analysis. Gastroenterology. 2013;145(1):105.e15–12.e15.
Abraham NS, et al. Comparative risk of gastrointestinal bleeding with dabigatran, rivaroxaban, and warfarin: population based cohort study. BMJ. 2015;350:h1857.
Touma L, et al. A meta-analysis of randomized controlled trials of the risk of bleeding with apixaban versus vitamin K antagonists. Am J Cardiol. 2015;115(4):533–41.
Mantha S, Ansell J. Indirect comparison of dabigatran, rivaroxaban, apixaban and edoxaban for the treatment of acute venous thromboembolism. J Thromb Thrombolysis. 2015;39(2):155–65.
Kearon C, et al. Antithrombotic therapy for VTE disease: CHEST guideline and expert panel report. Chest. 2016;149(2):315–52.
Schulman S, et al. Treatment of acute venous thromboembolism with dabigatran or warfarin and pooled analysis. Circulation. 2014;129(7):764–72.
Bauersachs R, et al. Oral rivaroxaban for symptomatic venous thromboembolism. N Engl J Med. 2010;363(26):2499–510.
Prins MH, et al. Oral rivaroxaban versus standard therapy for the treatment of symptomatic venous thromboembolism: a pooled analysis of the EINSTEIN-DVT and PE randomized studies. Thromb J. 2013;11(1):21.
Shore S, et al. Adherence to dabigatran therapy and longitudinal patient outcomes: insights from the veterans health administration. Am Heart J. 2014;167(6):810–7.
di Benedetto P, et al. Patient compliance with new oral anticoagulants after major orthopaedic surgery: rivaroxaban and dabigatran compared with subcutaneous injection of fondaparinux. Joints. 2016;4(4):214–21.
Shore S, et al. Site-level variation in and practices associated with dabigatran adherence. JAMA. 2015;313(14):1443–50.
Ponzetto M, et al. Risk factors for early and late mortality in hospitalized older patients: the continuing importance of functional status. J Gerontol A Biol Sci Med Sci. 2003;58(11):1049–54.
Favaloro EJ, Lippi G. Laboratory testing in the era of direct or non-vitamin K antagonist oral anticoagulants: a practical guide to measuring their activity and avoiding diagnostic errors. Semin Thromb Hemost. 2015;41(2):208–27.
Conway SE, et al. Laboratory and clinical monitoring of direct acting oral anticoagulants: what clinicians need to know. Pharmacotherapy. 2017;37(2):236–48.
Heidbuchel H, et al. Updated European Heart Rhythm Association practical guide on the use of non-vitamin K antagonist anticoagulants in patients with non-valvular atrial fibrillation. Europace. 2015;17(10):1467–507.
Ageno W, et al. Oral anticoagulant therapy: antithrombotic therapy and prevention of thrombosis, 9th ed: American College of Chest Physicians evidence-based clinical practice guidelines. Chest. 2012;141(2 Suppl):e44S–88S.
Eliquis® (apixaban) package insert. Princeton, NJ: Bristol-Myers Squibb Company; 2012. Revised 2016 Jul. 2012.
Kubitza D, et al. Effect of hepatic impairment on the pharmacokinetics and pharmacodynamics of a single dose of rivaroxaban, an oral, direct Factor Xa inhibitor. Br J Clin Pharmacol. 2013;76(1):89–98.
Ressel G. AAP updates statement for transfer of drugs and other chemicals into breast milk. American Academy of Pediatrics. Am Fam Physician. 2002;65(5):979–80.
Saouti N, et al. Left subclavian artery revascularization as part of thoracic stent grafting. Eur J Cardiothorac Surg. 2015;47(1):120–5. discussion 125
Pollack CVJ, et al. Idarucizumab for dabigatran reversal. N Engl J Med. 2015;373(6):511–20.
Ansell JE, et al. Use of PER977 to reverse the anticoagulant effect of edoxaban. N Engl J Med. 2014;371(22):2141–2.
Gogarten W, et al. Regional anaesthesia and antithrombotic agents: recommendations of the European Society of Anaesthesiology. Eur J Anaesthesiol. 2010;27(12):999–1015.
Healey JS, et al. Periprocedural bleeding and thromboembolic events with dabigatran compared with warfarin: results from the Randomized Evaluation of Long-Term Anticoagulation Therapy (RE-LY) randomized trial. Circulation. 2012;126(3):343–8.
Sherwood MW, et al. Outcomes of temporary interruption of rivaroxaban compared with warfarin in patients with nonvalvular atrial fibrillation: results from the rivaroxaban once daily, oral, direct factor Xa inhibition compared with vitamin K antagonism for prevention of stroke and embolism trial in atrial fibrillation (ROCKET AF). Circulation. 2014;129(18):1850–9.
Paikin JS, et al. Timing the first postoperative dose of anticoagulants: lessons learned from clinical trials. Chest. 2015;148(3):587–95.
Levy JH. Discontinuation and management of direct-acting anticoagulants for emergency procedures. Am J Emerg Med. 2016;34(11s):14–8.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2018 Springer International Publishing AG
About this chapter

Cite this chapter
Jorshery, S.D., Aurshina, A., Chaar, C.I.O. (2018). Overview of Anticoagulation Agents. In: Chaar, C. (eds) Current Management of Venous Diseases . Springer, Cham. https://doi.org/10.1007/978-3-319-65226-9_21
Download citation
DOI: https://doi.org/10.1007/978-3-319-65226-9_21
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-65225-2
Online ISBN: 978-3-319-65226-9
eBook Packages: MedicineMedicine (R0)