
Abstract
Prostate cancer is the second most common cancer in men worldwide. It has characteristic MR features and varying degrees of FDG uptake depending on grade. FDG PET/MR imaging is excellent at detecting pelvic lymph node involvement and distant metastases in more aggressive forms of cancer.
Access provided by CONRICYT-eBooks. Download chapter PDF
Similar content being viewed by others


Keywords
History
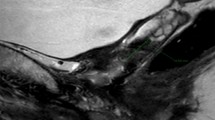
A 76-year-old male presents with gross hematuria and urinary incontinence with brachytherapy for prostate cancer 14 years ago (Fig. 86.1).

T2-weighted axial perineum (a), T1 VIBE with fat suppression post gadolinium contrast axial perineum (b), and PET/MR T2-weighted axial perineum fusion (c)
Diagnosis
Recurrent prostate cancer
Findings
-
Bulky soft tissue mass involves the prostate gland and surrounds the base of the bladder with high T2-weighted signal and post contrast enhancement.
-
Mass extends posteriorly to invade the anterior wall of the rectum (arrow).
-
Susceptibility artifacts within the prostate gland on the T1 image represent brachytherapy seeds (arrowheads).
-
PET/MR fusion images show avid FDG uptake compatible with recurrent malignancy.
Discussion
Prostate cancer is the second most common cancer in men worldwide. The use of PSA screening has increased the frequency of prostate biopsies and the diagnosis of prostate of cancer. Symptoms are nonspecific and include urinary frequency, urgency, nocturia, and hesitancy. The primary indication to perform an MRI after a biopsy-proven diagnosis of cancer is to evaluate for extracapsular extension. It may also identify suspicious areas for biopsy in a patient with an elevated PSA.
The prostate gland is comprised of the peripheral zone, central zone, and the transitional zone. The peripheral zone accounts for 70% of the prostate volume and is the most common site where adenocarcinoma arises. On T1-weighted images , the prostate gland appears homogenously medium signal intensity in all zones. With an endorectal coil, T2-weighted images of the prostate zones are well delineated but are more difficult to see with body or pelvic coils. T1-weighted images are acquired to depict post biopsy hemorrhage, tumor infiltration of the peri-prostatic fat, and metastatic disease in the pelvic lymph nodes. T2-weighted images of prostate cancer show an area of decreased signal intensity relative to the normally high signal intensity in the peripheral zone. Detection of small prostate cancer tumors is more difficult in the transitional and central zones because of normal heterogenous T2 signal. Prostate cancer may have early nodular enhancement and early washout on dynamic contrast-enhanced MR imaging. Diffusion-weighted imaging is usually useful since prostate cancer often shows restricted diffusion.
FDG PET imaging has limited value in the assessment of low grade or early prostate cancer. The degree of uptake in the prostate gland can vary both by age and individually. Early prostate cancer may have only mild relative increased uptake and false-positive findings include benign prostatic hyperplasia and prostatitis. FDG PET imaging is very useful at detecting pelvic lymph node involvement and distant metastases in more aggressive forms of cancer. Accurate registration of PET/MR would allow better detection of invasive prostatic cancer. The use of newer PET agents such as C-11 and F-18 labeled amino acids, and Ga-68 and F-18 labeled PSMA (prostate-specific membrane antigen) ligands offers superior prostate cancer evaluation including initial staging and detection of recurrent disease.
Suggested Reading
Hricak H, Choyke PL, Eberhardt SC, Leibel SA, Scardino PT. Imaging prostate cancer: a multidisciplinary perspective. Radiology. 2007;243(1):28–53.
de Perrot T, Rager O, Scheffler M. Potential of hybrid 18F-fluorocholine PET/MRI for prostate cancer imaging. Eur J Nucl Med Mol Imaging. 2014;41(9):1744–55.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Copyright information
© 2018 Springer International Publishing AG
About this chapter

Cite this chapter
Gupta, R. (2018). Prostate Cancer. In: PET/MR Imaging . Springer, Cham. https://doi.org/10.1007/978-3-319-65106-4_86
Download citation
DOI: https://doi.org/10.1007/978-3-319-65106-4_86
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-65105-7
Online ISBN: 978-3-319-65106-4
eBook Packages: MedicineMedicine (R0)