
Abstract
Introduction: The umbilical scar is undoubtedly the only scar that is accepted as a natural aspect of the human body. Changes made to its appearance, position, or even the lack of a belly button is seen as a distortion on the beholder, bringing about many repercussions.
Surgical Technique: For more than 50 years, the author has implemented this technique on a countless number of patients.
The release of the umbilical pedicle from the abdominal skin flap has been, to date, performed by making a circular incision, with a skin island of 1 cm diameter and the dissection of the pedicle down to the base. Four cardinal points transfix the edge of the periumbilical skin incision and separate stitches of 5.0 nylon are applied between the cardinal points to better adjust the scarring.
The neo-umbilicoplasty technique is ideal for specific cases of navel necrosis and other problems involving navel morphology and unnatural appearances (e.g., misplacements and/or discomfort of their carriers).
Conclusion: The umbilicus is the most remarkable aspect of the abdomen and this is why an exceptional effort must be made to achieve an aesthetically pleasing result. When performing an umbilicoplasty, we can encounter all kinds of unaesthetic cases and this is why it is necessary to address each one of them with a specific solution.
†Deceased
Access provided by CONRICYT-eBooks. Download chapter PDF
Similar content being viewed by others


Keywords
Introduction
The umbilical scar is undoubtedly the only scar that is accepted as a natural aspect of the human body. Changes to its appearance or position, or even the lack of one, are seen as a distortion by the beholder, bringing about many repercussions [1,2,3,4].
The umbilicus is positioned on the xifo-pubic median line, 20 cm above the vulvar commissure in women and the same distance from the base of the penis in men. Morphological alterations due to large variations in weight, celiotomies, aging, and pregnancy affect the abdominal wall, and this causes umbilical dimorphism. Psychological reactions also differ, from adaptation to the new umbilicus to the insistent pursuit to obtain the perfect umbilicus (more frequently seen later in the aging process, after weight changes in both genders, and in women who have given birth multiple times [5,6,7,8]).
Another situation of equal importance is related to the umbilical scar left after an abdominoplasty. This new umbilical scar can sometimes be far from what is considered natural, causing patients to react in many ways, ranging from acceptance to rejection. This rejection often results in the patient seeking surgical revision (Fig. 1a–d).

(a–d) Illustrations of unnatural navels after abdominoplasty performed by different plastic surgeons. This demonstrates the importance of the navel on the abdomen
Many years ago, we recorded a case in our clinic with a patient candidate for abdominoplasty. She emphasized how important the appearance of her navel was to her and let us know she was afraid the operation would change its morphology. During a party, knowing that several friends who underwent abdominoplasty would attend, many of which had been operated on by different surgeons (two of whom had been operated on by us), she took them into a private room for them to show her the results of their operations and to inquire in particular about the appearance of the navel. Satisfied by the results shown by her friends, she returned to us and we successfully operated on this patient. Literature describes numerous techniques on umbilicus and neo-umbilicoplasties, and this proves human inventiveness in this field [9,10,11,12].
Surgical Technique
Markings are carried out (Fig. 2) and the patient is placed under the same operative conditions for abdominoplasty. A low transversal incision of the “bicycle handlebar” type is performed and a subcutaneous dissection up to the umbilical line is carried out. The release of the umbilical pedicle from the abdominal skin wall is performed by making a circular incision, with a skin island of 1 cm diameter and the dissection of the pedicle down to the base. The undermining of the subcutaneous tissue on the epigastric abdominal wall reaches close to the sternal notch, leaving the dissected section with a triangular appearance. The plication of the aponeurosis of the rectus muscles throughout the dissected length, including the umbilical pedicle, is made by positioning the attached island of skin to the aponeurosis muscle plane. The umbilical pedicle is clamped with Kocher pliers. In special cases where abdominoplasty is combined with other intra-cavity procedures (e.g., gynecologic surgery), treatment of the rectus muscles can be diverse. The aponeurosis of these muscles is dissected bilaterally. The muscles are sutured in the middle line and the superposed aponeurosis are sutured to each other while crossed by the umbilical pedicle (Fig. 3a–d).

Schematic version of the “bicycle handlebars” demarcation of the abdomen begins with the XX′ line over the vulvar xiphoid-commissure axis. Two lines (transversal and parallel) are displayed: the lower one crossing the pubis at 7 cm from the frontal vulvar commissure and the other crossing the upper pole of the navel. From each antero-superior iliac spine, an arched line reaches the upper pole of the navel. From the end of the transversal pubic line, two other lines (vertical and parallel to each other) cross both the arched line coming from the anterior superior iliac spine and the horizontal line located in the upper pole of the navel. Marks such as 1–3–5 = 2–4–6 are created to guide the bilateral symmetry before and after the excess skin resection. Often these references may be erased during surgery, so it is suggested to apply a single stitch on each mark

(a) Dissection of the aponeurosis, exposure of abdominal rectus muscles, and the umbilical pedicle with the skin island in the far end. (b) Suture of the rectus in the midline. (c, d). Superimposed suture of the rectus husks, transfixed by the navel making it exposed to then be positioned on the skin
Next, the patient is positioned with a moderately elevated upper body. Traction flow and median incision of the abdominal skin flap are performed in a cranial direction up to the resection limit, surpassing the primary position of the navel, and a fixation point on the flap is applied over the median pubis line. Two new bilaterally-positioned incisions are made on the skin flap through to the limits of the skin excesses to then be resected. Four abdomen skin flap excesses are resected. The end of the Kocher pliers trapped at the base of the umbilical pedicle is manipulated against the dissected skin, indicating the exit point of the umbilical pedicle (Fig. 4a–h).

(a, b) The navel is dissected with the pedicle exposed. The island of skin (1 cm in diameter) at the extremity, before and after the plication of the aponeurosis of the rectus abdominal muscles, remains at this level. (c) The abdominal skin flap is sutured with two points at the pubis limit after excess skin resection, while Kocher pliers fixate the navel pedicle. (d) A transversal and transfixing skin incision of 2 cm in length is projected towards the belly button skin island. (e, f). The skin flap is everted and the fat tissue is resected around the perimetral umbilical skin incision. (g, h) The umbilical pedicle is dissected after plication of the rectus muscles, with the island of skin at the free end positioned level with the muscular wall. Kocher pliers (see Fig. 3c) clenched to the pedicle base, guide the transversal incision to be made for the final umbilicus position on the abdominal wall. When bound, it determines the skin umbilication. Additional isolated stitches of 5.0 complement the sutures
A transverse skin incision trans-fixating 2–2.5 cm is performed, depending on the thickness of the skin layer of the abdominal flap. The guiding stitch marks on the abdominal skin flap are removed and everted.
The excess adipose from 3–4 cm around the umbilical incision is resected depending on the final thickness of the skin flap. All supraumbilical segments of the abdominal skin flap receive binding stitches a few centimeters above the navel pedicle. Four cardinal points transfix the edge of the periumbilical skin incision, and then the aponeurosis, the navel base, and the skin edge at the free end of the umbilical pedicle emerge through the skin incision and are united and bound by hemostatic pliers.
Following this, adhesion stitches are sewn throughout the hypogastrium, down to the edge of the inguinal-pubis incision. When tied, the four cardinal points resemble the natural effect of the navel. Separate stitches of 5.0 nylon are applied between the cardinal points to better adjust the scarring. The four cardinal points are tied onto a spherical gauze pack with antibiotic ointment. These points remain in position for about 7 days post-operation. After this period, the gauze is removed and the wound is cleaned twice daily. The 5.0 nylon stitches are removed after 2 weeks and the cardinal points are removed after the third week.
Neo-umbilicoplasty
The neo-umbilicoplasty technique is used for specific cases of navel necrosis and other problems involving its morphology and natural appearance. These problematic navels can be caused by previous abdominoplasty, celiotomies where the final scar compromises the natural aspect of the navel, skin changes from excessive body weight, previous surgery, excessive weight loss, etc. (Fig. 5a–d).

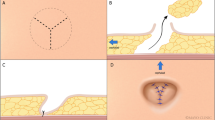
Trans- and post-operative neo-umbilicoplasty. (a, b) Umbilical orifice before and after fixation of the edges with the four repair stitches for attachment to the aponeurosis of the rectus muscles. (c) Healing patch covering the area of the neo-umbilicus, edges sutured and fixated by four cardinal and intermediate points. (d) Six months post-operative photograph
This technique involves surgically removing the affected area and replenishing the natural aspect of the navel. There are no recorded cases of umbilical hernias, except for those patients with cosmetic problems. In other words, all the skin within the affected navel area down to the scar limits is resected to the aponeurotic plane below.
The free edge of the skin is sutured to the aponeurosis with two or four separate cardinal stitches of 4–0 nylon thread, keeping each stitch at approximately 10–12 cm in length. Between these stitches, isolated 5–0 stitches are made around the central open area. Gauze drenched in antibiotic ointment and formed into a ball shape is tied with four long nylon threads, compressing the open area for approximately 10 days. The patients are advised not to wet the region during this period. The healing patch is removed after this duration, continuing with daily local cleansing and application of antibiotic ointment. The average time of re-epithelialization is approximately 30 days starting from the periphery into the center of the neo-umbilicus.
Conclusion
The umbilicus is the most remarkable aspect of the abdomen and this is why an exceptional effort must be made to achieve an aesthetically pleasing result. When performing umbilicoplasty, we can encounter all kinds of unaesthetic cases and this is why it is necessary to address each one of them with a specific solution. Among these unaesthetic cases, we can find stenosis (Figs. 6 and 7), enlarged umbilical size, flat aspect of the navel, necrosis of the umbilical stalk, and widening of the scar over-stepping the umbilical area. For each situation, it is necessary to address a specific solution. In that regard, necrosis of the stalk is treated by means of neo-umbilicoplasty, resecting through the former scar or umbilicus remnant. The fat below the new hole in the abdominal flap is resected and borders of approximately 2 cm diameter. are stitched to the aponeurosis. The raw area is left to heal by second intention, which occurs in about 4 weeks. When the problem is malposition, the umbilicus is relocated to its normal position, fixing it to the fascia and redoing the suture joining the skin island to the free stalk.

(a–d) If navel scar stenosis allows a simpler solution, resecting the scar ring keeps the umbilical pedicle and new suture on the new edge

(a–c) Scar (from navel stenosis) was redirected to neo-umbilicoplasty by completely resecting the scar and the navel pedicle followed by suturing of the edges to bloody tissue. (d) Its final appearance was achieved after complete healing by “second intent” a year later
Bibliography
Avelar JM. Abdominoplasty. Systematization of the technique without external umbilical scar. Aesthetic Plastic Surg. 1978;2:141–51.
Avelar JM. Umbilicus: its importance and technique making the abdominoplastias (Cicatriz umbilical: da sua importância e da técnica de confecção nas abdominoplastias). Rev Bras Cir Plast. 1979;69:41–52.
Vernon S. Umbilical transposition upward and abdominal contouring in lipectomy. Am J Surg. 1957;94:490.
Baroudi R, Keppke MK, Tozzi Neto FA. Abdominoplasty. Plast Reconstr Surg. 1974;54:161.
Delerm A. Refinements in abdominoplasty with emphasis on reimplantation of the umbilicus. Plast Reconstr Surg. 1982;70:362.
Baroudi R. Umbilicoplasty. Clin Plast Surg. 1975;2:431.
Baroudi R, Carvalho CGS. Neoumbilicoplastias: un procedimento en el trasnscorso de las abdominoplastias. Clin Plast Iberolatinoamer. 1981;7:391.
Freeman BS, Weimar BS. Abdominoplasty with special attention to the construction of the umbilicus: technique and complication. Aesthetic Plast Surg. 1978;2:65.
Jamra FA. Reconstruction of the umbilicus by double V-Y procedure. Plast Reconstr Surg. 1979;63:106.
Juri J, Juri C, Raiden G. Reconstruction of the umbilicus in abdominoplasty. Plast Reconstr Surg. 1979;64:580.
Rosique MJF, Rosique RG, Lee FDI, Kawakami H, Glattstein N, Mélega JM. Estudo comparativo entre técnicas de onfaloplastia. Rev Bras Cir Plast. 2009;24(1):47–51.
Daher JC, Benedik FCADC, Lamartine JD, Amaral G, Rodrigues Neto JN, Cosac OM, Cammarota MC. Umbilicoplastia: experiência com a técnica do minicírculo de pele. Rev Bras Cir Plast. 2011;26(2):302–5.
Author information
Authors and Affiliations
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2018 Springer International Publishing AG, part of Springer Nature
About this chapter

Cite this chapter
Baroudi, R. (2018). Omphalo and Neo-Omphaloplasty. In: Murillo, W. (eds) Omphaloplasty. Springer, Cham. https://doi.org/10.1007/978-3-319-64313-7_3
Download citation
DOI: https://doi.org/10.1007/978-3-319-64313-7_3
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-64312-0
Online ISBN: 978-3-319-64313-7
eBook Packages: MedicineMedicine (R0)