
Abstract
Stroke remains the leading cause of permanent disability. Embolic stroke due to severe carotid artery stenosis can be preventable. In this article, we review the management of carotid artery disease with particular focus in cancer patients. Carotid duplex ultrasonography is the screening modality of choice for the detection of cervical carotid artery disease. Surgical carotid endarterectomy remains the gold-standard therapy for all symptomatic patients with severe carotid artery stenosis. Carotid stenting is a minimally invasive alternative treatment for symptomatic patients deemed high-risk for carotid endarterectomy either due to medical or anatomical reasons. Head and neck cancer patients require special considerations due to higher incidence of carotid artery disease, particularly following the radiation treatment.
Access provided by CONRICYT-eBooks. Download chapter PDF
Similar content being viewed by others


Keywords
- Carotid
- Ischemic stroke
- Cerebral infarction
- Atherosclerosis
- Endarterectomy
- Stenting
- Angioplasty
- Cancer
- Radiation
- Head and neck
- Stenosis
- Vascular
Introduction
The decline in stroke mortality in the United States over the past decades has been recognized as a major improvement in the medical field. The progress in stroke outcomes results from medical interventions to control cardiovascular risk factors, reduced stroke incidence, and lower case fatality rates [1]. However, stroke remains a leading cause of long-term disability globally. Approximately 70% of stroke survivors require further medical care after sustaining an acute stroke. It is estimated that 87% of all strokes are due to acute ischemic cerebral infarction, 10% to intracranial hemorrhage and 3% to subarachnoid hemorrhage. Severe carotid artery plaque disease accounts for up to 20% of acute ischemic strokes (Fig. 10.1). The incidence of ischemic stroke related to cervical carotid artery plaque disease will likely continue to rise in the next decade due to the aging of the U.S. baby boomer population. Cardiovascular complications are common in cancer patients. For the cancer patient, the occurrence of an acute stroke will often delay oncologic treatment for that patient until he/she regains adequate functional or performance status. In this article, we review the management of carotid disease with particular focus in cancer patients and provide a consortium of clinical vignettes.

Carotid plaque . Intraoperative photograph of a bisected carotid artery bifurcation, showing the atherosclerotic plaque, intramural thrombus with hemorrhage, and friable debris
Stroke Risk Factors
Older age, cigarette smoking, hypertension, diabetes, and hyperlipidemia are well-established risk factors for atherosclerotic plaque formation in the cervical carotid arteries, similar to that seen in the coronary and other medium-size arteries. Artery-to-artery atheroembolization from carotid plaque to either a large intracranial branch (e.g. middle cerebral artery) or a smaller cortical branch is recognized as the most common mechanism leading to acute cerebral ischemia (Fig. 10.2). Stroke due to acute carotid artery thrombosis is less common (Fig. 10.3). In general, patients who sustain an acute ischemic stroke due to atheroembolization from carotid artery disease are more likely to experience a recurrent stroke than those with small vessel occlusion or cardioembolism [2]. Lacunar infarcts due to small vessel disease typically result in milder neurologic impairments and are associated with better outcomes when compared to ischemic strokes due to carotid artery atheroembolism. The current management of patients with carotid artery plaque disease is primarily based on the severity of stenosis, and the presence or absence of ipsilateral ischemic neurologic symptoms (symptomatic versus asymptomatic, respectively).

Embolic ischemic stroke . Head and neck MRI/MRA of a 72 year-old man who developed acute onset of slurred speech and right arm weakness in the post-anesthetic care unit, after undergoing nasal flap revision (the nasal flap had been created to provide soft tissue coverage to a defect which resulted from the surgical resection of a cutaneous melanoma lesion 3 weeks prior). (a) Axial MRI image showed multiple scattered foci of restricted diffusion (bright signals on DWI) concentrated in the left frontal and parietal lobes, and in the left occipital and right posterior frontal lobes, consistent with multiple acute embolic infarctions. (b) 2-D reformatted TOF MRA coronal image demonstrated focal moderate to severe stenosis of the left proximal internal carotid artery (thick white arrow), a typical appearance of bifurcation atherosclerotic disease, with normal distal internal carotid artery (thin white arrow). The left vertebral artery is normal and dominant (white asterisks). The right carotid bifurcation has mild disease (thick grey arrow) and distal right internal carotid artery is normal (thin grey arrow). The right vertebral artery is hypoplastic (grey asterisk). The patient also had paroxysmal atrial fibrillation

Acute internal carotid artery thrombosis . A 70 year-old man sustained acute middle cerebral artery territory large ischemic stroke due to acute right internal carotid artery thrombosis, following repair of a femoral artery pseudoaneurysm, which occurred after extensive common femoral endarterectomy and patch angioplasty reconstruction. CT angiogram axial images revealed (a) acute thrombosis of the proximal right internal carotid artery (arrow), extending into the (b) clinoid segment of the vessel (arrow), which is also heavily calcified, and (c) reconstitution of flow in the right middle (large arrow) cerebral and anterior (small arrow) cerebral arteries via collaterals. On sagittal views, (d) extensive calcified complex plaque disease (asterisk) is seen with interruption of contrast flow just above the carotid bifurcation in the right cervical internal carotid artery (arrow), and (e) moderate stenosis of the left proximal internal carotid artery is shown (arrow). (f) Brain MRI axial T2 flair image (11 days after the acute stroke event) showed the large acute/subacute infarction involving the right middle cerebral artery territory, and smaller acute embolic infarcts in the left middle cerebral territory. The patient had received immunotherapy (nivolumab trial) for metastatic urothelial cancer for approximately 3 years without progression of cancer disease and had remote history of coronary artery bypass
Diagnostic Imaging
Carotid duplex ultrasound examination is the initial imaging modality of choice to evaluate the cervical carotid artery bifurcation for the presence of plaque disease and stenosis (Fig. 10.4). Duplex ultrasound is a non-invasive test with high sensitivity and specificity. Characterization of the carotid bifurcation plaque on gray-scale imaging provides useful information about its morphology and composition. Certain characteristics such as soft plaque (homogenous and echolucent), intraplaque hemorrhage and plaque ulceration have been associated with higher incidence of distal embolization compared to heterogenous and calcified plaques. However, the severity of luminal stenosis is still the strongest predictor of stroke risk. By convention, the determination of carotid artery stenosis is provided in ranges based on the Doppler derived flow velocities, and not by diameter measurement. The criteria recommended by the Ultrasound Consensus Panel remains the most commonly used to determine the severity of stenosis of the cervical internal carotid artery [3].

Carotid Duplex ultrasound . (a–c) Duplex carotid ultrasound of an asymptomatic 75 year-old man, 30 years after surgical neck dissection, muscle flap reconstruction and external beam radiation for oropharyngeal squamous cell cancer. Gray scale ultrasound shows a focal dissection intimal flap (arrow) in the distal common carotid artery (CCA) on (a) longitudinal and (b) axial views; the intimal flap is likely chronic and related to the remote surgery. (c) Doppler interrogation demonstrates markedly increased peak systolic velocity indicating greater than 50% stenosis of the distal common carotid artery. (d–g) Duplex carotid ultrasound of a 72 year old-man with right small glottic cancer and asymptomatic severe bilateral carotid artery stenosis. Gray scale longitudinal ultrasound images show complex plaque (asterisk) disease in the (d) right and (e) left carotid internal carotid arteries (ICA). Doppler interrogation suggests high-grade stenosis in both (f) mid right internal carotid artery and (g) proximal left internal carotid artery. The patient had 75 pack-years smoking tobacco and hypertension. Clopidogrel and atorvastatin therapy was initiated and the patient had successful definitive intensity-modulated radiation therapy (IMRT) for the glottic cancer. Patient sustained a minor myocardial infarction 2 years after radiation treatment, but has had no ischemic neurologic events
Carotid duplex scanning in the head and neck cancer patient is often challenging. Preoperatively, a large tumor mass in the neck can displace, compress or encase the cervical carotid vessels (Fig. 10.5). Soft tissue changes secondary to surgery and/or radiation treatment can limit visualization. Irradiated tissue becomes fibrotic over time, hampering transmission of the ultrasound beam and causes acoustic shadowing that can obscure segment of the carotid arteries. Removal of the sternocleidomastoid muscle with radical neck dissection eliminates an important acoustic window for a posterior approach to the already superficial location of the carotid arteries. The presence of a tracheostomy further narrows the scanning window, and in particular, view of the common carotid artery, which is often very close to the stoma, can be suboptimal.



Thyroid tumor encasing carotid artery bifurcation. (a–e) Ultrasound images of a large papillary thyroid cancer mass (asterisk) encasing and narrowing the right mid-common carotid artery (CCA) in a 52 year-old woman: (a) gray scale long view of mid-CCA encased by tumor; transverse views showing (b) normal diameter of proximal CCA and (c) reduced diameter of mid CCA; (d) disturbed colorflow seen in mid CCA associated with (e) increased Doppler peak systolic velocities, indicating luminal stenosis (due to external compression by the encasing tumor). The vessel wall including intima is otherwise normal and free of plaque disease. (f) Axial CT neck shows the large papillary thyroid cancer mass (asterisk) with extensive locoregional disease, encasing the right mid-common carotid artery (arrow). (g) Reformatted 3-D CT angiogram depicts focal narrowing (arrow) of the right common carotid artery caused by tumor encasement. (h) Intra-operative photograph shows tumor (asterisk) encasing the right common carotid artery (a) and right vagus nerve (n). (i) Following en-bloc tumor and carotid artery resection, reconstruction of the right common carotid artery (c) using reversed saphenous vein graft (vg) is shown on photograph; proximal (short arrow) and distal (long arrow) anastomoses are depicted. (j) Colorflow ultrasound image of the reconstructed right common carotid artery (vein graft) at 6 months following surgery and post-operative external radiation
The finding of a severe carotid artery stenosis (70–99%) detected on duplex ultrasound performed in an accredited vascular laboratory is generally deemed sufficient evidence for determining therapy or intervention [4]. However, further evaluation with either magnetic resonance angiography (MRA) or computed tomographic angiography (CTA) is warranted to confirm the severity of stenosis, and to assess for presence of proximal vessel disease, or tandem intracranial stenosis. Imaging technology and post-processing methods of MRA and CTA are constantly evolving. In our institution, CTA is more commonly used than MRA to evaluate patients with suspected carotid disease, in part due to the local expertise (Fig. 10.6). The multi-slice helical CT scanner provides higher spatial resolution than MR imaging. One additional advantage of CTA over MRA is better characterization of calcification. However, the diagnostic value of conventional CTA (single-energy source CT) is limited when there is extensive calcification in the carotid bifurcation, and the severity of stenosis can be either over- or under-estimated. The recent introduction of dual-energy source CT systems may potentially overcome this limitation. Analysis of tube voltage-dependent attenuation differences between iodine and calcium enables rapid and fully automated subtraction of calcification from CTA datasets by dedicated post-processing software tools. Preliminary data suggests that dual-energy CTA may become the preferred imaging modality of choice for assessing patients with severely calcified carotid artery bifurcation disease [5]. Surveillance contrast-enhanced CT of the neck soft tissue is routinely obtained in head and neck cancer survivors in the first 5 years after completion of treatment and periodically thereafter. The presence of carotid artery disease can be noted on these CT, but it is often not assessed or reported because it is not the primary reason for the test. Indeed more attention should be paid to the carotid arteries in contrast-enhanced neck CT surveillance done for head and neck cancer patients, as the incidental finding of significant carotid stenosis is not infrequent. In our institution, we are working with our neuroradiologists towards standardizing reports on contrast-enhanced CT of neck soft tissue to include a comment on the carotid arteries.

3-D reformatted CT angiogram. A sixty-three year-old man who had left tonsillar HPV-related squamous cell cancer intensity modulated radiotherapy to 66 Gy in 2009. CT surveillance showed no evidence of cancer recurrence but revealed an incidental asymptomatic severe stenosis of the proximal left internal carotid artery in 2015. Reformatted 3-D image depicts the focal high-grade stenosis (arrow) of the proximal left internal carotid artery with small caliber vessel distal to the stenosis. The patient subsequently had successful carotid endarterectomy
MRA imaging incurs no radiation risk and does not require the use of intravenous iodinated contrast. Contrast-enhanced MRA with intravenous injection of gadolinium can provide accurate assessment of the plaque, residual lumen and degree of stenosis (Fig. 10.2b) [6]. However, in patients with renal insufficiency, TOF-MRA can provide adequate evaluation of the carotid artery bifurcation without need for contrast, avoiding the risk of nephrogenic systemic fibrosis. Invasive intra-arterial carotid angiography (selective digital subtraction angiography) was the historical gold standard test for evaluating carotid artery disease. However, with the improved diagnostic accuracy of the non-invasive carotid duplex ultrasound, MRA and CTA imaging, invasive carotid angiography is currently reserved for therapeutic intervention such as carotid stenting or when there is discordance in the findings of the non-invasive imaging tests.
Medical Therapy in Stroke Prevention
There is large body of evidence to support the routine use of aspirin and statin to prevent stroke in patients who either have symptomatic atherosclerotic cardiovascular disease, or are considered high-risk [7]. Aspirin (75–325 mg daily) has been shown to be effective in preventing stroke in patients at increased risk of for cardiovascular events, including those who sustain an acute myocardial infarction or ischemic stroke, unstable or stable angina, or those with prior history of myocardial infarction, stroke, and peripheral arterial disease [8, 9]. However, in patients without known cardiovascular disease or risk factors for atherosclerosis, the benefit of aspirin therapy remains uncertain. Large clinical trials have shown significant reduction in first and recurrent incidence of stroke in high-risk patients taking statin [10, 11]. Moreover, high-risk patients with established cardiovascular disease can benefit from statin regardless of their cholesterol level. In a prospective cohort of 68 asymptomatic patients with greater than 50% carotid artery stenosis, the use of statin therapy was associated with reduced rate of carotid plaque progression on MRI [12]. The beneficial effects of statin is not directly related to lipid-lowering, but rather can be linked to pleiotropic effects which are still not well understood [13].
In oncologic patients, there can often be competing treatment goals. Antiplatelet therapy is frequently put on hold during chemotherapy regimens that are known to cause bone marrow suppression and thrombocytopenia. However, patients with prior history of coronary artery or carotid disease (with or without stenting), myocardial events, or ischemic stroke should be reminded to remain on antiplatelet therapy throughout their oncologic treatment to reduce risk of cardiovascular events unless they develop major bleeding complications. The mere bleeding potential risk related to the combination of platelet inhibition and thrombocytopenia is not a valid contra-indication to interrupt antiplatelet therapy during oncologic treatment (Fig. 10.7). On occasions, patients may be temporarily unable to take their regular medications due to side effects of the oncologic treatment. When these side effects subside, patients with the above listed cardiovascular conditions should resume their cardiovascular drugs, including statin therapy as soon as possible while completing their cancer treatment.

Acute ischemic stroke during induction chemotherapy. A sixty-two year-old man, heavy smoker with prior history of myocardial infarction and coronary stenting, sustained right hemispheric stroke while undergoing induction chemotherapy (docetaxel and carboplatin) for synchronous squamous cell cancer in floor of the mouth and oropharynx. Although the patient had been on clopidogrel, it was halted for lymph node biopsy and not resumed until he developed an acute ischemic stroke. Duplex carotid ultrasound showed (a) calcified occlusive plaque (asterisk) in the right carotid bulb and (b) no Doppler colorflow, consistent with complete occlusion of the internal carotid artery. Fortunately, the patient recovered full neurologic function, and went on to receive successful definitive chemoradiation therapy within a month after the stroke. The patient remained on clopidogrel and atorvastatin during oncologic treatment and has had no recurrent ischemic neurologic events for 2 years since the incident stroke
Surgical Carotid Endarterectomy
Surgical carotid endarterectomy (CEA) remains the gold-standard treatment for stroke prevention in patients with severe cervical carotid artery stenosis. The benefit of CEA over medical therapy alone in stroke prevention is well established for symptomatic patients with severe carotid artery disease (70–99% stenosis). The North American Symptomatic Carotid Endarterectomy Trial (NASCET) reported a cumulative stroke rate of approximately 9% for patients with severe carotid artery stenosis randomized to CEA versus 26% for patients in the medical therapy group [14]. CEA was also shown to benefit patients with moderate carotid artery stenosis (50–69%); the 5-year fatal or nonfatal ipsilateral stroke rate was 16% in the surgically treated group versus 22% in the medically treated group [15]. The European Carotid Surgery Trial (ECST) demonstrated similar findings of the efficacy of CEA in reducing recurrent stroke rate for symptomatic patients with moderate to severe carotid artery stenosis [16]. However, CEA does not reduce risk of recurrent stroke in symptomatic patients with less than 50% carotid stenosis compared to medical therapy alone [15].
The surgical techniques of carotid endarterectomy continue to be refined. There are variations in the conduct of the procedure with regard to anesthesia, neurologic monitoring, type of skin incision, endarterectomy approach, artery closure, and carotid shunting. We describe our technique briefly as follows (Fig. 10.8). We prefer general anesthesia for most patients. A dedicated neurophysiology team monitors the patient’s intra-operative electroencephalography (EEG) and somatosensory evoked potentials (SSEP). Using a portable duplex ultrasound, we visualize the carotid bifurcation to be treated and we mark its level and side. We make a curvilinear transverse incision along a skin fold centered on the diseased carotid artery bifurcation. Superior and inferior subplatysmal myocutanous flaps are created. We open the carotid fascia and mobilize the common carotid and internal carotid arteries circumferentially, proximally from below the bifurcation to as high as possible distally. Not infrequently, we divide the inferior belly of the omohyoid muscle to get adequate exposure of the lower part of the common carotid artery in the neck. This is particularly desirable when intra-arterial shunting is used. Distally, the posterior belly of the digastric muscle can be divided to expose the distal internal carotid artery. The common facial vein is commonly divided as it crosses anterior to the carotid artery. The hypoglossal and vagus nerves are always preserved. We administer heparin (1 mg/kg) intravenously prior to carotid cross-clamping. The external, internal, and common carotid arteries are sequentially clamped. A longitudinal arteriotomy is made to open the common carotid artery from below the bifurcation to distally beyond the diseased plaque onto the mid-distal internal carotid artery. We perform the endarterectomy by gently finding the normal plane within the thickened wall of the carotid plaque, removing the occlusive plaque, and leaving the outer layer (adventitia) of the vessel wall intact. Tacking sutures are placed distally using 6-0 or 7-0 Polypropylene sutures when necessary to appose the intima (and prevent an intimal flap). We carefully flush out and remove any loose debris from the endarterectomized surface. To optimize distal cerebral flow, we routinely use an intra-arterial shunt and aim to keep the systolic blood pressure 90–120 mmHg during the period when the carotid artery is opened. We typically close the longitudinal arteriotomy by sewing a commercially available pericardial bovine patch (or autologous saphenous vein patch). The temporary shunt is removed just before completion of the patch angioplasty. Flow is restored to the external carotid artery first then to the internal carotid artery. Protamine sulfate is administered to reverse effect of heparin (1:1) before wound closure. Antiplatelet therapy is resumed immediately after surgery. Patients are typically discharged home 1–2 days after carotid endarterectomy.

Surgical carotid endarterectomy (CEA) . A fifty-five year-old man had right partial glossectomy, neck dissection and postoperative external beam radiation to total dose of 60 Gy to the right tongue and 50 Gy to the right neck in 1997. The patient developed new primary cancer of the left lateral tongue at the end of year 2013 and underwent left partial glossectomy and neck dissection. Patient received additional postoperative radiation using IMRT to total of 60 Gy. The patient subsequently developed bilateral osteoradionecrosis of mandibles and worsening asymptomatic severe stenosis of the cervical right internal carotid artery in 2016. The patient underwent combined mandibulectomy, reconstruction using left fibula osteocutanous free flap, and right carotid endarterectomy. Base of the neck is to right in photographs. (a) Standard exposure of the right carotid artery bifurcation is shown. Clamps are placed across the proximal common (large arrow), external (thin arrow) and distal internal (short arrow) carotid arteries. Through the longitudinal arteriotomy, the diseased ulcerated plaque (asterisk) is seen. (b) The endarterectomized surface (black asterisk) is shown after plaque excision, with the temporary shunt (white asterisk) inside the artery. (c) Image depicts the patch angioplasty closure (asterisk) and prophylactic tracheostomy (arrow). The patient recovered well without neurologic or other postoperative complications. Patient’s tracheotomy tube was removed and patient was discharged home on post-operative day 8
Carotid Artery Stenting
The introduction of carotid artery stenting (CAS) provided a minimally invasive alternative treatment for patients with severe carotid stenosis. Endovascular techniques for CAS and the use of temporary embolic protection have continued to evolve over the last decade. There have been numerous clinical studies examining the role of CAS in carotid revascularization. SAPPHIRE (Stenting and Angioplasty with Protection in Patients at High-Risk for Endarterectomy) was the first large clinical trial that showed results of carotid stenting comparable (non-inferior) to endarterectomy [17]. However, the initial enthusiasm for CAS was hampered by subsequent publication of the French multicenter randomized controlled Endarterectomy Versus Angioplasty (EVA-3S) trial showing higher rate of disabling stroke or death with CAS than with CEA in patients with symptomatic severe carotid artery stenosis (incidence of disabling stroke or death at 30-day was 1.5% after CEA and 3.4% after CAS) [18]. Furthermore, the findings of this study suggested that the use of temporary cerebral protection devices during CAS may reduce periprocedural strokes by approximately threefold [19]. Subsequently, the long awaited results of the North American randomized Carotid Revascularization Endarterectomy versus Stenting Trial (CREST) comparing CEA versus CAS were published in 2011 [20]. CREST demonstrated that both CEA and CAS are good options for carotid revascularization because the overall complication rates for both procedures are within the range of current treatment guidelines. However, peri-procedural risk of stroke and death was significantly higher in CAS versus CEA for the subgroup of symptomatic patients (6% vs. 3.2%).
Many carotid stents and distal embolic protection devices have become commercially available since the Federal Drug Administration first approved CAS in 2004. Transfemoral approach remains the standard conventional technique (Fig. 10.9). In brief, CAS is typically performed under conscious sedation. During the procedure, the patient’s neurologic status is assessed periodically. Intra-procedure transcranial Doppler monitoring can detect intra-operative cerebral embolization and flow disturbances. Following standard arch aortogram, the external carotid artery is cannulated and a 6F or 7F sheath is advanced into the common carotid artery. Bivalirudin, a bivalent direct thrombin inhibitor, is administered intravenously as an initial bolus (0.75 mg/kg) then continued as a continuous infusion at a rate of 1.75 mg/kg/h. Distal embolic protection device (filter) is navigated carefully across the diseased plaque and deployed in the normal distal internal carotid artery. Various stent diameters and lengths are available. The self-expandable carotid stent is deployed across the target lesion. Post-stent balloon angioplasty is inflated gently and briefly. Intravenous atropine is frequently required to treat severe bradycardia or asystole, which can occur during stent deployment or balloon angioplasty. Following satisfactory completion angiogram, the temporary filter is removed, completing the procedure. Peri-procedural embolic stroke risk, in part related to crossing of the aortic arch, remains the Achilles heel of transfemoral CAS. More recently, transcarotid stenting using a novel neuroprotection device (flow reversal) has produced promising results with lower perioperative stroke risk [21]. We recommend long-term clopidogrel therapy following carotid stenting.

Carotid artery stenting (CAS) . A seventy year-old man with history of supraglottic squamous cell cancer had definitive chemoradiation in 2009. Patient developed a recurrence in 2012 in a left retropharyngeal lymph node and received additional 66 Gy proton therapy. Patient subsequently developed severe right internal carotid artery stenosis with neurologic symptoms and had carotid artery stenting in 2015. (a) At 1-year follow-up, duplex ultrasound surveillance showed severe in-stent restenosis of the right internal carotid artery with recurrent neurologic symptoms. The patient underwent successful repeat carotid stenting without complications. (b) Selective carotid arteriogram confirmed severe stenosis at the distal edge of the previous stent in the right internal carotid artery. (c) Spot fluoroscopic image depicts the tip of the sheath (asterisk), top of the new stent (still constrained within the delivery catheter; small black arrow), existing overlapping stents in the carotid artery (large white arrow denotes distal edge), and the temporary filter wire (nitinol loop-white circle; thin white arrow points to distal tip of wire). (d) Completion arteriogram after new stent deployment and post-stent balloon angioplasty demonstrates satisfactory result
Asymptomatic Carotid Artery Stenosis
In 2012, 90,800 CEA and 16,300 CAS procedures were performed in the United States. Approximately 70–80% of carotid interventions (CEA and CAS) are done for asymptomatic carotid stenosis. Controversy remains in the treatment of asymptomatic carotid artery stenosis for primary stroke prevention [22]. Two large multicenter randomized clinical trials have shown significant reduction in stroke risk for patients with severe asymptomatic carotid artery stenosis treated by CEA versus medical therapy. The North American Asymptomatic Carotid Arteriosclerosis Study (ACAS) was published in 1998 and showed that the 5-year risk for any perioperative stroke or death was 5.1% for CEA patients and 11.0% for patients treated medically [23]. Subsequently, the European Asymptomatic Carotid Surgery Trial (ACST) showed similar results [24]. The first report of this trial showed 5-year risk for all strokes to be 6.4% in the surgical arm compared to 11.8% in the medical arm. This risk reduction was maintained in long-term follow up study for patients younger than 75 years of age, with 10-year stroke risk reduction observed to be 13.4% for CEA patients versus 17.9% for medically treated patients [25]. Critics of these older trials contend that medical therapy has improved greatly, and the current best medical therapy, particularly, the prevalent use of lipid-lowering drugs and the ameliorated control of hypertension, would void the potential benefits of CEA.
Results of more recent trials have emerged comparing CEA versus CAS for severe asymptomatic carotid stenosis in patients on contemporary medical therapy. There were 1181 asymptomatic patients with high-grade carotid artery stenosis randomized to CAS or CEA in the CREST trial, the periprocedural stroke and death rate was similar in both groups (2.5% in CAS versus 1.4% CEA) [20]. Most recently, results of the ACT randomized trial were published in February 2016, comparing CAS vs. CEA in patients with severe asymptomatic carotid artery stenosis [26]. The investigators showed that CAS was non-inferior to CEA for patients with severe asymptomatic carotid artery stenosis with 30-day rate of stroke or death of 2.9% in CAS group and 1.7% for CEA group, and cumulative 5-year rate of stroke-free survival of 93.1% in CAS and 94.7% in CEA groups, respectively. Three current multicenter randomized trials in Europe and North America, Stent-Protected Angioplasty versus Carotid Endarterectomy, Carotid Revascularization Endarterectomy versus Stenting Trial, and European Carotid Surgery Trial (SPACE-2, CREST-2, and ECST-2, respectively) are currently enrolling patients to address the important question: does intervention by either CAS or CEA offer additional benefit over contemporary best medical therapy alone in patients with severe asymptomatic carotid artery stenosis.
Special Considerations for Patients with Head and Neck Cancer
The development of carotid artery stenosis is a well-recognized late complication in patients receiving high-dose external beam radiation for head and neck cancers. It has been estimated that the relative risk of ischemic stroke is at least double following head and neck radiotherapy [27]. A review of a Medicare-cohort of 6862 patients with head and neck cancer (Surveillance Epidemiology and End-Results—SEER) between 1992 and 2012 found a 10-year incidence of cerebrovascular events of 34% in patients undergoing definitive radiotherapy, compared with 25% in patients with surgery plus post-operative radiotherapy, and 26% in patients treated with surgery alone [28]. Although this report did not differentiate the location or cause of stroke, it suggests an association between high radiation dose and an overall increased risk of stroke. The factors leading to radiation-induced vasculopathy and accelerated atherosclerosis have not yet been clearly defined, but are thought to be in part due to combined radiation effects on the vascular endothelium and the vasa vasorum of the adventitia [29]. Although most carotid lesions in radiated field have similar appearance compared to typical atherosclerotic bifurcation disease (Figs. 10.1 and 10.6), the former can be more extensive, involving the proximal common carotid, and/or mid to distal internal carotid artery not infrequently (Fig. 10.10). Several investigators have recommended routine screening and surveillance for carotid occlusive disease in all patients following external beam high dose radiation for head and neck [30,31,32,33]. However, evidence-based guidelines for the treatment of asymptomatic patients with radiation-induced carotid disease are still lacking, and optimal medical treatment has not yet been defined. Unfortunately, most of the past and current large carotid multicenter randomized trials, described in the prior sections, have excluded patients with history of neck radiation, neck dissection and active/recent cancer.

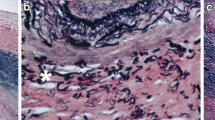
Radiation-induced carotid artery vasculopathy . Carotid plaque formation in patients after external radiation can lead to accelerated atherosclerosis of the carotid bifurcation, similar to the typical atherosclerotic process. However, radiation-induced vasculopathy can also produce more extensive plaque formation, involving the common carotid and/or the internal carotid artery beyond the bulb. Below we describe the progression of carotid disease in two patients who had neck radiation for nasopharyngeal and laryngeal cancer. (a) A sixty-three year-old woman presented with local cancer recurrence involving the left maxilla. Twelve years prior, the patient had surgical resection of squamous cell cancer of the right hard palate and alveolar ridge, and postoperative external beam radiation therapy (65 Gy to the operative bed and retropharyngeal nodes and 50 Gy to the right hemineck). The patient continued to smoke tobacco and was on chronic warfarin therapy for history of DVT. Carotid duplex ultrasound showed wall thickening of (i) right and (ii) left common carotid arteries (asterisk) and moderate to severe stenosis of (iii) right and (iv) left proximal internal carotid arteries (worse on the right). We recommended continuing medical therapy for her carotid disease. The patient then underwent partial resection of the left maxilla to remove the local recurrence without complications. (v) The patient subsequently developed asymptomatic interval occlusion of the right common (white arrow) and internal carotid arteries on CT imaging at 7 months postoperatively; black arrow points to a patent left common carotid artery. (b) A seventy-two year-old man smoker with known asymptomatic bilateral carotid artery stenosis was referred for laryngeal squamous cell cancer in 2014. Patient received IMRT to 63 Gy to the vocal cord without complications. The patient has since quit tobacco and remains on clopidogrel and statin. At 2-year follow-up, carotid duplex images show (i) moderate to severe stenosis of the right mid-internal carotid artery and (ii) moderate stenosis of the left mid-internal carotid artery; and (iii) axial CT image depicts significant calcification of bilateral carotid bifurcation. The patient has remained asymptomatic on medical therapy
Carotid endarterectomy in radiated field can be done safely, but can be associated with increased risk of surgical complications including up to approximately 25% incidence of cranial nerve injury [34, 35]. Carotid stenting provides an alternative less-invasive treatment for affected patients with radiation induced severe carotid artery stenosis. However, carotid stenting for radiation induced carotid artery stenosis have resulted in higher rate of in-stent restenosis (Fig. 10.9) [35, 36]. A recent three-center retrospective review showed no significant differences in the peri-operative complications and restenosis in patients having carotid artery stenting with or without prior neck radiation therapy [37]. At our institution, the management of patients with radiation induced carotid stenosis follows the same principles as that for non-radiated patients. Carotid intervention, either stenting or endarterectomy is recommended for symptomatic patients with moderate to severe carotid artery stenosis. Currently, our group offers surgical carotid endarterectomy as the first option to symptomatic patients considered good operative candidates. Surgical dissection in irradiated tissue can be more difficult because of presence of scar tissues with obliteration of the normal tissue planes. We have found sharp tissue dissection to be particularly useful in redo and irradiated neck to avoid inadvertent injuries. Admittedly, carotid endarterectomy in patients who had prior neck dissection or high dose radiation is more tedious than surgery in a neck without prior such treatment, but it can be done successfully in experienced hands. However, in patients with extensive soft tissue deformity in the neck, chronic tracheostomy, or high medical risks, we favor carotid stenting for symptomatic severe carotid artery stenosis.
On rare occasions, patients can present with neck wound complications after extensive neck dissection and radiation that can lead to contained carotid artery pseudoaneurysm or catastrophic carotid blow-out (Fig. 10.11). Emergency endovascular intervention to repair carotid artery rupture using covered stent can be a life-saving measure. Muscle flap reconstruction is often required to provide adequate soft tissue coverage of the carotid artery and soft tissue defect in irradiated neck wound (Fig. 10.11).

Neck wound complication and muscle flap coverage. A fifty-eight year-old woman was referred to our center for management of chronic non-healing neck wound. The patient had initially received definitive external radiation therapy for laryngeal cancer in 1999. She subsequently developed a recurrence in 2004 and underwent left neck dissection and had postoperative chemoradiation therapy. In 2010, the patient acquired a wound in her left neck, which progressed despite local wound care and hyperbaric treatment. The patient developed bleeding in the left neck wound associated with presence of a left common carotid artery pseudoaneurysm. Stenting of the pseudoaneurysm using covered stent temporarily stopped the bleeding. The patient was then transferred to our center for definitive treatment. Intra-operative photographs are provided courtesy of Dr. Peirong (Ron) Yu, Plastic Reconstructive Surgery, University of Texas MD Anderson Cancer Center. (a) Photograph of left neck wound (base of neck to right). (b) CT images show patent left common carotid artery stent (arrow) on (i) axial and (ii) sagittal views. (c) Intra-operative photograph showing covered stent (arrow; base of neck to right). (d) Reconstruction of the left common carotid artery using reversed saphenous vein graft (arrow) after extensive neck wound debridement; base of neck to the right. (e) Transposition of pedicle left latissimus dorsi myocutaneous flap to cover large wound defect. (f) Photograph of patient’s neck at 1-year follow up
The incidence perioperative stroke risk after neck dissection for head and neck cancer patients remains debatable with reports ranging from 0.2% to as high as 4.8% [38, 39]. We currently screened patients with newly diagnosed oropharyngeal or nasopharyngeal cancers for carotid artery disease if they have underlying risk factors for atherosclerotic disease such as tobacco smoking, older age, diabetes, hypertension, or hyperlipidemia. Screened patients are initiated on antiplatelet and statin therapy if found to have greater than 50% stenosis of the internal carotid artery. On rare occasions, we have successfully performed concomitant oncologic neck surgery such as nodal dissection, thyroidectomy, tracheal and esophageal resection combined with carotid endarterectomy in patients also found to have severe carotid artery stenosis (>80% stenosis) (Fig. 10.12). For cancer survivors who develop asymptomatic carotid artery stenosis following neck radiation, more studies are needed to determine whether any carotid intervention is indicated over best medical therapy. Currently, we reserved carotid intervention in asymptomatic patients only for truly high-grade (>80% stenosis). It is conceivable that early medical intervention can alter or halt the progression of radiation induced carotid plaque formation, but the role of routine screening for carotid disease in head and neck cancer patients remains to be determined in future longitudinal prospective studies. This is particularly important as we consider the changing demographics of patients diagnosed with oropharyngeal cancer. The new emerging data show that affected patients are of younger age and predominantly male (without cardiovascular risk factors), and have higher prevalence of human papilloma virus (HPV) infection and better long-term survival than in the past [40].

Concomitant oncologic neck dissection and CEA. A sixty-five year-old woman was found to have right tonsillar squamous cell cancer with nodal metastatic disease and severe right proximal internal carotid artery stenosis while undergoing work-up for right eye amaurosis fugax in 2011. Patient underwent concomitant tonsillectomy, right neck dissection, and right carotid endarterectomy. The patient received postoperative chemotherapy (cetuximab) and external neck radiation to the tumor bed (total dose of 66 Gy). At 5 years post-treatment, the patient is without evidence of cancer 5 years and has had no recurrent ischemic neurologic events. Pre-operative (a) CT image showed bulky calcified plaque causing near occlusion of the proximal right internal carotid artery (arrow), (b) ultrasound image demonstrated markedly elevated velocities consistent with greater than 80% stenosis of the proximal right internal carotid artery, and (c) PET/CT revealed large FGD-avid right neck lymph node. At 5 year post-treatment, (d) CT showed no evidence of recurrent cancer and satisfactory appearance of the right internal carotid artery patch angioplasty (arrow), and (e) normal flow velocities in the right internal carotid artery on Doppler ultrasound
Peri-operative Stroke Prevention
Routine preoperative carotid screening for cancer patients prior to oncologic surgical resection is generally not recommended. Carotid intervention for unilateral asymptomatic carotid stenosis is not warranted as the perioperative stroke risk is low in non-cardiac and non-vascular surgery [41]. However, some patients with bilateral high-grade carotid artery stenosis (or unilateral high grade carotid stenosis with contralateral carotid occlusion) may benefit from carotid revascularization before elective oncologic surgery. We have favored offering surgical carotid endarterectomy for these patients unless they are deemed to have high medical or anatomical risks. The rationale for carotid endarterectomy rather than carotid stenting is in part because of the need for at least 4–6 weeks of uninterrupted clopidogrel treatment after stenting, which would increase the perioperative risk of bleeding or delay oncologic surgery significantly. Typically, patients recover quickly after carotid endarterectomy and are ready for major oncologic surgery within 1–2 weeks, requiring only maintenance aspirin therapy peri-operatively.
The optimal level of blood pressure during surgery to prevent stroke is still controversial. For patients with occlusive cerebrovascular disease including carotid disease, we recommend keeping the peri-operative mean arterial systolic blood pressure at a level similar to preoperative baseline, or at 80–100 mmHg (permissive hypertension) to keep relatively higher cerebral perfusion pressure. In patients with known cardiovascular diseases, early resumption (or initiation) of aspirin and statin has been shown to reduce cardiovascular events [41]. Two particular subtypes of solid tumors, lung cancer and urothelial (urinary bladder) are particularly associated with tobacco smoking. Expectedly, there is a higher incidence of carotid disease and cardiovascular complications in these two subgroups of patients undergoing oncologic surgery. Cardiovascular screening and optimal medical therapy is strongly recommended in these patients with cardiovascular risk factors.
Carotid Body Tumor
Carotid body tumor (CBT) is the most common head and neck paraganglioma, a rare neuroendocrine tumor. CBT typically presents sporadically in the third or fourth decade as a slow-growing unilateral painless neck mass that is located in the carotid artery bifurcation. CBT is benign in >95% of cases with small risk of malignancy. Surgical resection is the treatment of choice for CBT. Pre-operative embolization for CBT >5 cm can be done prior to surgical excision and may help reduce intra-operative blood loss, although a recent meta-analysis did not show any benefit [42]. CBT has a very typical appearance on imaging (ultrasound, CT or MR). It is seen as a hypervascular mass, getting its blood supply from branches of the external carotid artery (most commonly the ascending pharyngeal branch), splaying the carotid artery bifurcation. Approximately 90% of CBTs can be resected without carotid artery reconstruction and only 10% require some form of carotid reconstruction such as graft interposition, patch angioplasty or primary repair [43]. The incidence of cranial nerve injury is slightly higher in patients with large tumor size (>5 cm). Surgical treatment is curative. Patients with heritable head and neck paragangliomas are more likely to present at a younger age, and have bilateral CBTs and multiple paragangliomas [44]. Management of a large CBT is shown in Fig. 10.13.


Carotid body tumor (Paraganglioma). The majority of carotid body tumors can be resected without requiring carotid artery reconstruction. We report a relatively rare case of a 17 year-old girl who presented with a large right carotid body tumor (5 cm) encasing the carotid artery bifurcation. The ascending pharyngeal branch of the right external carotid artery, the main blood supply to the tumor, was embolized using Onyx liquid polymer the day prior to surgical resection. (a) Pre-operative ultrasound images show (i) the large hypervascular tumor (asterisk), (ii) tumor encasing the internal and external carotid arteries on axial views; longitudinal view (iii) depicts normal flow in the encased internal carotid artery. (b) Pre-operative CT images demonstrates the large carotid body tumor encasing the carotid artery bifurcation on axial view (i), and sagittal view (ii). (c) Intra-operative photograph depicts the carotid body tumor (asterisk) encasing the carotid artery bifurcation (mobilized medially); other structures shown include the vagus nerve (vagus), hypoglossal nerve (arrow), an internal jugular vein (vein). Base of the neck to the right. (d) Intraoperative photograph of the reconstructed carotid artery with non-reversed ipsilateral jugular vein graft (after en-bloc resection of the carotid body tumor including the carotid artery bifurcation). Arrow points to the proximal end-to-end anastomosis of the vein graft to the proximal common carotid artery. Base of neck to the left. (e) Photograph of the excised specimen. (f) Duplex ultrasound surveillance of right carotid artery demonstrates satisfactory appearance of the vein graft at 22 months post-operatively
Recommendations Regarding Carotid Screening
Many professional societies and associations, including the Society for Vascular Surgery, the American Heart Association, American Stroke Association, and the American College of Cardiology, have put forth guidelines and recommendations regarding the management of extra-cranial carotid disease, individually or part of consensus statement [4, 7]. We have adopted these recommendations in part and put forth the following guidelines for carotid screening [45]:
-
1.
Carotid duplex ultrasound in an accredited vascular laboratory is the initial diagnostic imaging of choice for screening and evaluating the severity of stenosis in asymptomatic and symptomatic patients.
-
2.
Asymptomatic patients should be screened only if they have one or more of the following associated conditions:
-
(a)
Symptomatic peripheral arterial disease
-
(b)
Coronary artery disease
-
(c)
Risk factors for atherosclerosis including tobacco smoking, hypertension, hyperlipidemia, or family history in a first-degree relative of atherosclerosis manifested before age 60 years.
-
(a)
-
3.
Routine carotid duplex ultrasound screening is not indicated to detect clinically asymptomatic carotid stenosis in patients without associated risk factors of atherosclerosis (including patients with incidental neck bruits). The principal rationale against screening for carotid stenosis in these patients is that the potential for overall benefit is limited by low prevalence and possible harms of intervention.
-
4.
Post-intervention carotid duplex ultrasound surveillance is recommended within 30 days after carotid endarterectomy or stenting to assess the site of intervention. Further follow-up carotid duplex evaluation of the endarterectomy or stented carotid artery can be considered at intervals after intervention. Carotid duplex ultrasound evaluation of the contralateral carotid artery is also indicated if found to be greater than 50% stenosis.
-
5.
We caution the use of routine screening in asymptomatic patients after neck irradiation therapy until more studies can show its benefit.
Summary
In summary, carotid endarterectomy remains the gold-standard treatment for symptomatic patients with moderate to severe carotid artery stenosis. Carotid stenting is a comparable alternative treatment in symptomatic patients deemed high-risk for carotid endarterectomy either due to medical or anatomical reasons. For asymptomatic patients with severe carotid artery stenosis, carotid endarterectomy is warranted albeit with a narrow benefit margin over best medical therapy. Head and neck cancer patients are at increased risks for radiation-induced injury. The current management of carotid disease in head and neck cancer patients follows the same principles as that for non-cancer patients. While receiving oncologic treatment patients with known cardiovascular risk factors and carotid artery stenosis should be on concurrent antiplatelet agent and statin to minimize risk of stroke. We continue to refine our diagnostic imaging, medical therapy, surgical and endovascular techniques. The results of the ongoing clinical trials will hopefully resolve the controversy as to whether either method of carotid intervention (carotid endarterectomy or stenting) is superior to best medical therapy for asymptomatic patients with severe carotid artery stenosis.
References
Mozaffarian D, Benjamin EJ, Go AS, Arnett DK, Blaha MJ, et al. Heart Disease and Stroke Statistics-2016 update: a report from the American Heart Association. Circulation. 2016;133(4):e38–60.
Petty GW, Brown RD Jr, Whisnant JP, Sicks JD, O’Fallon WM, Wiebers DO. Ischemic stroke subtypes : a population-based study of functional outcome, survival, and recurrence. Stroke. 2000;31(5):1062–8.
Grant EG, Benson CB, Moneta GL, Alexandrov AV, Baker JD, Bluth EI, et al. Carotid artery stenosis: gray-scale and Doppler US diagnosis–Society of Radiologists in Ultrasound Consensus Conference. Radiology. 2003;229(2):340–6.
Ricotta JJ, Aburahma A, Ascher E, Eskandari M, Faries P, Lal BK. Updated Society for Vascular Surgery guidelines for management of extracranial carotid disease: executive summary. J Vasc Surg. 2011;54(3):832–6.
Korn A, Bender B, Brodoefel H, Hauser TK, Danz S, Ernemann U, et al. Grading of carotid artery stenosis in the presence of extensive calcifications: dual-energy CT angiography in comparison with contrast-enhanced MR angiography. Clin Neuroradiol. 2013;25:33–40.
Etesami M, Hoi Y, Steinman DA, Gujar SK, Nidecker AE, Astor BC, et al. Comparison of carotid plaque ulcer detection using contrast-enhanced and time-of-flight MRA techniques. AJNR Am J Neuroradiol. 2013;34(1):177–84.
Brott TG, Halperin JL, Abbara S, Bacharach JM, Barr JD, Bush RL, et al. ASA/ACCF/AHA/AANN/AANS/ACR/ASNR/CNS/SAIP/SCAI/SIR/SNIS/SVM/SVS guideline on the management of patients with extracranial carotid and vertebral artery disease: executive summary. A report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines, and the American Stroke Association, American Association of Neuroscience Nurses, American Association of Neurological Surgeons, American College of Radiology, American Society of Neuroradiology, Congress of Neurological Surgeons, Society of Atherosclerosis Imaging and Prevention, Society for Cardiovascular Angiography and Interventions, Society of Interventional Radiology, Society of NeuroInterventional Surgery, Society for Vascular Medicine, and Society for Vascular Surgery. Circulation. 2011;124(4):489–532.
Collaborative meta-analysis of randomised trials of antiplatelet therapy for prevention of death, myocardial infarction, and stroke in high risk patients. BMJ. 2002;324(7329):71–86.
Baigent C, Blackwell L, Collins R, Emberson J, Godwin J, Peto R, et al. Aspirin in the primary and secondary prevention of vascular disease: collaborative meta-analysis of individual participant data from randomised trials. Lancet. 2009;373(9678):1849–60.
Plehn JF, Davis BR, Sacks FM, Rouleau JL, Pfeffer MA, Bernstein V, et al. Reduction of stroke incidence after myocardial infarction with pravastatin: the Cholesterol and Recurrent Events (CARE) study. The Care Investigators. Circulation. 1999;99(2):216–23.
MRC/BHF Heart Protection Study of cholesterol lowering with simvastatin in 20,536 high-risk individuals: a randomised placebo-controlled trial. Lancet. 2002;360(9326):7–22.
Saam T, Yuan C, Chu B, Takaya N, Underhill H, Cai J, et al. Predictors of carotid atherosclerotic plaque progression as measured by noninvasive magnetic resonance imaging. Atherosclerosis. 2007;194(2):e34–42.
Paciaroni M, Bogousslavsky J. Primary and secondary prevention of ischemic stroke. Eur Neurol. 2010;63(5):267–78.
North American Symptomatic Carotid Endarterectomy Trial Collaborators. Beneficial effect of carotid endarterectomy in symptomatic patients with high-grade carotid stenosis. N Engl J Med. 1991;325(7):445–53.
Barnett HJ, Taylor DW, Eliasziw M, Fox AJ, Ferguson GG, Haynes RB, et al. Benefit of carotid endarterectomy in patients with symptomatic moderate or severe stenosis. North American Symptomatic Carotid Endarterectomy Trial Collaborators. N Engl J Med. 1998;339(20):1415–25.
Randomised trial of endarterectomy for recently symptomatic carotid stenosis: final results of the MRC European Carotid Surgery Trial (ECST). Lancet. 1998;351(9113):1379–87.
Yadav JS, Wholey MH, Kuntz RE, Fayad P, Katzen BT, Mishkel GJ, et al. Protected carotid-artery stenting versus endarterectomy in high-risk patients. N Engl J Med. 2004;351(15):1493–501.
Mas JL, Chatellier G, Beyssen B, Branchereau A, Moulin T, Becquemin JP, et al. Endarterectomy versus stenting in patients with symptomatic severe carotid stenosis. N Engl J Med. 2006;355(16):1660–71.
Mas JL, Chatellier G, Beyssen B. Carotid angioplasty and stenting with and without cerebral protection: clinical alert from the Endarterectomy Versus Angioplasty in Patients With Symptomatic Severe Carotid Stenosis (EVA-3S) trial. Stroke. 2004;35(1):e18–20.
Silver FL, Mackey A, Clark WM, Brooks W, Timaran CH, Chiu D, et al. Safety of stenting and endarterectomy by symptomatic status in the Cartotid Revascularization Endarterectomy Versus Stenting Trial (CREST). Stroke. 2011;42(3):675–80.
Kwolek CJ, Jaff MR, Leal JI, Hopkins LN, Shah RM, Hanover TM, et al. Results of the ROADSTER multicenter trial of transcarotid stenting with dynamic flow reversal. J Vasc Surg. 2015;62(5):1227–34.
Kakisis JD, Avgerinos ED, Antonopoulos CN, Giannakopoulos TG, Moulakakis K, Liapis CD. The European Society for Vascular Surgery guidelines for carotid intervention: an updated independent assessment and literature review. Eur J Vasc Endovasc Surg. 2012;44(3):238–43.
Endarterectomy for asymptomatic carotid artery stenosis. Executive Committee for the Asymptomatic Carotid Atherosclerosis Study. JAMA 1995;273(18):1421–8.
Halliday A, Mansfield A, Marro J, Peto C, Peto R, Potter J, et al. Prevention of disabling and fatal strokes by successful carotid endarterectomy in patients without recent neurological symptoms: randomised controlled trial. Lancet. 2004;363(9420):1491–502.
Halliday A, Harrison M, Hayter E, Kong X, Mansfield A, Marro J, et al. 10-year stroke prevention after successful carotid endarterectomy for asymptomatic stenosis (ACST-1): a multicentre randomised trial. Lancet. 2010;376(9746):1074–84.
Rosenfield K, Matsumura JS, Chaturvedi S, Riles T, Ansel GM, Metzger DC, et al. Randomized trial of stent versus surgery for asymptomatic carotid stenosis. N Engl J Med. 2016;374(11):1011–20.
Plummer C, Henderson RD, O’Sullivan JD, Read SJ. Ischemic stroke and transient ischemic attack after head and neck radiotherapy: a review. Stroke. 2011;42(9):2410–8.
Smith GL, Smith BD, Buchholz TA, Giordano SH, Garden AS, Woodward WA, et al. Cerebrovascular disease risk in older head and neck cancer patients after radiotherapy. J Clin Oncol. 2008;26(31):5119–25.
Abayomi OK. Neck irradiation, carotid injury and its consequences. Oral Oncol. 2004;40(9):872–8.
Cheng SW, Wu LL, Ting AC, Lau H, Lam LK, Wei WI. Irradiation-induced extracranial carotid stenosis in patients with head and neck malignancies. Am J Surg. 1999;178(4):323–8.
Carmody BJ, Arora S, Avena R, Curry KM, Simpkins J, Cosby K, et al. Accelerated carotid artery disease after high-dose head and neck radiotherapy: is there a role for routine carotid duplex surveillance? J Vasc Surg. 1999;30(6):1045–51.
Cheng SW, Ting AC, Ho P, Wu LL. Accelerated progression of carotid stenosis in patients with previous external neck irradiation. J Vasc Surg. 2004;39(2):409–15.
Ikawa H, Sato K, Tonogi M, Yamane GY, Kimura M, Tatsuno S, et al. Head and neck contrast-enhanced CT for identification of internal carotid artery stenosis progression on the affected side after treatment for oral squamous cell carcinoma. Oral Radiol. 2013;29(1):1–5.
Kashyap VS, Moore WS, Quinones-Baldrich WJ. Carotid artery repair for radiation-associated atherosclerosis is a safe and durable procedure. J Vasc Surg. 1999;29(1):90–6, discussion 97–9
Tallarita T, Oderich GS, Lanzino G, Cloft H, Kallmes D, Bower TC, et al. Outcomes of carotid artery stenting versus historical surgical controls for radiation-induced carotid stenosis. J Vasc Surg. 2011;53(3):629–36.e1–5.
Favre JP, Nourissat A, Duprey A, Nourissat G, Albertini JN, Becquemin JP. Endovascular treatment for carotid artery stenosis after neck irradiation. J Vasc Surg. 2008;48(4):852–8.
Ravin RA, Gottlieb A, Pasternac K, Cayne N, Schneider D, Krishnan P, et al. Carotid artery stenting may be performed safely in patients with radiation therapy-associated carotid stenosis without increased restenosis or target lesion revascularization. J Vasc Surg. 2015;62(3):624–30.
Thompson SK, Southern DA, McKinnon JG, Dort JC, Ghali WA. Incidence of perioperative stroke after neck dissection for head and neck cancer: a regional outcome analysis. Ann Surg. 2004;239(3):428–31.
Macellari F, Paciaroni M, Agnelli G, Caso V. Perioperative stroke risk in nonvascular surgery. Cerebrovasc Dis. 2012;34(3):175–81.
Pytynia KB, Dahlstrom KR, Sturgis EM. Epidemiology of HPV-associated oropharyngeal cancer. Oral Oncol. 2014;50(5):380–6.
Selim M. Perioperative stroke. N Engl J Med. 2007;356(7):706–13.
Abu-Ghanem S, Yehuda M, Carmel NN, Abergel A, Fliss DM. Impact of preoperative embolization on the outcomes of carotid body tumor surgery: a meta-analysis and review of the literature. Head Neck. 2016;38(Suppl 1):E2386–94.
Power AH, Bower TC, Kasperbauer J, Link MJ, Oderich G, Cloft H, et al. Impact of preoperative embolization on outcomes of carotid body tumor resections. J Vasc Surg. 2012;56(4):979–89.
Sridhara SK, Yener M, Hanna EY, Rich T, Jimenez C, Kupferman ME. Genetic testing in head and neck paraganglioma: who, what, and why? J Neurol Surg B Skull Base. 2013;74(4):236–40.
Huynh TT, Broadbent KC, Jacob AD, James S, Erasmus JJ. Screening for carotid artery stenosis. Semin Roentgenol. 2015;50(2):127–38.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2018 Springer International Publishing AG, part of Springer Nature
About this chapter

Cite this chapter
Huynh, T.T.T., Pisimisis, G.T., Broadbent, K.C., Mehran, R.J. (2018). Carotid Artery Disease in Patients with Cancer. In: Yusuf, S., Banchs, J. (eds) Cancer and Cardiovascular Disease. Springer, Cham. https://doi.org/10.1007/978-3-319-62088-6_10
Download citation
DOI: https://doi.org/10.1007/978-3-319-62088-6_10
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-62086-2
Online ISBN: 978-3-319-62088-6
eBook Packages: MedicineMedicine (R0)