
Abstract
An 84-year-old, partially dependent woman, presented with a progressive course of visual hallucinations and fluctuating confusional state for 2 months. One week prior to admission, she was found lying in bed, disoriented, with incoherent speech and refusing food and rapidly evolved with deterioration of conscience. On hospital admission, she was in a comatose state, severely dehydrated and emaciated. The initial workup showed no signs of infection.
Access provided by CONRICYT-eBooks. Download chapter PDF
Similar content being viewed by others


An 84-year-old, partially dependent woman, presented with a progressive course of visual hallucinations and fluctuating confusional state for 2 months. One week prior to admission, she was found lying in bed, disoriented, with incoherent speech and refusing food and rapidly evolved with deterioration of conscience. On hospital admission, she was in a comatose state, severely dehydrated and emaciated. The initial workup showed no signs of infection.
-
1.
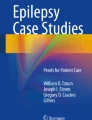
What bulbar structures are hyperintense in ◘ Fig. 44.1c (black arrows)?
-
2.
What other supratentorial structures would one expect to be typically involved in this disorder?
-
3.
What blood analysis could confirm the most likely diagnosis?

MRI a, b axial T2 FLAIR, c axial T2 TSE and d ADC map
Wernicke’s encephalopathy
FormalPara Answers-
1.
The hypoglossal nuclei
-
2.
Dorsomedial thalami
-
3.
Blood thiamine concentration
1 Comments
Wernicke’s encephalopathy is an acute neurological disorder, resulting from thiamine (vitamin B1) deficiency which, when untreated, produces severe deficits, with progression to coma and even death. The prognosis strongly relies on early recognition and thiamine supplementation. Neuroimaging plays a central role in the diagnosis of Wernicke’s encephalopathy, particularly in patients with no history of alcohol abuse or presenting with atypical clinical manifestations. MRI can show both typical, symmetric T2 hyperintensity in the dorsomedial thalami, tectal plate, periaqueductal area and mammillary bodies (◘ Fig. 44.1a, b), and atypical, T2 hyperintense lesions in the cerebellum, cerebellar vermis, cranial nerve nuclei (◘ Fig. 44.1c) and cerebral cortex, features, the latter being characteristic of non-alcoholic patients [1]. In the acute phase, affected regions may show restricted diffusion (◘ Fig. 44.1d) and contrast enhancement [2].
References
Zuccoli G, et al. Neuroimaging findings in acute Wernicke’s encephalopathy: review of the literature. AJR. 2009;192:501–8.
Manzo G, et al. MR imaging findings in alcoholic and nonalcoholic acute Wernicke’s encephalopathy: a review. Biomed Res Int. 2014;2014:503–96.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2018 Springer International Publishing AG
About this chapter
Cite this chapter
Martins, R., Alves, J.E. (2018). Case 44. In: Xavier, J., Vasconcelos, C., Ramos, C. (eds) Diagnostic and Therapeutic Neuroradiology. Springer, Cham. https://doi.org/10.1007/978-3-319-61140-2_44
Download citation
DOI: https://doi.org/10.1007/978-3-319-61140-2_44
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-61139-6
Online ISBN: 978-3-319-61140-2
eBook Packages: MedicineMedicine (R0)