
Abstract
The sphenopalatine ganglion (SPG), also termed the pterygopalatine ganglion, consists of a parasympathetic ganglion with multiple connections to the general sensory fibers of the head and to the internal carotid plexus without synapses. This ganglion can be blocked using a multitude of techniques to treat refractory facial, headache, and other types of pain. Documented techniques include an infrazygomatic, intranasal, and transnasal approach. The evidence for performing an SPG block is moderate in quality and has only weak recommendations. If this procedure is to be performed, diagnostic blocks should be performed initially and reproducibly with fluoroscopy before proceeding to neurolysis.
Access provided by CONRICYT-eBooks. Download chapter PDF
Similar content being viewed by others



Keywords
- Cluster headaches
- Facial pain
- Headache
- Migraines
- Oral pain
- Pterygopalatine
- Sphenopalatine
- Trigeminal neuralgia
Introduction
The sphenopalatine ganglion (SPG), also termed the pterygopalatine ganglion , is a parasympathetic ganglion with multiple connections to general sensory fibers of the head and to the internal carotid plexus without synapses as shown in Fig. 33.1 [1]. The SPG has been blocked using different techniques for the treatment of refractory facial, headache, and other types of pain. With moderate quality evidence from studies on SPG blockade, there are only weak recommendations. In parallel with the current evidence, reproducible pain relieving diagnostic blocks should be performed under fluoroscopy before proceeding to radiofrequency neurolysis.

Sphenopalatine ganglion (From Netter FH: Atlas of Human Anatomy, edn 4. Saunders-Elsevier; 2006; with permission). All rights reserved
History
In 1908, the SPG was described as a pain originator and transmitter by Sluder [1, 2]. He theorized infection of the sinuses and tissue membranes irritated the SPG leading to a neuralgic facial pain syndrome, also coined “Sluder’s neuralgia.” Years after Sluder’s theory, Ruskin [3] divided Sluder’s neuralgia into four separate categories that comprised facial pain syndrome . Ruskin’s theory postulated that SPG pathology caused trigeminal neuralgia [4]. In 1940, Eagle [5] suggested that SPG inflammation was secondary to intranasal deformities and infection.
The role that the SPG is involved in facial and head pain has been hypothesized by two different mechanisms. One hypothesis is an unequal sympathetic and parasympathetic tone existing within the SPG leading to blockade of enkephalins and release of substance P. The other hypothesis relates to an abnormal propagation of impulses through the afferent nociceptive C-fibers secondary to focal demyelination of the SPG [6]. Since then, multiple techniques and outcomes have been described [7,8,9,10,11,12,13,14,15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45].
Evidence Base
-
Sanders and Zuurmond [29] did a case series on SPG RFTC, which included 66 patients with a diagnosis of episodic and chronic cluster headaches.
-
34 of 56 patients with episodic and 3 of 10 with chronic headaches reported complete resolution of headaches during a mean follow-up of 29 months.
-
-
Salar et al. [28] had a case series performing RFTC lesions at 60° and 65° for 60 s on seven patients with sphenopalatine neuralgia.
-
All seven patients were pain-free from 6 to 34 months’ follow-up.
-
-
Prasanna and Murthy [30] reported that ten patients with pain secondary to cancer of the floor of the mouth and tongue were pain-free in the short term.
-
Bayer et al. [31] studied pulsed radiofrequency of the SPG in 30 patients with chronic face and head pain.
-
21% had complete pain relief, 65% had mild-moderate pain relief, and 14% had no pain relief.
-
65% of the patients had mild to moderate reductions of pain medications.
-
-
Janzen and Scudds [32] performed a randomized controlled trial studying the effectiveness of the SPG block for fibromyalgia and myofascial pain syndrome.
-
There was no significant difference between the lidocaine and control groups.
-
-
Quevedo et al. [33] showed in a case report that the SPG block was effective in two patients with complex regional pain syndrome of the lower extremities.
-
Costa et al. [34] performed a clinical trial revealing the effectiveness of cocaine and lidocaine during nitroglycerin-induced cluster headaches.
-
Cepero et al. [35] showed that SPG neurectomy for the treatment of facial pain was effective in 12 patients.
-
There was high recurrence of facial pain that was less severe and treated with medications.
-
-
Peterson et al. [36] along with Yang and Oraee [37] revealed the effectiveness of the transnasal SPG block.
-
Windsor and Jahnke [24] had success with the modified transnasal SPG.
-
Day [38] reviewed multiple publications and provided recommendations using Guyatt et al.’s [46] grading of recommendations. This took into consideration the benefits versus risks, methodological quality of supporting evidence, and implications (Table 33.1):
-
1C–strong recommendation, low- or very-low-quality evidence
-
2B–weak recommendations, moderate-quality evidence
Table 33.1 Graded evidence for the sphenopalatine ganglion block -
-
Nguyen and Wilkes [44] describe successful treatment of refractory V2 trigeminal neuralgia with a pulsed radiofrequency of V2, a series of sphenopalatine blocks, and methadone.
-
Cornelissen et al. [45] state when conservative therapy fails, pulsed radiofrequency (RF) of the pterygopalatinum is an option for treatment. The available evidence is classified as 2C+: effectiveness only demonstrated in observational studies; given there is no conclusive evidence of the effect, benefits closely balance with risk and burdens.
Indications
-
Common
-
Persistent idiopathic facial pain
-
Cancer
-
Floor of the mouth
-
Tongue
-
-
Headaches
-
Cluster
-
Migraine
-
Post-traumatic
-
Oral pain
-
Sphenopalatine neuralgia
-
Trigeminal neuralgia
-
-
-
Reported
-
Complex regional pain syndrome involving lower extremities
-
Fibromyalgia
-
Low back pain
-
Myofascial pain
-
Sinus arrest in post-herpetic neuralgia
-
Vasomotor rhinitis
-
-
Preoperative Evaluation
-
Evaluate patient for anticoagulant or antiplatelet therapy prior to any interventional pain management procedure .
-
The benefit of the patient receiving the procedure must outweigh the risk of withholding anticoagulation to justify the procedure.
-
Communication with the patient’s primary care physician (PCP) or cardiologist is a necessity to ensure patient safety and to protect the pain physician.
-
Please refer to guidance described in comprehensive reviews [47,48,49,50].
-
Coumadin should be withheld according to PCP’s or cardiologist’s recommendations, and a prothrombin time (PT) should be evaluated prior to the procedure.
-
Heparin use should receive the same precautions as Coumadin use, although a partial thromboplastin time (PTT) should be evaluated instead.
-
If the SPG block is anticipated to be difficult to perform due to the patient’s anatomy or unsuccessful block under fluoroscopy, a CT scan is recommended.
-
-
Anatomy
-
Pterygopalatine fossa
-
The SPG is the largest of the four parasympathetic ganglions of the head. It is located in the pterygopalatine fossa near the sphenopalatine foramen posterior to the foramen rotundum and anterior to the pterygoid canal (Figs. 33.1 and 33.2) [7].
Fig. 33.2 
The sensory innervation of the lateral wall of the nasal cavity, hard and soft palates, and nasopharynx
-
Anteriorly to the fossa is the maxillary sinus, while the medial pterygoid plate is located posteriorly. Medial to the fossa is the palatine bone with the sphenoid sinus superiorly (Fig. 33.3).
Fig. 33.3 
Fluoroscopic anteroposterior view of the face. MT middle turbinate, O orbit, R ramus, S septum
-
Superolaterally is the foramen rotundum, and inferomedially lies the pterygoid canal.
-
Vasculature that exists within the fossa includes the maxillary artery and its branches.
-
With a lateral fluoroscopic view, the fossa is V-shaped with dimensions of 1 cm in width and 2 cm in height.
-
Needle access to the fossa is via the pterygomaxillary fissure.
-
-
Sphenopalatine ganglion
-
The maxillary nerve is attached superiorly to the SPG by the pterygopalatine nerve within the pterygopalatine fossa. In the sagittal view, the SPG appears to be on the medial side of the maxillary nerve [8].
-
The Vidian nerve is attached posteriorly to the ganglion.
-
Efferent branches of the ganglion compose the superior posterior lateral nasal and pharyngeal nerves.
-
The greater and lesser palatine nerves exit the SGP caudally.
-
-
Sensory fibers
-
Sensory innervations to the nasal membrane, parts of the pharynx, soft palate, and the upper teeth originate from the maxillary nerve traveling through the SPG.
-
-
Motor fibers
-
Within the sensory trunks are thought to be a small number of secretomotor nerves .
-
-
Autonomic pathways
-
Sympathetic fibers
-
Originating in the upper thoracic spinal cord, the preganglionic sympathetic fibers comprise the white rami communicantes ascending through the sympathetic chain into the superior cervical ganglion.
-
Postganglionic fibers combine with the carotid plexus and then travel to the deep petrosal and Vidian nerves toward the SPG. From the SPG, the postganglionic fibers continue and innervate the lacrimal gland and the nasal and palatine mucosa.
-
-
Parasympathetic fibers
-
From the superior salivatory nucleus, the parasympathetic preganglionic fibers travel through the facial nerve becoming the greater petrosal nerve.
-
The greater and deep petrosal nerves combine to form the Vidian nerve ending in the SPG.
-
Preganglionic fibers synapse with postganglionic fibers in the SPG through the nasal mucosa joining the maxillary nerve and innervating the lacrimal gland.
-
-


Technical Aspects
Multiple approaches of sphenopalatine ganglion block have been reported [10,11,12,13,14,15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45]:
-
Technical approaches
-
Intranasal
-
Infrazygomatic
-
Transnasal
-
-
Medications
-
Cocaine 4%
-
Lidocaine 1–2%
-
Bupivacaine or ropivacaine 0.25–0.5%
-
Intranasal Approach
-
The advantage of this approach is that it may be done in an office setting.
-
The SPG may absorb local anesthetic via the middle turbinate and lateral nasal mucosa from a cotton-tipped applicator.
-
Due to vasoconstrictive properties of cocaine, it is the local anesthetic of choice.
-
Lidocaine, bupivacaine, or ropivacaine may be an alternative if cocaine is unavailable or contraindicated.
-
The patient is placed in the supine position.
-
Measuring the distance from the opening of the nares to the mandibular notch directly below the zygoma will estimate how deep the cotton-tipped applicator should be advanced.
-
Mark the cotton-tipped applicator with this depth measurement.
-
Soak the cotton-tipped applicator in the local anesthetic for a few minutes.
-
Phenylephrine may be administered into the patient’s nares to reduce the incidence of epistaxis.
-
Slowly advance the cotton-tipped applicator into the nares parallel to the zygoma with the tip angled laterally until the marked depth is reached.
-
If the nares is large enough, insert a second cotton-tipped applicator with local anesthetic superiorly, and advance it past the first applicator by 0.5–1 cm.
-
Allow the applicators to stay in place for 30–45 min.
-
Findings of conjunctival injection, ipsilateral tearing, and nasal congestion are consistent with a successful block.
-
If the patient relieves no pain relief within 30 min, apply additional local anesthetic by trickling a small volume of it down the side of the cotton-tipped applicator.
-
After 45 min, remove the cotton-tipped applicator(s).
-
If there is no pain relief, the SPG may not be the origin of pain, or it may not be accessible with the intranasal approach.
-
The infrazygomatic approach is recommended to rule out both possibilities.
-
-
Infrazygomatic Approach
-
Fluoroscopy or CT is recommended for this approach to improve the chance of a successful block and patient safety [19].
-
The patient may require light sedation, such as midazolam and fentanyl, or monitored anesthesia care.
-
The patient is placed in the supine position.
-
Sterile prepping and draping of the appropriate side of the face are required. This should span the area posteriorly from the nose toward the ear and inferiorly from the zygomatic arch toward the mandible. Leave the ipsilateral eye exposed. This allows for recognition of a retrobulbar hematoma should one occur.
-
Obtain a lateral fluoroscopic view to visualize the pterygopalatine fossa, and identify the mandibular notch.
-
In the lateral fluoroscopic view, the pterygopalatine fossa is identified, which appears to be a “V” (Fig. 33.4).
Fig. 33.4 
Lateral fluoroscopic view of the face. HP hard palate, MN mandibular notch, MS maxillary sinus, PF pterygopalatine fossa, SP sphenopalatine ganglion
-
Be sure to superimpose the right and left fossae by positionally adjusting the C-arm while maintaining the patient’s head midline.
-
A 10 cm curved blunt 20- or 22-gauge needle is preferred for this approach. Alternatively a 3.5 inch, 22-gauge, short-bevel needle with the distal tip bent (away from the notch in the hub) to a 15° angle may be used.
-
Anesthetize the skin above the mandibular notch. Insert a 1.25 inch, 16-gauge angiocatheter into the skin.
-
Remove the sharp needle from the angiocatheter, and insert the block needle.
-
Under intermittent fluoroscopy, advance the block needle in a medial, anterior, and slightly caudad toward the midpoint of the pterygopalatine fossa (Fig. 33.5).
Fig. 33.5 
Lateral fluoroscopic view with the block needle tip in the pterygopalatine fossa
-
Obtain an anterior-posterior fluoroscopic view, and advance the block needle under intermittent fluoroscopy toward the middle turbinate. Block needle tip advancement should stop adjacent to the palatine bone (Fig. 33.6).
Fig. 33.6 
Fluoroscopic anteroposterior view of the face with the block needle adjacent to the palatine bone. MT middle turbinate, O orbit, S septum
-
To rule out intravascular uptake and intranasal spread, 0.5–1 mL of nonionic, water-soluble contrast should be injected into the fossa under continuous fluoroscopy.
-
Inject 2 mL of local anesthetic (1–2% lidocaine or 0.25% bupivacaine) with or without steroids once satisfactory needle placement has been confirmed.
-
If the coronoid process does not obstruct access to the fossa, an alternative approach is to insert the angiocatheter and the block needle cephalad to the coronoid process using a coaxial technique. The needle is then advanced until the tip is in the fossa, adjacent to the palatine bone.
-
-
A CT-enhanced SPG block technique has been described by Vallejo et al. [23].
-
Both fluoroscopy and CT are used simultaneously to increase the chance of a successful block and safety.
-
The patient is placed in the supine position, and the patient’s head is rotated to until both rami of mandible are superimposed on lateral fluoroscopic view.
-
In this view, the pterygopalatine fossa looks like a “reverse vase” (Fig. 33.5).
-
Palpate the zygoma and insert a 3.5 inch 25-gauge needle perpendicularly to the skin.
-
Advance the needle under intermittent fluoroscopy in a medial cephalad dorsal trajectory toward the pterygopalatine fossa .
-
Intermittent anterior-posterior fluoroscopic view should be performed to avoid penetrating the lateral nasal mucosa (Fig. 33.6).
-
Under CT guidance , the needle tip may be placed in the fossa with a slight turn (Fig. 33.7).
Fig. 33.7 
(a, b) Reconstructed CT image, showing the needle inside the pterygopalatine fossa
-
-




Transnasal Approach
-
This technique may be done with or without fluoroscopy.
-
The area spanning between the inferior to middle turbinate and from the nares to the nasopharynx posterolateral wall should be anesthetized with lidocaine 1.5% with epinephrine 1:200,000 using a cotton-tipped applicator.
-
Next, the area is sterilized by using an iodine-soaked cotton-tipped applicator.
-
For the transnasal approach, a 5 inch, 26-gauage spinal needle in the plastic cover sheath utilized.
-
Using a sterile scalpel, the tip of the sheath is cut obliquely at 45° creating a sheath bevel to expose 2 mm of the spinal needle tip (Fig. 33.8).
Fig. 33.8 
(a–c) Fluoroscopic transnasal sphenopalatine ganglion
-
Mark the sheath’s end opposite to the cut to identify the orientation of the sheath’s bevel.
-
The spinal needle tip port side should be bent at 45° opposite to the sheath’s bevel. The side port indicator is now used as a tip pointer (Fig. 33.8).
-
Withdraw the needle into the sheath until the tip is not visible, and apply lidocaine 2% jelly to the outside of the sheath.
-
Advance the sheath into the nasal cavity while orienting the bevel mark facing laterally.
-
Once resistance is met due to the sheath contacting the nasopharynx posterolateral wall, confirm the spinal needle tip pointer is facing laterally. Next, advance the spinal needle into the nasopharyngeal mucosa.
-
Negative aspiration through the spinal needle must be confirmed, and then 1.5 mL of contrast is injected under continuous fluoroscopy in the anterior-posterior and lateral views. This is to confirm appropriate contrast flow in the pterygopalatine fossa with no intravascular uptake (Fig. 33.8).
-
At the level of the conch, the spinal needle tip should be positioned near the posterolateral wall of the nasal cavity and medial to the medial pterygoid plate.
-
Triamcinolone 20 mg and 1.5 mL of local anesthetic are injected to block the SPG.
-
The needle needs to be flushed and hemostasis obtained and confirmed using a cotton-tipped applicator.
-
A modification of the transnasal approach described by Windsor and Jahnke [24]:
-
This technique is to allow improved control of the amount of medication reaching the posterior nasopharynx, improved patient comfort, and increased exposure of local anesthetic to surrounding tissues of the SPG.
-
The patient is placed in the supine position with the cervical spine in extension.
-
Inspect the nares for any abnormal masses or septal deviation.
-
Viscous lidocaine 2% is administered to the patient nasally as he/she inhales to assist in anesthetizing the nasal mucosa.
-
This technique requires standard intravenous administration set:
-
The tubing is uncurled, and the flow regulator is moved against the Y-infusion port.
-
A 3 mL syringe is screwed onto the Y-port.
-
The tubing distal to the Y-infusion port is measured in relation to a 10 cm cotton-tipped applicator and cut immediately to the proximal end of the cotton tip.
-
The cotton-tipped applicator is inserted into the intravenous tubing distal to the Y-infusion port exposing only the cotton tip outside of the intravenous tubing (Figs. 33.9a, b).
Fig. 33.9 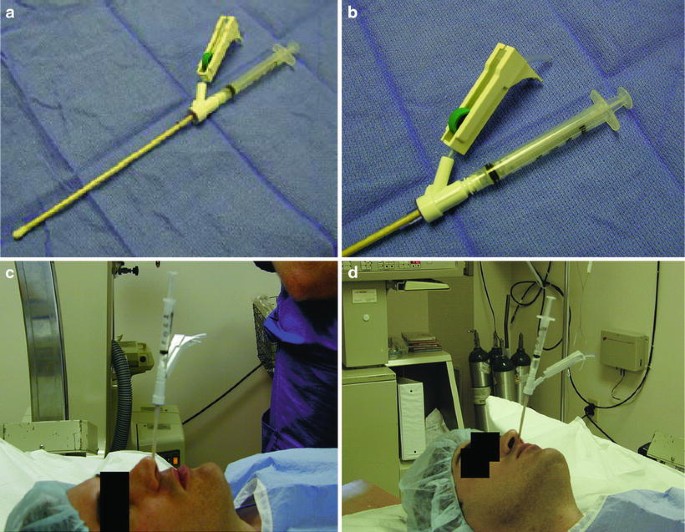
A modified transnasal SPG block technique. (a) Picture of the suggested SPG block device. Note that the cut end of the tubing reaches the proximal end of the cotton tip of the applicator and the infusion port lies immediately against the proximal tip of the applicator. (b) Close-up picture of the suggested SPG block device. Note the connection between the syringe, Y-infusion port, and cut tubing. (c) Lateral view of the SPG block device in place along the middle turbinate to the nasopharynx. (d) Oblique view of SPG block device in place along the middle turbinate to the nasopharynx
-
-
This device is inserted into the nostril traveling along the middle turbinate toward the nasopharynx. This may be performed for both nostrils if the patient has bilateral pain.
-
The attached 3 mL syringe is filled with 2 mL of local anesthetic.
-
The cotton tip of the applicator must be primed by injecting 0.5 mL of the local anesthetic from the attached 3 mL syringe.
-
The remaining 1.5 mL of local anesthetic is to be delivered over 5–10 min, and then the applicator is left in place for 20–30 min (Figs. 33.9c, d).
-


Radiofrequency Lesioning
-
Upon completion of successful diagnostic block(s), radiofrequency thermocoagulation (RFTC) and pulsed radiofrequency (P-RF) are options.
-
Using the infrazygomatic approach, an insulated RF needle with either a 3 or 5 mm active tip is used. The 3 mm active tip is preferred to avoid lesioning of nerves in close proximity to the SPG.
-
With proper RF needle placement, sensory stimulation is conducted at 50 Hz and up to 1 V. Paresthesia at the root of the nose should be described by the patient at less than 0.5 V.
-
Stimulation of the palatine nerves leads to paresthesia in the hard palate. Redirect the needle cephalad and medial.
-
Stimulation of the maxillary nerve causes paresthesia in the upper teeth. Redirect the needle caudally and medial.
-
2–3 mL of local anesthetic should be injected to anesthetize the area before lesioning.
-
RFTC should be performed for 90 s at 80 C for two cycles.
-
P-RF lesioning can be performed at 40–42 °C for 120 s for 2–4 cycles.
-
A case report by Shah and Racz [26] reveals long-term pain relief of post-traumatic headache with the use of pulsed radiofrequency to the SPG.
-
-
Precautions
-
Relative
-
Allergy to medications used
-
Anticoagulation
-
Antiplatelet therapy
-
History of facial trauma
-
-
Absolute
-
Allergy to medications used
-
Coagulopathy
-
History of chronic epistaxis (intranasal technique)
-
Infection
-
Patient refusal
-
-
Side Effects and Complications
-
Epistaxis secondary to aggressive placement of a cotton-tipped applicator into the nasal passage or needle penetration of the lateral nasal wall using the infrazygomatic approach.
-
Local or retro-orbital hematoma can result from puncturing the venous plexus overlying the pterygopalatine fossa or maxillary artery, including branches.
-
Infection may occur without aseptic technique.
-
Reflex bradycardia has been reported with the use of RFTC [27].
-
Transient hypoesthesia or anesthesia of the palate or pharynx secondary to RFTC [28, 29].
Key Points
-
1.
The sphenopalatine ganglion, also termed the pterygopalatine ganglion, is a parasympathetic ganglion with multiple connections to general sensory fibers of the head and to the internal carotid plexus without synapses.
-
2.
Reproducible pain-relieving diagnostic blocks should be performed under fluoroscopy before proceeding to radiofrequency neurolysis.
-
3.
Indications for an SPG block include persistent idiopathic facial pain, oral pain, and headaches.
-
4.
The patient must be evaluated preoperatively for anticoagulation, and the anticoagulant must be stopped accordingly prior to the procedure with consultation with the patient’s PCP or cardiologist.
-
5.
The three different technical approaches for the SPG block include the intranasal, infrazygomatic, and transnasal approach.
-
6.
The intranasal approach may be done in the office.
-
7.
It is recommended to use fluoroscopy or CT to perform the infrazygomatic approach.
-
8.
Complications documented include epistaxis, local or retro-orbital hematoma, infection, reflex bradycardia, and transient hypesthesia or anesthesia of the palate or pharynx.
References
Day M. Sphenopalatine ganglion block. In: Manchikanti L, Singh V, editors. Interventional techniques in chronic non-spinal pain. Paducah: ASIPP Publishing; 2009. p. 101–14.
Sluder G. The role of the sphenopalatine ganglion in nasal headache. NY State J Med. 1908;27:8–13.
Ruskin S. Contributions to the study of the sphenopalatine ganglion. Laryngoscope. 1925;36:87–108.
Waldman S. Sphenopalatine ganglion block 80 years later. Reg Anesth Pain Med. 1993;18:274–6.
Eagle W. Sphenopalatine neuralgia. Arch Otolaryngol. 1942;35:66–84.
Pollock B, Kondziolka D. Stereotactic radiosurgical treatment of sphenopalatine neuralgia. J Neurosurg. 1997;87:450–3.
Berkovitz BKB. Nose, nasal cavity, paranasal sinuses and peterogopalatine fossa. In: Strandrig S, editor. Gray’s anatomy: the anatomical basis of clinical practice. 39th ed. Edinburgh: Elsevier, Churchill Livingston; 2005. p. 567–79.
Puig C, Driscoll C, Kern E. Sluder’s sphenopalatine ganglion neuralgia – treatment with 88% phenol. Am J Rhinol. 1998;12:113–8.
Grigoryan YA, Slavin KV, Ogleznev KY. Ultrasonic lesion of trigeminal nucleus caudalis for differentiation facial pain. Acta Neurochir. 1994;131:229–35.
Felisati G, Arnone F, Lozza P, et al. Sphenopalatine endoscopic ganglion block: a revision of a traditional technique for cluster headache. Laryngoscope. 2006;116:1447–50.
Higuchi Y, Nashold B, Sluitjer ME, et al. Exposure of the dorsal root ganglion in rats to pulsed radiofrequency currents activates dorsal horn lamina 1 and 2 neurons. Neurosurgery. 2002;50:850–5.
Varghese BT, Koshy RC. Endoscopic transnasal neurolytic sphenopalatine ganglion block for head and neck cancer pain. J Laryngol Otol. 2001;115:385–7.
Brown CR. Sphenopalatine ganglion neuralgia. Pract Peridontics Anesthet Dent. 1997;9:99–100.
Klein RN, Burk DT, Chase PF. Anatomically and physiologically based guidelines for use of the sphenopalatine ganglion block versus the stellate ganglion block to reduce atypical facial pain. Cranio. 2001;19:48–55.
Ryan R, Facer G. Sphenopalatine neuralgia and cluster headache: comparisons, contrasts, and treatment. Headache. 1977;17:7–8.
Levbovits A, Alfred H, Lefkowitz MSPG. Block: clinical uses in the pain management clinic. Clin J Pain. 1990;6:131–6.
Saberski L, Ahmad M, Wiske P. Sphenopalatine ganglion block for treatment of sinus arrest in postherpetic neuralgia. Headache. 1999;38:42–4.
Prasanna A, Murphy P. Vasomotor rhinitis and sphenopalatine ganglion block. J Pain Symptom Manag. 1997;13:332–7.
Raj P, Lou L Erdine S, et al. Sphenopalatine ganglion block and Neurolysis. Radiographic imaging for regional Anesthesia and pain management. 1st ed. Philadelphia: Churchill Livingstone; 2003.
Raj P, Rauck R, Racz G. Autonomic nerve blocks. In: Raj P, editor. Pain medicine: a comprehensive review. St. Louis: Mosby; 1996. p. 227–56.
Day M. Neurolysis of the trigeminal and sphenopalatine ganglia. Pain Pract. 2001;1:171–82.
Day M. Sphenopalatine ganglion analgesia. Curr Rev Pain. 1999;3:342–7.
Vallejo R, Benyamin R, Yousuf N, et al. Computed tomography-enhanced sphenopalatine ganglion blockade. Pain Pract. 2007;7:44–6.
Windsor RE, Jahnke S. Sphenopalatine ganglion blockade: a review and proposed modification of the transnasal technique. Pain Physician. 2004;7:283–6.
Sluitjer M, Racz G. Technical aspects of radiofrequency. Pain Pract. 2002;2:195–200.
Shah R, Racz G. Long-term relief of posttraumatic headache by sphenopalatine ganglion pulse radiofrequency lesioning: a case report. Arch Phys Med Rehabil. 2004;85:1013–6.
Konen A. Unexpected effects due to radiofrequency thermocoagulation of the sphenopalatine ganglion: 2 case reports. Pain Digest. 2000;10:30–3.
Salar G, Ori C, Iob I. Percutaneous thermocoagulation for sphenopalatine ganglion neuralgia. Acta Neurochir. 1987;84:24–8.
Sanders M, Zuurmond W. Efficacy of sphenopalatine ganglion blockade in 66 patients suffering from cluster headache: a 12- to 70-month follow-up evaluation. J Neurosurg. 1997;87:876–80.
Prasanna A, Murthy PS. Sphenopalatine ganglion block and pain of cancer. J Pain Symptom Manag. 1993;8:125.
Bayer E, Racz GB, Day M, et al. Sphenopalatine ganglion pulsed radiofrequency treatment in 30 patients suffering from chronic face and head pain. Pain Pract. 2005;5:223–7.
Janzen VD, Scudds R. Sphenopalatine blocks in the treatment of pain in fibromyalgia and myofascial pain syndrome. Layrngoscope. 1997;1077:1420–2.
Quevedo J, Purgavie K, Platt H, et al. Complex regional pain syndrome involving the lower extremity: a report on 2 cases of sphenopalatine ganglion block as a treatment option. Arch Phys Med Rehabil. 2005;86:335–7.
Costa A, Pucci E, Antonaci F, et al. The effect of intranasal cocaine and lidocaine on nitroglycerin-induced attacks in cluster headache. Cephalagia. 2000;20:85–91.
Cepero R, Miller R, Bressler K. Long-term results of sphenopalatine ganglion neurectomy for facial pain. Am J Otolaryngol. 1987;8:171–4.
Peterson J, Schames J, Schames M, King E. Sphenopalatine ganglion block: a safe and easy method for the management of orofacial pain. J Craniomandibular Pract. 1995;13:177–81.
Yang IY, Oraee S. A novel approach to transnasal sphenopalatine ganglion injection. Pain Physican. 2006;9:131–4.
Day M. Sympathetic blocks: the evidence. Pain Pract. 2008;8:98–109.
Berger J, Pyles S, Saga-Rumley S. Does topical anesthesia of the sphenopalatine ganglion with cocaine or lidocaine relieve low back pain? Anesth Analg. 1986;65:700–2.
Ferrante FM, Kaufman AG, Dunbar SA, et al. Sphenopalatine ganglion block for the treatment of the head, neck, and shoulders. Reg Anesth Pain Med. 1998;23:30–6.
Gregoire A, Clair C, Delabrousse E, et al. CT guided neurolysis of the sphenopalatine ganglion for management of refractory trigeminal neuralgia. J Radiol. 2002;83:1082–4.
Manahan A, Malesker M, Malone P. Sphenopalatine ganglion block relieves symptoms of trigeminal neuralgia: a case report. Nebr Med J. 1996;9:306–9.
Saade E, Paige G. Patient-administered sphenopalatine ganglion block. Reg Anesth. 1996;21:68–70.
Nguyen M, Wilkes D. Pulsed radiofrequency V2 treatment and intranasal sphenopalatine ganglion block: a combination therapy for atypical trigeminal neuralgia. Pain Pract. 2010;10:370–4.
Cornelissen P, Van Kleef M, Mekhail N, et al. Persistent idiopathic facial pain. Pain Pract. 2009;9:443–8.
Guyatt G, Gutterman D, Bauman MH, Addrizzo-Harris D, Hylek EM, Phillilps B, Raskob G, Lewis SZ, Scgunemann H. Grading strength of recommendations and quality of evidence in clinical guidelines: report from an American college of chest physician’s task force. Chest. 2006;129:174–81.
Horlocker TT, Wedel DJ, Benzon H, et al. Regional anesthesia in the anticoagulated patient: defining the risks (the second ASRA consensus conference on Neuraxial Anesthesia and anticoagulation). Reg Anesth Pain Med. 2003;28:172–97.
Manchikanti L, FJE F, Benyamin RM, et al. Assessment of bleeding risk of interventional techniques: a best evidence synthesis of practice patterns and perioperative management of anticoagulant and antithrombotic therapy. Pain Physician. 2013;16:SE261–318.
Manchikanti L, Kaye AD, Falco FJE. Antithrombotic and antiplatelet therapy. In: Essentials of interventional techniques in managing chronic pain: New York, Springer; 2017.
Raj PP, Shah RV, Kay AD, et al. Bleeding risk in the interventional pain practice: assessment, management, and review of the literature. Pain Physician. 2004;6:3–52.
Acknowledgments
This book chapter is modified and updated from a previous book chapter, “Sphenopalatine Ganglion Block” by Miles Day, MD, in Interventional Techniques in Chronic Spinal Pain published by ASIPP Publishing. Permission has been obtained from ASIPP Publishing.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2018 Springer International Publishing AG
About this chapter

Cite this chapter
Skulpoonkitti, B., Day, M. (2018). Sphenopalatine Ganglion Blocks. In: Manchikanti, L., Kaye, A., Falco, F., Hirsch, J. (eds) Essentials of Interventional Techniques in Managing Chronic Pain. Springer, Cham. https://doi.org/10.1007/978-3-319-60361-2_33
Download citation
DOI: https://doi.org/10.1007/978-3-319-60361-2_33
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-60359-9
Online ISBN: 978-3-319-60361-2
eBook Packages: MedicineMedicine (R0)