
Abstract
Hematopoietic stem cell transplantation (HSCT) has significantly modified the natural history of many malignant and non-malignant disorders occurring in pediatric patients. In particular, allogeneic HSCT still represents the treatment of choice for life-threatening conditions, such as primary immune deficiencies or high-risk/relapsed leukemia, or the more effective option to improve the quality of life of patients with hemoglobinopathies. Continuous advances in transplantation outcomes achieved through the past three to four decades have led to the progressive expansion of the indications for HSCT, which is now used with success in several malignant and non-malignant disorders.
Since 2010, more than 30,000 transplants have been reported each year to the European Group for Blood and Marrow Transplantation (EBMT), with a record number of 40,829 HSCTs, in 36,469 patients, reported for the 2014 EBMT activity survey (16,946 allogeneic and 23,883 autologous HSCTs). Of the 656 currently active institutions, 107 (16%) are dedicated pediatric transplant centers and 118 centers (18%) perform HSCTs in both adults and children. These findings indicate that transplantation programs reserved for children must be implemented for those centers willing to take care of the pediatric population of patients. The number of HSCTs increases every year, with a continuous expansion of the use of human leucocyte antigen (HLA)-haploidentical transplantation, a slower increment for unrelated donor HSCTs, and a progressive reduction in cord blood use.
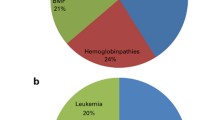
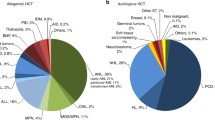
The main indications for allogeneic HSCT in the pediatric age group reported to the EBMT during the 2012 activity survey included acute lymphoblastic leukemia (26%) and primary immune-deficiencies (16%), while solid tumors (66%, in particular neuroblastoma) and lymphomas (15%) were the main indications for autologous HSCT.
Access provided by CONRICYT-eBooks. Download chapter PDF
Similar content being viewed by others

Keywords
- Hematopoietic stem cell transplantation
- Indications
- Children
- Leukemia
- Myelodysplastic syndromes
- Lymphoma
- Immune deficiencies
- Hemoglobinopathies
- Bone marrow failure syndromes
Introduction
The past few years have seen dramatic changes in the field of pediatric hemato-oncology, due to both significant advances in transplantation techniques and the introduction of new targeted therapies, thus modifying the position of hematopoietic stem cell transplantation (HSCT) in the therapeutic armamentarium for childhood hematologic malignancies.
Guidelines on the indications for allogeneic (allo-HSCT) and autologous HSCT (auto-HSCT) have been released by the American Society for Blood and Marrow Transplantation (ASBMT) [1] and the European Society for Blood and Marrow Transplantation (EBMT) [2] (Table 6.1).
Hematological Malignancies
Acute Lymphoblastic Leukemia (ALL)
Current frontline chemotherapy protocols for children with newly diagnosed acute lymphoblastic leukemia (ALL) can now cure more than 80% of patients [3]. Nonetheless, for subsets of children with high-risk (HR) features, identified by poor early response to therapy and/or genetic characteristics of leukemia cells, as well as for patients who experience disease relapse, outcomes are significantly worse.
The therapeutic advantage of allo-HSCT as a post-remission/consolidation strategy for these patients lies not only in the possibility to administer a more intensive treatment during the conditioning regimen, but also in the antileukemia alloreactions mediated by the graft.
Indications for HSCT in First Complete Remission (CR1)
The role of HSCT as a consolidation strategy in the frontline treatment of pediatric ALL must be considered in the context of a risk-stratified approach, based upon prognostic factors that can drive treatment intensity, with the aim of optimizing outcomes, while reducing unnecessary toxicities. The definition of these prognostic factors (namely, cytogenetic/molecular abnormalities at diagnosis and the response to induction treatment) is the result of the remarkable knowledge gathered from a series of large-scale analyses conducted by international cooperative groups.
HSCT in children with ALL in CR1 is currently reserved for subsets of patients with HR features.
In 2005, the International Berlin-Frankfurt-Münster (BFM) Study Group and the Pediatric Working Party of the EBMT Group reported the results of a cooperative prospective study comparing chemotherapy versus allo-HSCT from a human leucocyte antigen HLA–matched family donor (MFD) for very-HR childhood ALL in CR1, defined by the presence of at least one of the following criteria: (1) failure to achieve post-induction CR; (2) t(9;22) or t(4;11) clonal abnormality; (3) poor response to a 7-day prednisone prephase, associated with T-immunophenotype, white blood cell count (WBC) of 100×109/L or greater, or both. Five-year disease-free survival (DFS) was 40.6% in children allocated to chemotherapy and 56.7% in those given HSCT (p=0.02). The 5-year overall survival (OS) estimate in children assigned to chemotherapy or HSCT was 50.1% and 56.4%, respectively (p=0.12) [4].
A large prospective clinical trial has demonstrated that standardized quantitative assessment of minimal residual disease (MRD), using quantitative polymerase chain reaction (PCR) analysis of immunoglobulin gene rearrangements, measured at two time points (TPs) during induction treatment (TP1: day 33; TP2: day 78), can provide risk stratification of children with B-cell precursor (BCP) ALL and affect the choice of post-induction treatment [5]. Patients were considered MRD standard-risk (SR) if negative for MRD at both time points; MRD intermediate-risk (IR) if positive either at day 33 or day 78 and <10−3 leukemic cells at day 78; and MRD HR if positive ≥10−3 leukemic cells at day 78. In the multivariate analysis, PCR-MRD was observed to be the most relevant factor for discriminating prognosis. The 5-year event-free survival (EFS) estimates for MRD-SR, MRD-IR, and MRD-HR patients were 92.3%, 77.6%, and 50.1%, respectively, with 5-year OS probabilities of 97.8%, 93.4%, and 60.8%, respectively. High levels of MRD at TP2 were predictive of poor outcome (5-year EFS<50%). Fast clearance of MRD was associated with a favorable prognosis independently of non-MRD-related risk features, suggesting that, in patients undergoing relatively intensive treatment, if the MRD response is favorable, HSCT may not be indicated, even in the presence of any other combination of risk factors. On the other hand, for patients with a poor MRD response (i.e., MRD ≥10−3 leukemic cells after 2months of therapy) despite favorable non-MRD risk criteria, treatment intensification with HSCT may be indicated to compensate for the MRD-derived high risk of relapse.
The outcome of the cohort of HR patients enrolled in the Associazione Italiana Ematologia e Oncologia Pediatrica (AIEOP)-BFM ALL2000 study has been recently reported [6]. The statistical comparison of HSCT versus chemotherapy, accounting for waiting time to transplantation, did not show a significant advantage for HSCT over chemotherapy in terms of DFS. Nonetheless, in the larger subgroup of patients (subgroup 2), characterized by MRD-HR ≥5×10−4 and <5×10−3 leukemic cells at TP2 or by the presence of t(4;11) and prednisone good response, the initial advantage of chemotherapy changed to a disadvantage in favor of HSCT as time increased, due to late relapses after chemotherapy. Patients with T-cell lineage ALL belonging to subgroups 2 and 3 (MRD-HR ≥5×10−3 leukemic cells at TP2 or no remission at day +33 or the presence of t(4;11) and poor prednisone response) seemed to benefit from HSCT in terms of both DFS and OS.
The current approach of the AIEOP-BFM treatment scheme is to emphasize the role of MRD kinetics in the choice of the HSCT strategy in CR1 (see also Table 6.2).
Distinct mention needs to be made of two particular conditions:
-
BCR/ABL-positive ALL with poor early response.
-
ALL diagnosed within the first 12months of life (“infant ALL”) harboring rearrangements of the mixed-lineage-leukemia (MLL) gene.
In the pre-tyrosine kinase inhibitor (TKI) era, the prognosis of BCR/ABL-positive ALL was dismal, with low survival rates even with the combination of chemotherapy and HSCT. The introduction of TKIs into HR ALL chemotherapy backbones deeply modified the history of BCR/ABL-positive ALL.
In 2009, the Children’s Oncology Group (COG) reported data on the use of imatinib, progressively increased in five patient cohorts from 42 (cohort 1) to 280 continuous days (cohort 5), combined with an intensive chemotherapy regimen, in 92 BCR/ABL-positive ALL patients aged 1–21years. The addition of imatinib improved the outcome in cohort 5 patients, who achieved a 3-year EFS of 80%, higher than that of historical controls (35%; p<0.0001) and comparable to that of MFD or HLA-matched unrelated donor (MUD)-HSCT recipients [7].
In 2012, the results of a large collaborative European trial (EsPhALL) were reported [8]. Patients were classified as good risk or poor risk according to early response to induction treatment. Allo-HSCT was recommended for all poor-risk patients, from any type of donor, and for good-risk patients with any genotype-matched donor, and was performed in CR1 in 137 out of 178 (77%) patients. In both the good- and poor-risk groups, the outcomes of patients given imatinib without transplantation appeared to be poorer than those of HSCT recipients.
The current approach in the treatment of Philadelphia chromosome (Ph)-positive ALL emphasizes MRD monitoring in the therapeutic decision-making process . An ongoing combined follow-up study (ClinicalTrials.gov Identifier: NCT01460160), assessing the effect of earlier, continuous exposure to dasatinib, is pursuing the transplant approach in CR1 only in patients who fail to meet predefined MRD criteria and who have an HLA-matched donor.
The prognosis of infant ALL is still relatively poor if compared with that of older children with ALL, achieving EFS probabilities of about 40–50% with current therapies [9]. Treatment protocols developed in the past 10–15years have been investigating strategies to improve outcomes, such as treatment intensification with hybrid protocols including both lymphoblastic- and myeloid-oriented regimens, or the use of HSCT in CR1 [9, 10]. The potential benefits of HSCT for treating patients in this extremely vulnerable age group must be carefully weighed against the risk of long-term effects of the conditioning regimen on growth and development, requiring us to limit the transplant indication to infants with a poor probability of maintaining remission with chemotherapy alone.
In infants with MLL-positive ALL, a significant difference in DFS between patients receiving HSCT and those given chemotherapy alone was reported by the Interfant-99 Study Group. Furthermore, in the subgroup of infants younger than 6months and with either prednisone-poor response or leukocytes≥300×109cells/L, HSCT was associated with a 64% reduction in the risk of failure resulting from relapse or death in CR, while in the remaining patients, no advantage for HSCT over chemotherapy alone was observed [11].
The current International Collaborative Treatment Protocol for Infants (Interfant06; ClinicalTrials.gov Identifier: NCT00550992) identifies three risk groups, based upon MLL status, age, and WBC at diagnosis/prednisone response. All HR patients (infants with MLL rearrangement, age<6months, and either WBC>300×109/L or prednisone-poor response) are considered eligible for HSCT, whereas in the MR group (remaining MLL-rearranged patients) HSCT is indicated only in those with MRD level>10−4 leukemic cells at the end of consolidation.
Indications for HSCT in Second (CR2) or Subsequent Complete Remission
While the prognosis of newly diagnosed childhood ALL has dramatically improved, the outcome of children with relapsed ALL remains unsatisfactory. At relapse, about 30–50% of the children can be rescued with high-dose chemotherapy regimens, in most cases followed by allo-HSCT.
Factors identified to be predictors of outcome in relapsed ALL, and thus critical in the identification of patients who can be rescued with chemotherapy alone and those in need of allo-HSCT, are the time to relapse (very early, early, or late), the site of relapse (isolated bone marrow [BM], combined, or isolated extramedullary relapse), and the immunological lineage of the disease (BCP vs. T-lineage ALL) [12]. Combining these risk factors, a classification into four different risk groups has been proposed to stratify patients with relapsed ALL in order to deliver risk-adapted treatments. Details of this classification , together with its prognostic impact, are reported in Table 6.3.
Allo-HSCT from an MFD is able to guarantee a higher EFS probability in comparison to that achieved with second-line chemotherapy [13]. Some studies suggested that the advantage of HSCT over chemotherapy alone could be limited to specific subgroups, e.g., patients with HR relapse (S3/4 group) or IR relapse [14], or patients experiencing disease recurrence within 36months from diagnosis and receiving a total body irradiation-based conditioning regimen [15].
In patients with a standard risk profile (SR or S1/2), HSCT should be offered to those with BM involvement and MRD poor response after salvage induction therapy.
Thanks to the dramatic advances achieved in the field of allo-HSCT, outcomes after MUD-HSCT now approach those obtained in the MFD setting [16]. A matched-pair analysis from the BFM group, comparing MUD-HSCT with chemotherapy for children with ALL in CR2, documented a significantly higher EFS probability for the HR subgroup (44% vs. 0%), but not for IR patients (39% vs. 49%) given HSCT [17].
Current outcomes after umbilical cord blood transplantation (UCBT) have been observed to be similar to those obtained with unrelated BM grafts [18]. A retrospective analysis of children with ALL given unrelated UCBT reported to the Eurocord Registry documented a 4-year EFS of 44%, with high levels of pre-HSCT MRD predicting an increased risk of relapse [19].
The significant advances also achieved in the haploidentical setting have significantly broadened the applicability of HSCT, with outcomes currently approaching those obtained in the matched-donor setting.
In patients with ALL in CR3, the use of sole chemotherapy is associated with a very high risk of subsequent relapse; however, it has to be mentioned that allo-HSCT can also result in a considerable risk of transplant-related mortality (TRM), due to the pre-existing cumulative treatment toxicity.
Acute Myeloid Leukemia (AML)
The past two decades have seen a significant improvement in the outcomes of children with newly diagnosed acute myeloid leukemia (AML) [20], as a result of multiple factors, including advances in supportive care, progressive acquisitions of cytogenetic/molecular markers that have refined patient risk stratification, and the broad use of HSCT as consolidation strategy [21].
As in ALL, the therapeutic potential of HSCT results from both the possibility of delivering an intensive treatment before the allograft and the immunologic effect of the graft towards residual AML.
Indications for HSCT in First Complete Remission (CR1)
Allo-HSCT has been shown to be the most effective post-remission therapy for children with AML in CR1 when an MFD is available, in particular in patients with HR features [21], in whom transplantation is able to lower the relapse incidence to an extent comparable to that in SR children [22]. Thanks to the introduction of high-resolution HLA-typing, allowing a dramatic improvement in outcomes after transplantation from unrelated volunteers, indications for MUD-HSCT now partially coincide with those for MFD-HSCT.
In protocols in which the sole indication for HSCT was the availability of an MFD, a higher DFS was documented in patients transplanted in CR1, in comparison with patients receiving sole chemotherapy, without any difference in OS [23, 24].
More recently, a risk-stratified approach is being used, and candidates for HSCT in most current cooperative protocols are identified by the presence of HR features (i.e., unfavorable cytogenetic/molecular characteristics of leukemia cells and/or poor MRD clearance during induction therapy) [20].
Indications for HSCT in pediatric AML in CR1 are summarized in Table 6.4.
Genetic characterization of AML blast cells represents a major criterion for risk assessment at diagnosis, as first documented by the Medical Research Council (MRC) AML 10 trial [34].
Core-binding factor abnormalities , such as t(8;21) or inv.(16), identified a group of patients with a relatively favorable prognosis, while in patients lacking these favorable changes, the presence of a complex karyotype, monosomy 5, del(5q), monosomy 7, or abnormalities of 3q was found to predict a poor outcome.
More recently, other cytogenetic/molecular prognostic markers were identified [25]. In the favorable group, t(1;11)(q21;q23), normal karyotype with NPM1 mutation, and double mutant CEBPA were reported. Among adverse cytogenetic features, the following abnormalities have been associated with poor prognosis: del(7q); KMT2A (MLL) aberrations, excluding t(9;11)(p21;q23) and t(11;19)(q23;p13), t(9;22)(q34;q11), −17; and abnormalities of 12p, t(6;9), t(7;12), del(12p). A very poor outcome has been reported in the presence of the NUP98/NSD1 fusion gene, often associated with Fms-like tyrosine kinase 3 (FLT3)-internal tandem duplication (ITD) [35].
Considering that morphological CR is achieved in more 90% of children after induction therapy, but that relapse occurs in 30–40% of patients, the monitoring of MRD during treatment may allow the identification of patients at higher risk of relapse. A benefit of HSCT compared with chemotherapy alone has been reported in patients with poor MRD clearance, in particular when MRD levels remain above 1% after the first induction course [33]. For this reason, MRD monitoring has been included in many current protocols for the treatment of newly diagnosed pediatric AML, in order to refine patient stratification to receive HSCT in CR1.
The outcomes of children with HR-AML in CR1 given either auto- or allo-HSCT (based on the availability of an MFD) in the AIEOP AML 2002/01 Study Protocol were recently reported. Patients with M7 FAB subtype, complex karyotype or FLT3-ITD, were eligible for HSCT from alternative donors. The 8-year probability of DFS was 73.8% for recipients of MFD allografts, while for patients given MUD-HSCT, DFS was 75.5% in BM recipients, 53% in peripheral blood stem cell (PBSC) recipients, and 92.3% when UCB cells were employed (overall p=0.0035) [36].
Indications for HSCT in Second (CR2) or Subsequent Complete Remission
Allo-HSCT represents the best chance of cure in children with AML in CR2. Patients with favorable cytogenetic/molecular characteristics, long duration of CR1, not receiving HSCT in CR1, and with good response to reinduction therapy have a higher probability of being rescued by transplantation in CR2 [37].
Patients not given HSCT in CR1 and who receive HSCT in CR2 have a 5-year OS approaching 60%, whereas in those relapsing after HSCT performed in CR1, poor outcomes have been reported [38].
Acute Promyelocytic Leukemia (APL)
Given the excellent results obtained since the introduction of all-transretinoic acid (ATRA) in the treatment of APL, HSCT is currently not indicated in CR1. In patients with relapsed/refractory APL, the current role of HSCT as post-remission/consolidation strategy is controversial, as most reports of HSCT for APL in CR2 were published before the introduction of arsenic trioxide (ATO). Furthermore, as relapse incidence is very low in the ATRA and ATO era, randomized trials to compare different consolidation approaches in CR2 appear hardly feasible.
Experience with HSCT in treating pediatric relapsed APL is limited, the majority of data having been obtained from small retrospective studies. Data from the largest published series documented a 5-year EFS in the order of 70% for both auto- and allo-HSCT, with an incidence of TRM after auto- and allo-HSCT of 0% and 19%, respectively, all treatment-related deaths occurring in the early study period, before 1996. Relapse occurred in 27% of autografted patients and 10% of allo-HSCT recipients [39]. Even though the success of allo-HSCT is hampered by a higher risk of TRM, if compared with auto-HSCT, its use can provide a lower relapse incidence, probably due to the Graft versus Leukemia (GvL) potential of the donor graft against residual APL.
An expert panel of members from the COG and the International BFM Study Group recently published recommendations for the management of relapsed and refractory childhood APL. The authors suggest considering allo-HSCT in patients with prior ATO exposure, in patients with short duration of CR1, in patients with primary refractory disease , in those in second or further relapse, or those not achieving molecular CR after four salvage cycles. Auto-HSCT appears to be a reasonable option for treatment consolidation for ATO-naïve patients who achieve a second molecular CR after four salvage cycles [40].
Chronic Myeloid Leukaemia (CML)
In the pre-TKI era, allogeneic HSCT was the standard of care for children with Ph+ chronic myeloid leukemia (CML) . The introduction of TKIs into the treatment of Ph+CML deeply modified the history of the disease, leading to a significant decrease in the use of HSCT. Nonetheless, based on currently available data, no certain evidence of the complete eradication of the Ph+clone by prolonged treatment with TKIs exists. Furthermore, the long-life expectancy of pediatric patients, entailing the need for potentially life-long treatment, renders the alternative choice between TKIs and transplantation controversial.
Current algorithms for the management of children with newly diagnosed CML in chronic phase (CP) include frontline treatment with hydroxyurea and a first-generation TKI, with a switch to a second-generation TKI in cases of failure to obtain an acceptable response. Allo-HSCT is reserved for patients who experience progression or relapse or persistently high levels of the BCR/ABL fusion transcript on second-generation TKI treatment. For children presenting with CML in accelerated phase or blast crisis, initiation of TKI therapy is recommended, followed by allo-HSCT once a reversion to chronic phase has been obtained [41].
Myelodysplastic Syndromes and Myeloproliferative Neoplasms
Myelodysplastic syndromes (MDSs) encompass a group of clonal disorders of HSCs and their precursors, characterized by peripheral cytopenia, dysplasia in one of the myeloid lineages with ineffective hematopoiesis, and a variable propensity to evolve towards acute leukemia. The classification of pediatric MDSs includes low-grade forms (refractory cytopenia of childhood; RCC) and advanced MDSs; namely, refractory anemia with excess blasts (RAEB) and RAEB in transformation (RAEB-t). MDSs are rare in children, accounting for about 5% of hematologic malignancies, and they can be part of the natural evolution of inherited BM failure syndromes.
As childhood MDSs show relatively poor responses to conventional chemotherapy [42] and pre-transplant chemotherapy is not associated with improved outcomes [43], HSCT should be considered early in the course of the disease. Commonly accepted indications include advanced MDSs (i.e., RAEB and RAEB-t), MDS secondary to chemo-radiotherapy, and RCC associated with either cytogenetic anomalies (e.g., monosomy 7, complex karyotype) or severe neutropenia or transfusion dependence [43].
The results of the European Working Group on Childhood MDS (MDS) 98 study, which enrolled 97 patients with RAEB, RAEB-t, and myelodysplasia-related AML given HSCT from an MFD (N=39), MUD (N=57), or alternative family donor (N=1), were recently reported. The 5-year probability of OS was 63%, with a 21% cumulative incidence of TRM and relapse. Factors associated with increased TRM were age at HSCT >12years, time from diagnosis to HSCT longer than 4months, and occurrence of acute or extensive chronic graft-versus-host disease (GVH-D) [43].
Monosomy of chromosome 7 or partial deletion involving its long arm [del(7q)] are recurrent chromosomal aberrations in RCC and have been reported to be associated with a significantly higher probability of progression to advanced MDS [44]. Moreover, a significantly better probability of survival has been shown in patients transplanted before evolution to advanced MDS in comparison to patients experiencing disease progression (76% vs. 36%, respectively, p=0.03) [44].
For this reason, children with RCC and monosomy 7, del(7q), or a complex karyotype should be offered transplantation from either an MFD or a MUD early in the course of the disease. Conversely, children with RCC and normal karyotype or chromosomal abnormalities other than monosomy 7, del(7q) or a complex karyotype may experience a long, stable disease course, allowing a “watch and wait” approach. By virtue of the low TRM rates of MFD-HSCT, transplantation may be recommended for children with an available HLA-identical sibling. For patients lacking such a donor but experiencing transfusion dependence, severe neutropenia, or infections, transplantation from a MUD should be offered. A valid alternative is represented by immunosuppressive therapy (IST), with cyclosporine, anti-thymocyte globulin (ATG), and steroids.
Juvenile myelomonocytic leukemia (JMML) is an aggressive clonal hematopoietic disorder of infancy and early childhood, with features straddling myeloproliferative neoplasms and MDS. Approximately 90% of children with JMML carry either somatic or germline mutations in genes involved in the RAS/mitogen-activated protein kinase (MAPK) pathway, such as PTPN11, NRAS, KRAS, CBL, or NF1. Although spontaneous resolution has been rarely described, allogeneic HSCT remains the treatment of choice for most JMML patients, being able to cure more than 50% of such patients. Prompt HSCT is recommended for all children with JMML and NF-1, somatic PTPN-11 mutations, and K-RAS mutations, and for the majority of children with somatic N-RAS mutations (Table 6.5). Conversely, because spontaneous regression of myeloproliferation has been observed in children with germline CBL mutations, as well as in Noonan syndrome patients, a “watch and wait” strategy is appropriate in these cases [45].
Disease recurrence is the main cause of treatment failure in patients given allogeneic HSCT for JMML. Thus, strategies aimed at optimizing the GvL effect, such as, whenever possible, a rapid tapering and discontinuation of GVH-D prophylaxis after transplantation, are recommended in children with JMML.
Pediatric Lymphomas
Given the excellent outcomes achieved with current risk-adapted first-line therapy for both pediatric Hodgkin lymphoma (HL) and non-Hodgkin lymphomas (NHLs), there is no indication for HSCT during frontline treatment for either of these entities [46]. However, primary refractory disease or relapse can occur in up to 10–15% of children, for whom a dismal prognosis has been reported [47]. For those patients, both autologous and allogeneic HSCT have become part of salvage therapy strategies.
Data on children with lymphoma treated with high-dose chemotherapy followed by autologous stem cell rescue, as well as data on allo-HSCT, are limited to small case series, with heterogeneous pre-transplant chemotherapy and conditioning regimens. Historically, auto-HSCT has been preferred to allo-HSCT because of easier stem cell availability and a lower rate of TRM [46]. In a large EBMT registry-based analysis, including both pediatric and adult patients, and comparing allo-HSCT with auto-HSCT, the advantage of allo-HSCT, in terms of disease recurrence , was counterbalanced by a high incidence of treatment-associated complications, resulting in a higher OS after auto-HSCT [48]. Nonetheless, with recent advances in allo-HSCT techniques (including high-resolution HLA-typing, improvements in supportive care , and the implementation of less toxic conditioning regimens), this approach is being increasingly used in children with lymphomas.
Hodgkin Lymphoma
In adult patients, high-dose chemotherapy followed by the infusion of autologous HSCs has been shown to be superior to chemotherapy alone in randomized controlled trials including relapsed and primary refractory HL [49]. The improvement in progression-free survival (PFS) was particularly evident in patients with disease recurrence within 1year after the end of treatment (41% for auto-HSCT vs. 12% for chemotherapy alone, p=0.008), but was still significant for patients with later relapse (75% vs. 44%, p=0.025). Based on these results, auto-HSCT has also been increasingly used as salvage therapy in children with poor-risk features. Indeed, even among patients with HR HL with a first relapse, salvage therapies including auto-HSCT can result in long-term cure in approximately 50% of cases [50].
In a recent retrospective analysis from the Center for International Blood and Marrow Transplant Research (CIMBTR) on 606 Childhood, Adolescent and Young Adult (CAYA) patients, performance status at the time of HSCT, no extranodal involvement, and chemosensitivity were associated with a significantly improved PFS, while patients with time from diagnosis to first relapse shorter than 1year had a significantly inferior PFS [51].
Due to a reported higher rate of TRM in allo-HSCT than in auto-HSCT [48], the role of allo-HSCT in HL is still controversial, both in adults and the CAYA population. However, a meta-analysis showed a reduced (up to 5–10% lower) non-relapse mortality (NRM) with increased PFS and OS (up to 15–20% higher) in recent studies (i.e., those starting accrual in 2000 or later) [52]. The largest study reporting data for children and adolescents given allo-HSCT showed an NRM of 21%, with comparable results after reduced-intensity conditioning (RIC) or a myeloablative conditioning (MAC) regimen [53]. Relapse incidence was increased after RIC compared with MAC, thus resulting in a better PFS for patients given MAC (40 vs. 30%, p=0.02). Of note, while no difference in outcome was observed between MFD and MUD-HSCT, the use of mismatched donors significantly reduced PFS after HSCT. Unmanipulated haploidentical BM transplantation with post-transplantation cyclophosphamide showed good results in patients with advanced HL [54].
Non-Hodgkin Lymphoma (NHL)
In children and adolescents the four most frequent subtypes of NHL are Burkitt (BL), lymphoblastic (LBL), diffuse large B cell (DLBCL), and anaplastic large cell lymphoma (ALCL). Despite very good results obtained with first-line therapies, with long-term EFS up to 90%, depending on histological subtype [55], the prognosis of relapsed or refractory NHL is dismal, with the only exception being ALCL [56]. In adults, auto-HSCT has been proven to be superior to chemotherapy alone for the treatment of relapsed NHL [57], but no clear indications exist for selecting autologous or allogeneic HSCT.
The role of auto- and allo-HSCT is also still unclear in children with NHL. A recent registry-based study examined the role of HSCT in 182 patients affected by BL, LBL, DLBCL, and ALCL, given autologous (N=90) or allogeneic HSCT (N=92) from an MFD (N=43) or a MUD (N=49) [58]. After adjusting for disease status, no difference in 5-year EFS was observed between allo- and auto-HSCT for BL, DLBCL, or ALCL, while the outcome of relapsed/refractory LBL was superior after allo-HSCT [58].
A promising approach is the combination of MAC auto-HSCT, followed by a RIC allo-HSCT, which has been reported to allow a 10-year EFS of 70% [59].
Some children with NHL have a pre-existing condition predisposing to lymphoma (e.g., cancer predisposition syndromes or primary immune deficiencies). Because these patients suffer from increased treatment-related toxicities (leading to an inferior survival rate), special vigilance should be exerted when they are receiving chemotherapy or undergoing auto- or allo-HSCT [60].
Non-malignant Disorders
Primary Immune Deficiencies
Since the first successful attempt was made to cure primary immune deficiencies (PIDs) with HSCT, many significant changes have been made in transplant indications and techniques for these disorders. While the management of some PIDs is still based on conservative approaches, for other disorders HSCT is now becoming a widely accepted treatment strategy.
Taking into consideration the wide clinical heterogeneity of patients, the consensus of the EBMT and the European Society for Immunodeficiencies (ESID) is that each case should be carefully evaluated for indications and transplant strategy, in a center with significant experience [61].
Apart from severe combined immune deficiencies (SCIDs), for which there is a clear recommendation for HSCT [62], transplantat indications for non-SCID PIDs are being debated. Among the non-SCID PIDs, successful HSCTs have been performed in Wiskott-Aldrich syndrome (WAS) , chronic granulomatous disease (CGD) , hemophagocytic syndromes (such as hemophagocytic lymphohistiocytosis [HLH] and X-linked lymphoproliferative syndromes [XLP1 and XLP2], CD40-ligand deficiency, DNA repair disorders (such as ligase 4 deficiency, Cernunnos syndrome, and Nijmegen breakage syndrome), DOCK8 deficiency, and immunodysregulation polyendocrinopathy enteropathy X-linked (IPEX) syndrome [63].
Until recent years, the availability of an HLA-identical related donor was one of the main factors influencing the choice of transplantation in PIDs. However, the introduction of high-resolution molecular HLA-typing [64], together with the optimization of graft manipulation techniques, has broadened transplant access for these disorders [65]. Prognosis after HSCT for PIDs (influencing the decision to offer a transplantation) is dependent on the molecular defect at the basis of the disorder, disease status, donor type, HSC source, and the conditioning regimen [66].
Further, the increasing interest in gene therapy for the cure of PIDs is likely to render the therapeutic decision-making process and the definition of clear indications for HSCT more complex in coming years.
Hemoglobinopathies Disorders
The past 30 years have witnessed significant advances in supportive care and interventional therapies for thalassemia major (TM) and sickle cell disease (SCD). This has led to improved quality of life and survival rates for TM and SCD patients in many high-income countries, but has simultaneously brought about new medical needs associated with the progressive development of chronic disease and/or treatment-related complications. Conversely, in developing countries these disorders still represent a relevant cause of childhood mortality.
While the recent advances in gene-therapy approaches are likely to allow the forthcoming translation of promising preclinical and clinical evidence into a viable reality, at present allogeneic HSCT is the only consolidated possibility of definitive cure for hemoglobinopathies.
The widest experience of HSCT in these diseases has been obtained using BM cells harvested from an HLA-identical sibling donor. In this setting, major recently published studies report OS and DFS probabilities of over 90% and 85%, respectively, for TM, and more than 90% and 80%, respectively, for SCD [67, 68].
In 2014, a consensus document with recommendations on current HSCT strategies for TM and SCD was published by an expert panel selected by the EBMT Paediatric Diseases Working Party and Inborn Error Working Party [69].
Thalassemia Major
As indicated by the Pesaro experience [70], the disease status at the time of transplantation, and thus the timing of HSCT, appear to be critical to outcome in TM. Indeed, the identification and the adoption, in clinical practice, of three risk classes identified on the basis of three criteria, namely, hepatomegaly, liver fibrosis, and regularity of iron chelation, have been shown to influence HSCT outcomes. [70].
The EBMT recently reported data from a retrospective study of 1493 TM patients given allo-HSCT, with the best results observed in recipients of MFD-HSCT, in whom 2-year OS and EFS probabilities were 91% and 83%, respectively, while the 2-year estimates of both OS and EFS in the MUD-HSCT subgroup were 77%. A significant threshold age of 14years for optimal results was identified [71].
Based on these considerations, TM children with a suitable, unaffected, HLA-identical sibling should be offered HSCT at an early disease stage, before the development of treatment-related complications and/or tissue damage associated with iron overload. Unfortunately, for the majority of patients, a suitable MFD is not available, leading to the need for alternative transplantation strategies.
Thanks to the dramatic advances achieved in the field of allogeneic HSCT, outcomes after MUD-HSCT in TM now approach those obtained in the MFD setting, provided that the donor selection is performed using high-resolution molecular typing for HLA class I and II loci and according to strict criteria of donor/recipient compatibility (i.e., full match or single allelic disparity for HLA-A, B, C, DRB1, and DQB1 loci). Moreover, a significantly increased risk of graft rejection has been described in the presence of non-permissive HLA-DPB1 mismatches in the host-versus-graft (HvG) direction, with a lower probability of DFS in patients given HSCT from donors with at least one HLA-DPB1 non-permissive disparity [72].
Unrelated UCBT holds the potential to broaden the access to HSCT t o patients lacking an MFD or MUD, and this procedure appears appealing in non-malignant diseases by virtue of a suggested lower risk of GVH-D. Nevertheless, discordant results have been reported in the experience with unrelated UCBT in TM, with high rates of graft failure, largely attributable to low HSC content in cord blood units (CBUs) [73]. Based on currently available experience, unrelated UCBT appears to be a suboptimal strategy in TM, unless it is performed in the context of clinical trials aimed at exploring specific treatment platforms of ex-vivo UCB graft manipulation.
Although experience with haploidentical HSCT in children with TM is limited and this type of allograft is not routinely recommended, currently explored platforms hold the potential to extend the access to HSCT to the proportion of TM patients lacking both an HLA-matched related and unrelated donor [65, 74].
Sickle Cell Disease
While transfusion dependency is currently considered an indication for HSCT in TM, a general agreement on indications and timing for HSCT in SCD is less defined.
Indications for allogeneic HSCT in SCD include: (1) stroke or central nervous system event lasting longer than 24h, acute chest syndrome with recurrent hospitalizations or previous exchange transfusions; (2) recurrent vaso-occlusive pain (more than two episodes per year over several years) or recurrent priapism; (3) impaired neuropsychological function with abnormal cerebral magnetic resonance imaging (MRI) scan; (4) stage I or II sickle lung disease; (5) sickle nephropathy (moderate or severe proteinuria or a glomerular filtration rate 30–50% of the predicted normal value); (6) bilateral proliferative retinopathy with major visual impairment in at least one eye; (7) osteonecrosis of multiple joints; and (8) red-cell alloimmunization during long-term transfusion therapy [69].
More recently, additional risk factors have been suggested and these are being considered in the evaluation of the risk/benefit ratio for transplantation in SCD (see also Table 6.6) [75].
A further aspect to mention is that donor-host hematopoietic mixed chimerism after HSCT is not a rare finding in patients with hemoglobinopathies. As documented for both TM and SCD, the development of stable mixed chimerism in non-malignant disorders maintains the potential to correct the phenotypic expression of the disease [76]. This observation has provided a rational basis for considering RIC regimens in patients with hemoglobinopathies, with the aim of promoting stable engraftment of at least a threshold fraction of donor cells, sufficient to correct the abnormal hemoglobin phenotype, while reducing toxicity.
Acquired Severe Aplastic Anemia
Acquired aplastic anemia is a disorder characterized by BM failure and peripheral blood pancytopenia, assumed to result from an immune-mediated destructive mechanism that may be triggered by environmental exposures. First-line allo-HSCT is considered the treatment of choice if an HLA-identical sibling donor is available. For patients lacking an MFD, IST consisting of ATG, cyclosporine, and steroids is employed as frontline treatment strategy.
HSCT from a well-matched unrelated donor is currently considered a rescue option for children who have failed IST, with OS and EFS approaching 80% and 70%, respectively [77].
The results of two recently reported retrospective studies suggest a potential benefit also of upfront HSCT from unrelated donors in children affected by severe aplastic anemia (SAA) [78, 79]. In the first analysis of 29 children given frontline MUD-HSCT, outcomes were similar to those observed in a historical control group given MFD-HSCT (2-year OS: 96% in the upfront MUD-HSCT group and 91% in the MFD-HSCT group, P=0.30; 2-year EFS 92% in the upfront MUD-HSCT group and 87% in the MFD-HSCT group, P=0.20) and superior to IST (OS 94%, P=0.68; EFS 40%, P=0.0001) and MUD-HSCT post-IST failure (OS 74%, P=0.02; EFS 74%, P=0.02). Similar outcomes were reported in 42 children and adolescents (estimated failure-free survival rate of the frontline HSCT group 91.3% vs. 30.7% in the frontline IST group, P<0.001).
Alternative options, such as UCBT [80] or haploidentical HSCT [81], may be considered in patients lacking a matched related or unrelated donor and failing IST.
Constitutional Bone Marrow Failure Syndromes
Fanconi Anemia
Fanconi anemia (FA) is a genetically and phenotypically heterogeneous disorder, variably characterized by congenital somatic abnormalities, BM failure, and predisposition to clonal disorders. HSCT currently represents the only possibility of cure, having the potential to correct the hematologic manifestations associated with FA, as well as to prevent/treat myeloid malignancies. Due to the peculiar chromosome fragility and hypersensitivity to DNA interstrand cross-linking agents that characterize this disorder, conditioning regimens that are specifically developed for FA patients are employed.
In the therapeutic decision-making process for patients with FA , multiple factors should be taken into consideration. Indeed, the risk of developing BM failure and hematologic malignancies increases with age, and a variety of factors, such as the recipient’s age, extent of prior treatments, and disease stage have been shown to negatively affect the outcome of HSCT [82].
Commonly accepted absolute indications for HSCT are severe BM failure with transfusion dependence, and clonal evolution to HR MDS (i.e., RCC with HR chromosomal abnormalities or advanced MDS) or AML. Relative indications that may lead to the choice of transplantation in the presence of an MFD can also be moderate isolated cytopenias with evidence of progression towards transfusion dependence and low-risk MDS (i.e., RCC with no chromosomal abnormalities or low-risk chromosomal abnormalities).
Dyskeratosis Congenita
Dyskeratosis congenita (DC) is an inherited disorder characterized by mucocutaneous abnormalities, BM failure, and predisposition to cancer, resulting from mutations in genes involved in telomere maintenance.
HSCT represents the only chance of definitive cure for the hematologic abnormalities associated with DC, but it is, unfortunately, associated with significant early and late morbidity. As in FA, due to the underlying defect in genome maintenance, RIC protocols are required for DC. Transplantation should be performed at centers experienced in treating DC, considering the risk of graft failure and early mortality, as well as long-term complications such as diffuse vasculitis and lung fibrosis.
Diamond-Blackfan Anemia
Diamond-Blackfan anemia (DBA) is a disorder associated with mutations in genes that encode for ribosomal proteins, clinically characterized by hypo-regenerative anemia with absent or decreased BM erythroid precursors, which may be associated with somatic abnormalities. Conservative therapy in DBA includes chronic transfusions and corticosteroids. HSCT may be offered to patients who develop transfusion-dependence or other cytopenias.
Data from the Diamond-Blackfan Anemia Registry of North America and AIEOP indicate OS probabilities of 72–74% after MFD- or MUD-HSCT, and 17% after HSCT from alternative donors [83, 84].
Considering the incomplete penetrance of DBA, disease-causing mutations may be present in subjects without an evident DBA phenotype, rendering genetic analysis of any potential related donor mandatory.
Severe Congenital Neutropenias and Inherited Thrombocytopenias
The category of severe congenital neutrope nias includes a variety of hematologic disorders characterized by severe neutropenia, with a high risk of developing severe and life-threatening bacterial infections from early infancy.
More than 90% of patients respond to treatment with recombinant human (rHu) granulocyte colony-stimulating factor (G-CSF), obtaining neutrophil counts higher than 1.0×109/L. Allogeneic HSCT remains the only currently available treatment for patients with severe congenital neutropenia (Kostmann disease ) refractory to rHuG-CSF or those who develop clonal evolution into MDS or leukemia [85].
HSCT also represents the only possibility of cure in congenital amegakaryocytic thrombocytopenia (CAMT) , an autosomal recessive disorder cau sed by mutations of the gene encoding for the thrombopoietin (TPO) receptor (c-MPL), clinically characterized by early-onset thrombocytopenia (at birth) with reduced or absent BM megakaryocytes, and eventual progression to BM failure [86].
Inborn Errors of Metabolism
Inborn errors of metabolism (IEMs) are disorders derived from the deficiency of enzymes that play a key role in metabolic pathways. The consequent progressive accumulation of toxic metabolites within different cells/tissues leads to multisystemic impairment. The observation that the enzymatic activity in deficient cells could be restored by mixing, in culture, normal cells and fibroblasts derived from patients affected by mucopolysaccharidoses, led to the first attempts at HSCT in this kind of IEM. Moreover, unlike in enzyme-replacement therapy, donor-derived monocytes are able to cross the blood-brain barrier, thus alleviating/arresting central nervous system damage.
To date, more than 2000 transplants have been perfor med worldwide in patients with IEMS, with results showing that not all IEMs can benefit from HSCT [87]. A possible partial explanation for this observation could lie in the fact that HSCT seems to induce a response only in some tissues, probably due to the suboptimal delivery of the target enzyme in non-responder tissues. In IEMs, the timing of transplantation appears to be critical for outcome, as late HSCT may be ineffective in preventing disease progression [88]. In particular, for patients who have already developed central nervous system involvement or those with advanced disease, HSCT is contra-indicated. The use of donors who carry the enzymatic defect is not recommended, because the delivery of the target enzyme in recipient tissues is suboptimal. The full-donor chimerism rate was found to be significantly higher in recipients of UCBT as compared with patients receiving either BM or peripheral blood transplantation.
Solid Tumors
Because of continuous improvements in multimodal therapy and supportive care, the outcomes of children with solid tumors have constantly improved in the past few decades. However, some of these tumors, although initially chemosensitive, have a dismal prognosis. Against this background, both auto- and allo-HSCT have been employed for the treatment of HR solid tumors [89], with the former strategy being the most widely used (only 446 allogeneic transplant procedures were registered at the EBMT until 2011). However, with the exception of neuroblastoma (for which randomized trials have been conducted, showing a clear advantage of auto-HSCT versus sole chemotherapy) [90], prospective trials are lacking. From registry data, the following findings can be inferred [91]:
-
Outcomes of HSCT performed during first-line treatment are significantly better than those observed after transplantation in relapsed patients.
-
Patients with good response at the time of transplantation (i.e., complete response, very good partial response, and partial response) have, not surprisingly, an improved outcome when compared with those with an unsatisfactory response.
-
Recent years have seen a trend towards a reduction of TRM.
-
Peripheral blood autologous stem cells represent the currently most often used HSC source.
-
Total body irradiation has shown no advantage for any of the solid tumor indications; however, busulfan coupled with melphalan increased survival in neuroblastoma and Ewing sarcoma.
Tumors for which there is a general indication for auto- or allo-HSCT are listed in Table 6.1.
References
Majhail NS, Farnia SH, Carpenter PA, et al. Indications for autologous and allogeneic hematopoietic cell transplantation: guidelines from the American Society for Blood and Marrow Transplantation. Biol Blood Marrow Transplant. 2015;21:1863–9.
Sureda A, Bader P, Cesaro S, et al. Indications for allo- and auto-SCT for haematological diseases, solid tumours and immune disorders: current practice in Europe, 2015. Bone Marrow Transplant. 2015;50:1037–56.
Moricke A, Zimmermann M, Reiter A, et al. Long-term results of five consecutive trials in childhood acute lymphoblastic leukemia performed by the ALL-BFM study group from 1981 to 2000. Leukemia. 2010;24:265–84.
Balduzzi A, Valsecchi MG, Uderzo C, et al. Chemotherapy versus allogeneic transplantation for very-high-risk childhood acute lymphoblastic leukaemia in first complete remission: comparison by genetic randomisation in an international prospective study. Lancet. 2005;366:635–42.
Conter V, Bartram CR, Valsecchi MG, et al. Molecular response to treatment redefines all prognostic factors in children and adolescents with B-cell precursor acute lymphoblastic leukemia: results in 3184 patients of the AIEOP-BFM ALL 2000 study. Blood. 2010;115:3206–14.
Conter V, Valsecchi MG, Parasole R, et al. Childhood high-risk acute lymphoblastic leukemia in first remission: results after chemotherapy or transplant from the AIEOP ALL 2000 study. Blood. 2014;123:1470–8.
Schultz KR, Bowman WP, Aledo A, et al. Improved early event-free survival with imatinib in Philadelphia chromosome-positive acute lymphoblastic leukemia: a Children’s Oncology Group study. J Clin Oncol. 2009;27:5175–81.
Biondi A, Schrappe M, De Lorenzo P, et al. Imatinib after induction for treatment of children and adolescents with Philadelphia-chromosome-positive acute lymphoblastic leukaemia (EsPhALL): a randomised, open-label, intergroup study. Lancet Oncol. 2012;13:936–45.
Pieters R, Schrappe M, De Lorenzo P, et al. A treatment protocol for infants younger than 1 year with acute lymphoblastic leukaemia (Interfant-99): an observational study and a multicentre randomised trial. Lancet. 2007;370:240–50.
Koh K, Tomizawa D, Moriya Saito A, et al. Early use of allogeneic hematopoietic stem cell transplantation for infants with MLL gene-rearrangement-positive acute lymphoblastic leukemia. Leukemia. 2015;29:290–6.
Mann G, Attarbaschi A, Schrappe M, et al. Improved outcome with hematopoietic stem cell transplantation in a poor prognostic subgroup of infants with mixed-lineage-leukemia (MLL)-rearranged acute lymphoblastic leukemia: results from the Interfant-99 Study. Blood. 2010;116:2644–50.
Locatelli F, Schrappe M, Bernardo ME, Rutella S. How I treat relapsed childhood acute lymphoblastic leukemia. Blood. 2012;120:2807–16.
Uderzo C, Valsecchi MG, Bacigalupo A, et al. Treatment of childhood acute lymphoblastic leukemia in second remission with allogeneic bone marrow transplantation and chemotherapy: ten-year experience of the Italian Bone Marrow Transplantation Group and the Italian Pediatric Hematology Oncology Association. J Clin Oncol. 1995;13:352–8.
Einsiedel HG, von Stackelberg A, Hartmann R, et al. Long-term outcome in children with relapsed ALL by risk-stratified salvage therapy: results of trial acute lymphoblastic leukemia-relapse study of the Berlin-Frankfurt-Munster Group 87. J Clin Oncol. 2005;23:7942–50.
Eapen M, Raetz E, Zhang MJ, et al. Outcomes after HLA-matched sibling transplantation or chemotherapy in children with B-precursor acute lymphoblastic leukemia in a second remission: a collaborative study of the Children’s Oncology Group and the Center for International Blood and Marrow Transplant Research. Blood. 2006;107:4961–7.
Dini G, Zecca M, Balduzzi A, et al. No difference in outcome between children and adolescents transplanted for acute lymphoblastic leukemia in second remission. Blood. 2011;118:6683–90.
Borgmann A, von Stackelberg A, Hartmann R, et al. Unrelated donor stem cell transplantation compared with chemotherapy for children with acute lymphoblastic leukemia in a second remission: a matched-pair analysis. Blood. 2003;101:3835–9.
Smith AR, Baker KS, Defor TE, Verneris MR, Wagner JE, Macmillan ML. Hematopoietic cell transplantation for children with acute lymphoblastic leukemia in second complete remission: similar outcomes in recipients of unrelated marrow and umbilical cord blood versus marrow from HLA matched sibling donors. Biol Blood Marrow Transplant. 2009;15:1086–93.
Ruggeri A, Michel G, Dalle JH, et al. Impact of pretransplant minimal residual disease after cord blood transplantation for childhood acute lymphoblastic leukemia in remission: an Eurocord, PDWP-EBMT analysis. Leukemia. 2012;26:2455–61.
Creutzig U, van den Heuvel-Eibrink MM, Gibson B, et al. Diagnosis and management of acute myeloid leukemia in children and adolescents: recommendations from an international expert panel. Blood. 2012;120:3187–205.
Klusmann JH, Reinhardt D, Zimmermann M, et al. The role of matched sibling donor allogeneic stem cell transplantation in pediatric high-risk acute myeloid leukemia: results from the AML-BFM 98 study. Haematologica. 2012;97:21–9.
Pession A, Masetti R, Rizzari C, et al. Results of the AIEOP AML 2002/01 multicenter prospective trial for the treatment of children with acute myeloid leukemia. Blood. 2013;122:170–8.
Lie SO, Abrahamsson J, Clausen N, et al. Treatment stratification based on initial in vivo response in acute myeloid leukaemia in children without Down’s syndrome: results of NOPHO-AML trials. Br J Haematol. 2003;122:217–25.
Woods WG, Neudorf S, Gold S, et al. A comparison of allogeneic bone marrow transplantation, autologous bone marrow transplantation, and aggressive chemotherapy in children with acute myeloid leukemia in remission. Blood. 2001;97:56–62.
Hasle H. A critical review of which children with acute myeloid leukaemia need stem cell procedures. Br J Haematol. 2014;166:23–33.
Creutzig U, Zimmermann M, Bourquin JP, et al. Randomized trial comparing liposomal daunorubicin with idarubicin as induction for pediatric acute myeloid leukemia: results from Study AML-BFM 2004. Blood. 2013;122:37–43.
Creutzig U, Zimmemarin M, Dworzak M, et al. Study AML-BFM 2004: improved survival in childhood acute myeloid leukemia without increased toxicity. Blood. 2010;116:83.
Canner J, Alonzo TA, Franklin J, et al. Differences in outcomes of newly diagnosed acute myeloid leukemia for adolescent/young adult and younger patients: a report from the Children’s Oncology Group. Cancer. 2013;119:4162–9.
Tsukimoto I, Tawa A, Horibe K, et al. Risk-stratified therapy and the intensive use of cytarabine improves the outcome in childhood acute myeloid leukemia: the AML99 trial from the Japanese Childhood AML Cooperative Study Group. J Clin Oncol. 2009;27:4007–13.
Perel Y, Auvrignon A, Leblanc T, et al. Treatment of childhood acute myeloblastic leukemia: dose intensification improves outcome and maintenance therapy is of no benefit--multicenter studies of the French LAME (Leucemie Aigue Myeloblastique Enfant) Cooperative Group. Leukemia. 2005;19:2082–9.
Gibson BE, Webb DK, Howman AJ, et al. Results of a randomized trial in children with acute myeloid leukaemia: Medical Research Council AML12 trial. Br J Haematol. 2011;155:366–76.
Hasle H, Abrahamsson J, Forestier E, et al. Gemtuzumab ozogamicin as postconsolidation therapy does not prevent relapse in children with AML: results from NOPHO-AML 2004. Blood. 2012;120:978–84.
Rubnitz JE, Inaba H, Dahl G, et al. Minimal residual disease-directed therapy for childhood acute myeloid leukaemia: results of the AML02 multicentre trial. Lancet Oncol. 2010;11:543–52.
Grimwade D, Walker H, Oliver F, et al. The importance of diagnostic cytogenetics on outcome in AML: analysis of 1,612 patients entered into the MRC AML 10 trial. The Medical Research Council Adult and Children’s Leukaemia Working Parties. Blood. 1998;92:2322–33.
Shiba N, Ichikawa H, Taki T, et al. NUP98-NSD1 gene fusion and its related gene expression signature are strongly associated with a poor prognosis in pediatric acute myeloid leukemia. Genes Chromosom Cancer. 2013;52:683–93.
Locatelli F, Masetti R, Rondelli R, et al. Outcome of children with high-risk acute myeloid leukemia given autologous or allogeneic hematopoietic cell transplantation in the AIEOP AML-2002/01 study. Bone Marrow Transplant. 2015;50:181–8.
Sander A, Zimmermann M, Dworzak M, et al. Consequent and intensified relapse therapy improved survival in pediatric AML: results of relapse treatment in 379 patients of three consecutive AML-BFM trials. Leukemia. 2010;24:1422–8.
Beier R, Albert MH, Bader P, et al. Allo-SCT using BU, CY and melphalan for children with AML in second CR. Bone Marrow Transplant. 2013;48:651–6.
Dvorak CC, Agarwal R, Dahl GV, Gregory JJ, Feusner JH. Hematopoietic stem cell transplant for pediatric acute promyelocytic leukemia. Biol Blood Marrow Transplant. 2008;14:824–30.
Abla O, Kutny MA, Testi AM, et al. Management of relapsed and refractory childhood acute promyelocytic leukaemia: recommendations from an international expert panel. Br J Haematol. 2016;175(4):588–601.
Andolina JR, Neudorf SM, Corey SJ. How I treat childhood CML. Blood. 2012;119:1821–30.
Woods WG, Barnard DR, Alonzo TA, et al. Prospective study of 90 children requiring treatment for juvenile myelomonocytic leukemia or myelodysplastic syndrome: a report from the Children’s Cancer Group. J Clin Oncol. 2002;20:434–40.
Strahm B, Nollke P, Zecca M, et al. Hematopoietic stem cell transplantation for advanced myelodysplastic syndrome in children: results of the EWOG-MDS 98 study. Leukemia. 2011;25:455–62.
Kardos G, Baumann I, Passmore SJ, et al. Refractory anemia in childhood: a retrospective analysis of 67 patients with particular reference to monosomy 7. Blood. 2003;102:1997–2003.
Locatelli F, Niemeyer CM. How I treat juvenile myelomonocytic leukemia. Blood. 2015;125:1083–90.
Claviez A. HSCT for lymphomas in children and adolescents. In: Apperley J, et al., editors. ESH-EBMT handbook on haemopoietic stem cell transplantation. Paris: ESH; 2012. p. 530–41.
Michaux K, Bergeron C, Gandemer V, Mechinaud F, Uyttebroeck A, Bertrand Y. Relapsed or refractory lymphoblastic lymphoma in children: results and analysis of 23 patients in the EORTC 58951 and the LMT96 protocols. Pediatr Blood Cancer. 2016;63:1214–21.
Peniket AJ, Ruiz de Elvira MC, Taghipour G, et al. An EBMT registry matched study of allogeneic stem cell transplants for lymphoma: allogeneic transplantation is associated with a lower relapse rate but a higher procedure-related mortality rate than autologous transplantation. Bone Marrow Transplant. 2003;31:667–78.
Schmitz N, Pfistner B, Sextro M, et al. Aggressive conventional chemotherapy compared with high-dose chemotherapy with autologous haemopoietic stem-cell transplantation for relapsed chemosensitive Hodgkin’s disease: a randomised trial. Lancet. 2002;359:2065–71.
Kelly KM. Management of children with high-risk Hodgkin lymphoma. Br J Haematol. 2012;157:3–13.
Satwani P, Ahn KW, Carreras J, et al. A prognostic model predicting autologous transplantation outcomes in children, adolescents and young adults with Hodgkin lymphoma. Bone Marrow Transplant. 2015;50:1416–23.
Rashidi A, Ebadi M, Cashen AF. Allogeneic hematopoietic stem cell transplantation in Hodgkin lymphoma: a systematic review and meta-analysis. Bone Marrow Transplant. 2016;51:521–8.
Claviez A, Canals C, Dierickx D, et al. Allogeneic hematopoietic stem cell transplantation in children and adolescents with recurrent and refractory Hodgkin lymphoma: an analysis of the European Group for Blood and Marrow Transplantation. Blood. 2009;114:2060–7.
Raiola A, Dominietto A, Varaldo R, et al. Unmanipulated haploidentical BMT following non-myeloablative conditioning and post-transplantation CY for advanced Hodgkin’s lymphoma. Bone Marrow Transplant. 2014;49:190–4.
Gerrard M, Cairo MS, Weston C, et al. Excellent survival following two courses of COPAD chemotherapy in children and adolescents with resected localized B-cell non-Hodgkin’s lymphoma: results of the FAB/LMB 96 international study. Br J Haematol. 2008;141:840–7.
Attarbaschi A, Dworzak M, Steiner M, et al. Outcome of children with primary resistant or relapsed non-Hodgkin lymphoma and mature B-cell leukemia after intensive first-line treatment: a population-based analysis of the Austrian Cooperative Study Group. Pediatr Blood Cancer. 2005;44:70–6.
Philip T, Guglielmi C, Hagenbeek A, et al. Autologous bone marrow transplantation as compared with salvage chemotherapy in relapses of chemotherapy-sensitive non-Hodgkin’s lymphoma. N Engl J Med. 1995;333:1540–5.
Gross TG, Hale GA, He W, et al. Hematopoietic stem cell transplantation for refractory or recurrent non-Hodgkin lymphoma in children and adolescents. Biol Blood Marrow Transplant. 2010;16:223–30.
Satwani P, Jin Z, Martin PL, et al. Sequential myeloablative autologous stem cell transplantation and reduced intensity allogeneic hematopoietic cell transplantation is safe and feasible in children, adolescents and young adults with poor-risk refractory or recurrent Hodgkin and non-Hodgkin lymphoma. Leukemia. 2015;29:448–55.
Attarbaschi A, Carraro E, Abla O, et al. Non-Hodgkin’s lymphoma and pre-existing conditions: spectrum, clinical characteristics and outcome in 213 children and adolescents. Haematologica. 2016;101(12):1581–91.
Admiraal R, van Kesteren C, der Zijde CM, et al. Association between anti-thymocyte globulin exposure and CD4+ immune reconstitution in paediatric haemopoietic cell transplantation: a multicentre, retrospective pharmacodynamic cohort analysis. Lancet Haematol. 2015;2:e194–203.
Pai SY, Logan BR, Griffith LM, et al. Transplantation outcomes for severe combined immunodeficiency, 2000–2009. N Engl J Med. 2014;371:434–46.
Kang E, Gennery A. Hematopoietic stem cell transplantation for primary immunodeficiencies. Hematol Oncol Clin North Am. 2014;28:1157–70.
Dvorak CC, Hassan A, Slatter MA, et al. Comparison of outcomes of hematopoietic stem cell transplantation without chemotherapy conditioning by using matched sibling and unrelated donors for treatment of severe combined immunodeficiency. J Allergy Clin Immunol. 2014;134:935–943.e915.
Bertaina A, Merli P, Rutella S, et al. HLA-haploidentical stem cell transplantation after removal of alphabeta+ T and B cells in children with nonmalignant disorders. Blood. 2014;124:822–6.
Gennery AR, Slatter MA, Grandin L, et al. Transplantation of hematopoietic stem cells and long-term survival for primary immunodeficiencies in Europe: entering a new century, do we do better? J Allergy Clin Immunol. 2010;126:602–10.e1–11.
Hussein AA, Al-Zaben A, Ghatasheh L, et al. Risk adopted allogeneic hematopoietic stem cell transplantation using a reduced intensity regimen for children with thalassemia major. Pediatr Blood Cancer. 2013;60:1345–9.
Locatelli F, Kabbara N, Ruggeri A, et al. Outcome of patients with hemoglobinopathies given either cord blood or bone marrow transplantation from an HLA-identical sibling. Blood. 2013;122:1072–8.
Angelucci E, Matthes-Martin S, Baronciani D, et al. Hematopoietic stem cell transplantation in thalassemia major and sickle cell disease: indications and management recommendations from an international expert panel. Haematologica. 2014;99:811–20.
Lucarelli G, Galimberti M, Polchi P, et al. Marrow transplantation in patients with thalassemia responsive to iron chelation therapy. N Engl J Med. 1993;329:840–4.
Baronciani D, Angelucci E, Potschger U, et al. Hemopoietic stem cell transplantation in thalassemia: a report from the European Society for Blood and Bone Marrow Transplantation Hemoglobinopathy Registry, 2000–2010. Bone Marrow Transplant. 2016;51:536–41.
Fleischhauer K, Locatelli F, Zecca M, et al. Graft rejection after unrelated donor hematopoietic stem cell transplantation for thalassemia is associated with nonpermissive HLA-DPB1 disparity in host-versus-graft direction. Blood. 2006;107:2984–92.
Ruggeri A, Eapen M, Scaravadou A, et al. Umbilical cord blood transplantation for children with thalassemia and sickle cell disease. Biol Blood Marrow Transplant. 2011;17:1375–82.
Anurathapan U, Hongeng S, Pakakasama S, et al. Hematopoietic stem cell transplantation for homozygous beta-thalassemia and beta-thalassemia/hemoglobin E patients from haploidentical donors. Bone Marrow Transplant. 2016;51:813–8.
Gluckman E. Allogeneic transplantation strategies including haploidentical transplantation in sickle cell disease. Hematology Am Soc Hematol Educ Program. 2013;2013:370–6.
Andreani M, Testi M, Gaziev J, et al. Quantitatively different red cell/nucleated cell chimerism in patients with long-term, persistent hematopoietic mixed chimerism after bone marrow transplantation for thalassemia major or sickle cell disease. Haematologica. 2011;96:128–33.
Samarasinghe S, Steward C, Hiwarkar P, et al. Excellent outcome of matched unrelated donor transplantation in paediatric aplastic anaemia following failure with immunosuppressive therapy: a United Kingdom multicentre retrospective experience. Br J Haematol. 2012;157:339–46.
Choi YB, Yi ES, Lee JW, Sung KW, Koo HH, Yoo KH. Immunosuppressive therapy versus alternative donor hematopoietic stem cell transplantation for children with severe aplastic anemia who lack an HLA-matched familial donor. Bone Marrow Transplant. 2016;52(1):47–52.
Dufour C, Veys P, Carraro E, et al. Similar outcome of upfront-unrelated and matched sibling stem cell transplantation in idiopathic paediatric aplastic anaemia. A study on behalf of the UK Paediatric BMT Working Party, Paediatric Diseases Working Party and Severe Aplastic Anaemia Working Party of EBMT. Br J Haematol. 2015;171:585–94.
Peffault de Latour R, Rocha V, Socie G. Cord blood transplantation in aplastic anemia. Bone Marrow Transplant. 2013;48:201–2.
Clay J, Kulasekararaj AG, Potter V, et al. Nonmyeloablative peripheral blood haploidentical stem cell transplantation for refractory severe aplastic anemia. Biol Blood Marrow Transplant. 2014;20:1711–6.
Peffault de Latour R, Porcher R, Dalle JH, et al. Allogeneic hematopoietic stem cell transplantation in Fanconi anemia: the EBMT experience. Blood. 2013;122(26):4279–86.
Fagioli F, Quarello P, Zecca M, et al. Haematopoietic stem cell transplantation for Diamond Blackfan anaemia: a report from the Italian Association of Paediatric Haematology and Oncology Registry. Br J Haematol. 2014;165:673–81.
Lipton JM, Atsidaftos E, Zyskind I, Vlachos A. Improving clinical care and elucidating the pathophysiology of Diamond Blackfan anemia: an update from the Diamond Blackfan Anemia Registry. Pediatr Blood Cancer. 2006;46:558–64.
Fioredda F, Iacobelli S, van Biezen A, et al. Stem cell transplantation in severe congenital neutropenia: an analysis from the European Society for Blood and Marrow Transplantation. Blood. 2015;126:1885–92; quiz 1970.
Mahadeo KM, Tewari P, Parikh SH, et al. Durable engraftment and correction of hematological abnormalities in children with congenital amegakaryocytic thrombocytopenia following myeloablative umbilical cord blood transplantation. Pediatr Transplant. 2015;19:753–7.
Chiesa R, Wynn RF, Veys P. Haematopoietic stem cell transplantation in inborn errors of metabolism. Curr Opin Hematol. 2016;23(6):530–5.
Aldenhoven M, Wynn RF, Orchard PJ, et al. Long-term outcome of Hurler syndrome patients after hematopoietic cell transplantation: an international multicenter study. Blood. 2015;125:2164–72.
Gratwohl A, Baldomero H, Demirer T, Rosti G, Dini G, Ladenstein R, Urbano-Ispizua A. Hematopoetic stem cell transplantation for solid tumors in Europe. Ann Oncol. 2004;15:653–60.
Matthay KK, Reynolds CP, Seeger RC, et al. Long-term results for children with high-risk neuroblastoma treated on a randomized trial of myeloablative therapy followed by 13-cis-retinoic acid: a Children’s Oncology Group study. J Clin Oncol. 2009;27:1007–13.
Ladenstein R, Pötschger U. High-dose chemotherapy and HSCT in children and adolescents with solid tumours in Europe. In: Apperley J, et al., editors. The EBMT handbook. Paris: ESH; 2012. p. 598–611.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2018 Springer International Publishing AG
About this chapter
Cite this chapter
Locatelli, F., Strocchio, L. (2018). Indications for Hematopoietic Stem Cell Transplantation in Children. In: Gluckman, É., Niederwieser, D., Aljurf, M. (eds) Establishing a Hematopoietic Stem Cell Transplantation Unit . Springer, Cham. https://doi.org/10.1007/978-3-319-59358-6_6
Download citation
DOI: https://doi.org/10.1007/978-3-319-59358-6_6
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-59356-2
Online ISBN: 978-3-319-59358-6
eBook Packages: MedicineMedicine (R0)