
Abstract
Endometrioid endometrial adenocarcinoma is the most common form of endometrial cancer. While many endometrioid carcinomas are cured by hysterectomy, there is a substantial subset of patients who suffer from tumor recurrence. These recurrences, especially those outside the pelvis, are not optimally treated with current chemotherapeutic and radiation treatment strategies, so molecularly targeted therapeutics are an option. Being able to predict which low-grade, early-stage endometrioid-type endometrial carcinomas will recur is another unmet clinical need. With the advent of The Cancer Genome Atlas, there has been an explosion of molecular information made available for endometrial cancer. The challenge to future investigators will be to incorporate this information into standard clinical practice for the more optimal management of patients. In this chapter, the more common molecular features of endometrioid-type endometrial carcinoma are reviewed, with particular attention to associations with pathological variables and clinical outcomes. Specific genes/pathways discussed include PI3K/AKT pathway, KRAS, CTNNB1, microsatellite instability, TP53, and POLE. A brief overview of the endometrial Cancer Genome Atlas is also provided.
Access provided by CONRICYT-eBooks. Download chapter PDF
Similar content being viewed by others


Keywords
- Endometrioid adenocarcinoma
- Endometrial cancer
- CTNNB1 mutation
- PTEN mutation
- PIK3CA mutation
- KRAS mutation
- MLH1 methylation
- POLE mutation
- Microsatellite instability
Introduction
The most common subtype of endometrial adenocarcinoma is endometrioid adenocarcinoma, with prevalence rates of around 80% [1, 2]. According to the Bokhman classification [3], these tumors are generally classified as Type I and tend to be associated with a better prognosis than Type II tumors [1, 2]. Endometrioid endometrial adenocarcinomas generally present at an earlier stage than non-endometrioid tumors and often have lower rates of recurrence [2]. Despite these less aggressive clinical characteristics, a subset of endometrioid carcinomas does behave more aggressively, and recent research has focused on characterizing the genotypic differences that may account for this. Molecular characterization of endometrioid adenocarcinoma can also provide potential therapeutic targets for matched targeted therapy trials, as current chemotherapy and radiation therapy approaches to the treatment of advanced/recurrent endometrioid-type endometrial cancer are not optimal.
PI3K/AKT Pathway
Activation of the PI3K/AKT signaling pathway is common in endometrial cancer, with pathway alterations reported to occur in over 80% of endometrioid endometrial cancers [4,5,6]. PTEN alteration is the most common, but other genes in this pathway have been found to be mutated in endometrial cancer as well, including PIK3CA, PIK3R1, and PIK3R2 [4, 6, 7]. Additionally, mutations in multiple genes comprising this pathway have been shown to occur concomitantly [4, 8,9,10]. Survival outcomes have been mixed, but the literature suggests that PI3K pathway mutations may be associated with worse clinical outcomes [8, 11, 12]. Further, a study by Nout et al. showed a worse disease-free survival in endometrioid endometrial carcinomas when mutations within multiple signaling pathways, including the PI3K/AKT pathway, co-occur [8].
PTEN
The phosphatase and tensin homolog (PTEN) gene encodes a protein which functions as a tumor suppressor within the PI3K/AKT pathway [13, 14]. Inactivation of the PTEN gene is one of the most frequent mutations within this pathway and within endometrioid endometrial cancer in general, with described prevalence rates ranging from 15 to 80% [4, 13, 15,16,17,18,19,20].
PTEN mutations have been identified in both endometrial hyperplasia and in endometrial cancer and are thought to be an early event in tumorigenesis [21,22,23]. These mutations have been seen in both sporadic tumors and, to a lesser extent, in tumors associated with Lynch Syndrome [24]. PTEN mutations are more common in endometrioid endometrial cancer than in mixed or serous tumors [14, 16,17,18, 25]. Data regarding the relationship between PTEN mutations and microsatellite instability (MSI) status are mixed, with some studies showing higher rates of MSI-high in tumors with PTEN mutations, while others show no relationship [5, 25, 26].
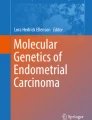
However, Djordjevic et al. recently demonstrated that intact PTEN protein expression (and the presence of PTEN wild-type gene) was associated with microsatellite-stable (MSS) non-endometrioid endometrial carcinomas, while no such relationship existed in endometrioid endometrial tumors [27]. Approximately 90% of deleterious PTEN mutations are associated with immunohistochemical (IHC) loss of PTEN protein [14] (Fig. 4.1). Interestingly, in approximately 40% of endometrial carcinomas, IHC loss of PTEN protein expression is associated with no gene sequence abnormality [14]. This is likely due to the fact that PTEN protein and mRNA can be regulated by a variety of different mechanisms independent of gene mutation [28]. Therefore, for clinical purposes, immunohistochemistry may be a preferable method of detecting endometrial carcinomas with loss of PTEN function.

PTEN immunohistochemistry. a Endometrial carcinoma with intact positive protein expression of PTEN. No PTEN gene mutation was detected by next-generation sequencing. b Endometrial carcinoma with PTEN gene mutation and associated loss of PTEN protein expression. Note intact expression of PTEN protein in adjacent stromal cells, which acts as an internal positive control
Multiple studies have attempted to characterize the relationship between PTEN endometrial cancer mutations and survival outcomes. In a single institution study of 221 endometrial cancer patients, Akiyama-Abe et al. performed IHC staining for PTEN and found loss of protein expression in 25% of tumors. In those with loss of PTEN expression, the authors found a significant association with endometrioid histology and decreased lymphatic–vascular invasion, as well as a significant improvement in overall survival [16]. Interestingly, they did not find any differences in rates of advanced stage at presentation or early grade tumors. Improved outcomes including survival and recurrence rates with PTEN mutations have similarly been shown in some, but not all, prior studies [25, 29, 30]. In contrast, a recent study of 187 endometrioid endometrial cancer patients by Westin et al. found that, in aggregate, there was no difference in progression-free survival of patients with IHC-determined loss of PTEN function compared with those tumors that retained PTEN function. However, on a sub-analysis of stratification by body mass index (BMI), loss of PTEN function in the presence of obesity (BMI ≥30) was associated with significantly improved progression-free survival, whereas non-obese patients (BMI <30) were found to have significantly worse progression-free survival in the setting of PTEN loss [31].
PIK3CA
The PIK3CA gene encodes the p110-alpha subunit of PI3K, which functions as the catalytic subunit of the protein complex [6, 32]. Mutation prevalence for endometrial cancer has been reported to be between 20 and 36% [4, 10, 11, 32,33,34,35], with mutations being more frequent in endometrioid than non-endometrioid tumors [4, 32]. Concurrent PIK3CA and PTEN mutations in endometrial carcinomas have been found in multiple studies [4, 10, 11]. There are also some data to support higher rates of MSI-high in endometrial tumors with PIK3CA mutations [36, 37], though not all studies have found this to be the case [5].
In general, endometrial tumors with PIK3CA mutation appear to be more aggressive than those without, with trends toward worse survival outcomes [12, 17, 36]. McIntyre et al. [36] found that PIK3CA mutations were associated with worse disease-specific survival in grade 3 endometrioid tumors, but this association did not persist on multivariate analysis and, interestingly, was not present for serous tumors harboring PIK3CA mutations. Catasus and colleagues similarly investigated 109 predominantly endometrioid endometrial carcinomas and found increased rates of myometrial invasion and lymphatic–vascular space invasion in association with PIK3CA mutations. Interestingly, they showed higher rates of grade 3 tumors as well as increased myometrial invasion or cervical involvement when mutations occurred in exon 20, compared with mutations on exon 9 which were more often associated with early grade tumors and invasion of less than half of the myometrium [11]. These data suggested that, in addition to PIK3CA mutations being important for survival outcomes, some PIK3CA mutations may be more relevant than others. This mutational diversity phenomenon, the overall tendency toward worse prognosis associated with PIK3CA mutations, and the complex nature of the PI3K/AKT pathway may account for some of the reasons why, despite the availability of multiple PI3K/AKT pathway inhibitors, clinical trials have failed to show consistent benefit with the use of PI3K/AKT targeted therapy in endometrial cancer [38].
PIK3R1 and PIK3R2
The PIK3R1 and PIK3R2 genes encode the p85-alpha and p85-beta regulatory subunits of PI3K [4, 6], which form a dimer that assists in stabilization of PTEN. A 2011 study by Cheung et al. further characterized the role of PIK3R1 in endometrial tumors and described largely for the first time the presence of PIK3R2 mutation in endometrial cancer [4, 39]. Mutation rates in endometrial carcinoma are 20–43% for PIK3R1 [4, 40], and 5% for PIK3R2 [4]. Findings from these studies suggest that PIK3R1 and PIK3R2 mutations may lead to activation of the PI3K/AKT pathway and thereby contribute to endometrial cancer tumorigenesis.
ARID1A
The ARID1A gene encodes a non-catalytic subunit of the SWI/SNF complex, which aids in chromatin remodeling [41, 42]. Bosse et al. [42] found that 27% of endometrioid endometrial cancers had ARID1A mutation and that these mutations were commonly associated with PI3K/AKT pathway mutations. ARID1A mutations appear to be more common with MSI-high tumors [37, 42,43,44], and it has been suggested that ARID1A may play a role in epigenetic silencing of MLH1 [42]. An interesting study by Mao et al. analyzed ARID1A mutations in 246 cases ranging from normal endometrium to high-grade endometrial cancer. They found no mutations in normal tissue, areas of clonal but not complete loss within 16% of complex atypical hyperplasia cases, complete loss in 25% of low-grade endometrioid endometrial cancers, and complete loss in 44% of high-grade endometrioid tumors [45]. These results were notable, as they suggested a possible role in tumor progression for ARID1A mutations which had not previously been well described. As data are still limited regarding ARID1A mutations in endometrial cancer, little is available regarding survival outcomes. While Allo and colleagues found that ARID1A mutations do appear to be present within high-grade endometrioid tumors, they were unable to find a difference in progression-free survival within the endometrioid endometrial cancer group [43].
KRAS
The KRAS gene encodes the K-Ras protein, which functions along the RAS/MAPK pathway and helps regulate cell division [46]. Prevalence rates of KRAS mutation in endometrial cancers have been reported to be between 10 and 30% [4, 47, 48]. Several studies have found similar rates of KRAS mutation in endometrial hyperplasias and endometrial cancers, suggesting that KRAS mutation may represent an early event during tumorigenesis [47, 49].
KRAS mutations are more frequent among endometrioid and mixed endometrioid histologies, compared to non-endometrioid endometrial cancers [18, 50, 51]. Furthermore, KRAS mutation rates are higher in endometrioid tumors showing increasing amounts of mucinous differentiation [52], which may be clinically significant since mucinous differentiation has been associated with lymph node involvement [53]. Some studies have suggested that endometrial cancers with KRAS mutation tend to be associated with lower endometrioid grade, though others have found no association with grade [50, 51, 54]. Like many other mutations in endometrioid endometrial cancer, KRAS mutations are more frequently found in MSI-high tumors than MSS tumors [44]. Interestingly, atypical endometrial hyperplasia with MSI-high exhibits wild-type KRAS, suggesting that defects in DNA mismatch repair precede KRAS mutation [24, 55].
There are limited data regarding clinical outcomes in endometrioid endometrial cancers with KRAS mutation. Birkeland et al. analyzed KRAS mutations from 264 primary and 22 metastatic endometrial carcinomas. They found KRAS mutations to be more prevalent among grade 1 and 2 tumors, in those with endometrioid histology, and in obese women. There was no association with prognosis, and there were no differences in mutation rates among the primary and metastatic tumors [56]. In contrast, Ito et al. showed that in a cohort of 221 endometrioid endometrial cancers, there was a higher prevalence of KRAS mutation among patients older than 60 years of age who had recurrence of their disease or died due to disease [54].
Several studies have also examined for a possible association between tamoxifen use and KRAS mutation within the endometrium [46, 57, 58]. A small retrospective study by Turbiner et al. found that women with endometrial cancer who were taking tamoxifen for breast cancer had a higher incidence of KRAS mutations. Within the tamoxifen cohort, 16 of the 18 tumors were endometrioid, one was of mixed histology, and one was a clear cell carcinoma [46]. Interestingly, a subsequent study by Tsujioka et al. similarly saw increased KRAS mutations in benign polyps within the endometrium of women taking tamoxifen, but found that after cessation of tamoxifen use the KRAS mutations were no longer identified [58].
Several studies have suggested that the presence of a KRAS mutation may correlate with poorer responses to several targeted therapies, especially those targeting the PI3K/AKT pathways such as mTOR inhibitors [6, 59]. A small in vitro study by Weigelt et al. found an increased resistance to mTOR inhibitors in endometrial cancer cell lines harboring PIK3CA and/or PTEN mutations with a coexisting KRAS mutation, though it did show that a subset of these cells still retained some sensitivity to other forms of PI3K pathway modulation [60]. A recent phase II trial of everolimus in 35 patients with recurrent endometrial cancer showed that none of the patients with a KRAS mutation and positive staining for pS6 (a marker of downstream activation of the PI3K/AKT/mTOR pathway) had a prolonged response to the mTOR inhibitor [61]. In contrast, an in vitro and in vivo study of the effects of metformin on endometrial cancer cell lines by Iglesias et al. found increased apoptosis in cells with KRAS mutation, as well as lower mean tumor weights. Interestingly, the presence of a PTEN mutation had no effect on tumor response to metformin in these cell lines. Metformin’s mechanism of action as a potential cancer therapeutic is thought to involve a decrease of tumor growth, and based on these data, it appears that this effect is potentiated in KRAS mutant cells. The authors therefore suggested that this may be due to phosphorylation of the activated K-Ras protein by Protein Kinase C, which subsequently leads to its removal from the plasma membrane and, ultimately, to apoptosis of the tumor cell [62].
CTNNB1
The CTNNB1 gene encodes the protein β-catenin, which functions as a member of the canonical Wnt pathway. In normal endometrium, β-catenin is expressed primarily at the cell membrane of glandular epithelial cells. CTNNB1 mutation leads to less degradation of β-catenin protein, causing the protein to accumulate in the cytoplasm or translocate to the nucleus (Fig. 4.2), where it subsequently serves as a transcription factor for Myc, cyclin D1, and E-cadherin [63,64,65]. CTNNB1 mutations have been discovered in up to 45% of endometrioid endometrial cancers [20, 65,66,67,68,69]. In 2013, The Cancer Genome Atlas (TCGA) reported on a genomic investigation of 373 endometrial carcinomas, which identified frequent mutations in the CTNNB1 gene, specifically in the subset of endometrioid carcinomas [44]. Interestingly, in this analysis, 52% of the microsatellite-stable (MSS) tumors tested had a mutation in CTNNB1. In contrast, tumors with high microsatellite instability showed infrequent CTNNB1 mutations [44].

β-catenin immunohistochemistry in normal endometrium (a) and endometrial carcinoma with CTNNB1 gene mutation (b). In normal endometrial epithelium, β-catenin protein shows strong, membranous expression, with little-to-no cytoplasmic or nuclear expression. In endometrial carcinomas with CTNNB1 (encodes β-catenin) mutation, β-catenin protein is inhibited from degradation, allowing translocation from the membrane to the cytoplasm and nucleus. Nuclear expression helps to drive activation of the WNT signaling pathway
Several earlier studies have suggested an association of CTNNB1 mutations with lower grade and earlier stage endometrial cancers, as well as with endometrioid histology [63, 66, 70,71,72]. Moreno-Bueno et al. investigated 128 endometrial cancers, including 95 with endometrioid and 33 with non-endometrioid histology. CTNNB1 mutations were detected in 14.9% of the endometrioid tumors, but in none of the non-endometrioid tumors [66]. Fukuchi et al. analyzed 76 endometrial tumors and found that of the 10 tumors with CTNNB1 mutations, all except one were well- or moderately differentiated endometrioid carcinomas. Among these tumors, all except one were stage 1 or 2 at the time of diagnosis [63]. Similarly, findings of a predominance of grade 1 or 2 tumors have been reported by several other studies [70,71,72].
Recent findings suggest that endometrial cancers with beta-catenin mutations may represent a more aggressive subset of early endometrioid endometrial cancers [72,73,74,75]. Liu et al. performed consensus clustering of 271 of the endometrioid endometrial cancers used in TCGA, which revealed four distinct clusters of gene signatures. The group designated Cluster 2 represented a subset of low-grade, low-stage tumors with significantly higher frequencies of CTNNB1 mutations and evidence for activation of the WNT/β-catenin signaling pathway. This group exhibited lower overall survival than even the higher grade and higher stage clusters, and was comprised of a younger, more obese subset of patients [73]. Similarly, Myers et al. performed a case-control analysis of 50 patients with low-grade, stage IA endometrioid endometrial carcinomas in order to further characterize those patients who had a recurrence of their early disease [74]. This study investigated the frequency of three commonly mutated genes in endometrial cancer, including PIK3CA, CTNNB1, and KRAS. They found that CTNNB1 mutations were more frequent among the 12 patients with recurrent disease than among the 38 patients who did not recur and that there were no differences in rates of PIK3CA or KRAS mutations. In contrast to Liu et al., however, Myers et al. found the subset of patients with a recurrence to have a lower body mass index (BMI) than those without a recurrence of their disease.
TP53
The TP53 gene encodes the p53 protein which assists in cell cycle arrest and apoptosis, and its mutation is frequent in numerous cancer types, including endometrial cancer [76, 77]. While prevalence rates are much higher in non-endometrioid than endometrioid endometrial carcinomas [18, 78], the majority of publications evaluating TP53 mutations in endometrial cancer were done in predominantly endometrioid tumors, and rates of TP53 mutation have still been reported to be 10–35% [44, 69, 77,78,79,80,81,82,83]. Lower grade endometrioid carcinomas may have higher frequencies of concurrent TP53 and PTEN mutations compared with serous carcinomas and grade 3 endometrioid tumors, suggesting that the mechanism for p53-related tumorigenesis is different in endometrioid versus non-endometrioid tumors [44]. In support of this idea, Kaku et al. found a higher rate of TP53 mutations in endometrial carcinomas without associated hyperplasia than in those with hyperplasia [84].
As discussed above, data from TCGA suggested that TP53 mutations tended to cluster within the endometrial tumors showing serous histology and grade 3 endometrioid histology [44]. Other authors have found a similar association between grade 3 tumors and TP53 mutation [78, 80, 85, 86]. Interestingly, a study by Kuhn et al. found prevalence rates of 30% within a sample of 20 undifferentiated endometrial tumors, 12 of which had both an endometrioid and undifferentiated component. When present, the TP53 mutations were seen in both the undifferentiated and its corresponding endometrioid components, with the exception of one tumor which only showed a TP53 mutation in the undifferentiated aspect of the tumor, suggesting a possible role of p53 in tumor progression (Kuhn). While several studies also suggest an association between TP53 mutation and advanced stage, not all studies have found this to be the case [78, 82, 85, 87]. Similarly, no consensus findings of a relationship between TP53 mutation and depth of invasion, lymphatic–vascular space invasion, or metastatic disease have been demonstrated [78, 82, 85, 87].
In general, clinical outcomes in patients with endometrioid endometrial cancer harboring TP53 mutations appear to be worse than in those without TP53 mutations. Lee et al. examined 131 patients with predominantly endometrioid endometrial cancer and found TP53 mutation to be an independent prognostic indicator of poor overall survival and disease-free survival [82]. Other studies have shown a similar association with poor overall survival or disease-free survival, though many studies were unable to demonstrate a statistically significant difference in multivariate analysis [78, 80, 85, 88,89,90,91,92,93]. Reasons for the somewhat heterogeneous findings of these studies may include the wide range of numbers of patients, differences in histologic representation, and variation in methodologies for evaluation of TP53 mutational status. Several studies have also looked at the effect of TP53 mutations on outcomes in important subpopulations. For example, a study of 136 endometrial cancer patients by Oreskovic and colleagues found worse overall survival on multivariate analysis in those patients with grade 1 and grade 2, but not grade 3, tumors [94]. There is some evidence that the presence of TP53 mutation can help impact therapeutic approaches to patients with endometrioid endometrial carcinoma. Saffari et al. found that, in a group of 53 endometrioid endometrial carcinoma patients, TP53 mutation was associated with worse overall survival on multivariate analysis. In those women with TP53 mutations who received adjuvant radiation therapy, survival outcomes were similar to wild-type patients with and without radiation treatment, and all three of these subgroups demonstrated better survival than patients with TP53 mutation-containing tumors who did not receive adjuvant radiotherapy [93].
Microsatellite Instability
DNA mismatch repair (MMR) is controlled by a family of nuclear proteins, including MLH1, MSH2, MSH6, and PMS2. Defects in MMR can result from germline mutations in the genes encoding these proteins (Lynch Syndrome) or, in sporadic endometrial and colorectal carcinoma, from hypermethylation of the MLH1 gene promoter. MMR defects are manifested as high levels of microsatellite instability (MSI-high, assessed clinically via a PCR-based assay) and by loss of mismatch repair protein expression in immunohistochemistry-based assays as demonstrated in Fig. 4.3 [95]. Prevalence of MSI-high in endometrial cancer has been reported to be around 15–40% [26, 50, 96,97,98,99,100,101,102], with 15–25% being the most common. In most published studies, no distinction is made between germline versus sporadic MMR loss, although it can be inferred that the vast majority of endometrial cancers with defective MMR are sporadic cancers with MLH1 protein loss due to MLH1 gene methylation.

MLH1 methylation associated with MLH1 protein loss by immunohistochemistry. a Endometrial carcinoma with retained nuclear expression of MLH1 protein. b Endometrial carcinoma with loss of MLH1 protein. Note retained positive expression of MLH1 in adjacent stromal cells. c PCR-based MLH1 promoter methylation analysis. Tumor DNA is analyzed concurrently with DNA from normal tissue control from the same patient. Top tracing, normal tissue with no MLH1 methylation; bottom tracing, tumor with presence of MLH1 methylation
MMR loss and MLH1 hypermethylation are thought to be early events during tumorigenesis in endometrial cancer, as hypermethylation patterns have been observed in endometrial hyperplasias [47, 103]. MSI-high is more common among endometrioid carcinomas compared to non-endometrioid tumors, including serous and clear cell carcinomas [27, 50, 101, 104, 105]. The relationship between tumor grade and MSI status is somewhat unclear, as some studies show an association with increasing grade in MSI-high tumors, while others show no association [104, 106,107,108]. Similarly, evaluating the relationship between MSI status and clinical stage has led to conflicting results, with several studies showing an association of MSI-high tumors with more advanced stage disease, others showing an association with earlier stages, and some studies showing no association with stage [101, 104, 106, 107, 109]. MSI-high tumors have been reported to have an increased risk of lymphatic–vascular space invasion [102, 104], but their relationship with depth of myometrial invasion is not clear [101, 104, 106]. MMR deficiency, particularly MLH1 protein loss and MLH1 methylation, has been associated with a subset of undifferentiated endometrial carcinoma [110,111,112,113]. It is uncertain whether undifferentiated endometrial carcinoma should be considered a subtype of grade 3 endometrioid adenocarcinoma or a non-endometrioid carcinoma. Compared to grade 3 endometrioid adenocarcinoma, undifferentiated carcinomas typically have lower hormone receptor and cytokeratin expression [110] and may have a more aggressive disease course [111, 114, 115].
The impact of MSI-high on survival outcomes in endometrial cancer is similarly unclear, despite a number of different publications examining this issue. Details of several of the larger studies evaluating MMR status and survival outcomes are summarized in Table 4.1. Some authors have identified improved outcomes in MSI-high tumors [97, 98, 101, 102], others found worse outcomes [116, 117], and some have found no association [100, 105, 106, 118]. One large study by Zighelboim et al. analyzed 446 prospectively collected endometrioid endometrial carcinomas [100]. MSI status was determined by PCR, as was MLH1 methylation status. No differences in overall survival or disease-free survival were observed between MSI-high and microsatellite-stable groups. Similarly, MLH1 methylation status had no impact on overall or progression-free survival. One of the more recent larger analyses was performed by Ruiz and colleagues, who evaluated 212 endometrioid endometrial tumors. MSI status was evaluated by IHC. They evaluated OS and PFS both within early stage (I and II) and advanced stage (III and IV) and found no differences in survival measures within either subgroup [106]. The reasons for conflicting results between these various publications are unclear. As noted in Table 4.1, MMR deficiency has been measured in a variety of different ways in these studies, which could impact results. Endometrioid and non-endometrioid carcinomas have very different clinical courses and survival outcomes; an impact of MMR on survival may be missed in studies that include both these histologies. Lower grade, early-stage endometrioid carcinomas can recur five or more years following hysterectomy, so studies with shorter follow-up intervals may miss an association with MSI-high. It is also possible that these differences may be due at least in part to underlying differences in other concurrent gene mutations not fully evaluated in these studies.
POLE
As discussed previously, based on the molecular analysis of 373 endometrial carcinomas, TCGA [44] proposed a genomic categorization of endometrial cancer into four groups. “Ultramutated tumors” represent the first category in this classification and consist of tumors with very high mutations rates. All of these tumors harbor mutations in the POLE gene, which encodes the catalytic subunit of the DNA polymerase epsilon, which synthesizes the leading strand during DNA replication and also plays a role in the recognition and removal of mispaired nucleotides [119, 120]. Tumors with POLE mutations may have as many as a million base substitutions per tumor, particularly of the G:C>T:A form [121]. It has recently been shown that germline exonuclease domain mutations of POLE and POLD1 genes confer a high risk of multiple colorectal adenomas and carcinomas [122]. In addition to endometrial and colorectal cancer, POLE mutations have also been reported in lung cancer and melanoma [123, 124]. Their inheritance is dominant, and they have a high penetrance with a variable phenotype.
The majority of POLE mutations in endometrial cancer are sporadic and have been reported to represent 5–7% [44, 121, 125] of endometrial cancers. In endometrial carcinoma, most POLE mutations tend to cluster in two hot spots, in exons 9 and 13 [126, 127]. Paradoxically, despite being “ultramutated,” these tumors have been associated with a favorable prognosis [44, 126, 128]. This observation has recently been corroborated by a large study, which reported the POLE mutant tumors as having approximately one-third the risk of recurrence as that of POLE wild-type (predominantly endometrioid in this study) endometrial cancers, and an even lower risk of death [125]. It has been hypothesized that improved prognostic outcome in patients with these tumors may be attributable to the fact that the marked number of base substitutions leads to too many gene alterations, which hinder tumor cell growth and survival.
Endometrial POLE mutant tumors have characterized by pure endometrioid histology, mixed histology with endometrioid components, or ambiguous histology [121, 126, 128]. Several studies also reported small numbers of serous endometrial carcinoma with POLE mutations, but it is not certain whether the cases underwent a centralized review [121, 129,130,131]. The majority of endometrioid tumors are of high cytological grade; as many as 84% have been described to have tumor infiltrating lymphocytes [128].
Similar to POLE wild-type endometrioid tumors, POLE mutants frequently carry PTEN (94%), PIK3CA (71%), and ARID1A (76%) mutations; however, unlike most POLE wild-type tumors, the majority of POLE mutants are microsatellite stable (65–100%) [44, 121, 126, 128]. It has been suggested that in cases where microsatellite instability and POLE mutations coexist, the latter is likely a secondary event [132]. Furthermore, while all eight TCGA POLE mutant cases were found to have mutations in at least one mismatch repair gene, only two of these cases were microsatellite instability high, suggesting that some of the mutations are “functionally suboptimal” with respect to their classical mismatch repair gene mutant counterparts [44, 126, 133].
Approximately one-third (35%) of POLE mutant endometrial tumors also have TP53 mutations [121, 126, 128]. Given the good prognostic outcome of the POLE mutant group, the clinical significance of these TP53 mutations is likely different than that of the TP53 mutations in serous carcinoma/copy number high (as per TCGA classification) tumors. The presence of TP53 mutation in some POLE mutants with histological features other than those of clear-cut endometrioid adenocarcinoma is important to note, as the use of p53 immunohistochemistry may lead to misclassification of these tumors as serous carcinomas.
POLE mutations may be a useful biomarker in order to spare patients with high-grade endometrioid tumors from aggressive post-adjuvant treatments, as the tumors appear to have an indolent course. Currently, the only way to detect POLE mutations is by sequencing the POLE gene. Therefore, development of surrogate markers to enable their detection would be very important.
The Cancer Genome Atlas
The Cancer Genome Atlas (TCGA) is a National Cancer Institute-funded effort to comprehensively classify, at a genomic level, various types of cancer. Genomic characterization included next-generation sequencing of the whole exome, methylation profiles, miRNA profiling, gene expression analysis, and reverse phase protein lysate array. These data are publicly available for individual investigator analysis.
Endometrial cancer, both serous carcinoma and endometrioid carcinoma, has been characterized by TCGA [44]. These data reaffirmed high rates of PI3K/AKT pathway mutations within the endometrioid subtype and showed significant rates of CTNNB1, KRAS, and POLE mutation as well. Additionally, TCGA described a subset of endometrioid tumors which molecularly appeared to be more similar to type 2 tumors, and the authors therefore postulated that treatment approaches mirroring those used in uterine serous carcinomas may be beneficial in this group.
Re-analysis of the endometrioid group only (271 patients) revealed extraordinary heterogeneity in these tumors [73]. Four transcriptome clusters of endometrioid endometrial carcinoma were identified, as highlighted in Fig. 4.4. Clusters 1 and 2 each consisted mainly of patients with early-stage and grade 1 or 2 tumors. Clusters 3 and 4 primarily comprised patients with grade 3 tumors presenting with stage III or IV disease at the time of hysterectomy. At the transcriptome level, Cluster 1 is the “classic” endometrial cancer, with high expression of ESR1 and PGR (genes encoding estrogen receptor and progesterone receptor). Remarkably, Cluster 2, which had a similar patient profile as Cluster 1, had significantly lower expression of these hormone receptors but higher expression of WNT5A and WNT5B, genes activated by WNT/β-catenin signaling. Cluster 2 patients were also significantly younger and more obese than patients in the other clusters, including Cluster 1. Unexpectedly, Cluster 2 patients had significantly worse survival than those in Cluster 1. Clusters 3 and 4 displayed similar transcriptome heterogeneity, with Cluster 3 characterized by higher expression of genes associated with cell cycle progression, such as FOXM1, CCNB1, and CDC20. This cluster had the worst survival of the 4 clusters. Cluster 4 had higher expression of genes associated with activation of the immune response, such as STAT1, LCK, GIMAP5, and GIMAP7. Although Cluster 4 was mainly composed of patients with high-grade, late-stage disease, these patients had better overall survival than the patients in Cluster 2. Cluster 3 patients had the worst overall survival.

Summary of The Cancer Genome Atlas (TCGA) analysis of 271 endometrioid-type endometrial carcinomas. Transcriptome Clusters 1 and 2 are primarily composed of patients with low-grade, early-stage disease, while Clusters 3 and 4 are dominated by patients with grade 3 endometrioid tumors, stages III or IV at the time of diagnosis. Clusters 3 and 4 also had significantly more mutations than tumors in Clusters 1 and 2
The four clusters also had distinctive mutation spectra. PTEN and PIK3CA mutations were common in all four clusters. KRAS mutations were common in Clusters 1, 3, and 4, but infrequent in Cluster 2. CTNNB1 mutations were most common in Cluster 2. Clusters 3 and 4 had the majority of the TP53 mutations. Clusters 3 and 4 had the highest mutations per megabase, significantly higher than the mutational load in Clusters 1 and 2.
The TCGA data highlight the genetic and clinical diversity of the endometrioid histotype. These data also help to refute “dogma” that is commonly taught regarding endometrioid-type endometrial cancer. For example, conventional wisdom holds that young, obese women with endometrial cancer have good prognosis disease that is hormone driven. While certainly their prognosis is better than that for patients diagnosed with endometrial serous carcinoma, the TCGA data highlight above that a substantial subset of patients actually has endometrial cancers driven not by hormones but rather by activation of the WNT/β-catenin signaling pathway. Similarly, the higher grade and advanced stage endometrioid cancers are also heterogeneous. The subset of grade 3 endometrioid tumors with a more “immune-driven” genotype has better outcomes. The challenge to young investigators caring for endometrial cancer patients will be to productively incorporate this substantial TCGA data into rational clinical trials and, ultimately, into routine clinical practice.
References
Amant F, et al. Endometrial cancer. Lancet. 2005;366(9484):491–505.
Sherman ME. Theories of endometrial carcinogenesis: a multidisciplinary approach. Mod Pathol. 2000;13(3):295–308.
Bokhman JV. Two pathogenetic types of endometrial carcinoma. Gynecol Oncol. 1983;15(1):10–7.
Cheung LW, et al. High frequency of PIK3R1 and PIK3R2 mutations in endometrial cancer elucidates a novel mechanism for regulation of PTEN protein stability. Cancer Discov. 2011;1(2):170–85.
Marchio C, et al. PIKing the type and pattern of PI3K pathway mutations in endometrioid endometrial carcinomas. Gynecol Oncol. 2015;137(2):321–8.
Slomovitz BM, Coleman RL. The PI3K/AKT/mTOR pathway as a therapeutic target in endometrial cancer. Clin Cancer Res. 2012;18(21):5856–64.
Berg A, et al. Molecular profiling of endometrial carcinoma precursor, primary and metastatic lesions suggests different targets for treatment in obese compared to non-obese patients. Oncotarget. 2015;6(2):1327–39.
Nout RA, et al. Improved risk assessment of endometrial cancer by combined analysis of MSI, PI3K-AKT, Wnt/beta-catenin and P53 pathway activation. Gynecol Oncol. 2012;126(3):466–73.
Oda K, et al. PIK3CA cooperates with other phosphatidylinositol 3’-kinase pathway mutations to effect oncogenic transformation. Cancer Res. 2008;68(19):8127–36.
Oda K, et al. High frequency of coexistent mutations of PIK3CA and PTEN genes in endometrial carcinoma. Cancer Res. 2005;65(23):10669–73.
Catasus L, et al. PIK3CA mutations in the kinase domain (exon 20) of uterine endometrial adenocarcinomas are associated with adverse prognostic parameters. Mod Pathol. 2008;21(2):131–9.
Salvesen HB, et al. Integrated genomic profiling of endometrial carcinoma associates aggressive tumors with indicators of PI3 kinase activation. Proc Natl Acad Sci U S A. 2009;106(12):4834–9.
Lin MC, et al. Involution of latent endometrial precancers by hormonal and nonhormonal mechanisms. Cancer. 2009;115(10):2111–8.
Djordjevic B, et al. Clinical assessment of PTEN loss in endometrial carcinoma: immunohistochemistry outperforms gene sequencing. Mod Pathol. 2012;25(5):699–708.
Boruban MC, et al. From endometrial hyperplasia to endometrial cancer: insight into the biology and possible medical preventive measures. Eur J Cancer Prev. 2008;17(2):133–8.
Akiyama-Abe A, et al. Loss of PTEN expression is an independent predictor of favourable survival in endometrial carcinomas. Br J Cancer. 2013;109(6):1703–10.
Garcia-Dios DA, et al. High-throughput interrogation of PIK3CA, PTEN, KRAS, FBXW7 and TP53 mutations in primary endometrial carcinoma. Gynecol Oncol. 2013;128(2):327–34.
Coenegrachts L, et al. Mutation profile and clinical outcome of mixed endometrioid-serous endometrial carcinomas are different from that of pure endometrioid or serous carcinomas. Virchows Arch. 2015;466(4):415–22.
Koul A, et al. Distinct sets of gene alterations in endometrial carcinoma implicate alternate modes of tumorigenesis. Cancer. 2002;94(9):2369–79.
Byron SA, et al. FGFR2 point mutations in 466 endometrioid endometrial tumors: relationship with MSI, KRAS, PIK3CA, CTNNB1 mutations and clinicopathological features. PLoS ONE. 2012;7(2):e30801.
Joshi A, et al. Activated mutant p110alpha causes endometrial carcinoma in the setting of biallelic Pten deletion. Am J Pathol. 2015;185(4):1104–13.
Hayes MP, et al. PIK3CA and PTEN mutations in uterine endometrioid carcinoma and complex atypical hyperplasia. Clin Cancer Res. 2006;12(20 Pt 1):5932–5.
Albertini AF, Devouassoux-Shisheboran M, Genestie C. Pathology of endometrioid carcinoma. Bull Cancer. 2012;99(1):7–12.
Huang M, et al. Molecular pathogenesis of endometrial cancers in patients with Lynch syndrome. Cancer. 2013;119(16):3027–33.
Risinger JI, et al. PTEN mutation in endometrial cancers is associated with favorable clinical and pathologic characteristics. Clin Cancer Res. 1998;4(12):3005–10.
Bilbao C, et al. The relationship between microsatellite instability and PTEN gene mutations in endometrial cancer. Int J Cancer. 2006;119(3):563–70.
Djordjevic B, et al. Relationship between PTEN, DNA mismatch repair, and tumor histotype in endometrial carcinoma: retained positive expression of PTEN preferentially identifies sporadic non-endometrioid carcinomas. Mod Pathol. 2013;26(10):1401–12.
Zhang S, Yu D. PI(3)king apart PTEN’s role in cancer. Clin Cancer Res. 2010;16(17):4325–30.
Mackay HJ, et al. Prognostic value of microsatellite instability (MSI) and PTEN expression in women with endometrial cancer: results from studies of the NCIC Clinical Trials Group (NCIC CTG). Eur J Cancer. 2010;46(8):1365–73.
Kanamori Y, et al. PTEN expression is associated with prognosis for patients with advanced endometrial carcinoma undergoing postoperative chemotherapy. Int J Cancer. 2002;100(6):686–9.
Westin SN, et al. PTEN loss is a context-dependent outcome determinant in obese and non-obese endometrioid endometrial cancer patients. Mol Oncol. 2015;9(8):1694–703.
Rudd ML, et al. A unique spectrum of somatic PIK3CA (p110alpha) mutations within primary endometrial carcinomas. Clin Cancer Res. 2011;17(6):1331–40.
Catasus L, et al. Concomitant PI3K-AKT and p53 alterations in endometrial carcinomas are associated with poor prognosis. Mod Pathol. 2009;22(4):522–9.
Velasco A, et al. PIK3CA gene mutations in endometrial carcinoma: correlation with PTEN and K-RAS alterations. Hum Pathol. 2006;37(11):1465–72.
Janku F, et al. PIK3CA mutations in patients with advanced cancers treated with PI3K/AKT/mTOR axis inhibitors. Mol Cancer Ther. 2011;10(3):558–65.
McIntyre JB, et al. PIK3CA missense mutation is associated with unfavorable outcome in grade 3 endometrioid carcinoma but not in serous endometrial carcinoma. Gynecol Oncol. 2014;132(1):188–93.
Huang HN, et al. Ovarian and endometrial endometrioid adenocarcinomas have distinct profiles of microsatellite instability, PTEN expression, and ARID1A expression. Histopathology. 2015;66(4):517–28.
Myers AP. New strategies in endometrial cancer: targeting the PI3K/mTOR pathway–the devil is in the details. Clin Cancer Res. 2013;19(19):5264–74.
Herrero-Gonzalez S, Di Cristofano A. New routes to old places: PIK3R1 and PIK3R2 join PIK3CA and PTEN as endometrial cancer genes. Cancer Discov. 2011;1(2):106–7.
Urick ME, et al. PIK3R1 (p85alpha) is somatically mutated at high frequency in primary endometrial cancer. Cancer Res. 2011;71(12):4061–7.
Wu RC, Wang TL, ShihIe M. The emerging roles of ARID1A in tumor suppression. Cancer Biol Ther. 2014;15(6):655–64.
Bosse T, et al. Loss of ARID1A expression and its relationship with PI3K-Akt pathway alterations, TP53 and microsatellite instability in endometrial cancer. Mod Pathol. 2013;26(11):1525–35.
Allo G, et al. ARID1A loss correlates with mismatch repair deficiency and intact p53 expression in high-grade endometrial carcinomas. Mod Pathol. 2014;27(2):255–61.
Cancer Genome Atlas Research Network, et al. Integrated genomic characterization of endometrial carcinoma. Nature. 2013;497(7447):67–73.
Mao TL, et al. Loss of ARID1A expression correlates with stages of tumor progression in uterine endometrioid carcinoma. Am J Surg Pathol. 2013;37(9):1342–8.
Turbiner J, et al. Clinicopathological and molecular analysis of endometrial carcinoma associated with tamoxifen. Mod Pathol. 2008;21(8):925–36.
Zauber P, et al. Strong correlation between molecular changes in endometrial carcinomas and concomitant hyperplasia. Int J Gynecol Cancer. 2015;25(5):863–8.
Lagarda H, et al. K-ras mutations in endometrial carcinomas with microsatellite instability. J Pathol. 2001;193(2):193–9.
Samarnthai N, Hall K, Yeh IT. Molecular profiling of endometrial malignancies. Obstet Gynecol Int. 2010;2010:162363.
Peterson LM, et al. Molecular characterization of endometrial cancer: a correlative study assessing microsatellite instability, MLH1 hypermethylation, DNA mismatch repair protein expression, and PTEN, PIK3CA, KRAS, and BRAF mutation analysis. Int J Gynecol Pathol. 2012;31(3):195–205.
Lax SF, et al. The frequency of p53, K-ras mutations, and microsatellite instability differs in uterine endometrioid and serous carcinoma: evidence of distinct molecular genetic pathways. Cancer. 2000;88(4):814–24.
Xiong J, et al. Endometrial carcinomas with significant mucinous differentiation associated with higher frequency of k-ras mutations: a morphologic and molecular correlation study. Int J Gynecol Cancer. 2013;23(7):1231–6.
Musa F, et al. Mucinous histology is a risk factor for nodal metastases in endometrial cancer. Gynecol Oncol. 2012;125(3):541–5.
Ito K, et al. K-ras point mutations in endometrial carcinoma: effect on outcome is dependent on age of patient. Gynecol Oncol. 1996;63(2):238–46.
Cohn DE, et al. Genotypic and phenotypic progression in endometrial tumorigenesis: determining when defects in DNA mismatch repair and KRAS2 occur. Genes Chromosom Cancer. 2001;32(4):295–301.
Birkeland E, et al. KRAS gene amplification and overexpression but not mutation associates with aggressive and metastatic endometrial cancer. Br J Cancer. 2012;107(12):1997–2004.
Hachisuga T, et al. K-ras mutation in the endometrium of tamoxifen-treated breast cancer patients, with a comparison of tamoxifen and toremifene. Br J Cancer. 2005;92(6):1098–103.
Tsujioka H, et al. Monitoring of endometrial K-ras mutation in tamoxifen-treated patients with breast cancer. Int J Gynecol Cancer. 2009;19(6):1052–6.
Shoji K, et al. Genotype-dependent efficacy of a dual PI3K/mTOR inhibitor, NVP-BEZ235, and an mTOR inhibitor, RAD001, in endometrial carcinomas. PLoS ONE. 2012;7(5):e37431.
Weigelt B, et al. PI3K pathway dependencies in endometrioid endometrial cancer cell lines. Clin Cancer Res. 2013;19(13):3533–44.
Meyer LA, et al. The search continues: looking for predictive biomarkers for response to mammalian target of rapamycin inhibition in endometrial cancer. Int J Gynecol Cancer. 2014;24(4):713–7.
Iglesias DA, et al. Another surprise from Metformin: novel mechanism of action via K-Ras influences endometrial cancer response to therapy. Mol Cancer Ther. 2013;12(12):2847–56.
Fukuchi T, et al. Beta-catenin mutation in carcinoma of the uterine endometrium. Cancer Res. 1998;58(16):3526–8.
Markowska A, et al. Signalling pathways in endometrial cancer. Contemp Oncol (Pozn). 2014;18(3):143–8.
McConechy MK, et al. Ovarian and endometrial endometrioid carcinomas have distinct CTNNB1 and PTEN mutation profiles. Mod Pathol. 2014;27(1):128–34.
Moreno-Bueno G, et al. Abnormalities of the APC/beta-catenin pathway in endometrial cancer. Oncogene. 2002;21(52):7981–90.
O’Hara AJ, Bell DW. The genomics and genetics of endometrial cancer. Adv Genomics Genet. 2012;2012(2):33–47.
Yeramian A, et al. Endometrial carcinoma: molecular alterations involved in tumor development and progression. Oncogene. 2013;32(4):403–13.
McConechy MK, et al. Use of mutation profiles to refine the classification of endometrial carcinomas. J Pathol. 2012;228(1):20–30.
Saegusa M, et al. beta-Catenin mutations and aberrant nuclear expression during endometrial tumorigenesis. Br J Cancer. 2001;84(2):209–17.
Schlosshauer PW, et al. Mutational analysis of the CTNNB1 and APC genes in uterine endometrioid carcinoma. Mod Pathol. 2000;13(10):1066–71.
Athanassiadou P, et al. The prognostic value of PTEN, p53, and beta-catenin in endometrial carcinoma: a prospective immunocytochemical study. Int J Gynecol Cancer. 2007;17(3):697–704.
Liu Y, et al. Clinical significance of CTNNB1 mutation and Wnt pathway activation in endometrioid endometrial carcinoma. J Natl Cancer Inst. 2014;106(9).
Myers A, et al. beta-Catenin mutations in recurrent FIGO IA grade I endometrioid endometrial cancers. Gynecol Oncol. 2014;134(2):426–7.
Liu Y, Broaddus RR, Zhang W. Identifying aggressive forms of endometrioid-type endometrial cancer: new insights into molecular subtyping. Expert Rev Anticancer Ther. 2015;15(1):1–3.
Olivier M, Hollstein M, Hainaut P. TP53 mutations in human cancers: origins, consequences, and clinical use. Cold Spring Harb Perspect Biol. 2010;2(1):a001008.
Niederacher D, et al. Loss of heterozygosity of BRCA1, TP53 and TCRD markers analysed in sporadic endometrial cancer. Eur J Cancer. 1998;34(11):1770–6.
Graesslin O, et al. Fluorescence in situ hybridization and immunohistochemical analysis of p53 expression in endometrial cancer: prognostic value and relation to ploidy. Ann Surg Oncol. 2008;15(2):484–92.
Luo W, et al. Amifostine enhancement of the anti-cancer effects of paclitaxel in endometrial cancer is TP53-dependent. Int J Oncol. 2010;37(5):1187–94.
Kihana T, et al. Mutation and allelic loss of the p53 gene in endometrial carcinoma. Incidence and outcome in 92 surgical patients. Cancer. 1995;76(1):72–8.
Janiec-Jankowska A, et al. TP53 mutations in endometrial cancers: relation to PTEN gene defects. Int J Gynecol Cancer. 2010;20(2):196–202.
Lee EJ, et al. p53 alteration independently predicts poor outcomes in patients with endometrial cancer: a clinicopathologic study of 131 cases and literature review. Gynecol Oncol. 2010;116(3):533–8.
Stelloo E, et al. Refining prognosis and identifying targetable pathways for high-risk endometrial cancer; a TransPORTEC initiative. Mod Pathol. 2015;28(6):836–44.
Kaku T, et al. Endometrial carcinoma associated with hyperplasia–immunohistochemical study of angiogenesis and p53 expression. Gynecol Oncol. 1999;72(1):51–5.
Jeon YT, et al. Cyclooxygenase-2 and p53 expressions in endometrial cancer. Cancer Epidemiol Biomarkers Prev. 2004;13(9):1538–42.
Semczuk A, et al. Allelic loss at TP53 is not related to p53 protein overexpression in primary human endometrial carcinomas. Oncology. 2005;69(4):317–25.
Ozsaran AA, et al. p53 staining as a prognostic indicator in endometrial carcinoma. Eur J Gynaecol Oncol. 1999;20(2):156–9.
Erdem O, et al. Angiogenesis, p53, and bcl-2 expression as prognostic indicators in endometrial cancer: comparison with traditional clinicopathologic variables. Int J Gynecol Pathol. 2003;22(3):254–60.
Lundgren C, et al. Nuclear DNA content, proliferative activity, and p53 expression related to clinical and histopathologic features in endometrial carcinoma. Int J Gynecol Cancer. 2002;12(1):110–8.
Soong R, et al. Overexpression of p53 protein is an independent prognostic indicator in human endometrial carcinoma. Br J Cancer. 1996;74(4):562–7.
Engelsen IB, et al. Pathologic expression of p53 or p16 in preoperative curettage specimens identifies high-risk endometrial carcinomas. Am J Obstet Gynecol. 2006;195(4):979–86.
Kohler MF, et al. p53 overexpression in advanced-stage endometrial adenocarcinoma. Am J Obstet Gynecol. 1996;175(5):1246–52.
Saffari B, et al. Association of p53 mutations and a codon 72 single nucleotide polymorphism with lower overall survival and responsiveness to adjuvant radiotherapy in endometrioid endometrial carcinomas. Int J Gynecol Cancer. 2005;15(5):952–63.
Oreskovic S, et al. A significance of immunohistochemical determination of steroid receptors, cell proliferation factor Ki-67 and protein p53 in endometrial carcinoma. Gynecol Oncol. 2004;93(1):34–40.
Djordjevic B, Broaddus RR. Role of the clinical pathology laboratory in the evaluation of endometrial carcinomas for Lynch syndrome. Semin Diagn Pathol. 2014;31(3):195–204.
Kawaguchi M, et al. Analysis of candidate target genes for mononucleotide repeat mutation in microsatellite instability-high (MSI-H) endometrial cancer. Int J Oncol. 2009;35(5):977–82.
Maxwell GL, et al. Favorable survival associated with microsatellite instability in endometrioid endometrial cancers. Obstet Gynecol. 2001;97(3):417–22.
Kato M, et al. DNA mismatch repair-related protein loss as a prognostic factor in endometrial cancers. J Gynecol Oncol. 2015;26(1):40–5.
Thoury A, et al. Evidence for different expression profiles for c-Met, EGFR, PTEN and the mTOR pathway in low and high grade endometrial carcinomas in a cohort of consecutive women. Occurrence of PIK3CA and K-Ras mutations and microsatellite instability. Histol Histopathol. 2014;29(11):1455–66.
Zighelboim I, et al. Microsatellite instability and epigenetic inactivation of MLH1 and outcome of patients with endometrial carcinomas of the endometrioid type. J Clin Oncol. 2007;25(15):2042–8.
Black D, et al. Clinicopathologic significance of defective DNA mismatch repair in endometrial carcinoma. J Clin Oncol. 2006;24(11):1745–53.
Cohn DE, et al. Improved survival with an intact DNA mismatch repair system in endometrial cancer. Obstet Gynecol. 2006;108(5):1208–15.
Esteller M, et al. hMLH1 promoter hypermethylation is an early event in human endometrial tumorigenesis. Am J Pathol. 1999;155(5):1767–72.
An HJ, et al. Microsatellite instability in endometrioid type endometrial adenocarcinoma is associated with poor prognostic indicators. Am J Surg Pathol. 2007;31(6):846–53.
Nelson GS, et al. MMR deficiency is common in high-grade endometrioid carcinomas and is associated with an unfavorable outcome. Gynecol Oncol. 2013;131(2):309–14.
Ruiz I, et al. Lack of association between deficient mismatch repair expression and outcome in endometrial carcinomas of the endometrioid type. Gynecol Oncol. 2014;134(1):20–3.
Joehlin-Price AS, et al. Mismatch repair protein expression in 1049 endometrial carcinomas, associations with body mass index, and other clinicopathologic variables. Gynecol Oncol. 2014;133(1):43–7.
Konopka B, et al. Molecular genetic defects in endometrial carcinomas: microsatellite instability, PTEN and beta-catenin (CTNNB1) genes mutations. J Cancer Res Clin Oncol. 2007;133(6):361–71.
Alvarez T, et al. Molecular profile of grade 3 endometrioid endometrial carcinoma: is it a type I or type II endometrial carcinoma? Am J Surg Pathol. 2012;36(5):753–61.
Broaddus RR, et al. Pathologic features of endometrial carcinoma associated with HNPCC: a comparison with sporadic endometrial carcinoma. Cancer. 2006;106(1):87–94.
Tafe LJ, et al. Endometrial and ovarian carcinomas with undifferentiated components: clinically aggressive and frequently underrecognized neoplasms. Mod Pathol. 2010;23(6):781–9.
Garg K, et al. Selection of endometrial carcinomas for DNA mismatch repair protein immunohistochemistry using patient age and tumor morphology enhances detection of mismatch repair abnormalities. Am J Surg Pathol. 2009;33(6):925–33.
Garg K, et al. Endometrial carcinomas in women aged 40 years and younger: tumors associated with loss of DNA mismatch repair proteins comprise a distinct clinicopathologic subset. Am J Surg Pathol. 2009;33(12):1869–77.
Kuhn E, et al. Molecular characterization of undifferentiated carcinoma associated with endometrioid carcinoma. Am J Surg Pathol. 2014;38(5):660–5.
Altrabulsi B, et al. Undifferentiated carcinoma of the endometrium. Am J Surg Pathol. 2005;29(10):1316–21.
Kanopiene D, et al. Impact of microsatellite instability on survival of endometrial cancer patients. Medicina (Kaunas). 2014;50(4):216–21.
Bilbao-Sieyro C, et al. Microsatellite instability and ploidy status define three categories with distinctive prognostic impact in endometrioid endometrial cancer. Oncotarget. 2014;5(15):6206–17.
Cote ML, et al. A pilot study of microsatellite instability and endometrial cancer survival in white and African American women. Int J Gynecol Pathol. 2012;31(1):66–72.
Nick McElhinny SA, et al. Division of labor at the eukaryotic replication fork. Mol Cell. 2008;30(2):137–44.
Pursell ZF, et al. Yeast DNA polymerase epsilon participates in leading-strand DNA replication. Science. 2007;317(5834):127–30.
Church DN, et al. DNA polymerase epsilon and delta exonuclease domain mutations in endometrial cancer. Hum Mol Genet. 2013;22(14):2820–8.
Palles C, et al. Germline mutations affecting the proofreading domains of POLE and POLD1 predispose to colorectal adenomas and carcinomas. Nat Genet. 2013;45(2):136–44.
Govindan R, et al. Genomic landscape of non-small cell lung cancer in smokers and never-smokers. Cell. 2012;150(6):1121–34.
Pleasance ED, et al. A comprehensive catalogue of somatic mutations from a human cancer genome. Nature. 2010;463(7278):191–6.
Church DN, et al. Prognostic significance of POLE proofreading mutations in endometrial cancer. J Natl Cancer Inst. 2015;107(1):402.
Meng B, et al. POLE exonuclease domain mutation predicts long progression-free survival in grade 3 endometrioid carcinoma of the endometrium. Gynecol Oncol. 2014;134(1):15–9.
Forbes SA, et al. COSMIC: mining complete cancer genomes in the catalogue of somatic mutations in cancer. Nucleic Acids Res. 2011;39(Database issue):945–50.
Hussein YR, et al. Clinicopathological analysis of endometrial carcinomas harboring somatic POLE exonuclease domain mutations. Mod Pathol. 2015;28(4):505–14.
Le Gallo M, et al. Exome sequencing of serous endometrial tumors identifies recurrent somatic mutations in chromatin-remodeling and ubiquitin ligase complex genes. Nat Genet. 2012;44(12):1310–5.
Zhao S, et al. Landscape of somatic single-nucleotide and copy-number mutations in uterine serous carcinoma. Proc Natl Acad Sci U S A. 2013;110(8):2916–21.
Kuhn E, et al. Identification of molecular pathway aberrations in uterine serous carcinoma by genome-wide analyses. J Natl Cancer Inst. 2012;104(19):1503–13.
Kim TM, Laird PW, Park PJ. The landscape of microsatellite instability in colorectal and endometrial cancer genomes. Cell. 2013;155(4):858–68.
Heitzer E, Tomlinson I. Replicative DNA polymerase mutations in cancer. Curr Opin Genet Dev. 2014;24:107–13.
Acknowledgement
This work was supported by NIH 1P50CA098258 (SPORE in Uterine Cancer) (RRB) and NIH T32CA101642 (Research Training grant T32) (KCK).
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2017 Springer International Publishing AG
About this chapter

Cite this chapter
Kurnit, K.C., Djordjevic, B., Broaddus, R.R. (2017). Molecular Pathology of Endometrioid Adenocarcinoma. In: Deavers, M., Coffey, D. (eds) Precision Molecular Pathology of Uterine Cancer. Molecular Pathology Library, vol 11. Springer, Cham. https://doi.org/10.1007/978-3-319-57985-6_4
Download citation
DOI: https://doi.org/10.1007/978-3-319-57985-6_4
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-57983-2
Online ISBN: 978-3-319-57985-6
eBook Packages: MedicineMedicine (R0)