
Abstract
The accuracy and reproducibility of the femtosecond laser has made it an ideal tool to perform astigmatic keratotomy. The laser can potentially offer no skipped lesions, minimized risk of perforation, and increased precision through reproducible incision depth, length, angulation, and centration. The incisions can be made both full thickness and intrastromal. Compared with manual astigmatic keratotomy, the results were similar; however, it was less likely to have an axis shift or misalignment.
Access provided by CONRICYT-eBooks. Download chapter PDF
Similar content being viewed by others


1 Background
The femtosecond laser is an ultrashort pulse laser (100 fs or 10−13 s) that operates in the infrared wavelength (~1045 nm). It causes photoionization of the tissue resulting in vaporization and the formation of cavitation bubbles. The bubbles consist of carbon dioxide and water which is dissipated in the tissue, forming a cleavage plane. Its precise and controllable properties allow for many ocular applications from the creation of corneal flap in laser-assisted in situ keratomileusis to the capsularhexis in cataract surgery.
The accuracy and reproducibility of the laser makes it an ideal tool to address the variability in performing astigmatic keratotomy. The femtosecond laser potentially offers no skip lesions, minimized risk of perforation, and increased precision through reproducible incision depth, length, angulation, and centration. This provides a safe and consistent means of performing astigmatic keratotomy.
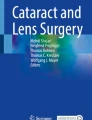
Femtosecond astigmatic keratotomy (FSAK) can create three types of incisions. These include full thickness, intrastromal, and reverse full thickness (Fig. 7.1). Of these, full thickness is the only incision available using manual techniques. Stabilization has been shown to occur after a minimum of 3 months [1]. While the long-term stability and regression in manual techniques have been described, there are only short-term results for FSAK. The full-thickness incisions may have similar regression to manual techniques, but there is no published comparative data. In contrast, intrastromal FSAK has short-term data showing clinically insignificant regression over 6 months [2].

The theoretically types of incision that can be made in femtosecond astigmatic keratotomy. (a) Full thickness, (b) Intrastromal, (c) Reverse full thickness
Intrastromal FSAK has the benefit of not disrupting the epithelium or Bowman’s. This results in minimal wound healing and no fibroblast growth [3] that is associated with visual symptoms such as glare and halos. As the epithelium is not disturbed, these patients are comfortable and asymptomatic postoperatively. As the integrity of Bowman’s is kept intact, the intrastromal FSAK has mostly been studied in minor or medium astigmatism—up to 3.5D. There is, however, one case report of it successfully treating a post-penetrating keratoplasty (PKP) patient with reduction in cylinder from 10.4D to 1.12D [4].
2 Surgical Planning
Preoperative evaluation of the patient should include a comprehensive exam and a combination of objective testing that may include keratometry, corneal topography, corneal tomography, pachymetry, and anterior segment optical coherence tomography. Those patients with ectatic disorders or highly irregular astigmatism can be identified as they need to be approached with caution with FSAK [1].
There are numerous described nomograms that vary the treatment parameters (depth, arc length, optical zone diameter) based on the amount of astigmatism and patient age. Most of these are based on the nomograms available for manual AK that have been adjusted. One such modification is using 70% of the Donnenfeld nomogram. Our current nomogram consists of paired incisions, 85% depth, 80 μm below anterior surface, and 8.5 mm optical zone. The arc length depends on the axis and amount of astigmatism (Table 7.1). There is no augmentation performed, and if the patient needs more correction, then laser vision correction is offered.
There is only one study that has specifically developed a nomogram for FSAK after PKP and DALK [5]. The presence of peripheral blood vessels will interfere with the laser, so the location of the optical zone may need to be adjusted. The plasma shape of the laser and its extension beyond the set depth needs to be considered to avoid accidental perforation.
3 Surgical Technique
There are several commercially available femtosecond laser systems available that can perform astigmatic keratotomy. The settings will vary with each machine as per the manufactures guidelines.
To compensate for cyclotorsion, marking the limbus preoperatively at the slit lamp has been advocated. The patient is then prepped and anesthetized topically. In some devices, the axis is required to be marked and the pachymetry measured to be used to calculate the depth prior to engaging the suction ring. The more recent devices have built-in optical coherence tomography that allows for real-time measurement and simultaneous treatment. Once the suction ring is used to secure the eye, the applanation cone is applied and can be adjusted to ensure proper alignment. The inputted treatment parameters are then applied and the incisions created (Video 7.1). After creation, the applanation cone and suction ring are released. In full-thickness incisions, the incisions can be opened using a Sinskey hook. This can be done at the time of surgery or even delayed by several weeks.
4 Outcomes
Most of the early use of FSAK has been reported in patients following penetrating keratoplasty (PKP) [1, 6,7,8,9,10,11,12,13]. Its use in patients after cataract surgery [14, 15], after previous refractive surgery [16], after Descemet stripping automated endothelial keratoplasty [17, 18], and in those with naturally occurring high astigmatism [19] has also been reported. With the advent of femto-assisted cataract surgery, FSAK has been incorporated into treatment at the time of cataract surgery [2]. As shown in Table 7.2, there was a marked reduction in keratometric astigmatism following the treatment. This correction also resulted in improvement in the patients uncorrected visual acuity as well.
Comparing FSAK to manual astigmatic keratotomy, the results were similar; however, the manual technique had a tendency for greater axis misalignment or a shift in the astigmatism axis [6, 9]. In a randomized comparison between FSAK and manual AK, there was no significant difference in the worsening of high-order aberrations. The FSAK group had better uncorrected visual acuity and best correct visual acuity than manual AK [6].
5 Complications
Perforation is more likely to occur with manual AK with both comparative studies having perforations in manual AK and none in the FSAK [6, 9]. There is one report of a perforation after FSAK in a post-Descemet stripping automated endothelial keratoplasty patient, where it was recommended to not count the graft thickness into corneal thickness calculation [18].
Overcorrection is also more likely to occur in patients who have ectatic corneas [1]. In all studies published, excepted one case report [18], there was improvement in the patient’s astigmatism.
The potential complications that can occur include transecting the corneal nerves and reducing corneal sensation, endothelial damage from the energy, incomplete cylinder creation, and no separation of the arc walls. Eye rotation or coronal movement at the time of laser can result in imprecise treatment. With the modification of the cornea, there exists the long-term risk of ectasia. This is likely lower with intrastromal FSAK, but there are no long-term studies to support this.
Conflict of Interests
G. Belovay—none
B. Khan—Consultant with Alcon, AMO, Bausch & Lomb, Allergan and Zeiss
References
Kumar NL, Kaiserman I, Shehadeh-Mashor R, Sansanayudh W, Ritenour R, Rootman DS. IntraLase-enabled astigmatic keratotomy for post-keratoplasty astigmatism: on-axis vector analysis. Ophthalmology. 2010;117:1228–1235.e1. https://doi.org/10.1016/j.ophtha.2009.10.041.
Day AC, Stevens JD. Stability of keratometric astigmatism after non-penetrating femtosecond laser intrastromal astigmatic keratotomy performed during laser cataract surgery. J Refract Surg. 2016;32:152–5. https://doi.org/10.3928/1081597X-20160204-01.
Meltendorf C, Burbach GJ, Buhren J, Bug R, Ohrloff C, Deller T. Corneal femtosecond laser keratotomy results in isolated stromal injury and favorable wound-healing response. Invest Ophthalmol Vis Sci. 2007;48:2068–75. https://doi.org/10.1167/iovs.06-1150.
Viswanathan D, Kumar NL. Bilateral femtosecond laser-enabled intrastromal astigmatic keratotomy to correct high post-penetrating keratoplasty astigmatism. J Cataract Refract Surg. 2013;39:1916–20. https://doi.org/10.1016/j.jcrs.2013.08.019.
St Clair RM, Sharma A, Huang D, Yu F, Goldich Y, Rootman D, Yoo S, Cabot F, Jun J, Zhang L, Aldave AJ. Development of a nomogram for femtosecond laser astigmatic keratotomy for astigmatism after keratoplasty. J Cataract Refract Surg. 2016;42:556–62. https://doi.org/10.1016/j.jcrs.2015.12.053.
Bahar I, Levinger E, Kaiserman I, Sansanayudh W, Rootman DS. IntraLase-enabled astigmatic keratotomy for postkeratoplasty astigmatism. Am J Ophthalmol. 2008;146:897–904.e1. https://doi.org/10.1016/j.ajo.2008.07.004.
Buzzonetti L, Petrocelli G, Laborante A, Mazzilli E, Gaspari M, Valente P. Arcuate keratotomy for high postoperative keratoplasty astigmatism performed with the intralase femtosecond laser. J Refract Surg. 2009;25:709–14.
Harissi-Dagher M, Azar DT. Femtosecond laser astigmatic keratotomy for postkeratoplasty astigmatism. Can J Ophthalmol. 2008;43:367–9. https://doi.org/10.3129/i08-043.
Hoffart L, Proust H, Matonti F, Conrath J, Ridings B. Correction of postkeratoplasty astigmatism by femtosecond laser compared with mechanized astigmatic keratotomy. Am J Ophthalmol. 2009;147:779–787., 787.e1. https://doi.org/10.1016/j.ajo.2008.12.017.
Kiraly L, Herrmann C, Amm M, Duncker G. Reduction of astigmatism by arcuate incisions using the femtosecond laser after corneal transplantation. Klin Monatsbl Augenheilkd. 2008;225:70–4. https://doi.org/10.1055/s-2008-1027126.
Kook D, Buhren J, Klaproth OK, Bauch AS, Derhartunian V, Kohnen T. Astigmatic keratotomy with the femtosecond laser: correction of high astigmatisms after keratoplasty. Ophthalmologe. 2011;108:143–50. https://doi.org/10.1007/s00347-010-2239-z.
Kymionis GD, Yoo SH, Ide T, Culbertson WW. Femtosecond-assisted astigmatic keratotomy for post-keratoplasty irregular astigmatism. J Cataract Refract Surg. 2009;35:11–3. https://doi.org/10.1016/j.jcrs.2008.08.039.
Nubile M, Carpineto P, Lanzini M, Calienno R, Agnifili L, Ciancaglini M, Mastropasqua L. Femtosecond laser arcuate keratotomy for the correction of high astigmatism after keratoplasty. Ophthalmology. 2009;116:1083–92. https://doi.org/10.1016/j.ophtha.2009.01.013.
Nejima R, Terada Y, Mori Y, Ogata M, Minami K, Miyata K. Clinical utility of femtosecond laser-assisted astigmatic keratotomy after cataract surgery. Jpn J Ophthalmol. 2015;59:209–15. https://doi.org/10.1007/s10384-015-0383-3.
Ruckl T, Dexl AK, Bachernegg A, Reischl V, Riha W, Ruckhofer J, Binder PS, Grabner G. Femtosecond laser-assisted intrastromal arcuate keratotomy to reduce corneal astigmatism. J Cataract Refract Surg. 2013;39:528–38. https://doi.org/10.1016/j.jcrs.2012.10.043.
Venter J, Blumenfeld R, Schallhorn S, Pelouskova M. Non-penetrating femtosecond laser intrastromal astigmatic keratotomy in patients with mixed astigmatism after previous refractive surgery. J Refract Surg. 2013;29:180–6. https://doi.org/10.3928/1081597X-20130129-09.
Levinger E, Bahar I, Rootman DS. IntraLase-enabled astigmatic keratotomy for correction of astigmatism after Descemet stripping automated endothelial keratoplasty: a case report. Cornea. 2009;28:1074–6. https://doi.org/10.1097/ICO.0b013e318199fa2c.
Yoo SH, Kymionis GD, Ide T, Diakonis VF. Overcorrection after femtosecond-assisted astigmatic keratotomy in a post-Descemet-stripping automated endothelial keratoplasty patient. J Cataract Refract Surg. 2009;35:1833–4. https://doi.org/10.1016/j.jcrs.2009.06.017.
Abbey A, Ide T, Kymionis GD, Yoo SH. Femtosecond laser-assisted astigmatic keratotomy in naturally occurring high astigmatism. Br J Ophthalmol. 2009;93:1566–9. https://doi.org/10.1136/bjo.2008.149971.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
1 Electronic Supplementary Materials
Femtosecond laser arcuates
Rights and permissions
Copyright information
© 2018 Springer International Publishing AG
About this chapter
Cite this chapter
Belovay, G.W., Khan, B. (2018). Correction of Corneal Astigmatism with Femtosecond Relaxing Incisions. In: Febbraro, JL., Khan, H., Koch, D. (eds) Surgical Correction of Astigmatism. Springer, Cham. https://doi.org/10.1007/978-3-319-56565-1_7
Download citation
DOI: https://doi.org/10.1007/978-3-319-56565-1_7
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-56563-7
Online ISBN: 978-3-319-56565-1
eBook Packages: MedicineMedicine (R0)