
Abstract
Frontotemporal dementia (FTD) comprises two primary variants: behavioral variant FTD (bvFTD) and primary progressive aphasia (PPA). BvFTD includes prominent behavioral disinhibition, apathy and inertia, loss of empathy or sympathy, perseverative stereotyped or ritualistic behaviors, and hyperorality and dietary changes. The diagnosis of PPA is based on an insidious decline in language, which must remain the most prominent deficit for the initial 1–2 years, and be the principle cause of impairment of Activities of Daily Living. There is a non-fluent variant of PPA, a semantic variant of PPA, and logopenic variant of PPA. The latter is typically due to Alzheimer’s disease. The former may be secondary to tau or TDP-43 pathology. There is no specific pharmacologic treatment for FTD.
Access provided by CONRICYT-eBooks. Download chapter PDF
Similar content being viewed by others

Keywords
- Frontotemporal dementia
- Frontotemporal lobar degeneration
- Primary progressive aphasia
- Non-fluent variant of primary progressive aphasia
- Semantic variant of primary progressive aphasia
- Logopenic variant of primary progressive aphasia
- Motor neuron disease
- Pick’s disease
- Tau protein
- TDP-43 protein
Clinical Pearls
-
Although considered a “young-onset” dementia, FTD can occur at later ages, with approximately 25% of patients occurring after age 65.
-
The early accurate diagnosis of bvFTD depends on a detailed history of significant behavioral changes representing a departure from the premorbid state. Neuropsychological assessment and imaging alone are not sufficient for a diagnosis.
-
Motor changes can emerge as FTD progresses, but can also be present at the time of diagnosis. These take the form of Parkinsonism (PSP and CBD—usually associated with tau pathology) or motor neuron disease (MND or ALS—invariably associated with TDP-43 pathology).
-
Isolated progressive language deficits must be present for at least 1 or 2 years for PPA to be diagnosed. These language deficits must remain the principle cause of disability as the disease progresses.
-
FTD is a highly genetic syndrome, with up to 50% of patients showing a strong familial inheritance. Many genes have been identified, but MAPT, C9orf72, and GRN account for most familial cases.
-
The underlying pathology in FTD is complex. Although any one case will generally be the consequence of a single pathology, FTD remains a syndrome that results from many possible processes, the two most common being tau and TDP-43.
-
There are no specific treatments for FTD or PPA. Unless Alzheimer’s disease pathology is highly suspected (as in lvPPA), there is no role for cholinesterase inhibitors or memantine, which may worsen the clinical symptoms. Serotonergic agents are the treatment of choice for behavioral changes. Non-pharmacologic management such as the “ABC” approach may be useful.
Introduction—Nomenclature, Epidemiology, Genetics, and Pathology
Frontotemporal dementia (FTD) is a term used to express a collection of possible clinical presentations that develop as the consequence of one of a number of distinct pathologic processes. Frontotemporal Lobar Degeneration (FTLD ) is a pathological term that refers to the fairly selective degeneration of the frontal and anterior temporal lobes and results in the clinical manifestations of FTD [1]. Although these clinical manifestations are fairly consistent, the underlying pathological processes can be varied.
Reflecting its focal onset, FTD presents classically as a progressive degenerative disorder involving the initially selective disintegration of either behavior (behavioral variant FTD or bv-FTD) or language (primary progressive aphasia—PPA). PPA generally evolves from one of three different patterns of speech dysfunction: semantic dementia (or semantic variant, sv-PPA), non-fluent or agrammatic variant (nfv-PPA) and the logopenic variant (lv-PPA). Behavioral variants account for nearly 60% of cases while PPA accounts for 40% [2]. There is also significant overlap with movement disorders (progressive supranuclear palsy and corticobasal degeneration—PSP and CBD) and motor neuron disease or amyotrophic lateral sclerosis (MND/ALS). Patients may initially present with a defined clinical syndrome, such as nfv-PPA, and then evolve to develop features of CBD, PSP, or even MND [3, 4]. Some have recommended the use of “overlap” terms such as PPA-CBD to better reflect this evolution [5].
Although often a “young-onset” dementia, accounting for nearly half of dementias occurring before age 65 [6], FTD also affects older patients. One quarter of patients with FTD present after age 65, often being misdiagnosed as AD [7]. Younger onset patients are often misdiagnosed with psychiatric disorders, including depression, obsessive compulsive disorder (OCD), bipolar disorder, and even schizophrenia [8]. The reported prevalence of FTD varies, but is estimated at 15–22/100,000 [7]. Average age of presentation is in the sixth decade. There may be a slight overrepresentation of male patients.
FTD is a highly heritable disease. As many as 50% of cases report a family history with approximately 15% showing a clear autosomal dominant pattern of inheritance [9], with most familial cases explained by one of three common mutations (Microtubule Associated Protein Tau—MAPT, progranulin—GRN, and Chromosome 9 open reading frame 72—C9orf72). Together, these three mutations account for up to 20% of all cases of FTD.
Unlike Alzheimer’s disease, in which diagnostic pathological changes must include the combined presence of both amyloid-based plaques and tau-based neurofibrillary tangles, pathologic changes in FTLD can be varied. Two different abnormal inclusions each account for about 45% of cases. These are accumulations of either abnormal tau or TDP-43 . The remaining 10% of cases include FUS based pathology (FUsed in Sarcoma) or other yet to be characterized changes. Pathologic MAPT mutations always lead to tau pathology, while mutations in GRN and C9orf72 result in TDP-43 related changes. Clinically, cases that progress to include movement disorders tend to be the consequence of tau changes, while the development of motor neuron disease is almost exclusively the result of TDP-43 pathology.
Although frequently used interchangeably, Pick’s disease (PiD) is currently considered a subgroup of the FTLDs. It is pathologically defined by the presence of circumscribed frontotemporal atrophy and associated tau containing intraneuronal agyrophilic spherical aggregations called Pick bodies.
Clinical Manifestations, Radiologic Findings, and Diagnostic Criteria
Patients with FTD present with insidious changes involving either behavior (bvFTD) and/or language (PPA) and the core diagnostic criteria reflect this dichotomy [10, 11].
Behavioral Variant FTD (bvFTD)
The primary manifestations of bvFTD involve early progressive changes in socioemotional behavior or comportment, and include (1) behavioral disinhibition, (2) apathy and inertia, (3) loss of sympathy or empathy, (4) perseverative, stereotyped or compulsive/ritualistic behaviors, and (5) hyperorality and dietary changes. (6) Cognitive changes may also be present and involve executive/generation deficits with relative preservation of memory and visual spatial abilities.
Apathy and inertia are possibly the earliest and most common manifestations and can present as subtle changes such as difficulties making decisions, increased passivity, and reduced interest in usual hobbies. Progression often leads to more significant and impactful changes such as reduced attention to (or care about) work and home responsibilities, and personal hygiene. Early loss of functional independence is not uncommon, despite relative preservation of cognition.
Disinhibition may be less common than apathy, but is often more disruptive. Socially inappropriate behaviors and loss of decorum or manners are embarrassing to family and include excessive familiarity, inappropriate touching or hugging of strangers, or loud rude unconsidered remarks (such as about people’s weight or appearance). Disinhibition can also take the form of impulsivity and lead to rash or careless actions. Criminal behavior, including speeding, theft (i.e., shoplifting), public nudity or urination, and even assault, can occur.
Loss of empathy usually manifests as reduced personal warmth and affection towards love ones. There is often inability to properly appreciate or respond to others’ needs or emotions. This may manifest as striking selfishness or lack of concern for a loved ones’ illness or tragedy.
Compulsive, repetitive, or ritualistic behaviors can take on various forms. There can be repetitive stereotyped behaviors such as incessant humming, rocking, or tapping. Verbal stereotypies may include repetition of words or catch phrases. Obsessive cleaning and insistence on rigid orderliness can occur. Other complex behaviors may involve hoarding, repetitive trips to the bathroom, or rigid and ritualistic feeding habits (such as eating only certain foods at certain times).
Dietary changes may include excessive sometimes compulsive binge eating (even in the face of satiety), new food preferences (most often for carbohydrates) or rigid or ritualistic food fads. There may be disregard for the poor comestible nature of the food in question (eating discarded foods from the garbage). There may even be consumption of inedible objects such as buttons or coins. Weight gain is common and is a relatively unique feature of FTD.
Early cognitive changes are usually subtle and may not be detectable with routine bedside diagnostic testing. Neuropsychological testing may capture deficits in attention and executive functions: working memory, cognitive flexibility and control (set-shifting), generation (lexical fluency), and abstraction. Performance in other cognitive domains, in particular episodic memory and visual spatial functions is generally sparred, although there are documented exceptions. Experimental tasks that probe Theory of Mind or social cognition may turn out to be most sensitive to early changes, but their development has not yet reached widespread clinical use. Failure on any task may be more the consequence of rule-breaking or poor effort than from an actual cognitive deficit.
Additional manifestations of the disease not captured by the diagnostic criteria can include psychosis, mood disorder, or OCD. Coupled with the relative initial mildness and frequent delayed appearance of cognitive deficits, as well as the younger age of onset, these changes often lead to psychiatric misdiagnosis for as many as 50% of patients [12]. This results in diagnostic and effective treatment delays.
Another critical finding in patients with bvFTD is the early presence of profound anosodiaphoria (awareness of a deficit but absence of adequate concern about its importance or impact) or anosognosia (lack of awareness altogether).
Physical examination in bvFTD is usually normal. As the disease evolves, patients may begin to show signs of asymmetric or axial extrapyramidal involvement, apraxia, eye movement abnormalities, and early falls, heralding a clinical trajectory towards CBD or PSP, or upper and lower motorneuron disease (weakness, spasticity, and fasciculations), betraying the development of FTD-ALS. These disorders are discussed elsewhere in this book. Occasionally, ALS or CBD/PSP disorders can be the initial manifestations of an FTLD -based pathology, and behavioral or language changes appear later in the course of the disease.
Radiological Findings
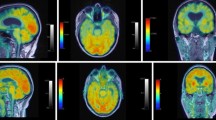
Using the Rascovsky criteria , the presence of characteristic findings on brain imaging raise the diagnostic confidence of bvFTD from possible to probable (Figs. 9.1 and 9.2). These include early and isolated, often circumscribed frontal and/or anterior temporal atrophy on magnetic resonance imaging (MRI) or computerized tomography (CT), or hypoperfusion or hypometabolism in the same areas on single photon emission computed tomography (SPECT) or fluorodeoxyglucose positron emission tomography (FDG) PET scan. For bvFTD, right-sided predominance of abnormalities is more frequent. SPECT or PET finding may precede the development of MRI changes by a few years. Absence of atrophy on MRI does not exclude the diagnosis. Conversely, the presence of such atrophy should never lead to a diagnosis in the absence of the clinical syndrome.

FDG-PET (axial view). Note profound hypometabolism involving anterior right frontal mesial, polar, and convexity

FLAIR-MRI (axial view). Note knife-like cortical atrophy of frontal areas
New imaging techniques such as resting state functional MRI (fMRI) may reveal very early disintegration of key networks involving the anterior cingulate and frontoinsular cortices. Further development will be required before these can be applied clinically.
Each group of behavioral changes described above have been attributed to pathologic involvement of specific brain areas or disruption of networks involving: (1) anterior cingulate for apathy, (2) right orbitofrontal for disinhibition, (3) right frontoinsular and anterior temporal for loss of empathy, (4) lateral temporal and basal ganglia for compulsive behaviors, and (5) right orbitofrontal and insular cortices, and ventral striatum and hypothalamus for dietary or appetitive changes. The presence of specific behavioral changes and matching atrophy patterns on brain imaging (MRI or PET) help bolster diagnostic confidence.
Diagnosis of bvFTD
The diagnosis of possible bvFTD requires the clinician to elicit at least three of the six core behavioral (5) and cognitive (1) criteria described above (Table 9.1 and “Diagnostic flowchart for bvFTD”; Fig. 9.3). Because of the presence of early anosognosia, a detailed interview with a reliable caregiver or life partner is usually necessary. Although many of the relevant changes are sometimes spontaneously volunteered, directed questioning with examples as described above are often required. Neuropsychological testing may be required to capture the presence of early executive dysfunction. In moderately advanced cases, bedside cognitive testing (such as a Montreal Cognitive Assessment [MoCA]) may be adequate. Patients with early disease may not initially meet three criteria and reassessment in 6–12 months may be required. The diagnosis becomes probable when corresponding imaging abnormalities are found on MRI/CT or PET/SPECT and there is clear functional decline. The Rascovsky criteria have been found to be 85–95% sensitive and 82% specific for a diagnosis of possible bvFTD and 75–85% sensitive and 95% specific for probable bvFTD [10, 13]. Interrater reliability is also very high at 0.81 and 0.82 for possible and probable disease [14]. The presence of a pathologic mutation or confirmation (biopsy or post-mortem) of histopathologic changes raise the level diagnostic certainty to one of “definite”.

Diagnostic flowchart for bvFTD
The presence of any non-degenerative neurological, medical, or psychiatric disorder that better accounts for the behavioral changes should preclude a diagnosis of bvFTD. The presence of biomarkers that strongly support other neurodegenerative diseases (AD, Lewy body diseases, vascular disease) is allowed in “possible” bvFTD, but would exclude a “probable” diagnosis.
Primary Progressive Aphasia (PPA)
There are three variants of PPA: nonfluent/agrammatic (nfv), semantic (sv), and logopenic (lv) [11, 15]. While the histological changes underlying semantic and nonfluent variants are most often consistent with FTLD , the logopenic variant is more frequently (although not exclusively) the consequence of Alzheimer’s disease pathology. The 2011 Gorno-Tempini criteria allow for the classification of most progressive aphasias, but some patients may fail to meet criteria for any, or meet them for more than one, leading to terms such as “mixed” PPA (PPA-M) [16] or “not otherwise specified” (PPA-NOS) [5]. Closely related to nfv-PPA, primary progressive apraxia or speech (PPAoS) has been described and is characterized by impaired articulation and production as a consequence of a breakdown in motor programming, with a general sparing of language, at least initially [17].
Diagnosis of PPA is a two-step process. Before subtyping, patients must first meet basic PPA criteria as defined by Mesulam [11, 18, 19]: there must be (A) an insidious isolated decline in language, affecting at least one of speech production, object naming, syntax, or word comprehension, and (B) the aphasia must be the most prominent deficit for at least the initial 1–2 years and remain the principle cause of any impairment in activities of daily living (ADLs) (see “Diagnostic flow chart for PPA”; Fig. 9.4).

Diagnostic flowchart for PPA
Further characterization of the aphasia can normally be accomplished by examining the main language domains, through simple observation and specific tasks. These domains include speech production (grammar, motor speech, sound errors, and word finding pauses), repetition (both short and longer sentences), single-word and syntax comprehension, confrontational naming, semantic knowledge, and reading/spelling [11]. See Table 9.1 for diagnostic criteria. See also “Approach to the clinical evaluation of a speech disorder” and to Table 9.2 for examples of tests and criteria specific findings. See the “Simplified flowchart for the diagnosis of PPA” for a streamlined approach based on the most critical diagnostic findings (Fig. 9.5).

Simplified flowchart for diagnosis of PPA variants
As with bvFTD, there are levels of confidence in the diagnosis: clinical, “imaging-supported”, and pathologic. Clinical diagnosis depends on the classification of the patient’s deficits according to the clinical criteria explored below. Once clinical criteria are met, imaging-supported criteria are considered. Because there is generally a direct correspondence between language symptoms and the site of anatomic damage, there must be structural or functional imaging changes in a distribution consistent with the clinical syndrome. A particular genetic mutation or specific pathology defines the disorder as FTLD spectrum, AD, or some other known disease entity. Unfortunately, pathologic diagnoses do not further enhance characterization of the clinical syndrome as there is significant overlap between clinical presentations and possible underlying pathologies. Mixed pathologies are also not uncommon in older patients.
Nonfluent Variant PPA (nfvPPA)
NfvPPA is characterized by early difficulties in motor speech output and loss of syntax (Table 9.1). Speech is effortful (slow and labored), with frequent pauses and grammatical errors. Utterances are generally short and simple, with omission of function words and inflections. There may be articulatory deficits with inconsistent speech sound errors, including distortions, deletions, substitutions, insertions, or transpositions of speech sounds. Prosody is usually also affected. Patients are often aware of, and frustrated by, these deficits. Spared are single-word comprehension and object knowledge. There may be deficits in comprehension of grammatically complex sentences.
In some patients, very mild apraxia or slowing of fine finger movements may be present. These findings are harbingers as progression predominantly involves the development of motor changes consistent with CBD or PSP.
MRI shows focal atrophy and FDG-PET reveals focal hypometabolism involving left posterior frontal and insular regions (Figs. 9.6 and 9.7). The most frequent histopathology is tau, with less frequent cases involving TDP-43. Well characterized nfvPPA is almost never the consequence of AD pathology.

FDG-PET (axial view). Note subtle hypometabolism involving left anterior perisylvian (frontal opercular) areas

T1-MRI (axial view). Note extensive atrophy of anterior perisylvian areas on the left relative to the right
Semantic Variant PPA (svPPA)
Previously labeled Semantic Dementia, this clinical syndrome is characterized by the presence of anomia and single-word comprehension deficits (Table 9.1). These represent core features and both must be present for the diagnosis. Anomia is not uncommon in many neurodegenerative conditions, but it tends to be severe in svPPA, in which additional information about the object in question (“object knowledge”, a form of semantic knowledge) may also be missing. A pen, for instance, is held in the dominant hand in a particular way and is used for writing. This kind of information may be completely lost, especially for less common (low-frequency) words—contrast for instance the less common word “zebra” with the more common or familiar “cat”.
Single-word comprehension deficits arise when the patient cannot recognize, describe, or define an object or idea. It is also the consequence of loss of object knowledge. When asked to draw a clock, patients with moderately severe svPPA may simply say: “Clock? What’s a clock?”. They will be unable to name a clock when shown a picture or a cartoon of one, know that clocks are used to tell time, or recognize “tic-toc” as the sound that a clock may produce. As suggested by the eventual inability to recognize the sound “tic-toc”, deficits in object recognition and knowledge can be multimodal. Recognition failure will ultimately transcend all sensory modalities such that the tactile experience of a rose petal or thorn, or the scent of its flower, will not be of any additional benefit in identifying a rose bush.
Early deficits in naming and word comprehension usually involve low-frequency words, but with progression, the meaning and semantic knowledge of more common words will also be lost. Selective involvement of certain object categories (tools, animals, people, or concrete vs. abstract) may be present early, but all are involved, eventually.
Another consequence of loss of object or word knowledge is the inability to recognize words with irregular spelling or pronunciation (e.g. “yacht”, “colonel”, and “cellist”). This results in so-called surface dyslexia and dysgraphia , where the patient will “regularize” such words when read or written: the word colonel would be read as “kol-o-nel” and written in some form to sound like “kur-nl”.
Typically, even in advanced disease, repetition and motor speech remain intact. Adequate grammar, albeit with a shrinking vocabulary pool, is generally retained.
Even in the earliest stages, PET and MRI show focal hypometabolism or atrophy in the lateral and ventral aspects of the temporal poles, usually more prominent on the left (Figs. 9.8 and 9.9). Although uncommon, preferential involvement of the right temporal lobe can occur and results in a more behavioral syndrome (the so-called right-temporal variant FTD [20]).

FDG-PET (axial view). Note profound hypometabolism of the left anterior temporal lobe

T1-MRI (axial view). Note profound cortical atrophy of the left anterior temporal lobe with involvement of the hippocampus
The pathological findings in svPPA are more frequently TDP-43 related, although there are case reports of abnormal tau deposition [21]. Genetics are rarely involved.
Logopenic Variant PPA (lvPPA)
Logopenic variant PPA is the most recently described language variant [22]. The most salient features are word retrieval and length-dependent sentence repetition deficits (Table 9.1). Word retrieval or word finding deficits are most obvious during spontaneous speech or conversation. Speech is slowed, with frequent word finding pauses, but without agrammatism. Prosody is generally conserved, although the word-finding pauses disrupts the natural flow and can be frustrating to both the speaker and listener. Naming difficulties (anomia) may be present, but object knowledge is preserved so that the patient may describe objects in other more roundabout ways (circumlocution). Single word comprehension is also intact.
The disorder is thought to arise from damage to structures supporting phonologic short term memory (left temporoparietal areas). This type of memory is critical in word and sentence repetition. With disease progression, there is a gradual length-dependent sentence repetition deficit. The patient is able to repeat single words and short sentences, but fails to repeat longer sentences, regardless of their grammatical complexity. A similarly length-dependent deficit will emerge affecting sentence comprehension.
Additional features include phonologic paraphasias (e.g., “greel” for “green”) during spontaneous speech and confrontational naming. Words are misspoken because of phonetic substitutions, but there is no distortion of the word sounds, as seen in nfvPPA.
PET and MRI imaging abnormalities involve the left temporoparietal junction (Figs. 9.10 and 9.11). When lvPPA is well characterized, the underlying pathology is most often Alzheimer’s disease, although there are published exceptions, with FTD-type pathology.

FDG-PET (axial view). Note presence of bilateral parieto-temporal hypometabolism characteristic of AD, worse on the left

T1-MRI (axial view). Note selective posterior perisylvian atrophy, much worse on the left
Differential Diagnosis
As for all conditions leading to gradual changes in mental status, reversible causes should be excluded. These involve endocrine, metabolic, and neoplastic or paraneoplastic conditions, central nervous system (CNS) infections, and dietary deficiencies.
The differential diagnosis for FTD will vary according to age. In younger patients it is often misdiagnosed as atypical depression, bipolar disorder, or late onset schizophrenia. Early-onset Alzheimer’s disease can sometimes be difficult to differentiate clinically. Analysis of cerebrospinal fluid (CSF) for A-beta and tau proteins, demonstration of hippocampal atrophy on volumetric MRI, temporoparietal and posterior cingulate hypometabolism (rather than frontotemporal) on FDG PET, or the presence of amyloid on amyloid PET help accurately diagnose Alzheimer’s disease. Late-onset major psychiatric disease should always raise suspicion for the presence of bvFTD.
In older patients, atypical depression, Alzheimer’s disease, and Vascular Cognitive Impairment (VCI) are more frequent. Careful attention to the core criteria and a search for clinically consistent focal hypometabolism on PET and atrophy MRI, as well as absence of significant or strategic vascular disease, will generally lead to an accurate diagnosis.
Because of its slow evolution, progressive aphasia is rarely confused with aphasias due to stroke or space occupying lesions. Alzheimer’s disease represents the most common alternative diagnosis and is the most common pathological finding in lvPPA. CSF analysis for A-beta and tau, volumetric MRI and FDG or amyloid PET are helpful in this regard. CSF is typically normal in FTD; in Alzheimer’s disease, the signature findings are elevated tau protein and reduced A-beta protein levels. If the clinical syndrome can be well characterized into one of the three PPA variants, the differential diagnosis becomes moot.
Treatment
As is the case for Alzheimer’s disease, there are currently no approved or established treatments that address the underlying pathology or disease progression of FTD. Current approaches focus on addressing individual symptoms and promoting increased brain health and resilience (see healthybrains.org). Support and education of both patients and caregivers is critical. Education can be enhanced through referral to support groups and social work. The Association for Frontotemporal Degeneration (AFTD) and the Alzheimer’s Association offer useful resources (www.theaftd.org & http://www.alz.org/dementia/fronto-temporal-dementia-ftd-symptoms.asp). Unfortunately, there still exit significant barriers to helping patients with FTD and their families access adequate care and resources [23].
Because judgment is often impaired early, usually resulting in poor job performance and impacting family finances, involvement of social work at the outset can help guide patients and caregivers though discussions of power of attorney. Additionally, patients with FTD and PPA may eligible for “compassionate allowance” from the Social Security Administration and be fast-tracked for access to Social Security disability benefits (http://www.alz.org/living_with_alzheimers_social_security_disability.asp#compassionate).
Driving and gun safety should always be addressed as early as possible. Occupational therapists and state Division of Motor Vehicles may be used for more formal assessments of driving capacity.
Non-pharmacological management of behavioral and psychological symptoms in dementia (BPSD) should be part of a patient-centered, systematic, and evidence-based approach [24, 25]. An “ABC” (antecedent—behavior—consequence) approach [26] to understanding problem behaviors and adopting preemptive plans should be encouraged. The AFTD offers concrete examples of most problematic behaviors and specific interventions that have been helpful in preventing or mitigating their impact (https://www.theaftd.org/wp-content/uploads/2011/09/Packet-Changes-in-behavior-chart.pdf).
All current symptomatic pharmacologic treatments remain off-label. Serotonergic agents such as trazodone, sertraline, or escitalopram can be helpful in controlling disinhibition, agitation, irritability, and obsessive/compulsive behavioral changes. Serotonergic agents are particularly helpful in PPA, especially when there is preserved deficit awareness that can lead to anxiety and depression.
Antipsychotics may be helpful if there is aggression or frank psychosis but have limited usefulness otherwise. Because of the higher risk of parkinsonism, atypical neuroleptics such as quetiapine, risperidone, olanzapine, aripiprazole, and possibly pimavanserin (recently approved for the treatment of psychosis in Parkinson’s disease) are preferred.
Agents approved for the treatment of Alzheimer’s disease have been de facto adopted in treating FTD [27], but data supporting such usage is lacking. In fact, cholinesterase inhibitors have been associated with increased agitation in bvFTD [28]. A possible role remains in the treatment of PPA, particularly for lvPPA or if Alzheimer’s disease remains in the differential. Treatment with memantine has been found to be of no benefit to patients with FTD [29].
There may be a role for dextromethorphan/quinidine in the treatment of agitation. It is approved for the treatment of pseudobulbar affect and has recently been demonstrated to be helpful in the control of agitation in Alzheimer’s disease [30].
ICD-10 Codes
-
G30 Alzheimer disease
-
G30.0 Alzheimer disease with early onset
-
G30.1 Alzheimer disease with late onset
-
G30.8 Other Alzheimer disease
-
G30.9 Alzheimer disease, unspecified
-
-
G31 Other degenerative disease of nervous system, not elsewhere classified
-
G31.0 Frontotemporal dementia
-
G31.01 Pick disease
-
G31.09 Other frontotemporal dementia
-
-
There are no specific billable codes for PPA. All three variants can be coded under G31.09, although lvPPA might better be coded under G30.0 or G30.1.
References
Neary D, Snowden J, Gustafson L, Passant U, Stuss D, Black S, et al. Frontotemporal lobar degeneration: a consensus on clinical diagnostic criteria. Neurology. 1998;51:1546–54.
Johnson JK, Diehl J, Mendez MF, Neuhaus J, Shapira JS, Forman M, et al. Frontotemporal lobar degeneration: demographic characteristics of 353 patients. Arch Neurol. 2005;62:925–30.
Kertesz A, Blair M, McMonagle P, Munoz DG. The diagnosis and course of frontotemporal dementia. Alzheimer Dis Assoc Disord. 2007;21:155–63.
Devenney E, Vucic S, Hodges JR, Kiernan MC. Motor neuron disease-frontotemporal dementia: a clinical continuum. Expert Rev Neurother. 2015;15:509–22.
Woollacott IO, Rohrer JD. The clinical spectrum of sporadic and familial forms of frontotemporal dementia. J Neurochem. 2016;138(S1):6–31.
Ratnavalli E, Brayne C, Dawson K, Hodges J. The prevalence of frontotemporal dementia. Neurology. 2002;58:1615–21.
Onyike CU, Diehl-Schmid J. The epidemiology of frontotemporal dementia. Int Rev Psychiatry. 2013;25:130–7.
Lanata SC, Miller BL. The behavioural variant frontotemporal dementia (bvFTD) syndrome in psychiatry. J Neurol Neurosurg Psychiatry. 2016;87:501–11.
Rohrer J, Guerreiro R, Vandrovcova J, Uphill J, Reiman D, Beck J, et al. The heritability and genetics of frontotemporal lobar degeneration. Neurology. 2009;73:1451–6.
Rascovsky K, Hodges JR, Knopman D, Mendez MF, Kramer JH, Neuhaus J, et al. Sensitivity of revised diagnostic criteria for the behavioural variant of frontotemporal dementia. Brain. 2011;134:2456–77.
Gorno-Tempini ML, Hillis AE, Weintraub S, Kertesz A, Mendez M, Cappa SF, et al. Classification of primary progressive aphasia and its variants. Neurology. 2011;76:1006–14.
Woolley JD, Khan BK, Murthy NK, Miller BL, Rankin KP. The diagnostic challenge of psychiatric symptoms in neurodegenerative disease: rates of and risk factors for prior psychiatric diagnosis in patients with early neurodegenerative disease. J Clin Psychiatry. 2011;72:126–33.
Harris JM, Gall C, Thompson JC, Richardson AMT, Neary D, Plessis Du D, et al. Sensitivity and specificity of FTDC criteria for behavioral variant frontotemporal dementia. Neurology. 2013;80:1881–7.
Lamarre AK, Rascovsky K, Bostrom A, Toofanian P, Wilkins S, Sha SJ, et al. Interrater reliability of the new criteria for behavioral variant frontotemporal dementia. Neurology. 2013;80:1973–7.
Gorno-Tempini M, Dronkers N, Rankin K, Ogar J, Phengrasamy L, Rosen H, et al. Cognition and anatomy in three variants of primary progressive aphasia. Ann Neurol. 2004;55:335–46.
Mesulam M, Wieneke C, Rogalski E, Cobia D, Thompson C, Weintraub S. Quantitative template for subtyping primary progressive aphasia. Arch Neurol. 2009;66:1545–51.
Josephs KA, Duffy JR, Strand EA, Machulda MM, Senjem ML, Master AV, et al. Characterizing a neurodegenerative syndrome: primary progressive apraxia of speech. Brain. 2012;135:1522–36.
Mesulam M. Primary progressive aphasia. Ann Neurol. 2001;49:425–32.
Mesulam M. Primary progressive aphasia—a language-based dementia. N Engl J Med. 2003;349:1535–42.
Chan D, Anderson V, Pijnenburg Y, Whitwell J, Barnes J, Scahill R, et al. The clinical profile of right temporal lobe atrophy. Brain. 2009;132:1287–98.
Josephs KA, Whitwell JL, Knopman DS, Boeve BF, Vemuri P, Senjem ML, et al. Two distinct subtypes of right temporal variant frontotemporal dementia. Neurology. 2009;73:1443–50.
Gorno-Tempini M, Brambati S, Ginex V, Ogar J, Dronkers N, Marcone A, et al. The logopenic/phonological variant of primary progressive aphasia. Neurology. 2008;71:1227–34.
Morhardt D. Accessing community-based and long-term care services: challenges facing persons with frontotemporal dementia and their families. J Mol Neurosci. 2011;45:737–41.
O’Neil ME, Freeman M, Christensen V, Telerant R, Addleman A, Kansagara D. A systematic evidence review of non-pharmacological interventions for behavioral symptoms of dementia. Washington, DC: Department of Veterans Affairs; 2011. https://www.ncbi.nlm.nih.gov/books/NBK54971/
Gitlin LN, Kales HC, Lyketsos CG. Nonpharmacologic management of behavioral symptoms in dementia. JAMA. 2012;308:2020.
Merrilees J. A Model for management of behavioral symptoms in frontotemporal lobar degeneration. Alzheimer Dis Assoc Disord. 2007;21:S64–9. http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation&list_uids=18090427
Kerchner GA, Tartaglia MC, Boxer A. Abhorring the vacuum: use of Alzheimer’s disease medications in frontotemporal dementia. Expert Rev Neurother. 2011;11:709–17.
Mendez M, Shapira J, McMurtray A, Licht E. Preliminary findings: behavioral worsening on donepezil in patients with frontotemporal dementia. Am J Geriatr Psychiatry. 2007;15:84–7.
Boxer AL, Knopman DS, Kaufer DI, Grossman M, Onyike C, Graf-Radford N, et al. Memantine in patients with frontotemporal lobar degeneration: a multicentre, randomised, double-blind, placebo-controlled trial. Lancet Neurol. 2013;12:149–56.
Cummings JL, Lyketsos CG, Peskind ER, Porsteinsson AP, Mintzer JE, Scharre DW, et al. Effect of dextromethorphan-quinidine on agitation in patients with Alzheimer disease dementia: a randomized clinical trial. JAMA. 2015;314:1242–54.
Disclosures
Dr. Léger reports no disclosures.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2017 Springer International Publishing AG
About this chapter
Cite this chapter
Léger, G.C. (2017). Frontotemporal Dementia. In: Tousi, B., Cummings, J. (eds) Neuro-Geriatrics. Springer, Cham. https://doi.org/10.1007/978-3-319-56484-5_9
Download citation
DOI: https://doi.org/10.1007/978-3-319-56484-5_9
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-56483-8
Online ISBN: 978-3-319-56484-5
eBook Packages: MedicineMedicine (R0)