
Abstract
The Frank-Starling mechanism describes a relationship where increasing ventricular filling increases cardiac output. Increased preload increases sarcomere stretch inside cardiac myocytes which generate more force during contraction and thereby allows the heart to eject more blood. However, there is a limit to which this relationship can be maintained. In failing ventricles, overstretch can limit or decrease cardiac output. In these cases, reducing myocyte stretch to a more optimal length can improve overall cardiac function.
Graphically, the Frank-Starling mechanism can be illustrated by cardiac function curves. Cardiac output can change by moving between different points on a single curve or changing to different curves. Physiologic changes altering preload can cause movement along the same cardiac curve, while changes in inotropy can cause shifts to different curves. On the steep, positively sloped portion of a cardiac function curve (sometimes called the preload dependent segment), cardiac output increases as ventricular stretch increases. If preload continues to increase, the point of overstretch is reached and eventually passed. Cardiac output plateaus and then begins to fall. The plateaued segment is sometimes called the preload independent portion.
Access provided by CONRICYT-eBooks. Download chapter PDF
Similar content being viewed by others


Keywords

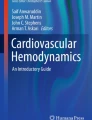
75.1
Depicted above is a family of cardiac function curves representing a ventricle under various conditions. Point A represents baseline cardiac function with normal preload; points A1 and A2 show states of decreased and increase preload, respectively. After reviewing this figure, please answer the following questions.
Questions
-
1.
What is Frank-Starling mechanism? Intracellularly, how can it cause a more forceful contraction?
-
2.
For the Frank-Starling curves depicted in Fig. 75.1, what are other parameters that can be substituted for the cardiac output label on the y-axis?
-
3.
What parameters can replace preload on the x-axis?
-
4.
What physiological changes might cause the system to move from:
-
(a)
Point A to A2
-
(b)
Point A to A1
-
(c)
Point A to B
-
(d)
Point A to D
-
(a)
-
5.
Graphically, which direction(s) will adding a beta-blocker shift a ventricle on Fig. 75.1?
-
6.
Following a premature ventricular contraction in a normal ventricle, how will the force generated by the next contraction change?
-
7.
After a single bolus dose of phenylephrine, what effect can be expected on cardiac output?
-
8.
If starting at point D2 on Fig. 75.1, would a fluid bolus be expected to increase cardiac output? If not, what interventions could increase output?
Answers
-
1.
The Frank-Starling mechanism describes a relationship where increasing ventricular filling increases cardiac output. Increased preload increases sarcomere stretch inside cardiac myocytes which generate more force during contraction and thereby allows the heart to eject more blood. However, there is a limit to which this relationship can be maintained. In failing ventricles, overstretch can limit or decrease cardiac output. In these cases, reducing myocyte stretch to a more optimal length can improve overall cardiac function. Although the cellular basis has not been definitively determined, the most widely accepted mechanism is that as sarcomeres are stretched, there is a length-dependent reduction in the spacing between thick and thin filaments. As the filaments are stretched and get closer together, tropomyosin on the thin filament becomes more sensitive to calcium. When contraction occurs, the sarcoplasmic reticulum releases calcium. The more sensitive tropomyosin now allows more actin-myosin cross-bridges to form yielding greater force generation [1–3].
-
2.
Multiple measurements have been developed to describe how well or efficiently a cardiac ventricle can pump. Essentially any measure that varies directly to cardiac output can be substituted on the y-axis. Some of the more popular metrics include venous return, stroke volume, cardiac index, and stroke work.
-
3.
Measurements that are essentially synonyms for preload on a cardiac function curve include end-diastolic volume, end-diastolic pressure, right atrial pressure, and pulmonary capillary wedge pressure.
-
4.
Cardiac output can change by moving between different points on a single curve or changing to different curves. Physiologic changes altering preload can cause movement along the same cardiac curve, while changes in inotropy can cause shifts to different curves. On the steep, positively sloped portion of a cardiac function curve (sometimes called the preload dependent segment), cardiac output increases as ventricular stretch increases. If preload continues to increase, the point of overstretch is reached and eventually passed. Cardiac output plateaus and then begins to fall. The plateaued segment is sometimes called the preload independent portion.
-
(a)
Moving from A to A2 shows an increase in cardiac output that is the result of increasing preload. Fluid resuscitation, passive leg raise, and decreasing PEEP are examples of interventions that can cause such a change.
Point A2 also represents the end of the preload-dependent and the start of the preload-independent portion of the cardiac function curve. Cardiac output levels off beyond A2 and eventually drops as overdistension is reached.
-
(b)
Decreasing preload shifts the systems leftward. As ventricular filling approaches 0, so does the cardiac output. Physiologically, anything that decreases venous return will cause a move from A to A1. Examples include hemorrhage, dehydration, obstructive shock, and high levels of PEEP.
-
(c)
With preload being constant, moving from point A to B requires either an increase in cardiac inotropy or a decrease in afterload. Catecholamines (such as epinephrine or dobutamine) that stimulate beta-1 adrenergic receptors in the heart can cause a more forceful contraction by a stretch-independent mechanism. Increasing intracellular calcium levels can also increase inotropy independent of preload. Administering calcium or a phosphodiesterase-3 inhibitor (PDE3), like milrinone, is a clinical way of achieving this.
Afterload is the pressure the ventricle must overcome in order to eject blood. Therefore, reducing afterload will also increase cardiac output independent of myocyte stretch. Clinically there are many pharmacologic agents that decrease afterload. Example drug classes include the following: nitric oxide inducers (such as nitroglycerin, nitroprusside, and isosorbide), alpha-1 adrenergic antagonists (such as prazosin), beta-2 adrenergic agonists, and PDE3 inhibitors.
Exercise, through multiple mechanisms including beta-1 and beta-2 receptor agonism, increases preload and decreases afterload simultaneously.
-
(d)
Shifting to a lower cardiac function curve, such as from A to D, indicates that inotropy has dropped significantly independent of stretch. A clinical example of this is myocardial infarction causing myocyte damage or death. Fewer sarcomeres will be present, so less force will be generated. The result is a downward shift in the cardiac function curve as well as a decreased slope in the preload dependent portion.
-
(a)
-
5.
Beta-1 adrenergic antagonists decrease cardiac chronotropy and inotropy. The overall effect will be a shift toward the right and toward a lower curve. Depending on the starting point, this can result in an increase or decrease in cardiac output:
-
(a)
Pure inotropy reduction will lead to less cardiac output at any fixed preload. Graphically, this will be a shift to a lower curve (such as from A to C).
-
(b)
However, there are situations when beta-1 antagonism can yield a net increase in cardiac output. If the ventricle is still in the preload-dependent segment of a given curve, a lower heart rate can allow for more time in diastole and therefore more filling. Also, beta-blockers can calm some cardiac arrhythmias. Better atrial-ventricular coordination preserves the function of atrial kick, which increases ventricular filling.
-
(c)
If starting at point A1, more preload will shift the ventricle toward point A. Inotropy reduction will drop the ventricle to a lower curve. Will it be as low as point C (or lower)? It depends on how sensitive the myocytes are and how much they are relying on beta stimulation in their current state. The final position will be lower than point A, but the net result could be a higher cardiac output than the original A1 starting point.
-
(a)
-
6.
Following a PVC, there is a longer than usual time for diastole, more ventricular filling and myocyte stretch. More force will be generated during the next contraction, and the extra blood that entered the ventricle will be ejected.
-
7.
Phenylephrine causes vasoconstriction via alpha-1 adrenergic agonism. This can cause an increase in afterload, which can decrease cardiac output. However, vasoconstriction can also shift pooled blood from peripheral and splanchnic venous beds into central circulation; this can increase preload. The resulting net effect is controversial and may depend on the starting point on the cardiac function curve. Porcine models suggest that starting on the steep (preload dependent) part of a cardiac function curve causes a net increase in cardiac output [4]. While giving phenylephrine on the flatter (preload independent) part of the cardiac function curve causes a net decrease in cardiac output.
-
8.
At point D2, the ventricle is overdistended and in failure. Additional fluid will not improve stroke volume. Decreasing myocyte stretch so that sarcomeres can get closer to their optimal length would be more helpful. Diuretics or hemoconcentration is more appropriate; the result will be moving from point D2 toward D. Adding inotropic support or significantly decreasing afterload with vasodilators can also improve cardiac output. These changes can shift the entire curve closer to curve C.
References
Hall J. Cardiac muscle: the heart as a pump and function of the valves. In: Hall J, editor. Guyton and Hall textbook of medical physiology. 13th ed. Philadelphia: Elsevier; 2016. p. 245–258
Noble MI. The Frank—Starling Curve. Clinical Science. 1978 Jan 1;54(1):1–7.
Kobirumaki-Shimozawa F, Inoue T, Shintani SA, et al. Cardiac thin filament regulation and the Frank–Starling mechanism. J Physiol Sci. 2014;64:221.
Maxime C, Zhongping J, et al. Effects of phenylephrine on cardiac output and venous return depend on the position of the heart on the Frank-Starling relationship. J Appl Physiol. 2012;113(2):281–9.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2017 Springer International Publishing AG
About this chapter
Cite this chapter
Mann, D. (2017). Frank-Starling Curve. In: Raj, T. (eds) Data Interpretation in Anesthesia. Springer, Cham. https://doi.org/10.1007/978-3-319-55862-2_75
Download citation
DOI: https://doi.org/10.1007/978-3-319-55862-2_75
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-55861-5
Online ISBN: 978-3-319-55862-2
eBook Packages: MedicineMedicine (R0)