
Abstract
Medicine including surgical techniques has been flourishing since ancient societies. All efforts have aimed to increase patient’s survival in addition to quality of life. Lately, along with the increased popularity of laparoscopic surgery, minimally invasive surgical techniques have taken its place in surgical practice for various type of procedures, owing to several advantages such as rapid recovery, less pain as well as improved cosmetic outcomes [1]. However, for treatment of malignant diseases, safety and feasibility of minimally invasive surgery (MIS) has remained under debate for years until recently. With the increasing amount of evidence and surgical experience, MIS is now commonly favored practice for oncological surgery that made of more sophisticated processes compared to those of surgery for benign diseases [2]. Whereas MIS represents a developing trend, some limitations faced by surgeon during conventional laparoscopy led surgeons for innovative solutions and robotic technology has been introduced with many advantages including articulated instruments, three-dimensional images, and tremor filtering. Although several robotic systems have been developed, its popularity has increased just after the approval of Da Vinci robotic system (Intuitive Surgical, California, USA), many robotic systems have been started being used worldwide [3].
Access provided by CONRICYT-eBooks. Download chapter PDF
Similar content being viewed by others


Keywords
Medicine including surgical techniques has been flourishing since ancient societies. All efforts have aimed to increase patient’s survival in addition to quality of life. Lately, along with the increased popularity of laparoscopic surgery, minimally invasive surgical techniques have taken its place in surgical practice for various type of procedures, owing to several advantages such as rapid recovery, less pain as well as improved cosmetic outcomes [1]. However, for treatment of malignant diseases, safety and feasibility of minimally invasive surgery (MIS) has remained under debate for years until recently. With the increasing amount of evidence and surgical experience, MIS is now commonly favored practice for oncological surgery that made of more sophisticated processes compared to those of surgery for benign diseases [2]. Whereas MIS represents a developing trend, some limitations faced by surgeon during conventional laparoscopy led surgeons for innovative solutions and robotic technology has been introduced with many advantages including articulated instruments, three-dimensional images, and tremor filtering. Although several robotic systems have been developed, its popularity has increased just after the approval of Da Vinci robotic system (Intuitive Surgical, California, USA), many robotic systems have been started being used worldwide [3].
Despite the decreasing trend for overall incidence, gastric cancer is still one of the most common cancer type and one of the most common cause of cancer-related mortality worldwide. Radical gastrectomy with en-bloc lymphadenectomy is fundamental cornerstone for curative treatment in resectable gastric cancer patients. With the mass-screening programs and advances in diagnostic tools, the incidence of early gastric cancer (EGC) has increased particularly in eastern countries. Subsequent studies using conventional open surgery reported over 90% survival rate for EGC and surgeons’ interest have increased for function preservation and quality of life in addition to the oncological curability for patients with gastric cancer particularly for EGC [4].
Laparoscopic surgery for gastric cancer have been used for limited resections in the early 1990s. Laparoscopic intragastric mucosal resections and laparoscopic wedge resection were two methods that historically used for lesions without the risk of lymph node metastasis. However, with the advance of endoscopic resection techniques such as mucosal resection and submucosal dissection, their usage has declined recently. Currently, only laparoscopic wedge resection is being investigated within sentinel lymph node mapping concept. Following the Kitano’s report presenting first laparoscopic-assisted gastrectomy for gastric cancer in 1994, laparoscopic gastrectomy (LG) has been introduced as an alternative to conventional open surgery [5]. LG that is initially used for EGC located in distal stomach has been started being used for tumors located in proximal stomach and for advanced gastric cancers (AGC) including extended lymphadenectomy. Number of cases that LG was used has increased tenfold between 1991 and 2009 in Japan mainly for Stage I disease, and from 6.6 to 25.8% between 2004 and 2009 in South Korea, even for the Western countries but with slower trend [6]. During this development period, improvements in robotic surgery has also followed the those of LG, and robotic gastrectomy (RG) for gastric cancer now became a frequently performed procedure especially in Korea, Japan and Italy.
1 Indications for Minimally Invasive Gastrectomy
Although endoscopic treatment modalities are the ideal approaches to preserve patient’s functions and quality of life, these techniques can be used only for a limited number of patient that meet rigorous criteria. Regarding LG, while previous Japanese Gastric Cancer Treatment guideline recommends LG as an investigational treatment, in the fourth edition that was published in 2016, laparoscopic surgery is recognized as an option in general clinical practice for clinical Stage I gastric cancer that is indicated only for distal gastrectomy but patients require total gastrectomy [7]. Correspondingly, in South Korea, patients that does not required extended lymphadenectomy such as cN-, patients that does not required total gastrectomy and tumors that limited to the submucosa can be considered as initial indication for laparoscopic surgery with the exception of the patients that are suitable for endoscopic treatment.
In experienced centers from East Asia, the current indication for LG has been extended beyond EGC to AGC irrespective of perigastric node involvement. However, outcomes of ongoing studies are needed to utilize LG with extended indications. The indications for RG does not differ from those of LG.
2 Operative Strategy
Terminology: Gastrectomy procedures have various definitions based on the extent of resection such as distal, total, proximal or pylorus-preserving. Besides, when MIS techniques are used, it can be defined as laparoscopic assisted or totally laparoscopic. For cases which anastomosis are made extracorporeally, it is defined as laparoscopic assisted and when intracorporeal anastomosis is used, as totally laparoscopic. Despite the variations in the literature, usual definitions include laparoscopic assisted distal gastrectomy (LADG), laparoscopic assisted total gastrectomy (LATG), totally laparoscopic distal gastrectomy (TLDG), totally laparoscopic total gastrectomy (TLTG). When robotic systems are used, they can be called as robotic-assisted distal gastrectomy (RADG or RDG) or robotic-assisted total gastrectomy (RATG or RTG). In addition to LADG and LATG, proximal gastrectomy and pylorus preserving distal gastrectomy are the other procedures can be performed by either laparoscopic and robotic.
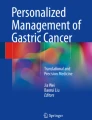
Port placement. While some surgeons prefer using six port including one for liver retraction, most surgeons prefer a total of five ports (Fig. 16.1a, b) [8]. For LG, the first 10-mm camera port is placed using open method at the infra-umbilical area, and pneumoperitoneum is achieved at 12 mmHg. Four other trocars are inserted, one in the right upper quadrant, one in the upper left quadrant, one in the right lateral side, and one to the left lateral side of the abdomen. The surgeon and scope operator are located on the right side of the patient and an assistant is on patient’s left side. The RG procedure follows the identical steps as those of LG with some modifications in port placements (Fig. 16.1c). A 12-mm camera port placed below the umbilicus, and four other trocars including three 8-mm port for the robotic arms and one 12-mm assistant’s port are placed. Assistant port is usually placed between the camera port and first arm that placed patient’s left side below the costal margin. Then, robotic arms are docked to initiate the procedure.

Port placement for minimally invasive gastrectomy. 6-port (a) or 5-port (b) surgery can be used for laparoscopic gastrectomy. (c) Shows the place for ports in robotic gastrectomy (C camera, S surgeon, A assistant, R retractor)
Liver retraction. Various techniques have been defined thus far to retract the liver and to have clear visualization for hepatogastric/hepatoduodenal ligaments. Although using liver retractor requires one extra port, using suture-gauze technique maintains ideal liver retraction and allows surgeon to use one less port [9].
Intraoperative tumor localization. Particularly for EGC, it is challenging to locate tumor by using laparoscopic or robotic instruments, therefore surgeon needs to use some techniques to determine safe surgical margin. Various methods such as intraoperative ultrasound, intraoperative endoscopy, and abdominal plain radiograph following preoperative endoscopic clipping have been defined for this key step [10].
Extent of omentectomy. Although total omentectomy is recommended for T3–T4 tumors, partial omentectomy which removes the 3 cm away from gastroepiploic vessels can be used for T1 and T2 tumors.
Extent of lymphadenectomy. Clinical stage of the tumor and type of gastrectomy are the markers to decide the extent of lymphadenectomy. For distal gastrectomy, D1+ lymphadenectomy includes the lymph nodes numbered as #1, #3, #4sb, #4d, #5, #6, #7, #8a and #9. D2 lymphadenectomy includes #11p and #12a in addition to D1+ lymphadenectomy. For total gastrectomy, D1+ lymphadenectomy includes #1–7, #8a, #9, #11p and D2 lymphadenectomy includes #10, #11d, #12a in addition to D1+ lymphadenectomy. D1+ lymphadenectomy for proximal gastrectomy requires the dissection of #1, #2, #3a, #4sa, #4sb, #7, #8a, #9, #11p.
Left side dissection. Despite minor differences among surgeons, each individual surgeon uses standardized steps for minimally invasive gastrectomy. It is usually preferred to start from the left side. Following the division of gastrocolic ligament, the left gastroepiploic vessels are divided at their root on the left side, #4sb and #4d are removed for distal gastrectomy and then greater curvature is cleared for transection and anastomosis (Fig. 16.2a). If total gastrectomy is intended, short gastric vessels are divided up to left diaphragmatic crus and #2 and #4a are removed. To maintain D2 dissection when necessary, #10 and #11d should be removed with or without splenectomy.

Steps for lymphadenectomy during minimally invasive gastrectomy. (a): left side dissection for #4sb around LGEV. (b): right side dissection for #6 lymph nodes above the pancreas. (c): for #5 and #8a, RGA is exposed and soft tissues around the CHA are dissected. (d): soft tissues medial to the PV and PHA are dissected for proper #12a dissection in D2 lymphadenectomy. (e): LGA is exposed above the celiac trunk. (f): for #11p dissection, SV and SA are exposed and all soft tissues are cleaned along these vessels. (g): lesser curvature is cleaned to remove #1 lymph nodes. (h): final view of lymph node dissection. (LGEV left gastroepiploic vessels, ASPDV anterior superior pancreaticoduodenal vein, RCV right colic vein, MCV middle colic vein, MCA middle colic artery, RGA right gastric artery, PHA proper hepatic artery, CHA common hepatic artery, PV portal vein, LGA left gastric artery, LGV left gastric vein, SV splenic vein, SA splenic artery, LC lesser curvature, AHA accessory hepatic artery arising from LGA)
Right side dissection and duodenal division. After completion of left side, procedure move to right side and tissues around the gastrocolic trunk are cleared (Fig. 16.2b). right gastroepiploic vein is divided and the soft tissues above the pancreas are retrieved (#6). Right gastroepiploic artery is divided and dissection continues up to the root of gastroduodenal artery to mobilize the duodenum from the pancreas. In supraduodenal area, minor periduodenal vessels are divided and duodenum is transected by using linear endoscopic stapler.
Suprapancreatic dissection. Right gastric vessels are divided and soft tissues around the common hepatic artery are dissected (#5–8a) (Fig. 16.2c). For D2 dissection, soft tissues medial to the portal vein and proper hepatic artery are included in the specimen (#12a) (Fig. 16.2d). After left gastric vein division, soft tissues around left gastric artery are dissected on the right side (#7, #9), and splenic artery on the left side (#11p) (Fig. 16.2e, f). Retroperitoneal attachments of stomach including posterior gastric vessels if present are detached. Right diaphragmatic crus is reached and lesser curvature of the stomach is cleaned to remove #1 and some parts of #3 for distal gastrectomy (Fig. 16.2g, h).
Reconstruction. It is possible to perform anastomosis by either intra- or extracorporeally after gastrectomy. After distal gastrectomy, Billroth-I gastroduodenostomy, Billroth-II gastrojejunostomy, or Roux-en-Y gastrojejunostomy are the options to maintain intestinal continuity. For Billroth-I gastroduodenostomy, small full-layer incisions are created on the edge of greater curvature side of the stomach and on the edge of the posterior side of the duodenum. The 45-mm endoscopic linear stapler is inserted towards both intestinal lumens and the posterior walls of the stomach and duodenum are anastomosed (Fig. 16.3a). The entry hole is closed with another endoscopic linear stapler and Delta-Shaped Anastomosis is achieved (Fig. 16.3b) [11]. For Billroth-II gastrojejunostomy roughly 20 cm distal to the treitz ligament is brought up and anastomosis is performed by using two linear staplers (Fig. 16.3c, d). When jejenum is divided from same distance, it is possible to perform roux-en-Y gastrojejunostomy by using linear staplers and then jejunojejunostomy is added 25–30 cm distal to the gastrojejunostomy with similar stapling technique. After total gastrectomy, most common anastomosis type is Roux-en-Y esophagojejunostomy. For years, it has been performed by circular stapling technique which require mini-laparotomy, however, it is now possible to perform safely with side-to-side linear stapling technique (Fig. 16.3e, f). Linear staplers can also be used for esophagogastrostomy after proximal gastrectomy and for gastro-gastrostomy after pylorus-preserving gastrectomy to achieve all reconstructive process intracorporeally. For reconstruction, in addition to the techniques mentioned above, jejunal interposition and double-tract method are alternative options.

Intracorporeal anastomosis for Billroth-I gastroduodenostomy (a, b), Billroth-II gastrojejunostomy (c, d) after distal gastrectomy, and intracorporeal Roux-en-Y esophagojejunostomy (e, f) after total gastrectomy
3 Current Evidences for Minimally Invasive Gastrectomy
After first report of LG, many studies including randomized controlled trials (RCT) are conducted in various centers. However, because the stage of tumor (EGC vs. AGC) and type of gastrectomy (distal vs. total) determine the extent and invasiveness of surgery, it is not possible to gather all studies in one pool, and short-term and long-term outcomes should be evaluated with distinct subgroups.
3.1 Laparoscopic Gastrectomy Versus Open Gastrectomy
Up to now, there are several published retrospective series, RCTs and meta-analysis comparing LADG vs. open distal gastrectomy (ODG) for EGC located in the mid-to-lower part of the stomach. The most recent meta-analysis including seven RCTs (five from Japan and two from South Korea) published in 2015 demonstrated that LADG provides less blood loss (WMD: −108.11; 95% CI: −145.97 to −70.26), less analgesic requirement (WMD: −1.70; 95% CI: −2.19 to −1.22), lower incidence of complications (OR: 0.26; 95% CI: 0.13–0.54), shorter hospital stay (WMD: −1.0; 95% CI: −1.83 to −0.16), and earlier passage of flatus (WMD: −0.62; 95% CI: −0.96 to −0.27), though at the price of longer operative times (WMD: 79.60; 95% CI: 59.86–99.35) and the number of harvested lymph nodes (WMD: −2.77; 95% CI: −4.38 to −1.16) lesser as compared to ODG [12]. Despite the combination of several RCTs, total number of patients was 390 (195 LADG and 195 ODG) in this meta-analysis and might be considered as a limitation for proper conclusion. To overcome this limitation, we need to look into the outcomes of phase III studies. Multi-institutional randomized KLASS-01 study conducted by the Korea Laparoscopic Gastrointestinal Surgery Study Group (KLASS), that started in 2006, is a study that compares LDG and ODG and short-term outcomes were published recently [13]. While the major intraabdominal complication (LADG vs. ODG; 7.6% vs. 10.3%) and mortality rates (0.6% vs. 0.3%) were comparable between two groups, overall complication rate (13.0% vs. 19.9%) including wound complication rate (3.1% vs. 7.7%) were lower in LADG group. In addition to these findings, LADG was associated with significantly longer operation time (184.1 ± 53.3 vs. 139.4 ± 42.7), less blood loss (110.8 ± 135.7 vs. 190.6 ± 156.3), shorter hospital stay (7.1 ± 3.1 vs. 7.9 ± 4.1), and less number of harvested lymph nodes (40.5 ± 15.3 vs. 43.7 ± 15.7). The other randomized study JCOG0912, which was carried out by the Japan Clinical Oncology Group (JCOG), demonstrated similar outcomes and concluded that LADG can be considered as a safe alternative to open surgery in terms of adverse events and short-term outcomes [14]. The study showed longer operation time (LADG vs. ODG, median 278 min vs. 194 min) with less blood loss (median 38 mL vs. 115 mL) in LADG group, and no difference was found in terms of major complications (3.3% vs. 3.7%), only liver enzymes elevation was observed more (16.4% vs. 5.3%) in LADG group possibly due to long duration of liver retraction. As for oncologic safety of LADG for EGC, while a recent meta-analysis demonstrated comparable oncological outcomes in terms of long-term mortality and relapse rate, we need to wait little bit more to obtain the long-term outcomes of large-scale RCTs.
Apart from the increasing number of evidence on LADG for EGC, high-level evidences neither for LATG and nor for advanced stage disease are available, because of the technical difficulties and the technical heterogeneity among the surgeons during LATG or lymphadenectomy for AGC. Because AGC requires extensive lymphadenectomy for patients with gastric cancer, it is difficult to standardize the surgery and to have high-quality evidence. Recently published Chinese study includes total 1056 patients (The Chinese Laparoscopic Gastrointestinal Surgery Study, CLASS-01) showed no difference in terms of morbidity and mortality in patients with AGC require distal gastrectomy [15]. Postoperative morbidity was 15.2% for LDG and 12.9% in ODG group, while 0.4% mortality rate in LDG and no mortality was observed in ODG group. As for oncological safety, the only RCT showing long-term outcomes demonstrated 67.1 and 53.8% survival rates respectively for LG and open gastrectomy with no statistical difference. There are two ongoing large-scale study in South Korea and Japan, KLASS-02 and JLSSG0901 (Japanese Laparoscopic Surgery Study Group). The oncological outcomes of these two as well as the CLASS-01 study will answer the questions on the safety and efficacy of LG for AGC [3].
Because the incidence of proximal gastric cancer is low in Asian countries, and owing to difficulties in the reconstruction phase after total gastrectomy, LTG could not have been generalized in surgical practice. Although recent meta-analysis that includes EGC or AGC regardless of stage and compare LTG vs. open total gastrectomy demonstrated the benefits of LTG in terms of blood loss, pain, hospital stay and morbidity with the comparable long-term outcomes, relatively small sample size of studies and the lack of RCTs are the obstacles to have exact conclusion. Although the outcomes of prospective phase-II KLASS-03 study aiming to evaluate the feasibility of LTG for patients with EGC will shed light on the future of LTG, randomized trials are still required [16].
3.2 Robotic Gastrectomy Versus Open Gastrectomy
Following the first report of large case series evaluating RG that was published in 2009, and that demonstrated RG as a safe and effective alternative, surgeons have conducted some comparative studies [17]. Meta-analysis of seven retrospective case-matched series argued that RG is safe and efficient method and may be a more practical and feasible alternative to open gastrectomy [18]. Similarly, recent RCT comparing RG with intra-corporeal robot-sewn anastomosis and open gastrectomy demonstrated that RG ensures less blood loss (94.2 ± 51.5 vs. 152.8 ± 76.9 mL), shorter hospital stay (5.6 ± 1.9 vs. 6.7 ± 1.9 days) and earlier restoration of bowel function (2.6 ± 1.1 vs. 3.1 ± 1.2 days), however surgical duration was longer (242.7 ± 43.8 vs. 192.4 ± 31.5 min) in RG group [19]. Neither complication rates (10.3 vs. 9.3%) nor number of harvested lymph node (30.9 ± 10.4 vs. 29.3 ± 9.7 days) were different. As was shown in this RCT and previous large series, besides the benefits of minimal invasiveness of RG compared to open surgery, some issues such as cost and surgical duration are the shortcomings to be solved in the future. For oncological safety, a matched-case control study showed comparable outcomes between RG and open gastrectomy, however, further studies are needed [20].
3.3 Robotic Gastrectomy Versus Laparoscopic Gastrectomy
Even though both are minimally invasive techniques, some studies try to find out whether there is a difference between RG and LG. Recent multicenter prospective study from South Korea, both groups showed comparable overall complication rates (robotic: 11.9% vs. laparoscopic: 10.3%) and major complication rates (robotic: 1.1% vs. laparoscopic: 1.1%) [21]. Owing to the higher cost of robotic surgery and longer operative time in RG group, any superiority of RG over LG could not have been demonstrated in this study. Furthermore, in subgroup analysis of that study showed that RG compared to LG is more beneficial in terms of blood loss for the patients underwent D2 lymph node dissection [22]. However, robotic assistance was not helpful to overcome the obstacles of LG for obese patients or for patients underwent total gastrectomy. Given that use of robot for gastrectomy has a short history, long-term oncologic outcomes of RG still remains controversial. Even so, retrospective series comparing survival between RG and LG revealed that survival was comparable between the two approaches [23].
3.4 Robotic Gastrectomy Versus Laparoscopic Gastrectomy Versus Open Gastrectomy
In a study comparing three approaches in terms of major early complications in a total of 5839 patients (4542 open gastrectomy, 861 LG and 436 RG), while no significant difference was found between the three groups, intestinal obstruction and intra-abdominal fluid collection was observed more after open gastrectomy and MIS led to more anastomotic leakage [24].
3.5 Overview to Evidences
Because gastric cancer treatment depends on various factors such as tumor location, tumor stage, and patient characteristics, it is not rational to place all gastric cancer patients in one pool to evaluate the efficacy of MIS. Indeed, MIS for gastric cancer does not have a long history, thus we have recently started having some evidence as regard to its safety and feasibility. The evidences we have had thus far may demonstrate that MIS is safe, technically feasible and oncological effective approach for early gastric cancer patients requiring distal gastrectomy. Although we have some evidence concerning the safety for advanced gastric cancer and for patients requiring total gastrectomy, we need to wait the outcomes of ongoing Korean and Japanese studies to have exact conclusion.
Less blood loss, improved recovery, and shorter hospital stay are the main advantages of the laparoscopic surgery as was observed in other gastrointestinal malignancies. Given that gastric cancer surgery including lymphadenectomy is a complex procedure, it is conceivable to suppose that robotic instruments will assist surgeons overcome the difficulties during laparoscopic gastrectomy. Surgical duration is one of the disadvantage of MIS, however, it should be kept in mind that learning curve effect is a key point for complex procedures. And, as recent studies revealed, with the increasing surgeon experience, time having spent in operation room is getting shorter not only for LG and also for RG. The cost is another obstacle for MIS and this should be investigated and solved in future studies.
In the lights of current evidences, although LG and RG are complex procedures for surgeon, can be performed safely with the expected advantages of minimally invasive surgery. Given the difficulties during laparoscopic surgery, robotic surgery may offer a promising alternative to traditional open or conventional laparoscopic gastrectomy.
References
Arezzo A. The past, the present, and the future of minimally invasive therapy in laparoscopic surgery: a review and speculative outlook. Minim Invasive Ther Allied Technol. 2014;23(5):253–60. doi:10.3109/13645706.2014.900084.
Son T, Hyung WJ. Laparoscopic gastric cancer surgery: current evidence and future perspectives. World J Gastroenterol. 2016;22(2):727–35. doi:10.3748/wjg.v22.i2.727.
Son T, Kwon IG, Hyung WJ. Minimally invasive surgery for gastric cancer treatment: current status and future perspectives. Gut Liver. 2014;8(3):229–36. doi:10.5009/gnl.2014.8.3.229.
Jeong O, Park YK. Clinicopathological features and surgical treatment of gastric cancer in South Korea: the results of 2009 nationwide survey on surgically treated gastric cancer patients. J Gastric Cancer. 2011;11(2):69–77. doi:10.5230/jgc.2011.11.2.69.
Kitano S, Iso Y, Moriyama M, Sugimachi K. Laparoscopy-assisted Billroth I gastrectomy. Surg Laparosc Endosc. 1994;4(2):146–8.
Antonakis PT, Ashrafian H, Isla AM. Laparoscopic gastric surgery for cancer: where do we stand? World J Gastroenterol. 2014;20(39):14280–91. doi:10.3748/wjg.v20.i39.14280.
Japanese Gastric Cancer Association. Japanese gastric cancer treatment guidelines 2014 (ver. 4). Gastric Cancer. 2016;20(1):1–19. doi:10.1007/s10120-016-0622-4.
Guner A, Hyung WJ. Minimally invasive surgery for gastric cancer. Ulus Cerrahi Derg. 2014;30(1):1–9. doi:10.5152/ucd.2014.2607.
Woo Y, Hyung WJ, Kim HI, Obama K, Son T, Noh SH. Minimizing hepatic trauma with a novel liver retraction method: a simple liver suspension using gauze suture. Surg Endosc. 2011;25(12):3939–45. doi:10.1007/s00464-011-1788-9.
Kim HI, Hyung WJ, Lee CR, Lim JS, An JY, Cheong JH, Choi SH, Noh SH. Intraoperative portable abdominal radiograph for tumor localization: a simple and accurate method for laparoscopic gastrectomy. Surg Endosc. 2011;25(3):958–63. doi:10.1007/s00464-010-1288-3.
Kanaya S, Kawamura Y, Kawada H, Iwasaki H, Gomi T, Satoh S, Uyama I. The delta-shaped anastomosis in laparoscopic distal gastrectomy: analysis of the initial 100 consecutive procedures of intracorporeal gastroduodenostomy. Gastric Cancer. 2011;14(4):365–71. doi:10.1007/s10120-011-0054-0.
Deng Y, Zhang Y, Guo TK. Laparoscopy-assisted versus open distal gastrectomy for early gastric cancer: a meta-analysis based on seven randomized controlled trials. Surg Oncol. 2015;24(2):71–7. doi:10.1016/j.suronc.2015.02.003.
Kim W, Kim HH, Han SU, Kim MC, Hyung WJ, Ryu SW, Cho GS, Kim CY, Yang HK, Park DJ, Song KY, Lee SI, Ryu SY, Lee JH, Lee HJ. Decreased morbidity of laparoscopic distal gastrectomy compared with open distal gastrectomy for stage I gastric cancer: short-term outcomes from a multicenter randomized controlled trial (KLASS-01). Ann Surg. 2016;263(1):28–35. doi:10.1097/sla.0000000000001346.
Katai H, Mizusawa J, Katayama H, Takagi M, Yoshikawa T, Fukagawa T, Terashima M, Misawa K, Teshima S, Koeda K, Nunobe S, Fukushima N, Yasuda T, Asao Y, Fujiwara Y, Sasako M. Short-term surgical outcomes from a phase III study of laparoscopy-assisted versus open distal gastrectomy with nodal dissection for clinical stage IA/IB gastric cancer: Japan Clinical Oncology Group Study JCOG0912. Gastric Cancer. 2016. [Epub ahead of print]. doi:10.1007/s10120-016-0646-9
Hu Y, Huang C, Sun Y, Su X, Cao H, Hu J, Xue Y, Suo J, Tao K, He X, Wei H, Ying M, Hu W, Du X, Chen P, Liu H, Zheng C, Liu F, Yu J, Li Z, Zhao G, Chen X, Wang K, Li P, Xing J, Li G. Morbidity and mortality of laparoscopic versus open D2 distal gastrectomy for advanced gastric cancer: a randomized controlled trial. J Clin Oncol. 2016;34(12):1350–7. doi:10.1200/jco.2015.63.7215.
Kim KH, Kim SH, Kim MC. How much progress has been made in minimally invasive surgery for gastric cancer in Korea?: a viewpoint from Korean prospective clinical trials. Medicine (Baltimore). 2014;93(28):e233. doi:10.1097/MD.0000000000000233.
Song J, Oh SJ, Kang WH, Hyung WJ, Choi SH, Noh SH. Robot-assisted gastrectomy with lymph node dissection for gastric cancer: lessons learned from an initial 100 consecutive procedures. Ann Surg. 2009;249(6):927–32. doi:10.1097/01.sla.0000351688.64999.73.
Yang Y, Wang G, He J, Wu F, Ren S. Robotic gastrectomy versus open gastrectomy in the treatment of gastric cancer. J Cancer Res Clin Oncol. 2016;143(1):105–14. doi:10.1007/s00432-016-2240-2.
Wang G, Jiang Z, Zhao J, Liu J, Zhang S, Zhao K, Feng X, Li J. Assessing the safety and efficacy of full robotic gastrectomy with intracorporeal robot-sewn anastomosis for gastric cancer: a randomized clinical trial. J Surg Oncol. 2016;113(4):397–404. doi:10.1002/jso.24146.
Caruso S, Patriti A, Marrelli D, Ceccarelli G, Ceribelli C, Roviello F, Casciola L. Open vs robot-assisted laparoscopic gastric resection with D2 lymph node dissection for adenocarcinoma: a case-control study. Int J Med Rob Comput Assisted Surg. 2011;7(4):452–8. doi:10.1002/rcs.416.
Kim HI, Han SU, Yang HK, Kim YW, Lee HJ, Ryu KW, Park JM, An JY, Kim MC, Park S, Song KY, Oh SJ, Kong SH, Suh BJ, Yang DH, Ha TK, Kim YN, Hyung WJ. Multicenter prospective comparative study of robotic versus laparoscopic gastrectomy for gastric adenocarcinoma. Ann Surg. 2016;263(1):103–9. doi:10.1097/SLA.0000000000001249.
Park JM, Kim HI, Han SU, Yang HK, Kim YW, Lee HJ, An JY, Kim MC, Park S, Song KY, Oh SJ, Kong SH, Suh BJ, Yang DH, Ha TK, Hyung WJ, Ryu KW. Who may benefit from robotic gastrectomy?: a subgroup analysis of multicenter prospective comparative study data on robotic versus laparoscopic gastrectomy. Eur J Surg Oncol. 2016;42(12):1944–9. doi:10.1016/j.ejso.2016.07.012.
Son T, Lee JH, Kim YM, Kim HI, Noh SH, Hyung WJ. Robotic spleen-preserving total gastrectomy for gastric cancer: comparison with conventional laparoscopic procedure. Surg Endosc. 2014;28(9):2606–15. doi:10.1007/s00464-014-3511-0.
Kim KM, An JY, Kim HI, Cheong JH, Hyung WJ, Noh SH. Major early complications following open, laparoscopic and robotic gastrectomy. Br J Surg. 2012;99(12):1681–7. doi:10.1002/bjs.8924.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2017 Springer International Publishing AG
About this chapter
Cite this chapter
Guner, A., Hyung, W.J. (2017). Minimally Invasive Surgery of Gastric Cancer. In: Cuesta, M. (eds) Minimally Invasive Surgery for Upper Abdominal Cancer. Springer, Cham. https://doi.org/10.1007/978-3-319-54301-7_16
Download citation
DOI: https://doi.org/10.1007/978-3-319-54301-7_16
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-54300-0
Online ISBN: 978-3-319-54301-7
eBook Packages: MedicineMedicine (R0)