
Abstract
Puberty is the developmental stage of physical and psychological maturation in which reproductive capacity is attained. The onset of puberty is driven by the activation of the hypothalamic–pituitary–gonadal axis after the break that restrains this axis during the majority of childhood is released. This review will cover the clinical assessment of puberty, variation in the timing of puberty, and the complex factors that regulate the onset and timing of puberty. In addition, the presentation, diagnosis, and differential diagnosis of male delayed puberty will be discussed. Male delayed puberty is common, affecting up to three percent of the population. The main differential diagnoses of delayed puberty in males include self-limited delayed puberty (DP), idiopathic hypogonadotropic hypogonadism (IHH), and hypergonadotropic hypogonadism. Treatment of isolated CDGP involves expectant observation or short courses of low-dose sex steroid supplementation. More complex and involved management is required in males with hypogonadism to achieve both the development of secondary sexual characteristics and to maximize the potential for fertility.
Access provided by CONRICYT-eBooks. Download chapter PDF
Similar content being viewed by others


Keywords
- Puberty
- Delayed puberty
- Self-Limited delayed puberty
- Constitutional delay of growth and puberty
- Hypogonadotropic hypogonadism
- Hypogonadism
- Testosterone
- Gnrh/HPG axis
- Testis
Normal Puberty
Physiology
Puberty is the maturational process of the reproductive endocrine system that results in final adult height and body proportion as well as the development of the genital organs and the capacity to reproduce. The onset of puberty is driven by an increase in the frequency and amplitude of pulsatile release of gonadotropin-releasing hormone (GnRH) from the hypothalamus. This activation results in increased luteinizing hormone (LH) and follicular-stimulating hormone (FSH) production by the anterior pituitary which acts on the gonads to stimulate their development, gametogenesis, and sex steroid secretion.
Clinical Markers of Puberty
In boys, the first physical marker of pubertal onset is an increase in testis volume above the prepubertal volume of 3 mL (Tanner stage G2) [1] (Fig. 4.1). There is a classic pattern of pubertal progression with the onset of testicular enlargement followed by pubic hair development and penile growth. The testes increase in size from a prepubertal volume of 1–2 to 4–8 mL even before pubic hair appears and reach 20–30 mL in adulthood [2]. Development of mature spermatogenesis is called spermarche, at which time mature spermatozoa are found in the urine. This hallmark of gonadal maturation occurs at a mean age of 13.5 years, when the mean testis volume reaches 11.5 mL [3]. The tempo and process of puberty are well conserved across ethnicities and populations (Table 4.1).

Tanner staging of puberty onset in boys from Palmer and Dunkel [4]. Copyright © (2012) Massachusetts Medical Society. Reprinted with permission
Timing of Puberty
In the general population, there is a near-normal distribution of the timing of puberty, with the mean age of onset of G2 at 11.5 years in boys (Fig. 4.2). In healthy boys, the normal age limits for G2 development are between 9.5 and 14 years [4]. While a large variability in the timing of pubertal onset exists, clear age cutoffs for normal pubertal development have been established. However, the age limits for identifying children who need evaluation for precocious or delayed puberty may vary among different ethnic groups. Within this distribution, there has been in recent years an increasing degree of skew at both ends of the spectrum, as an increasing prevalence of an earlier age of pubertal onset (G2) has been documented in some populations as well as an increase in the number of children completing puberty at a later age [5].

Puberty normogram of the timing of genital Tanner staging in healthy boys. This staged line drawing gives age in years on the x-axis and centiles on the y-axis. Each curved line represents one genital tanner stage from 1–5 and illustrates the distribution of the timing of each stage in the normal population. These data have been incorporated into UK growth charts and are available at www.growthcharts.rcpch.ac.uk. Original concept and data from van Buuren [167]
Peak height velocity (PHV) and peak pubertal growth hormone production coincide approximately with the midpoint of pubertal development (Fig. 4.3). In boys, the PHV coincides with G3-4 at an average age of 13.5 years and achieves an incremental rate of 9.5 cm/yr [6]. Up to 25% of total adult height is achieved from growth during puberty, but the amplitude and peak velocity of the pubertal growth spurt are not fixed and vary with age at onset of puberty [7]. Early puberty is associated with a large pubertal growth spurt, while late maturers, who have a longer prepubertal period of growth, in turn experience a less pronounced pubertal growth spurt [8]. Therefore, although extremes of pubertal timing may lead to a small degree of final height reduction due to the reduced overall period of growth in precocious puberty, or poor PHV in delayed puberty [9], in general within wide limits, the timing of puberty does not influence adult height.

Relationship between peak height velocity and pubertal development (male). P pubic hair stage; PHV peak height velocity; T testicular growth; G genital stage. Age ranges presented: in linear format—3rd–97th centiles for each Tanner stage, e.g., G2; in colored boxes—age range in years for each parameter
Regulators of the Timing of Puberty
Variability in the timing of puberty in healthy adolescents is governed by complex regulatory mechanisms involving genetic, environmental, and other factors [10]. Nutritional status, adoption, geographical migration, and emotional well-being have all been shown to affect pubertal timing [11,12,13]. While the timing of pubertal onset in girls in most countries in the developed world exhibited a rapid decrease in the first half of the twentieth century [14, 15], in boys, these trends are less clear. A small but significant change in the normal spectrum of timing of G2 development was documented in a European cohort [16] and in the USA [17] but remains controversial [18]. Much has been postulated about this observed secular trend toward an earlier age of pubertal onset in the developed world [19]. It also follows that it is difficult to understand the pathophysiology of delayed puberty before we can interpret this population level advancement in pubertal age.
Nutritional changes clearly have an important role, as shown by the positive correlation between age at puberty onset and childhood body size [20], most markedly in girls [11]. He and Karlberg demonstrated in a large dataset (n = 3650) that one BMI unit increase between the ages of 2 and 8 years is associated with a 0.11 year advancement in the timing of puberty as measured by peak height velocity in both genders [21]. In boys, however, the data are less consistent, with some studies documenting an earlier onset of puberty with greater adiposity, and some a later onset. In particular, more European studies have noted the former trend, while US studies have more often shown the latter [22]. A recent study from the USA reported a far more complex relationship between fat mass and pubertal timing, with overweight status being associated with earlier pubertal onset, while obesity was associated with later onset. These effects also vary between ethnic groups [23]. Thus, one hypothesis in boys is that greater BMI leads to earlier pubertal timing up to the threshold at which obesity occurs. Obesity may delay pubertal timing in boys due to the suppression of the HPG axis with adiposity leading to excess aromatase activity and thus increased estrogen production.
Additional data point to an earlier trend in the age of puberty onset that is independent of BMI [24]. As detailed above, some studies suggest that over the last decade, the age of completion of puberty in males in some populations has become skewed toward later ages [5]. The effect of possible endocrine-disrupting chemicals (EDCs) on the timing of puberty is also an ongoing concern [5, 25]. Polybrominated biphenyls, bisphenol A, atrazine (herbicides), and phthalates, among others, have been suggested as possible EDCs responsible for contributing to this observed trend [26]. For example, children migrating for international adoption, and previously exposed to the estrogenic insecticide DTT in their country of origin, displayed early or precocious pubertal timing [27]. However, a mechanism of action for EDCs through the early initiation of the pulsatility of GnRH has not been conclusively demonstrated. Studies are complicated by the likely differing and possibly divergent influence of variable doses and mixtures of EDCs, and differing effects depending on age and length of exposure [5, 27, 28].
Epigenetic regulators are potential mediators of the effects of the environment on the hypothalamic control of puberty. However, while experimental data from rats provide evidence for changes in histone acetylation and gene methylation leading to altered gene expression during sexual development, the link between environmental factors and the epigenetic control of puberty has not been established. Although the window of opportunity for the effects of EDC exposure was historically considered to occur in the late prepubertal period, evidence of a fetal and neonatal origin for changes in pubertal timing counters this dogma. A multicenter US study found that prenatal exposure of boys to EDCs such as phthalates, based on the concentrations of four phthalate metabolites in a sample of urine, was associated with a short anogenital index, a marker for reduced masculinization of genital structures [29] (see Chap. 14). Epigenetic changes during fetal life are a potential mechanism for the effects of EDCs in utero [5]. Recent evidence suggests that effects of EDCs may persist in pregnant rats in not only their unborn fetus but into the next generation [30].
Despite the demonstrated importance of environmental factors, the genetic influence on pubertal timing is clearly fundamental. While the timing of pubertal onset varies within and between different populations, it is a highly heritable trait. The timing of sexual maturation is highly correlated within families and in twin studies, suggesting strong genetic determinants [31]. Previous epidemiological studies and genetic approaches estimate that 60–80% of the variation in pubertal onset is under genetic regulation [14, 32, 33]. Despite this strong heritability, however, little is known about the genetic control of human puberty either in the normal population or in cases of disturbed pubertal timing [4]. A lack of clear understanding of the genetic factors that control and trigger the onset of puberty is an important barrier to deciphering the mystery of EDC and other environment/external cues to understand the secular trend toward earlier puberty [34].
Endocrine Changes During Puberty
Gonadotropin-Releasing Hormone and Gonadotropins
The hypothalamus–pituitary–gonadal (HPG) axis is already functional in the late fetal and neonatal period. The development of the HPG axis is exceptional in that GnRH is produced by hypothalamic neurons that develop outside of the central nervous system. The embryonic migration of GnRH neurons from the posterior wall of the nasal cavity to hypothalamus is key for the creation of the neuroendocrine pathways that allow normal pubertal development [35]. The whole process of migration involves no more than a few hundred neurons per hemisphere in the mouse (several thousand in primates or humans) [36]. The absolute number of GnRH neurons required for pubertal development is not known, but there appears to be a degree of redundancy in the system [37]. In addition, adult reeler mice have significantly fewer GnRH neurons in the hypothalamus and display a phenotype of delayed pubertal maturation and low fertility [38].
During gestation, there is an increase in GnRH content, which peaks at 34–38 weeks in the male fetus [39]. At mid-gestation, there is a striking rise in circulating gonadotropin levels in both male and female fetuses which fall to low levels in late gestation. This change in gonadotropin secretion is thought to result from the development of sex steroid negative feedback and from inhibiting influences from the CNS to GnRH neurons.
LH and FSH secretions rise during the first month after birth, probably because the negative feedback effect of placental estrogens is withdrawn. LH is secreted in pulses during this postnatal period indicating control by GnRH [40]. While the HPG axis is active during this ‘mini-puberty,’ it becomes dormant in young children between the age of 2 and 8–9 years [41]. Suppression of the axis is not absolute, however, as LH pulsatility is detectable during this stage using ultrasensitive assays, but pulses are infrequent, of low amplitude and occur mostly at night [42].
The clinical features of puberty are initiated by reactivation of the HPG axis after this relative quiescence during childhood. During this reactivation, there is a gradual development of a dynamic interplay between the central production of GnRH and gonadotropins, and gonadal sex steroid production, with progressive maturation of negative and positive feedback loops. The central suppressant drive from the CNS gradually abates, and intensifying positive feedback results from the increase in sex steroid production by the gonads. The gonadal inhibition of the hypothalamic–pituitary system occurs later, becoming operative only at mid-puberty, and eventually becomes dominant over the central inhibitory feedback drive (Fig. 4.4). Both mean LH and FSH levels increase through pubertal development, although LH rises to a greater extent, probably due to mechanistic differences in feedback by estradiol and inhibin for these two hormones [43]. These rises are due to both an increase in basal levels of LH and FSH, and to a greater number and amplitude of LH pulses.

A model showing the regulation of the hypothalamic–pituitary–gonadal axis during pubertal development
Sex Steroids and Inhibin-B
LH controls sex steroid production by upregulating expression of the steroidogenic enzymes and by controlling metabolic activity of the steroid-producing Leydig cells (see Chap. 2). LH may also stimulate Leydig cell proliferation and differentiation [44]. During puberty, plasma testosterone levels increase dramatically. Table 4.2 summarizes the levels of testosterone at various developmental stages with respective testis sizes. The pubertal increase in testis size results primarily from an increased number of proliferating and differentiating germ cells and to an increase in the number of Sertoli cells [45]. In early and mid-puberty, there is a pronounced diurnal rhythm with a morning peak in testosterone levels, but this is less pronounced in later puberty, and declines gradually with age [46], probably due to decreased day–night ratios of gonadotropins [47].
Inhibin-B is a heterodimeric glycoprotein produced by Sertoli cells beginning in the fetus. Several studies show that serum inhibin-B levels in children change in concert with the secretion of gonadotropins [48,49,50]. During the ‘mini-puberty,’ serum inhibin-B levels increase to similar [51, 52] or even higher [49] levels than in adolescent boys and adult men. This early inhibin-B secretion is sustained until the age of 18–24 mo; thereafter, serum concentrations decline to lower but readily measurable levels [49]. Early in puberty, between Tanner stages G1 and G2, serum inhibin-B concentrations again increase to reach peak levels at the Tanner stage G2, but then the levels plateau [48, 50].
Central Control of Puberty via GnRH Upstream Pathways
GnRH pulsatility is coordinated by a balancing act between a number of inhibitory and excitatory neuronal and glial inputs (Fig. 4.5) [53]. Inhibitory inputs are primarily from GABAergic and opiatergic neurons, while glutamate and kisspeptin are the central excitatory neuronal signals. Glial cells additionally facilitate GnRH secretion via growth factor-derived signaling [54]. The onset of puberty is triggered by a decline in these inhibitory signals and an amplification of excitatory inputs, leading to increased frequency and amplitude of GnRH pulses [55]. Before the onset of puberty, GABA release in the preoptic area decreases in female rats [56], and in the rhesus monkey, GABA release into the median eminence decreases concomitant with the pubertal increase of GnRH secretion [57]. In female rats, glutamine synthase is downregulated, and glutamate dehydrogenase becomes more abundant in the hypothalamus at puberty, both leading to increased availability of glutamate [58]. Glutamate agonists are potent stimulators of GnRH secretion, and administration in prepubertal primates can stimulate LH and testosterone secretion [59].

Genetic regulators in the trans-synaptic and glial control of GnRH neurons during puberty. Adapted from Ojeda et al. [53]
Another vital piece in the puzzle of the central control of GnRH release came with the discovery of Kisspeptin. This excitatory neuropeptide was identified as a permissive factor in puberty onset by the discovery of patients with GnRH deficiency who had loss-of-function mutations in the KISS1 receptor, KISS1R (previously known as GPR54) [60, 61]. Mice with knockout of kiss1r were simultaneously discovered to be infertile despite anatomically normal GnRH neurons and normal hypothalamic GnRH content [61]. Their phenotype can be rescued by exogenous delivery of GnRH. Kiss1 knockout mice also have a phenotype consistent with normosmic GnRH deficiency. However, to date, only very rarely have mutations in KISS1 been found in patients with delayed or absent puberty [62], although two potential activating mutations were identified in patients with central precocious puberty (CPP) [63].
Kisspeptin signals directly to GnRH neurones to control pulsatile GnRH release. Kisspeptin is upregulated in both primates and mice in the peri-pubertal period, and its administration in prepubertal rodents advances the onset of puberty [64]. Kisspeptin also appears to be downregulated in functional hypogonadism, suggesting its role as a mediator of the action of environmental factors such as nutritional status and emotional well-being on puberty and reproductive capacity. Kisspeptin signaling is an important element of both positive and negative feedback loops in the HPG axis. While kisspeptin has been identified as a pivotal upstream regulator of GnRH neurons, whether kisspeptin is the key factor that triggers the onset of puberty remains unclear.
An additional excitatory neuropeptide, neurokinin B, has been implicated in the upstream control of GnRH secretion. Identification of this pathway was via the discovery of loss-of-function mutations in TAC3, encoding neurokinin B, and its receptor TACR3, in patients with normosmic GnRH deficiency and pubertal failure [65, 66]. Both KISS1 and TAC3 are expressed by neurons in the arcuate nucleus of the hypothalamus that project to GnRH neurons, and their expression is downregulated by estrogen [67]. However, studies of the effects of neurokinin B administration have provided conflicting results. While central administration of neurokinin B agonists failed to stimulate GnRH release in rodents, and Tacr3 knockout mice have grossly normal fertility [68, 69], primate studies showed that neurokinin B can act to stimulate GnRH release via kisspeptin signaling [70]. Additionally, neurokinin B is expressed more widely in the central nervous system than in kisspeptin, suggesting some differences in the roles of these two neuropeptides in the control of pubertal onset.
Dynorphin, an opioid peptide that is coexpressed with kisspeptin and neurokinin B in so-called KNDy neurons, inhibits the release of GnRH, and together, these peptides are currently believed to play a fundamental role in the GnRH pulse generator. Other neurons regulate GnRH including GABAergic signaling pathways which function in the stress-induced suppression of LH, and RFamide-related peptide gene (RFRP), the mammalian ortholog of the avian peptide gonadotrophin-inhibiting hormone (GnIH) [71].
Glial inputs appear to be predominantly facilitory during puberty, acting via growth factors and small diffusible molecules, including TGFβ1, IGF-1, and neuregulins that directly or indirectly stimulate GnRH secretion [72]. Glial cells in the median eminence regulate GnRH secretion through the production of growth factors that activate receptors with tyrosine kinase activity. FGF signaling is required for GnRH neurons to reach their final destination in the hypothalamus [73], as well as for GnRH neuronal differentiation and survival [74]. Additionally, GnRH neuron secretory activity is facilitated by IGF-1 and by members of the epidermal growth factor family such as neuregulin 1β [54, 75]. Moreover, plastic rearrangements of glia–GnRH neuron adhesiveness, mediated by soluble molecules such as neuronal cell adhesion molecule (NCAM) and synaptic cell adhesion molecule (SynCAM), coordinate the controlled delivery of GnRH to the portal vasculature [72], a process that is subject to sex steroid regulation [76].
The interplay between puberty and metabolism has been the focus of intense study. The role of fat mass in pubertal timing is thought to be mediated, at least in part, through the permissive actions of the metabolic hormone leptin, a key regulator of body mass, secreted from white adipose tissue (WAT) [77]. Absence of leptin signaling results in obesity and infertility, whereas leptin treatment decreases food intake and restores reproductive functions. During fasting, leptin levels decrease and gonadotropin secretion is suppressed. These findings imply that nutritional status, especially fat tissue and leptin, could contribute to pubertal development. Clinical observations have further supported a role for leptin signaling in the onset of puberty, e.g., humans and mice lacking leptin (Lep ob/ob) or the leptin receptor (LepR db/db) fail to complete puberty and are infertile [78], and in a 12-yr-old girl with congenital leptin deficiency, treatment with recombinant leptin was followed by a pubertal pattern of LH release [79].
GnRH neurons do not express the LepR. Instead, leptin appears to indirectly regulate GnRH via actions on cells that are afferent to GnRH neurons such as LEPR-expressing GABA neurons from the arcuate nucleus [80], or via cells that interact morphologically with GnRH neurons, partly through nitric oxide signaling, which is required for leptin action [81], and via kisspeptin/neuropeptide Y neurons [82, 83]. Cross-sectional studies showed that serum leptin levels rise in girls in early puberty [84] but not in boys. In careful longitudinal studies in male rhesus monkeys, leptin levels decreased during the juvenile period and were unchanged during puberty [85, 86], and leptin gene expression in the hypothalamus is unchanged during the development in the rat [87, 88]. Therefore, leptin is probably not the requisite metabolic trigger for the onset of puberty, but rather is a permissive factor signaling healthy energy balance.
Neuropeptide Y (NPY) is involved in many CNS functions, including appetite control and reproduction. Evidence from primate studies suggests that NPY may also have a contributory role in the break restraining the onset of puberty in primates [68, 89]. Ghrelin and other gut-derived peptides may also form part of the mechanism by which energy homeostasis regulates reproductive development [90]. Both low birthweight and prematurity are associated with earlier onset of puberty [91, 92], particularly in those children with rapid increase in length or weight in the first two years of life [93]. It remains unclear, however, whether childhood obesity, insulin resistance, excess androgens, or other factors may explain this association [94, 95].
While GnRH pulsatility is clearly the central driver of pubertal onset, and aberrant GnRH neuronal development and function lead to hypogonadotropic hypogonadism (HH), our collective understanding of the upstream neurocircuitry regulating GnRH neurons remains incomplete. Data pointing to hypothalamic regulation via a hierarchical network of genes (Fig. 4.6) have mainly come from a systems biology approach and from animal models, with little data from human subjects [96]. Candidate transcriptional regulators that have been identified via these approaches include Oct-2, TTF-1, and EAP1 [97,98,99].

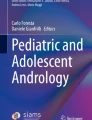
Algorithm for the evaluation of boys with delayed puberty. CDGP constitutional delay of growth and puberty, GI gastrointestinal, GH growth hormone, GHD GH deficiency, PRL prolactin, and IGF-1 insulin-like growth factor 1. Adapted from Palmer and Dunkel [4]. Copyright © (2012) Massachusetts Medical Society. Reprinted with permission
Delayed Puberty
Presentation
Disturbances of puberty encompass an important group of pathologies within the field of pediatric endocrinology. First, they are common, affecting over 4% of adolescents. In addition, abnormal timing of pubertal development is associated with adverse health and psychosocial outcomes [100,101,102]. This has importance for the individual, but also has a potential major impact on public health, especially in view of the secular trend toward an earlier age of puberty onset [25]. Early puberty, in particular, is associated with adverse health outcomes, including breast [103] and endometrial cancer [104], obesity [105], type 2 diabetes [102], cardiovascular disease [106, 107], short stature [108], and even increased mortality [106]. However, persons with delayed puberty are also at risk of short adult height [109,110,111,112], decreased bone mineral density [113, 114], and psychological sequelae [115, 116].
Self-limited Delayed Puberty
Self-limited delayed puberty (DP), also known as constitutional delay of growth and puberty (CDGP), represents the most common cause of delayed puberty in both sexes. Up to 63% of boys with delayed puberty have self-limited DP [117]. Self-limited DP segregates within families, with the majority of families displaying an autosomal dominant pattern of inheritance (with or without complete penetrance) [31]. Fifty to 75% of subjects with self-limited DP have a family history of delayed puberty onset [118].
Patients with self-limited DP represent the extreme tail of normal puberty, defined as the markers of the onset of puberty occurring two or more standard deviation (SD) later than the population mean age for gender. In addition, self-limited DP may encompass older children with delayed pubertal progression, a diagnosis that is aided by the use of puberty nomograms (Fig. 4.2) [119]. The absence of a pathological medical history, signs and symptoms, and a positive family history of delayed puberty in one or both of the parents suggests a diagnosis of self-limited DP; however, before making that diagnosis, pathological conditions must be excluded.
In DP, probably because of a low estrogen concentration for chronological age (but not for bone age), growth hormone (GH) secretion is functionally and temporally reduced for age, and when this functional GH deficiency is prolonged, it may also impact adult height. After the onset of puberty or the initiation of appropriate treatment, growth velocity and GH secretion return to normal. Additionally, in about half of the subjects with constitutional delay, there is delayed maturation during early childhood, and consequently, they are shorter than their peers even before the mean age for the pubertal growth spurt [119].
It has been shown that those self-limited DP subjects who also have reduced growth in childhood may not fully exploit their genetic height potential, resulting in an adult height below their mid-parental target height [112, 120,121,122], with an average loss of 4.2 cm if untreated [122]. However, the majority of the patients seen at pediatric endocrinology clinics are short because their condition is compounded by two independent factors: short genetic height potential and DP. Other studies showed only a negligible difference in final height, even in DP subjects who have received no intervention [109, 123,124,125,126,127,128]. This may imply a pathophysiological mechanism in addition to lack of sex steroids contributing to the growth phenotype in some patients with DP, but not in others [128].
In self-limited DP, adrenarche may also occur later than usual [4]. Bone age in self-limited DP is retarded compared to chronological age, but the developmental milestones are achieved at a normal bone age, that is, onset of signs of pubertal development by a bone age of 13.5 years in boys. Gonadotropin and sex steroid concentrations increase in concert with the progression of the bone age. Thus, all stages of pubertal development occur at an age that is later than average.
There are three main differential diagnoses of self-limited DP [4, 117] (Table 4.3): hypergonadotropic hypogonadism, with primary gonadal failure leading to elevated gonadotropin levels (approximately 7% of males with delayed puberty); functional hypogonadotropic hypogonadism, where late pubertal development is due to maturational delay in the HPG axis secondary to a chronic disease [129] (found in 19–20%), malnourishment [130], excessive exercise [131, 132], or psychological or emotional stress [133]; and permanent hypogonadotropic hypogonadism (HH), characterized by low LH and FSH levels (9% of boys).
Hypogonadotropic Hypogonadism
HH is often diagnosed during the second or third decades of life. Common presenting signs are delayed onset of puberty, poorly developed secondary sexual characteristics, eunuchoid body proportions, or infertility [134]. This condition can be due to a congenital hypothalamic or pituitary disorder or to an acquired central dysfunction secondary to irradiation, surgery, tumor, or a vascular lesion. Tumors causing delayed puberty most commonly interfere with GnRH synthesis or secretion, the most common being craniopharyngioma, germinoma, and Langerhans cell histiocytosis. A deficiency of other anterior pituitary hormones, diabetes insipidus, and visual disturbance is common. Congenital malformation of the pituitary, hypothalamic, and other midline structures may cause HH, often in conjunction with other pituitary hormone deficiencies.
A picture of ‘idiopathic’ hypogonadotropic hypogonadism (IHH) with no associated anatomical or functional defect in the hypothalamic–pituitary–gonadal axis occurs in 1–10 cases per 100,000 births. Because of different causes and incomplete penetrance, there is a wide spectrum of phenotypes, ranging from complete hypogonadotropic hypogonadism, with lack of pubertal development, to partial hypogonadism with an arrest of pubertal development, and even reversible HH in some patients post treatment [135]. Despite recent advances, with over twenty genes linked with this disorder having been identified, the pathophysiological basis of hypogonadotropic hypogonadism in the majority of individuals remains unclear [136] (see Chap. 5). The condition may be due to the failure of the development of gonadotropin-releasing hormone (GnRH) neurons, lack of activation of GnRH secretion, or disrupted GnRH signaling (including mutations in the GNRHR gene). Kallmann syndrome (hypogonadotropic hypogonadism associated with anosmia) is the most common form of isolated HH, accounting for 60% of cases.
Downstream mutations in the GnRH signaling pathway can also present as delayed puberty. LH and FSH are encoded by a common α-subunit gene and a specific β-subunit gene. Mutations of the β-subunits genes of LH or FSH are extremely rare causes of HH [137, 138] (see Chap. 6).
Functional Hypogonadotropic Hypogonadism
Functional HH is seen in malnutrition and chronic diseases, as exemplified by patients with inflammatory bowel disease, celiac disease, chronic kidney disease, cystic fibrosis, and sickle cell anemia. Undernutrition in states of starvation such as anorexia nervosa, or an imbalance due to excess energy consumption in extreme athletic training, can also cause central GnRH suppression. The factors contributing to these states of functional HH include low fat mass, inflammation, and stress [139, 140].
Hypergonadotropic Hypogonadism
Hypergonadotropic states (chromosomal alterations, syndromes, genetic disorders, and radiotherapy/chemotherapy) are covered elsewhere in this volume (see Chaps. 9 and 10) and may present as pubertal delay. Testicular abnormalities are characterized by elevated gonadotropin and low inhibin-B concentrations, and patients with these abnormalities sometimes have specific physical features.
Delayed Puberty—Diagnosis
The cutoff age for boys who need an evaluation for delayed puberty may vary in different ethnic groups, but in most populations, early signs of secondary sexual development should be present by age 14 years. The evaluation of testicular volume is vital, as an accurate diagnosis of delayed puberty cannot be made without assessment of Tanner genital stage. A thorough medical history should note the symptoms and signs of anorexia nervosa, the intensity of athletic training, and the timing of puberty of both parents, as there is often a family history of DP in cases of self-limited DP (Fig. 4.6). A history of chronic illness, such as celiac disease or inflammatory bowel disease, suggests a temporary or secondary delay of puberty. Stature and height velocity should be evaluated using appropriate growth charts. Bone age (X-ray film of left hand and wrist read according to standards such as Greulich and Pyle) delay provides useful information in the growth analysis but contributes little to the differential diagnosis. It may be very difficult to distinguish clinically between the diagnosis of self-limited DP and congenital HH in the teenage years [141]. While gonadotropin levels are generally increased in primary testicular failure or in Klinefelter syndrome, single basal serum LH and FSH determinations are not useful in the differential diagnosis of self-limited delay vs hypogonadotropic hypogonadism.
In some cases, the diagnosis of permanent HH can be suspected before the age of pubertal onset, and importantly, if this suspicion arises in the first six months of life, it can be confirmed on the basis of low testosterone and gonadotropin levels, indicating an absence of the normal ‘mini-puberty.’ The presence or absence of ‘red flag’ features remains the strongest discriminator between self-limited DP and IHH. These red flags include cryptorchidism or micropenis, or the presence of the other components of the Kallmann syndrome which include anosmia or hyposmia due to hypoplasia of the olfactory bulbs, as well as cleft lip and palate, unilateral renal agenesis, short metacarpals, sensorineural hearing loss, synkinesia, and color blindness.
Investigation of the differential diagnosis of the two conditions may involve a number of physiological and dynamic tests including assessment of LH pulsatility by frequent blood sampling [42], the prolactin response to provocation [142, 143], the gonadotropin response to GnRH [144, 145] and analogs [146], the testosterone response to hCG [146,147,148], and first morning-voided urinary FSH and LH levels [149]. Boys with self-limited delay who are destined to undergo spontaneous pubertal development within 6 to 12 months may have a pubertal pattern of response to GnRH (post-GnRH maximum LH levels higher than maximum FSH levels). However, a low prepubertal LH response to GnRH is usually found in boys with self-limited DP who will develop later than that, as well as in boys with permanent HH. Most recently, a single measurement of inhibin-B <35 pg/mL has been shown to help discriminate prepubertal boys with IHH from DP with high sensitivity [150]; nevertheless, patient follow-up is necessary for a definitive diagnosis in the majority of cases. With the discovery in the last two decades of genes causing HH, genetic testing will no doubt modify the management of many of our male delayed puberty patients [151].
Male Delayed Puberty—Therapeutic Indications
Induction or progression of puberty is indicated for adolescents who have either significantly delayed or arrested puberty, or have been diagnosed with permanent hypogonadism. Appropriate treatment modalities are directed according to the underlying diagnosis.
A management strategy of ‘watchful waiting’ may be appropriate in self-limited DP, where pubertal onset is late but expected to occur spontaneously. However, this decision should be taken in conjunction with the patients, taking into consideration their concerns and expectations. One major concern often raised by patients and their families is the effect of delayed puberty on both current and final height, particularly for patients with concurrent familial short stature. However, patients can be reassured that adult height in DP is usually only slightly below genetic height potential (target height), although there may be large individual variation [121, 152]. If height is not a major concern, reassurance with accurate adult height prediction is frequently sufficient, especially if puberty has already started. DP in adolescents can, however, be associated with significant anxiety about body image in terms of physical size and pubertal immaturity, decreased self-esteem with social isolation, withdrawal from sporting activities, and psychosocial and peer relationship difficulties. In these circumstances, there is evidence that hormonal therapy can be beneficial [153, 154]. The link between DP and reduced academic performance, substance misuse, and behavioral difficulties is less well established.
In contrast, if ‘red flag’ markers of hypogonadism are present, or if endogenous gonadotropin-dependent puberty has not started after one year of treatment, then permanent HH and other diagnoses should be reconsidered, and a brain MRI should be performed. In such instances, treatment should be initiated promptly in order to optimize skeletal growth and induce secondary sexual characteristics and, therefore, minimize the psychosocial difficulties faced by adolescents with hypogonadism.
Management of Delayed Puberty—Therapeutic Principles
The options for the management of male patients with self-limited DP include monitoring with reassurance, or therapy with low-dose testosterone to augment the growth rate and induce secondary sexual characteristics (Table 4.4). There are numerous published studies of treatment of DP in boys, but most are observational, with a few small randomized controlled trials [154,155,156]. Most report treatment with short courses of low-dose androgens with outcomes of increased height velocity without advanced bone age, advanced sexual maturation, and often improvement in psychosocial parameters.
The most commonly used treatment regimen for low-dose testosterone for boys with DP is supplementation using intramuscular depot preparations of a testosterone ester [157], at a starting dose of 50 mg each month for 3–6 months; a further 3–6 months of treatment may be given, with dose escalation as required. Oral testosterone undecanoate (where available) at a dose of 40–160 mg daily has recently been shown to be safe and efficacious for pubertal induction in DP, without compromise in final height [119] (Table 4.4). Topical testosterone gels may also be suitable for this indication [158]. Monitoring via serum testosterone increase (to mid-reference range one week post injection), basal LH increase, height velocity, testicular volume, and extent of virilization is appropriate. GH deficiency must be excluded if height velocity does not increase with testosterone therapy. Testosterone esters should be avoided in patients with hepatic impairment or hypercalcaemia and used with caution in chronic kidney disease [159]. Preparations are generally well tolerated, but side effects may include headaches, depression, and androgenic effects such as acne. Although anabolic steroids such as oxandrolone have been used historically for short-term increase in height velocity, they are less effective in stimulating pubertal development and therefore are not recommended for the management of boys with delayed puberty.
As discussed above, self-limited DP is commonly seen in combination with idiopathic short stature (ISS). After exclusion of GH deficiency, for example, by the use of a primed GH provocation test, the treatment of GH-replete DP patients with growth hormone remains controversial: It has been approved by the US Food and Drug Administration for the treatment of ISS and height SDS <2.25 for age, but leads to only a modest increase in adult height, and its use is not recommended by the authors [160, 161].
A further potential pharmacological target in short boys with DP is the inhibition of estrogen biosynthesis from androgens using aromatase inhibitors [162, 163]. Epiphyseal closure is dependent on estrogens, and thus, aromatase inhibitors (AIs) can potentially act to extend the time period in which long bone growth occurs and therefore increase adult height. Some published data support this use of AIs to delay bone maturation and increase adult height in boys with short stature and/or delayed puberty [162, 163]. However, there remains much uncertainty in terms of efficacy, optimization, and safety profile of AI therapy [164], and the optimal dose, timing, and duration of treatment in ISS and DP remain uncertain. Controlled trials have pointed to potential adverse effects, in particular compromised trabecular bone health in the form of vertebral body deformities in boys with ISS treated with letrozole [165]. Until more information from ongoing studies of these agents is available, active management should not involve aromatase inhibitors unless used within the setting of a clinical trial.
Concluding Remarks
In healthy boys, the normal age limits for the first signs of secondary sexual development are between 9.5 and 14 years. There are multiple genetic and environmental influences on the timing of puberty in the general population, and appropriate age cutoffs for delayed puberty in different ethnic groups may vary.
DP is a frequent problem, and the most common underlying condition is self-limited (or constitutional) DP, which is usually accompanied by delayed growth. However, the differential diagnoses include hypogonadotropic and hypergonadotropic hypogonadism, and these conditions must be considered in boys with pubertal delay. Distinguishing between self-limited DP and permanent hypogonadotropic hypogonadism remains difficult.
Management of male adolescents with DP is dependent on the underlying cause. Treatment of isolated DP involves expectant observation or short courses of testosterone in low doses, while more complex and involved management is required for males with permanent hypogonadism. However, a proportion of young men with DP will remain adversely affected by their delayed pubertal development and/or short stature in adolescence, which may have long-term consequences. It is not known whether pubertal delay has a negative impact on adult bone mass [166], and whether potentially compromised bone health is a reason to initiate sex steroid replacement. Additionally, the optimal management of males with severe hypogonadotropic hypogonadism (cryptorchidism, micropenis, and lack of spontaneous increase in testicular size in puberty) remains uncertain. Whether such patients would benefit from prepubertal FSH treatment to improve potential for future fertility is another unanswered question (see Chap. 20).
The genetic and environmental basis for both DP and HH is an area of research where there is still much to be discovered, and may bring future benefits for patient management. Our understanding of the key controllers of pubertal onset and its timing is advancing but remains a complex puzzle to be unlocked. Mechanistic discoveries in DP and hypogonadism patients are also likely to shed light on the changes in pubertal timing in the general population.
References
Marshall WA, Tanner JM. Variations in the pattern of pubertal changes in boys. Arch Dis Child. 1970;45(239):13–23.
Knorr D, Bidlingmaier F, Butenandt O, Fendel H. Plasma testosterone in male puberty. I. Physiology of plasma testosterone. Acta Endocrinol. 1974;75(1):181–94.
Nielsen CT, Skakkebaek NE, Richardson DW, Darling JA, Hunter WM, Jorgensen M, et al. Onset of the release of spermatozoa (spermarche) in boys in relation to age, testicular growth, pubic hair, and height. J Clin Endocrinol Metab. 1986;62(3):532–5.
Palmert MR, Dunkel L. Clinical practice. Delayed puberty. N Engl J Med. 2012;366(5):443–53.
Parent AS, Franssen D, Fudvoye J, Gerard A, Bourguignon JP. Developmental variations in environmental influences including endocrine disruptors on pubertal timing and neuroendocrine control: revision of human observations and mechanistic insight from rodents. Front Neuroendocrinol. 2015;38:12–36.
Wagner IV, Sabin MA, Pfaffle RW, Hiemisch A, Sergeyev E, Korner A, et al. Effects of obesity on human sexual development. Nat Rev Endocrinol. 2012;8(4):246–54.
Bourguignon JP. Growth and timing of puberty: reciprocal effects. Horm Res. 1991;36(3–4):131–5.
Gasser T, Sheehy A, Molinari L, Largo RH. Growth of early and late maturers. Ann Hum Biol. 2001;28(3):328–36.
Biro FM, McMahon RP, Striegel-Moore R, Crawford PB, Obarzanek E, Morrison JA, et al. Impact of timing of pubertal maturation on growth in black and white female adolescents: the national heart, lung, and blood institute growth and health study. J Pediatr. 2001;138(5):636–43.
Gamba M, Pralong FP. Control of GnRH neuronal activity by metabolic factors: the role of leptin and insulin. Mol Cell Endocrinol. 2006;254–255:133–9.
Juul A, Teilmann G, Scheike T, Hertel NT, Holm K, Laursen EM, et al. Pubertal development in Danish children: comparison of recent European and US data. Int J AndroL. 2006;29(1):247–55; discussion 86–90.
Teilmann G, Pedersen CB, Skakkebaek NE, Jensen TK. Increased risk of precocious puberty in internationally adopted children in Denmark. Pediatrics. 2006;118(2):e391–9.
Mul D, Fredriks AM, van Buuren S, Oostdijk W, Verloove-Vanhorick SP, Wit JM. Pubertal development in The Netherlands 1965–1997. Pediatr Res. 2001;50(4):479–86.
Parent AS, Teilmann G, Juul A, Skakkebaek NE, Toppari J, Bourguignon JP. The timing of normal puberty and the age limits of sexual precocity: variations around the world, secular trends, and changes after migration. Endocr Rev. 2003;24(5):668–93.
de Muinich Keizer SM, Mul D. Trends in pubertal development in Europe. Human Reprod Update. 2001;7(3):287–91.
Sorensen K, Aksglaede L, Petersen JH, Juul A. Recent changes in pubertal timing in healthy Danish boys: associations with body mass index. J Clin Endocrinol Metab. 2010;95(1):263–70.
Herman-Giddens ME, Steffes J, Harris D, Slora E, Hussey M, Dowshen SA, et al. Secondary sexual characteristics in boys: data from the pediatric research in office settings network. Pediatrics. 2012;130(5):e1058–68.
Euling SY, Herman-Giddens ME, Lee PA, Selevan SG, Juul A, Sorensen TI, et al. Examination of US puberty-timing data from 1940 to 1994 for secular trends: panel findings. Pediatrics. 2008;121(Suppl 3):S172–91.
Ong KK, Ahmed ML, Dunger DB. Lessons from large population studies on timing and tempo of puberty (secular trends and relation to body size): the European trend. Mol Cell Endocrinol. 2006;254–255:8–12.
Biro FM, Khoury P, Morrison JA. Influence of obesity on timing of puberty. Int J Androl. 2006;29(1):272–7; discussion 86–90.
He Q, Karlberg J. Bmi in childhood and its association with height gain, timing of puberty, and final height. Pediatr Res. 2001;49(2):244–51.
De Leonibus C, Marcovecchio ML, Chiarelli F. Update on statural growth and pubertal development in obese children. Pediatr Rep. 2012;4(4):e35.
Lee JM, Wasserman R, Kaciroti N, Gebremariam A, Steffes J, Dowshen S, et al. Timing of puberty in overweight versus obese boys. Pediatrics. 2016;137(2):1–10.
Aksglaede L, Juul A, Olsen LW, Sorensen TI. Age at puberty and the emerging obesity epidemic. PLoS ONE. 2009;4(12):e8450.
Mouritsen A, Aksglaede L, Sorensen K, Mogensen SS, Leffers H, Main KM, et al. Hypothesis: exposure to endocrine-disrupting chemicals may interfere with timing of puberty. Int J Androl. 2010;33(2):346–59.
Caserta D, Maranghi L, Mantovani A, Marci R, Maranghi F, Moscarini M. Impact of endocrine disruptor chemicals in gynaecology. Human Reprod Update. 2008;14(1):59–72.
Krstevska-Konstantinova M, Charlier C, Craen M, Du Caju M, Heinrichs C, de Beaufort C, et al. Sexual precocity after immigration from developing countries to Belgium: evidence of previous exposure to organochlorine pesticides. Hum Reprod. 2001;16(5):1020–6.
van den Driesche S, Macdonald J, Anderson RA, Johnston ZC, Chetty T, Smith LB, et al. Prolonged exposure to acetaminophen reduces testosterone production by the human fetal testis in a xenograft model. Sci Transl Med. 2015;7(288):288ra80.
Swan SH, Main KM, Liu F, Stewart SL, Kruse RL, Calafat AM, et al. Decrease in anogenital distance among male infants with prenatal phthalate exposure. Environ Health Perspect. 2005;113(8):1056–61.
Dean A, van den Driesche S, Wang Y, McKinnell C, Macpherson S, Eddie SL, et al. Analgesic exposure in pregnant rats affects fetal germ cell development with inter-generational reproductive consequences. Sci Rep. 2016;6:19789.
Wehkalampi K, Widen E, Laine T, Palotie A, Dunkel L. Patterns of inheritance of constitutional delay of growth and puberty in families of adolescent girls and boys referred to specialist pediatric care. J Clin Endocrinol Metab. 2008;93(3):723–8.
Gajdos ZK, Hirschhorn JN, Palmert MR. What controls the timing of puberty? An update on progress from genetic investigation. Curr Opin Endocrinol Diabetes Obes. 2009;16(1):16–24.
Morris DH, Jones ME, Schoemaker MJ, Ashworth A, Swerdlow AJ. Familial concordance for age at menarche: analyses from the breakthrough generations study. Paediatr Perinat Epidemiol. 2011;25(3):306–11.
Tena-Sempere M. Kisspeptin/GPR54 system as potential target for endocrine disruption of reproductive development and function. Int J Androl. 2010;33(2):360–8.
Wray S. From nose to brain: development of gonadotrophin-releasing hormone-1 neurones. J Neuroendocrinol. 2010;22(7):743–53.
Cariboni A, Maggi R, Parnavelas JG. From nose to fertility: the long migratory journey of gonadotropin-releasing hormone neurons. Trends Neurosci. 2007;30(12):638–44.
Herbison AE, Porteous R, Pape JR, Mora JM, Hurst PR. Gonadotropin-releasing hormone neuron requirements for puberty, ovulation, and fertility. Endocrinology. 2008;149(2):597–604.
Cariboni A, Rakic S, Liapi A, Maggi R, Goffinet A, Parnavelas JG. Reelin provides an inhibitory signal in the migration of gonadotropin-releasing hormone neurons. Development. 2005;132(21):4709–18.
Siler-Khodr TM, Khodr GS. Studies in human fetal endocrinology. I. Luteinizing hormone-releasing factor content of the hypothalamus. Am J Obstet Gynecol. 1978;130(7):795–800.
Waldhauser F, Weissenbacher G, Frisch H, Pollak A. Pulsatile secretion of gonadotropins in early infancy. Eur J Pediatr. 1981;137(1):71–4.
Beate K, Joseph N, de Nicolas R, Wolfram K. Genetics of isolated hypogonadotropic hypogonadism: role of GnRH receptor and other genes. Int J Endocrinol. 2012;2012:147893.
Dunkel L, Alfthan H, Stenman UH, Tapanainen P, Perheentupa J. Pulsatile secretion of LH and FSH in prepubertal and early pubertal boys revealed by ultrasensitive time-resolved immunofluorometric assays. Pediatr Res. 1990;27(3):215–9.
Albertsson-Wikland K, Rosberg S, Lannering B, Dunkel L, Selstam G, Norjavaara E. Twenty-four-hour profiles of luteinizing hormone, follicle-stimulating hormone, testosterone, and estradiol levels: a semilongitudinal study throughout puberty in healthy boys. J Clin Endocrinol Metab. 1997;82(2):541–9.
Chemes HE, Gottlieb SE, Pasqualini T, Domenichini E, Rivarola MA, Bergada C. Response to acute hCG stimulation and steroidogenic potential of Leydig cell fibroblastic precursors in humans. J Androl. 1985;6(2):102–12.
Rey RA, Campo SM, Bedecarras P, Nagle CA, Chemes HE. Is infancy a quiescent period of testicular development? Histological, morphometric, and functional study of the seminiferous tubules of the cebus monkey from birth to the end of puberty. J Clin Endocrinol Metab. 1993;76(5):1325–31.
Brambilla DJ, Matsumoto AM, Araujo AB, McKinlay JB. The effect of diurnal variation on clinical measurement of serum testosterone and other sex hormone levels in men. J Clin Endocrinol Metab. 2009;94(3):907–13.
Ankarberg-Lindgren C, Norjavaara E. Changes of diurnal rhythm and levels of total and free testosterone secretion from pre to late puberty in boys: testis size of 3 ml is a transition stage to puberty. Eur J Endocrinol/Eur Fed Endocr Soc. 2004;151(6):747–57.
Andersson AM, Juul A, Petersen JH, Muller J, Groome NP, Skakkebaek NE. Serum inhibin B in healthy pubertal and adolescent boys: relation to age, stage of puberty, and follicle-stimulating hormone, luteinizing hormone, testosterone, and estradiol levels. J Clin Endocrinol Metab. 1997;82(12):3976–81.
Andersson AM, Toppari J, Haavisto AM, Petersen JH, Simell T, Simell O, et al. Longitudinal reproductive hormone profiles in infants: peak of inhibin B levels in infant boys exceeds levels in adult men. J Clin Endocrinol Metab. 1998;83(2):675–81.
Raivio T, Perheentupa A, McNeilly AS, Groome NP, Anttila R, Siimes MA, et al. Biphasic increase in serum inhibin B during puberty: a longitudinal study of healthy Finnish boys. Pediatr Res. 1998;44(4):552–6.
Byrd W, Bennett MJ, Carr BR, Dong Y, Wians F, Rainey W. Regulation of biologically active dimeric inhibin A and B from infancy to adulthood in the male. J Clin Endocrinol Metab. 1998;83(8):2849–54.
Bergada I, Rojas G, Ropelato G, Ayuso S, Bergada C, Campo S. Sexual dimorphism in circulating monomeric and dimeric inhibins in normal boys and girls from birth to puberty. Clin Endocrinol. 1999;51(4):455–60.
Ojeda SR, Lomniczi A, Mastronardi C, Heger S, Roth C, Parent AS, et al. Minireview: the neuroendocrine regulation of puberty: is the time ripe for a systems biology approach? Endocrinology. 2006;147(3):1166–74.
Ojeda SR, Prevot V, Heger S, Lomniczi A, Dziedzic B, Mungenast A. Glia-to-neuron signaling and the neuroendocrine control of female puberty. Ann Med. 2003;35(4):244–55.
Plant TM. Neuroendocrine control of the onset of puberty. Front Neuroendocrinol. 2015;38:73–88.
Goroll D, Arias P, Wuttke W. Preoptic release of amino acid neurotransmitters evaluated in peripubertal and young adult female rats by push-pull perfusion. Neuroendocrinology. 1993;58(1):11–5.
Terasawa E, Luchansky LL, Kasuya E, Nyberg CL. An increase in glutamate release follows a decrease in gamma aminobutyric acid and the pubertal increase in luteinizing hormone releasing hormone release in the female rhesus monkeys. J Neuroendocrinol. 1999;11(4):275–82.
Erecinska M, Silver IA. Metabolism and role of glutamate in mammalian brain. Prog Neurobiol. 1990;35(4):245–96.
Plant TM, Gay VL, Marshall GR, Arslan M. Puberty in monkeys is triggered by chemical stimulation of the hypothalamus. Proc Natl Acad Sci USA. 1989;86(7):2506–10.
de Roux N, Genin E, Carel JC, Matsuda F, Chaussain JL, Milgrom E. Hypogonadotropic hypogonadism due to loss of function of the KiSS1-derived peptide receptor GPR54. Proc Natl Acad Sci USA. 2003;100(19):10972–6.
Seminara SB, Messager S, Chatzidaki EE, Thresher RR, Acierno JS Jr, Shagoury JK, et al. The GPR54 gene as a regulator of puberty. N Engl J Med. 2003;349(17):1614–27.
Topaloglu AK, Tello JA, Kotan LD, Ozbek MN, Yilmaz MB, Erdogan S, et al. Inactivating KISS1 mutation and hypogonadotropic hypogonadism. N Engl J Med. 2012;366(7):629–35.
Silveira LG, Noel SD, Silveira-Neto AP, Abreu AP, Brito VN, Santos MG, et al. Mutations of the KISS1 gene in disorders of puberty. J Clin Endocrinol Metab. 2010;95(5):2276–80.
Navarro VM, Fernandez-Fernandez R, Castellano JM, Roa J, Mayen A, Barreiro ML, et al. Advanced vaginal opening and precocious activation of the reproductive axis by KiSS-1 peptide, the endogenous ligand of GPR54. J Physiol. 2004;561(Pt 2):379–86.
Topaloglu AK, Reimann F, Guclu M, Yalin AS, Kotan LD, Porter KM, et al. TAC3 and TACR3 mutations in familial hypogonadotropic hypogonadism reveal a key role for Neurokinin B in the central control of reproduction. Nat Genet. 2009;41(3):354–8.
Guran T, Tolhurst G, Bereket A, Rocha N, Porter K, Turan S, et al. Hypogonadotropic hypogonadism due to a novel missense mutation in the first extracellular loop of the neurokinin B receptor. J Clin Endocrinol Metab. 2009;94(10):3633–9.
Rance NE. Menopause and the human hypothalamus: evidence for the role of kisspeptin/neurokinin B neurons in the regulation of estrogen negative feedback. Peptides. 2009;30(1):111–22.
Sandoval-Guzman T, Rance NE. Central injection of senktide, an NK3 receptor agonist, or neuropeptide Y inhibits LH secretion and induces different patterns of Fos expression in the rat hypothalamus. Brain Res. 2004;1026(2):307–12.
Kung TT, Crawley Y, Jones H, Luo B, Gilchrest H, Greenfeder S, et al. Tachykinin NK3-receptor deficiency does not inhibit pulmonary eosinophilia in allergic mice. Pharmacol Res Official J Ital Pharmacol Soc. 2004;50(6):611–5.
Ramaswamy S, Seminara SB, Plant TM. Evidence from the agonadal juvenile male rhesus monkey (Macaca mulatta) for the view that the action of neurokinin B to trigger gonadotropin-releasing hormone release is upstream from the kisspeptin receptor. Neuroendocrinology. 2011;94(3):237–45.
Ducret E, Anderson GM, Herbison AE. RFamide-related peptide-3, a mammalian gonadotropin-inhibitory hormone ortholog, regulates gonadotropin-releasing hormone neuron firing in the mouse. Endocrinology. 2009;150(6):2799–804.
Ojeda SR, Lomniczi A, Sandau US. Glial-gonadotrophin hormone (GnRH) neurone interactions in the median eminence and the control of GnRH secretion. J Neuroendocrinol. 2008;20(6):732–42.
Gill JC, Tsai PS. Expression of a dominant negative FGF receptor in developing GNRH1 neurons disrupts axon outgrowth and targeting to the median eminence. Biol Reprod. 2006;74(3):463–72.
Voigt P, Ma YJ, Gonzalez D, Fahrenbach WH, Wetsel WC, Berg-von der Emde K, et al. Neural and glial-mediated effects of growth factors acting via tyrosine kinase receptors on luteinizing hormone-releasing hormone neurons. Endocrinology. 1996;137(6):2593–605.
Prevot V, Rio C, Cho GJ, Lomniczi A, Heger S, Neville CM, et al. Normal female sexual development requires neuregulin-erbB receptor signaling in hypothalamic astrocytes. J Neurosci Official J Soc Neurosci. 2003;23(1):230–9.
Garcia-Segura LM, Melcangi RC. Steroids and glial cell function. Glia. 2006;54(6):485–98.
Elias CF. Leptin action in pubertal development: recent advances and unanswered questions. Trends Endocrinol Metab TEM. 2012;23(1):9–15.
Barash IA, Cheung CC, Weigle DS, Ren H, Kabigting EB, Kuijper JL, et al. Leptin is a metabolic signal to the reproductive system. Endocrinology. 1996;137(7):3144–7.
Farooqi IS, Jebb SA, Langmack G, Lawrence E, Cheetham CH, Prentice AM, et al. Effects of recombinant leptin therapy in a child with congenital leptin deficiency. N Engl J Med. 1999;341(12):879–84.
Zuure WA, Quennell JH, Anderson GM. Leptin responsive and GABAergic projections to the rostral preoptic area in mice. Journal of Neuroendocrinol. 2015.
Bellefontaine N, Chachlaki K, Parkash J, Vanacker C, Colledge W, d’Anglemont de Tassigny X, et al. Leptin-dependent neuronal NO signaling in the preoptic hypothalamus facilitates reproduction. J Clin Investig. 2014;124(6):2550–9.
Qiu X, Dao H, Wang M, Heston A, Garcia KM, Sangal A, et al. Insulin and leptin signaling interact in the mouse KISS1 neuron during the peripubertal period. PLoS ONE. 2015;10(5):e0121974.
Pralong FP. Insulin and NPY pathways and the control of GnRH function and puberty onset. Mol Cell Endocrinol. 2010;324(1–2):82–6.
Ahmed ML, Ong KK, Morrell DJ, Cox L, Drayer N, Perry L, et al. Longitudinal study of leptin concentrations during puberty: sex differences and relationship to changes in body composition. J Clin Endocrinol Metab. 1999;84(3):899–905.
Mann DR, Akinbami MA, Gould KG, Castracane VD. A longitudinal study of leptin during development in the male rhesus monkey: the effect of body composition and season on circulating leptin levels. Biol Reprod. 2000;62(2):285–91.
Plant TM, Durrant AR. Circulating leptin does not appear to provide a signal for triggering the initiation of puberty in the male rhesus monkey (Macaca mulatta). Endocrinology. 1997;138(10):4505–8.
Flier JS. Clinical review 94: What’s in a name? In search of leptin’s physiologic role. J Clin Endocrinol Metab. 1998;83(5):1407–13.
Cheung CC, Thornton JE, Nurani SD, Clifton DK, Steiner RA. A reassessment of leptin’s role in triggering the onset of puberty in the rat and mouse. Neuroendocrinology. 2001;74(1):12–21.
El Majdoubi M, Sahu A, Ramaswamy S, Plant TM. Neuropeptide Y: a hypothalamic brake restraining the onset of puberty in primates. Proc Natl Acad Sci USA. 2000;97(11):6179–84.
Pomerants T, Tillmann V, Jurimae J, Jurimae T. Relationship between ghrelin and anthropometrical, body composition parameters and testosterone levels in boys at different stages of puberty. J Endocrinol Invest. 2006;29(11):962–7.
Persson I, Ahlsson F, Ewald U, Tuvemo T, Qingyuan M, von Rosen D, et al. Influence of perinatal factors on the onset of puberty in boys and girls: implications for interpretation of link with risk of long term diseases. Am J Epidemiol. 1999;150(7):747–55.
Adair LS. Size at birth predicts age at menarche. Pediatrics. 2001;107(4):E59.
Wehkalampi K, Hovi P, Dunkel L, Strang-Karlsson S, Jarvenpaa AL, Eriksson JG, et al. Advanced pubertal growth spurt in subjects born preterm: the Helsinki study of very low birth weight adults. J Clin Endocrinol Metab. 2011;96(2):525–33.
Dunger DB, Ahmed ML, Ong KK. Early and late weight gain and the timing of puberty. Mol Cell Endocrinol. 2006;254–255:140–5.
Ibanez L, Valls C, Ong K, Dunger DB, de Zegher F. Metformin therapy during puberty delays menarche, prolongs pubertal growth, and augments adult height: a randomized study in low-birth-weight girls with early-normal onset of puberty. J Clin Endocrinol Metab. 2006;91(6):2068–73.
Ojeda SR, Dubay C, Lomniczi A, Kaidar G, Matagne V, Sandau US, et al. Gene networks and the neuroendocrine regulation of puberty. Mol Cell Endocrinol. 2010;324(1–2):3–11.
Ojeda SR, Hill J, Hill DF, Costa ME, Tapia V, Cornea A, et al. The Oct-2 POU domain gene in the neuroendocrine brain: a transcriptional regulator of mammalian puberty. Endocrinology. 1999;140(8):3774–89.
Lee BJ, Cho GJ, Norgren RB Jr, Junier MP, Hill DF, Tapia V, et al. TTF-1, a homeodomain gene required for diencephalic morphogenesis, is postnatally expressed in the neuroendocrine brain in a developmentally regulated and cell-specific fashion. Mol Cell Neurosci. 2001;17(1):107–26.
Heger S, Mastronardi C, Dissen GA, Lomniczi A, Cabrera R, Roth CL, et al. Enhanced at puberty 1 (EAP1) is a new transcriptional regulator of the female neuroendocrine reproductive axis. J Clin Investig. 2007;117(8):2145–54.
Widen E, Silventoinen K, Sovio U, Ripatti S, Cousminer DL, Hartikainen AL, et al. Pubertal timing and growth influences cardiometabolic risk factors in adult males and females. Diabetes Care. 2012;35(4):850–6.
Ritte R, Lukanova A, Tjonneland A, Olsen A, Overvad K, Mesrine S, et al. Height, age at menarche and risk of hormone receptor positive and negative breast cancer: a cohort study. Int J Cancer J Int du Cancer. 2012.
He C, Zhang C, Hunter DJ, Hankinson SE, Buck Louis GM, Hediger ML, et al. Age at menarche and risk of type 2 diabetes: results from 2 large prospective cohort studies. Am J Epidemiol. 2010;171(3):334–44.
Kvale G, Heuch I, Nilssen S. Re: “Endometrial cancer and age at last delivery: evidence for an association”. Am J Epidemiol. 1992;135(4):453–5.
Purdie DM, Green AC. Epidemiology of endometrial cancer. Best Pract Res Clin Obstet Gynaecol. 2001;15(3):341–54.
Elks CE, Loos RJ, Sharp SJ, Langenberg C, Ring SM, Timpson NJ, et al. Genetic markers of adult obesity risk are associated with greater early infancy weight gain and growth. PLoS Med. 2010;7(5):e1000284.
Lakshman R, Forouhi NG, Sharp SJ, Luben R, Bingham SA, Khaw KT, et al. Early age at menarche associated with cardiovascular disease and mortality. J Clin Endocrinol Metab. 2009;94(12):4953–60.
Prentice P, Viner RM. Pubertal timing and adult obesity and cardiometabolic risk in women and men: a systematic review and meta-analysis. Int J Obes. 2013;37(8):1036–43.
Ong KK, Northstone K, Wells JC, Rubin C, Ness AR, Golding J, et al. Earlier mother’s age at menarche predicts rapid infancy growth and childhood obesity. PLoS Med. 2007;4(4):e132.
Albanese A, Stanhope R. Does constitutional delayed puberty cause segmental disproportion and short stature? Eur J Pediatr. 1993;152(4):293–6.
Bierich JR, Nolte K, Drews K, Brugmann G. Constitutional delay of growth and adolescence. Results of short-term and long-term treatment with GH. Acta Endocrinol. 1992;127(5):392–6.
Crowne EC, Shalet SM, Wallace WH, Eminson DM, Price DA. Final height in girls with untreated constitutional delay in growth and puberty. Eur J Pediatr. 1991;150(10):708–12.
Crowne EC, Shalet SM, Wallace WH, Eminson DM, Price DA. Final height in boys with untreated constitutional delay in growth and puberty. Arch Dis Child. 1990;65(10):1109–12.
Moreira-Andres MN, Canizo FJ, de la Cruz FJ, Gomez-de la Camara A, Hawkins FG. Bone mineral status in prepubertal children with constitutional delay of growth and puberty. Eur J Endocrinol/Eur Fed Endocr Soc. 1998;139(3):271–5.
Finkelstein JS, Neer RM, Biller BM, Crawford JD, Klibanski A. Osteopenia in men with a history of delayed puberty. N Engl J Med. 1992;326(9):600–4.
Crowne EC, Shalet SM. Management of constitutional delay in growt and puberty. Trends Endocrinol Metab TEM. 1990;1(5):239–42.
Kaltiala-Heino R, Kosunen E, Rimpela M. Pubertal timing, sexual behaviour and self-reported depression in middle adolescence. J Adolesc. 2003;26(5):531–45.
Sedlmeyer IL, Palmert MR. Delayed puberty: analysis of a large case series from an academic center. J clin Endocrinol Metab. 2002;87(4):1613–20.
Sedlmeyer IL. pedigree analysis of constitutional delay of growth and maturation: determination of familial aggregation and inheritance patterns. J Clin Endocrinol Metab. 2002;87(12):5581–6.
Lawaetz JG, Hagen CP, Mieritz MG, Blomberg Jensen M, Petersen JH, Juul A. Evaluation of 451 Danish boys with delayed puberty: diagnostic use of a new puberty nomogram and effects of oral testosterone therapy. J clin Endocrinol Metab. 2015;100(4):1376–85.
LaFranchi S, Hanna CE, Mandel SH. Constitutional delay of growth: expected versus final adult height. Pediatrics. 1991;87(1):82–7.
Albanese A, Stanhope R. Predictive factors in the determination of final height in boys with constitutional delay of growth and puberty. J Pediatr. 1995;126(4):545–50.
Wehkalampi K, Vangonen K, Laine T, Dunkel L. Progressive reduction of relative height in childhood predicts adult stature below target height in boys with constitutional delay of growth and puberty. Horm Res. 2007;68(2):99–104.
Rensonnet C, Kanen F, Coremans C, Ernould C, Albert A, Bourguignon JP. Pubertal growth as a determinant of adult height in boys with constitutional delay of growth and puberty. Horm Res. 1999;51(5):223–9.
Volta C, Ghizzoni L, Buono T, Ferrari F, Virdis R, Bernasconi S. Final height in a group of untreated children with constitutional growth delay. Helv Paediatr Acta. 1988;43(3):171–6.
Bramswig JH, Fasse M, Holthoff ML, von Lengerke HJ, von Petrykowski W, Schellong G. Adult height in boys and girls with untreated short stature and constitutional delay of growth and puberty: accuracy of five different methods of height prediction. J Pediatr. 1990;117(6):886–91.
Arrigo T, Cisternino M, De Luca F, Saggese G, Messina MF, Pasquino AM, et al. Final height outcome in both untreated and testosterone-treated boys with constitutional delay of growth and puberty. J Pediatr Endocrinol Metab JPEM. 1996;9(5):511–7.
Sperlich M, Butenandt O, Schwarz HP. Final height and predicted height in boys with untreated constitutional growth delay. Eur J Pediatr. 1995;154(8):627–32.
Cools BL, Rooman R, Op De Beeck L, Du Caju MV. Boys with a simple delayed puberty reach their target height. Horm Res. 2008;70(4):209–14.
Pozo J, Argente J. Delayed puberty in chronic illness. Best Pract Res Clin Endocrinol Metab. 2002;16(1):73–90.
Watson HJ, Bulik CM. Update on the treatment of anorexia nervosa: review of clinical trials, practice guidelines and emerging interventions. Psychol Med. 2013;43(12):2477–500.
Kujala UM, Alen M, Huhtaniemi IT. Gonadotrophin-releasing hormone and human chorionic gonadotrophin tests reveal that both hypothalamic and testicular endocrine functions are suppressed during acute prolonged physical exercise. Clin Endocrinol. 1990;33(2):219–25.
Roberts AC, McClure RD, Weiner RI, Brooks GA. Overtraining affects male reproductive status. Fertil Steril. 1993;60(4):686–92.
Parra Covarrubias A, Ramos Galvan R. The influence of psychosocial deprivation and body composition on plasma gonadotrophins in children and adolescents. Gac Med Mex. 1992;128(1):7–13.
Silveira LF, Latronico AC. Approach to the patient with hypogonadotropic hypogonadism. J clin Endocrinol Metab. 2013;98(5):1781–8.
Raivio T, Falardeau J, Dwyer A, Quinton R, Hayes FJ, Hughes VA, et al. Reversal of idiopathic hypogonadotropic hypogonadism. N Engl J Med. 2007;357(9):863–73.
Silveira LF, Trarbach EB, Latronico AC. Genetics basis for GnRH-dependent pubertal disorders in humans. Mol Cell Endocrinol. 2010;324(1–2):30–8.
Themmen APN, Huhtaniemi IT. Mutations of gonadotropins and gonadotropin receptors: elucidating the physiology and pathophysiology of pituitary-gonadal function. Endocr Rev. 2000;21(5):551–83.
Layman LC, Lee EJ, Peak DB, Namnoum AB, Vu KV, van Lingen BL, et al. Delayed puberty and hypogonadism caused by mutations in the follicle-stimulating hormone beta-subunit gene. N Engl J Med. 1997;337(9):607–11.
Savage MO, Beattie RM, Camacho-Hubner C, Walker-Smith JA, Sanderson IR. Growth in crohn’s disease. Acta Paediatr Suppl. 1999;88(428):89–92.
Opstad PK. Androgenic hormones during prolonged physical stress, sleep, and energy deficiency. J clin Endocrinol Metab. 1992;74(5):1176–83.
Dunkel L, Perheentupa J, Virtanen M, Maenpaa J. GnRH and HCG tests are both necessary in differential diagnosis of male delayed puberty. Am J Dis Child. 1985;139(5):494–8.
Dunkel L, Huhtaniemi I. Abnormal prolactin secretion in prepubertal boys with hypogonadotrophic hypogonadism–possible involvement in regulation of testicular steroidogenesis. Int J Androl. 1985;8(5):385–92.
Winters SJ, Johnsonbaugh RE, Sherins RJ. The response of prolactin to chlorpromazine stimulation in men with hypogonadotrophic hypogonadism and early pubertal boys: relationship to sex steroid exposure. Clin Endocrinol. 1982;16(4):321–30.
Zevenhuijzen H, Kelnar CJ, Crofton PM. Diagnostic utility of a low-dose gonadotropin-releasing hormone test in the context of puberty disorders. Horm Res. 2004;62(4):168–76.
Dunkel L, Perheentupa J, Virtanen M, Maenpaa J. Gonadotropin-releasing hormone test and human chorionic gonadotropin test in the diagnosis of gonadotropin deficiency in prepubertal boys. J Pediatr. 1985;107(3):388–92.
Segal TY, Mehta A, Anazodo A, Hindmarsh PC, Dattani MT. Role of gonadotropin-releasing hormone and human chorionic gonadotropin stimulation tests in differentiating patients with hypogonadotropic hypogonadism from those with constitutional delay of growth and puberty. J Clin Endocrinol Metab. 2009;94(3):780–5.
Degros V, Cortet-Rudelli C, Soudan B, Dewailly D. The human chorionic gonadotropin test is more powerful than the gonadotropin-releasing hormone agonist test to discriminate male isolated hypogonadotropic hypogonadism from constitutional delayed puberty. Eur J Endocrinol/Eur Fed Endocr Soc. 2003;149(1):23–9.
Martin MM, Martin AL. Constitutional delayed puberty in males and hypogonadotropic hypogonadism: a reliable and cost-effective approach to differential diagnosis. J Pediatr Endocrinol Metab JPEM. 2005;18(9):909–16.
Demir A, Voutilainen R, Juul A, Dunkel L, Alfthan H, Skakkebaek NE, et al. Increase in first morning voided urinary luteinizing hormone levels precedes the physical onset of puberty. J Clin Endocrinol Metab. 1996;81(8):2963–7.
Coutant R, Biette-Demeneix E, Bouvattier C, Bouhours-Nouet N, Gatelais F, Dufresne S, et al. Baseline inhibin B and anti-Mullerian hormone measurements for diagnosis of hypogonadotropic hypogonadism (HH) in boys with delayed puberty. J Clin Endocrinol Metab. 2010;95(12):5225–32.
Semple RK, Topaloglu AK. The recent genetics of hypogonadotrophic hypogonadism - novel insights and new questions. Clin Endocrinol. 2010;72(4):427–35.
Poyrazoglu S, Gunoz H, Darendeliler F, Saka N, Bundak R, Bas F. Constitutional delay of growth and puberty: from presentation to final height. J Pediatr Endocrinol Metab JPEM. 2005;18(2):171–9.
Rosenfeld RG, Northcraft GB, Hintz RL. A prospective, randomized study of testosterone treatment of constitutional delay of growth and development in male adolescents. Pediatrics. 1982;69(6):681–7.
Soliman AT, Khadir MM, Asfour M. Testosterone treatment in adolescent boys with constitutional delay of growth and development. Metab Clin Exp. 1995;44(8):1013–5.
Kelly BP, Paterson WF, Donaldson MD. Final height outcome and value of height prediction in boys with constitutional delay in growth and adolescence treated with intramuscular testosterone 125 mg per month for 3 months. Clin Endocrinol. 2003;58(3):267–72.
Wilson DM, Kei J, Hintz RL, Rosenfeld RG. Effects of testosterone therapy for pubertal delay. Am J Dis Child. 1988;142(1):96–9.
De Luca F, Argente J, Cavallo L, Crowne E, Delemarre-Van de Waal HA, De Sanctis C, et al. Management of puberty in constitutional delay of growth and puberty. J Pediatr Endocrinol Metab JPEM. 2001;14 Suppl 2:953–7.
Rogol AD, Swerdloff RS, Reiter EO, Ross JL, ZumBrunnen TL, Pratt GA, et al. A multicenter, open-label, observational study of testosterone gel (1%) in the treatment of adolescent boys with klinefelter syndrome or anorchia. J Adolesc Health. 2014;54(1):20–5.
Johansen KL. Treatment of hypogonadism in men with chronic kidney disease. Adv Chronic Kidney Dis. 2004;11(4):348–56.
Jeong HR, Shim YS, Lee HS, Hwang JS. The effect of growth hormone treatment on height in children with idiopathic short stature. J Pediatr Endocrinol Metab JPEM. 2014.
Bryant J, Baxter L, Cave CB, Milne R. Recombinant growth hormone for idiopathic short stature in children and adolescents. Cochrane Database Syst Rev. 2007(3):CD004440.
Hero M, Norjavaara E, Dunkel L. Inhibition of estrogen biosynthesis with a potent aromatase inhibitor increases predicted adult height in boys with idiopathic short stature: a randomized controlled trial. J Clin Endocrinol Metab. 2005;90(12):6396–402.
Wickman S, Sipila I, Ankarberg-Lindgren C, Norjavaara E, Dunkel L. A specific aromatase inhibitor and potential increase in adult height in boys with delayed puberty: a randomised controlled trial. Lancet. 2001;357(9270):1743–8.
de Ronde W. Therapeutic uses of aromatase inhibitors in men. Curr Opin Endocrinol Diabetes Obes. 2007;14(3):235–40.
Hero M, Toiviainen-Salo S, Wickman S, Makitie O, Dunkel L. Vertebral morphology in aromatase inhibitor-treated males with idiopathic short stature or constitutional delay of puberty. J Bone Miner Res. 2010;25(7):1536–43.
Gilsanz V, Chalfant J, Kalkwarf H, Zemel B, Lappe J, Oberfield S, et al. Age at onset of puberty predicts bone mass in young adulthood. J Pediatr. 2011;158(1):100–5, 5 e1–2.
van Buuren S. Growth charts of human development. Stat Methods Med Res. 2013;23(4):346–68.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2017 Springer International Publishing AG
About this chapter
Cite this chapter
Howard, S., Dunkel, L. (2017). Normal and Delayed Puberty. In: Winters, S., Huhtaniemi, I. (eds) Male Hypogonadism. Contemporary Endocrinology. Humana Press, Cham. https://doi.org/10.1007/978-3-319-53298-1_4
Download citation
DOI: https://doi.org/10.1007/978-3-319-53298-1_4
Published:
Publisher Name: Humana Press, Cham
Print ISBN: 978-3-319-53296-7
Online ISBN: 978-3-319-53298-1
eBook Packages: MedicineMedicine (R0)